Evaluation of the Reporting Standard Guidelines of Network Meta-Analyses in Physical Therapy: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration
2.2. Information Sources and Search Strategy
2.3. Identification of Studies
2.4. Hand Search
2.5. Study Selection
2.6. Data Collection Process and Coding Items of Clinical Study Characteristics
2.7. Reporting of General Components and Key Methodological Components of the Systematic Review Process
2.8. Evaluation of Reporting Standard Guidelines Assessment Tools
2.9. Statistical Analysis: Descriptive Statistics and Frequency
2.10. Ethical Approval
3. Results
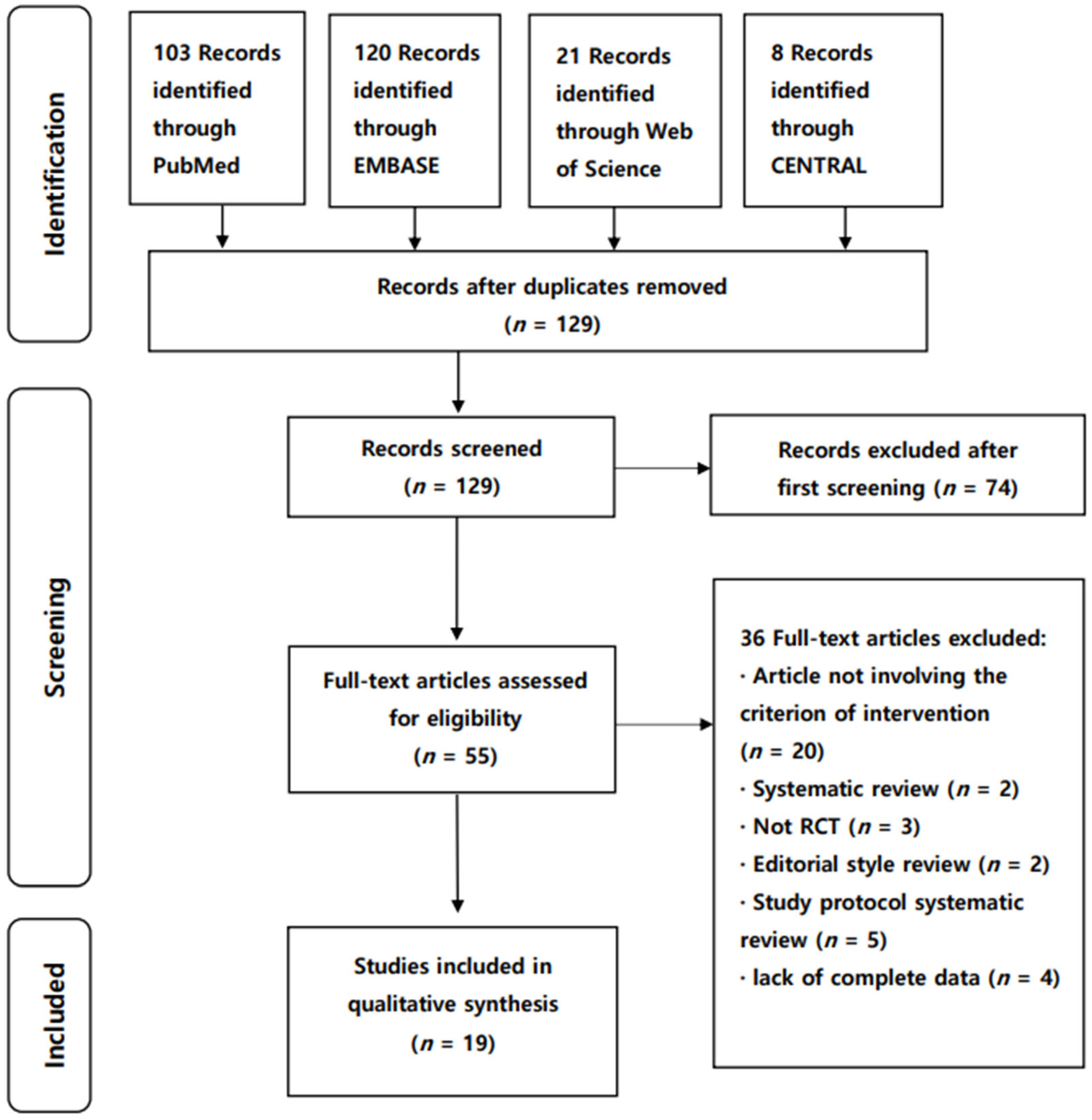
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Epidemiological and Descriptive Characteristics
3.2.2. Clinical and General Characteristics of Included Studies
4. Reporting Standard Guidelines Assessment
4.1. Reporting of Key Methodological Components of the NMA Process (New Items, S1–5)
4.2. Descriptive Analysis
5. Discussion
5.1. Reporting of 16 Items from the Original PRISMA Statement
5.2. Reporting of 11 Modified Items
5.3. Reporting of Five New Items and NMA Assumptions
5.4. Limitation and Implication of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bagg, M.K.; Salanti, G.; McAuley, J.H. Comparing interventions with network meta-analysis. J. Physiother. 2018, 64, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Bafeta, A.; Trinquart, L.; Seror, R.; Ravaud, P. Analysis of the systematic reviews process in reports of network meta-analyses: Methodological systematic review. BMJ 2013, 347, f3675. [Google Scholar] [CrossRef] [Green Version]
- Leucht, S.; Chaimani, A.; Cipriani, A.S.; Davis, J.M.; Furukawa, T.A.; Salanti, G. Network meta-analyses should be the highest level of evidence in treatment guidelines. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 477–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolakopoulou, A.; Chaimani, A.; Veroniki, A.A.; Vasiliadis, H.S.; Schmid, C.H.; Salanti, G. Characteristics of networks of interventions: A description of a database of 186 published networks. PLoS ONE 2014, 9, e86754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petropoulou, M.; Nikolakopoulou, A.; Veroniki, A.A.; Rios, P.; Vafaei, A.; Zarin, W.; Giannatsi, M.; Sullivan, S.; Tricco, A.C.; Chaimani, A.; et al. Bibliographic study showed improving statistical methodology of network meta-analyses published between 1999 and 2015. J. Clin. Epidemiol. 2017, 82, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Zarin, W.; Veroniki, A.A.; Nincic, V.; Vafaei, A.; Reynen, E.; Motiwala, S.S.; Antony, J.; Sullivan, S.M.; Rios, P.; Daly, C.; et al. Characteristics and knowledge synthesis approach for 456 network meta-analyses: A scoping review. BMC Med. 2017, 15, 3. [Google Scholar] [CrossRef] [Green Version]
- Goh, S.L.; Persson, M.S.M.; Stocks, J.; Hou, Y.; Welton, N.J.; Lin, J.; Hall, M.C.; Doherty, M.; Zhang, W. Relative efficacy of different exercises for pain, function, performance and quality of life in knee and hip osteoarthritis: Systematic review and network meta-analysis. Sports Med. 2019, 49, 743–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.C.; Chen, S.Y.; Yang, J.L.; Lin, J.J. Effectiveness of stretching exercise versus kinesiotaping in improving length of the pectoralis minor: A systematic review and network meta-analysis. Phys. Ther. Sport. 2019, 40, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Ades, A.E.; Caldwell, D.M.; Reken, S.; Welton, N.J.; Sutton, A.J.; Dias, S. Evidence synthesis for decision making 7: A reviewer’s checklist. Med. Decis. Mak. 2013, 33, 679–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scapini, K.B.; Bohlke, M.; Moraes, O.A.; Rodrigues, C.G.; Inácio, J.F.; Sbruzzi, G.; Leguisamo, C.P.; Sanches, I.C.; Tourinho Filho, H.; Irigoyen, M.C. Combined training is the most effective training modality to improve aerobic capacity and blood pressure control in people requiring haemodialysis for end–stage renal disease: Systematic review and network meta-analysis. J. Physiother. 2019, 65, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Donegan, S.; Williamson, P.; Gamble, C.; Tudur-Smith, C. Indirect comparisons: A review of reporting and methodological quality. PLoS ONE 2010, 5, e11054. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Shin, I.S. Critical quality evaluation of network meta-analyses in dental care. J. Dent. 2018, 75, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Tonin, F.S.; Borba, H.H.; Leonart, L.P.; Mendes, A.M.; Steimbach, L.M.; Pontarolo, R.; Fernandez-Llimos, F. Methodological quality assessment of network meta-analysis of drug interventions: Implications from a systematic review. Int. J. Epidemiol. 2019, 48, 620–632. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Wang, H.; Zou, J.; Li, X.; Jin, X.; Cao, Y.; Tian, J.; Ge, L.; Lee, M.S.; Zhang, J. Assessing the methodological and reporting quality of network meta-analyses in Chinese medicine. Medicine 2018, 97, e13052. [Google Scholar] [CrossRef] [PubMed]
- Pratt, M.; Wieland, S.; Ahmadzai, N.; Butler, C.; Wolfe, D.; Pussagoda, K.; Skidmore, B.; Veroniki, A.; Rios, P.; Tricco, A.C.; et al. A scoping review of network meta-analyses assessing the efficacy and safety of complementary and alternative medicine interventions. Syst. Rev. 2020, 9, 97. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Zhang, L.; Gu, S.; Sun, J.; Qin, Z.; Yue, J.; Zhong, Y.; Ding, N.; Gao, R. Comparative effectiveness of extracorporeal shock wave, ultrasound, low-level laser therapy, noninvasive interactive neurostimulation, and pulsed radiofrequency treatment for treating plantar fasciitis: A systematic review and network meta-analysis. Medicine 2018, 97, e12819. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.F.; Lin, M.T.; Hsiao, M.Y.; Yeh, Y.C.; Liang, Y.C.; Wang, T.G. Comparative efficacy of noninvasive neurostimulation therapies for acute and subacute poststroke dysphagia: A systematic review and network meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 739–750.e4. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Tu, Y.K.; Wang, T.G.; Huang, Y.T.; Chien, K.L. Effects of resistance training, endurance training and whole-body vibration on lean body mass, muscle strength and physical performance in older people: A systematic review and network meta-analysis. Age Ageing 2018, 47, 367–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Yin, H.; Wang, X.; Jia, Y.; Wang, C.; Wang, L.; Chen, L. Efficacy of different types of exercises on global cognition in adults with mild cognitive impairment: A network meta-analysis. Aging Clin. Exp. Res. 2019, 31, 1391–1400. [Google Scholar] [CrossRef] [PubMed]
- Tsikopoulos, K.; Mavridis, D.; Georgiannos, D.; Cain, M.S. Efficacy of non-surgical interventions on dynamic balance in patients with ankle instability: A network meta-analysis. J. Sci. Med. Sport 2018, 21, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Li, H.; Yang, T.; Deng, Z.H.; Yang, Y.; Zhang, Y.; Lei, G.H. Electrical stimulation for pain relief in knee osteoarthritis: Systematic review and network meta-analysis. Osteoarthr. Cart. 2015, 23, 189–202. [Google Scholar] [CrossRef] [Green Version]
- Uthman, O.A.; van der Windt, D.A.; Jordan, J.L.; Dziedzic, K.S.; Healey, E.L.; Peat, G.M.; Foster, N.E. Exercise for lower limb osteoarthritis: Systematic review incorporating trial sequential analysis and network meta-analysis. BMJ 2013, 347, f5555. [Google Scholar] [CrossRef] [Green Version]
- Pan, B.; Ge, L.; Xun, Y.Q.; Chen, Y.J.; Gao, C.Y.; Han, X.; Zuo, L.Q.; Shan, H.Q.; Yang, K.H.; Ding, G.W.; et al. Exercise training modalities in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 72. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Missbach, B.; Dias, S.; König, J.; Hoffmann, G. Impact of different training modalities on glycaemic control and blood lipids in patients with type 2 diabetes: A systematic review and network meta-analysis. Diabetologia 2014, 57, 1789–1797. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Dias, S.; Strasser, B.; Hoffmann, G. Impact of different training modalities on anthropometric and metabolic characteristics in overweight/obese subjects: A systematic review and network meta-analysis. PLoS ONE 2013, 8, e82853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, W.K.W.; Wu, I.X.Y.; Sit, R.W.S.; Ho, R.S.T.; Wong, C.H.L.; Wong, S.Y.S.; Chung, V.C.H. Low-level laser therapy for carpal tunnel syndrome: Systematic review and network meta-analysis. Physiotherapy 2020, 106, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Young, L.; Li, F. Network meta-analysis of various nonpharmacological interventions on pain relief in older adults with osteoarthritis. Am. J. Phys. Med. Rehabil. 2019, 98, 469–478. [Google Scholar] [CrossRef]
- Tang, L.; Fang, Y.; Yin, J. The effects of exercise interventions on Parkinson’s disease: A Bayesian network meta–analysis. J. Clin. Neurosci. 2019, 70, 47–54. [Google Scholar] [CrossRef]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sport Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Hilfiker, R.; Meichtry, A.; Eicher, M.; Nilsson Balfe, L.; Knols, R.H.; Verra, M.L.; Taeymans, J. Exercise and other non–pharmaceutical interventions for cancer–related fatigue in patients during or after cancer treatment: A systematic review incorporating an indirect–comparisons meta-analysis. Br. J. Sport Med. 2018, 52, 651–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.C.; Tsai, W.C.; Tu, Y.K.; Yu, T.Y. Comparative effectiveness of nonoperative treatments for chronic calcific tendinitis of the shoulder: A systematic review and network meta-analysis of randomized controlled trials. Arch. Phys. Med. Rehabil. 2017, 98, 1678–1692.e6. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Zhang, J.; Ge, L.; Yang, K.; Song, F. The methodological and reporting quality of systematic reviews from China and the USA are similar. J. Clin. Epidemiol. 2017, 85, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.L.; Ge, L.; Ma, J.C.; Zeng, Q.L.; Yao, L.; An, N.; Ding, J.X.; Gan, Y.H.; Tian, J.H. Quality of reporting of systematic reviews published in “evidence-based” Chinese journals. Syst. Rev. 2014, 3, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldwell, D.M.; Dias, S.; Welton, N.J. Extending treatment networks in health technology assessment: How far should we go? Value Health 2015, 18, 673–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reken, S.; Sturtz, S.; Kiefer, C.; Böhler, Y.B.; Wieseler, B. Assumptions of mixed treatment comparisons in health technology assessments-challenges and possible steps for practical application. PLoS ONE 2016, 11, e0160712. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G.; Del Giovane, C.; Chaimani, A.; Caldwell, D.M.; Higgins, J.P. Evaluating the quality of evidence from a network meta-analysis. PLoS ONE 2014, 9, e99682. [Google Scholar] [CrossRef]
- Dias, S.; Sutton, A.J.; Ades, A.E.; Welton, N.J. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 2013, 33, 607–617. [Google Scholar] [CrossRef] [Green Version]
- Salanti, G.; Kavvoura, F.K.; Ioannidis, J.P. Exploring the geometry of treatment networks. Ann. Intern. Med. 2008, 148, 544–553. [Google Scholar] [CrossRef]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Caldwell, D.M.; Lu, G.; Ades, A.E. Evidence synthesis for decision making 4: Inconsistency in networks of evidence based on randomized controlled trials. Med. Decis. Mak. 2013, 33, 641–656. [Google Scholar] [CrossRef]


{kind=link}
| Criteria | Determinants |
|---|---|
| Population | Adults or patients related to physical therapy |
| Intervention | At least one group received physical therapy |
| Comparison | At least one group received a comparison intervention or no intervention |
| Outcome measures | Functional outcome relating to physical therapy |
| Design | Randomized trial with physical therapy as treatment |
| Database | Detailed Search Strategies | Records Found |
|---|---|---|
| PubMed | (“network meta-analysis” [MeSH] OR “network meta-analyses” [all] OR “network meta analysis” [all] OR “network meta analyses” [all]) AND (“Physical Therapy Modalities” [MeSH]) | 73 |
| (“network meta-analysis” [MeSH] OR “network meta-analyses” [all] OR “network meta analysis” [all] OR “network meta analyses” [all]) AND (“Physiotherapy” [all]) | 30 | |
| (“network meta-analysis” [MeSH] OR “network meta-analyses” [all] OR “network meta analysis” [all] OR “network meta analyses” [all]) AND (“Physical Therapy Specialty” [MeSH]) | 0 | |
| EMBASE | (‘network meta-analysis’/exp OR ‘network meta-analysis’ OR ‘network meta-analyses’/exp OR ‘network meta-analyses’ OR ‘network meta analysis’/exp OR ‘network meta analysis’ OR ‘network metaanalysis’/exp OR ‘network metaanalysis’) AND (‘physical therapy modalities’/exp OR ‘physical therapy modalities’) | 31 |
| (‘network meta-analysis’/exp OR ‘network meta-analysis’ OR ‘network meta-analyses’/exp OR ‘network meta-analyses’ OR ‘network meta analysis’/exp OR ‘network meta analysis’ OR ‘network metaanalysis’/exp OR ‘network metaanalysis’) AND (‘physiotherapy’/exp OR ‘physiotherapy’) | 58 | |
| (‘network meta-analysis’/exp OR ‘network meta-analysis’ OR ‘network meta-analyses’/exp OR ‘network meta-analyses’ OR ‘network meta analysis’/exp OR ‘network meta analysis’ OR ‘network metaanalysis’/exp OR ‘network metaanalysis’) AND (‘physical therapy specialty’/exp OR ‘physical therapy specialty’) | 31 | |
| Web of Science | TOPIC: (“network meta-analysis” OR “network metaanalysis”) AND (“Physical Therapy Modalities” OR “Physical Therapy Specialty” OR “Physiotherapy”) | 21 |
| Cochrane Central Register of Controlled Trials | (network meta-analysis OR network metaanalysis) AND (Physical Therapy Modalities OR Physical Therapy Specialty OR Physiotherapy) | 8 |
| No. | Items | Checklist (Summary) | PRISMA n (%) | PRISMA-NMA n (%) | |
| Common items for PRISMA and PRISMA-NMA | |||||
| 4 | Introduction, objectives | Provide an explicit statement of questions (e.g., PICOS) | 18 (94.7%) | 18 (94.7%) | |
| 5 | Methods, protocol and registration | Indicate whether a review protocol was followed, provide the registration number | 13 (68.4%) | 13 (68.4%) | |
| 7 | Methods, information sources | Describe all information sources in the search and date last searched | 19 (100%) | 19 (100%) | |
| 8 | Methods, search | Present the full electronic search strategy for at least one database | 19 (100%) | 19 (100%) | |
| 9 | Methods, study selection | State the process for selecting studies | 18 (94.7%) | 18 (94.7%) | |
| 10 | Methods, data collection process | Describe the method of data extraction from the selected reports | 19 (100%) | 19 (100%) | |
| 11 | Methods, data items | List and define all variables for which data were sought | 13 (68.4%) | 13 (68.4%) | |
| 12 | Methods, risk of bias within studies | Describe the methods used to assess the risk of bias | 18 (94.7%) | 18 (94.7%) | |
| 15 | Methods, risk of bias across studies | Specify any risk of bias assessment that might have affected the cumulative evidence | 13 (68.4%) | 13 (68.4%) | |
| 17 | Results, study selection | Provide the numbers of studies screened, assessed for eligibility, and included | 19 (100%) | 19 (100%) | |
| 18 | Results, study characteristics | For each study, present the characteristics for which data were extracted | 19 (100%) | 19 (100%) | |
| 19 | Results, risk of bias within studies | Present data on the risk of bias of each study | 19 (100%) | 19 (100%) | |
| 22 | Results, risk of bias across studies | Present the results of assessment of risk of bias across studies | 12 (63.2%) | 12 (63.2%) | |
| 24 | Discussion, summary evidence | Summarize the main findings including the strength of evidence | 19 (100%) | 19 (100%) | |
| 26 | Discussion, conclusion | Provide a general interpretation of the results and their implications | 19 (100%) | 19 (100%) | |
| 27 | Funding | Describe sources of funding | 6 (31.6%) | 6 (31.6%) | |
| PRISMA items modified for PRISMA-NMA | |||||
| 1 | Title | Identify the report as a systematic review incorporating a network meta-analysis (or related form) | 19 (100%) | 17 (89.5%) | |
| 2 | Abstract, structured summary | Provide a structured summary mentioning the network meta-analysis | 19 (100%) | 19 (100%) | |
| 3 | Introduction, rationale | Describe the rationale for the review; mention why a network meta-analysis has been conducted | 19 (100%) | 19 (100%) | |
| 6 | Methods, eligibility criteria | Specify study characteristics, clearly describe eligible treatments included in the network | 11 (57.9%) | 1 (5.3%) | |
| 13 | Methods, summary measures | State the principal summary measures, describe the use of additional measures such as treatment rankings, SUCRA values | 19 (100%) | 16 (84.2%) | |
| 14 | Methods, planned analyses | Describe the methods of handling data and combining results (e.g., handling of multi-arm trials; selection of variance structure; prior distributions in Bayesian analyses; model fit) | 19 (100%) | 9 (47.4%) | |
| 16 | Methods, additional analyses | Describe the methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression, or alternative formulations of the network) | 13 (68.4%) | 13 (68.4%) | |
| 20 | Results, individual studies | Present simplified summary data for each intervention group, effect estimates and confidence intervals; modified approaches may be used in larger networks | 19 (100%) | 19 (100%) | |
| 21 | Results, synthesis of results | Present the results of each meta-analysis performed including confidence/credible intervals | 19 (100%) | 19 (100%) | |
| 23 | Results, additional analyses | Provide the results of other analyses (e.g., sensitivity/subgroup analyses, meta-regression, alternative geometries, alternative prior distributions) | 11 (57.9%) | 11 (57.9%) | |
| 25 | Discussion, limitations | Discuss the limitations and comment on the validity of the assumptions such as transitivity and consistency, comment on concerns of network geometry | 19 (100%) | 18 (94.7%) | |
| Items included exclusively in PRISMA-NMA | PRISMA n (%) | PRISMA-NMA n (%) | |||
| N = 19 | N = 17 a | ||||
| S1 | Methods, geometry of the network | Describe the methods used to explore the network geometry, including how the evidence was graphically summarized | - | 6 (31.6%) | 4 (23.5%) a |
| S2 | Methods, assessment of consistency | Describe the statistical methods used to evaluate the agreement between direct and indirect evidence | - | 15 (78.9%) | 13 (76.5%) a |
| S3 | Results, network structure | Provide a network graph of the included studies | - | 18 (94.7%) | 17 (100%) a |
| S4 | Results, summary of geometry | Provide a brief overview of the network characteristics | - | 18 (94.7%) | 17 (100%) a |
| S5 | Results, exploration of inconsistency | Describe results from investigations of inconsistency; this may include such information as measures of model fit to compare factors such as consistency and inconsistency models, or p-values | - | 15 (78.9%) | 13 (76.5%) a |
| Common Items for PRISMA and PRISMA-NMA | Summary | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | C | P | N |
| 4 | Introduction, objectives | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 18 | 0 | 1 |
| 5 | Methods, protocol and registration | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 13 | 0 | 6 |
| 7 | Methods, information sources | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 8 | Methods, search | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 9 | Methods, study selection | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 18 | 0 | 1 |
| 10 | Methods, data collection process | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 11 | Methods, data items | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 13 | 0 | 6 |
| 12 | Methods, risk of bias within studies | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 18 | 1 | 0 |
| 15 | Methods, risk of bias across studies | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 13 | 0 | 6 |
| 17 | Results, study selection | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 18 | Results, study characteristics | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 19 | Results, risk of bias within studies | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 22 | Results, risk of bias across studies | 0.5 | 0.5 | 1 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 1 | 1 | 1 | 12 | 7 | 0 |
| 24 | Discussion, summary evidence | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 26 | Discussion, conclusions | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 27 | Funding | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 6 | 0 | 13 |
| PRISMA items modified for PRISMA-NMA | Summary | ||||||||||||||||||||||
| No. | Section | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | C | P | N |
| 1 | Title | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 17 | 2 | 0 |
| 2 | Abstract, structured summary | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 2 | 17 | 0 |
| 3 | Introduction, rationale | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 6 | Methods, eligibility Criteria | 0.5 | 0.5 | 0.5 | 0.5 | 0 | 0.5 | 0.5 | 0.5 | 0 | 0.5 | 0 | 0.5 | 0 | 0 | 0.5 | 0 | 1 | 0 | 0 | 1 | 10 | 8 |
| 13 | Methods, summary measures | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 16 | 0 | 3 |
| 14 | Methods, planned analyses | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 1 | 1 | 0.5 | 1 | 0.5 | 9 | 10 | 0 |
| 16 | Methods, additional analyses | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 13 | 0 | 6 |
| 20 | Results, individual studies | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 21 | Results, synthesis of results | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 19 | 0 | 0 |
| 23 | Results, additional analyses | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 11 | 0 | 8 |
| 25 | Discussion, limitations | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 18 | 1 | 0 |
| Items included exclusively in PRISMA-NMA | Summary | ||||||||||||||||||||||
| No. | Section | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | C | P | N |
| S1 | Methods, geometry of the network | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 6 | 0 | 13 |
| S2 | Methods, assessment of consistency | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 15 | 0 | 4 |
| S3 | Results, network structure | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 18 | 0 | 1 |
| S4 | Results, summary of network geometry | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 18 | 0 | 1 |
| S5 | Results, exploration of inconsistencies | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 15 | 0 | 4 |
| Summary | 26.5 | 28.5 | 27.5 | 23.5 | 27 | 24 | 26.5 | 26.5 | 25.5 | 27 | 29.5 | 28 | 22.5 | 28 | 29 | 21 | 29.5 | 27 | 26 | ||||
| Quality assessment | H | H | H | M | H | M | H | H | M | H | H | H | M | H | H | M | H | H | H | ||||
| Quality Score | Year | Impact Factor | Study Number | Participants | |
|---|---|---|---|---|---|
| Mean | 26.5 | 2018 | 5.20 | 42.2 | 3406 |
| Median | 27.0 | 2018 | 3.61 | 19.0 | 1254 |
| Standard deviation | 2.32 | 2.17 | 3.62 | 55.6 | 5533 |
| Interquartile range | 2.25 | 1.50 | 4.53 | 18.5 | 1884 |
| Range | 8.50 | 7.00 | 10.5 | 239 | 23,394 |
| Minimum | 21.0 | 2013 | 1.55 | 6.00 | 263 |
| Maximum | 29.5 | 2020 | 12.0 | 245 | 23,657 |
| 25th percentile | 25.8 | 2018 | 2.59 | 16.5 | 834 |
| 50th percentile | 27.0 | 2018 | 3.61 | 19.0 | 1254 |
| 75th percentile | 28.0 | 2019 | 7.12 | 35.0 | 2718 |
| Group | N | Mean | Median | SD | SE | |
|---|---|---|---|---|---|---|
| Quality score | High | 9 | 27.5 | 27.0 | 1.46 | 0.486 |
| Low | 10 | 25.6 | 26.3 | 2.62 | 0.831 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, S.-H.; Shin, I.-S. Evaluation of the Reporting Standard Guidelines of Network Meta-Analyses in Physical Therapy: A Systematic Review. Healthcare 2022, 10, 2371. https://doi.org/10.3390/healthcare10122371
Cho S-H, Shin I-S. Evaluation of the Reporting Standard Guidelines of Network Meta-Analyses in Physical Therapy: A Systematic Review. Healthcare. 2022; 10(12):2371. https://doi.org/10.3390/healthcare10122371
Chicago/Turabian StyleCho, Sung-Hyoun, and In-Soo Shin. 2022. "Evaluation of the Reporting Standard Guidelines of Network Meta-Analyses in Physical Therapy: A Systematic Review" Healthcare 10, no. 12: 2371. https://doi.org/10.3390/healthcare10122371