1. Introduction
The coronavirus disease 2019 (COVID-19) pandemic is an unparalleled challenge for the health sector, mostly for pulmonology departments, followed closely by emergency care departments and ambulance services [
1,
2,
3,
4,
5,
6,
7]. Soon after the appearance of this novel virus, it caused a considerable burden for healthcare systems globally. In Hungary, the first case was reported on 4 March 2020 [
8]. The first reported COVID-19-related death occurred on 15 March [
9]. On 18 March, the Operational Corps Responsible for the Containment of the Coronavirus Epidemic (Koronavírus-járvány Elleni Védekezésért Felelős Operatív Törzs) declared that the infectious virus could be present anywhere in Hungary [
10]. Hungary has since experienced its fourth COVID-19 wave, resulting in the deaths of more than 48,000 citizens [
11].
In Hungary, the National Ambulance Service (NAS) is responsible for all ambulance-related tasks nationwide, and during the pandemic, their role became even more important. In addition to the general care, in late March 2020, the service received additional duties. In cooperation with the universities of clinical medicine, the screening of possible COVID-19 patients became the task of the NAS, and the transportation of all confirmed cases of patients was also their responsibility [
12].
The NAS already faced considerable challenges before the pandemic because the Hungarian health indicators are among the worst in the European Union [
13,
14,
15]. Therefore, it is imperative to understand the degree to which the COVID-19 wave increased the workload of the “first responders” in health care. Despite the importance of the topic, only one study investigated how emergency ambulance deliveries within the United Kingdom were affected by the COVID-19 pandemic [
16]. Because this study was conducted relatively early during the pandemic, the researchers could only investigate the first COVID-19 wave; thus, there is no information regarding the impact of the following more severe waves, which could be useful for those organizing emergency ambulance services. Although other articles have discussed the increased burden on ambulance services during the COVID-19 pandemic, these published papers mainly focused on how to identify COVID-19 infections and other factors related to medical technology [
17,
18,
19,
20]. Owing to the lack of knowledge and the concern that a new global pandemic may emerge in the future, it is important to investigate this question thoroughly. Therefore, the primary aim of this research was to examine the performance of the NAS during the first four waves of the pandemic.
2. Materials and Methods
This is a retrospective follow-up study of Hungarian citizens conducted to estimate the incidence of cases of emergency assistance in the period of 2019–2021. All data regarding ambulance activities were provided by the management of the NAS, which is the largest medical and ambulance institution in Hungary, and which operates the national registry of ambulance performance implemented in late 2018. In order to obtain at least two whole years of baseline data before the COVID-19 pandemic, the original intention was to obtain data starting from January 2018. However, because the NAS only implemented a uniform data recording method in late 2018, the time period under consideration ranged from January 2019 to December 2021. The subjects of our study are the deliveries and COVID-19 screenings related to patients aged 15 years and older and performed by the NAS from 2019 to 2021. Our outcome variables were annual number of deliveries of patients with diagnosis of COVID-19 (ICD-10: U07.1), COVID-19 screening (ICD-10: Z11.52), acute myocardial infarction (ICD10: I21, I22), haemorrhagic stroke (ICD10: I60, I61, I62), ischemic stroke (ICD10: I63, I64), and non-COVID-19 (ICD-10: all but U07.1 and Z11.52). The specific medical conditions were chosen because, in connection with ambulance deliveries, it is the most important for these three diseases to start with the appropriate quality of care at the right time. These data were aggregated for each week of the investigated time period, then stratified by gender and age (15–64 vs. 65+).
For the descriptive statistical analysis ratios, means, standard deviations, medians, and interquartile ranges were calculated for each subgroup. The Shapiro–Wilk test was used to investigate the distribution of the executed COVID-19 screenings and ambulance activities regarding the aforementioned types of deliveries.
To determine whether the distribution of gender and age significantly differed between the three investigated years, Pearson’s chi-squared test was used. Cases in which gender or age were not recorded by the ambulance staff were excluded from the analysis. Student’s t-test was applied to explore whether the number of COVID-19 screenings and the number of investigated ambulance deliveries significantly changed during the period of 2020–2021.
A weekly moving average was calculated to visualize the overall trends of acute myocardial infarction, stroke, and non-COVID-19-related ambulance deliveries. In addition, we calculated the upper and lower 95% standard deviations using the year 2019 as a baseline reference. This approach was adopted from a British study investigating emergency ambulance deliveries during the first COVID-19 wave for STEMI (ST elevation myocardial infarction) and stroke [
16]. By doing so, the goal was to explore which weeks had considerably more or fewer deliveries. Additionally, a linear trend was inserted into each figure to visualize the overall trends. R-squared values were calculated to determine how these trends fit the dataset. These calculations were not conducted for COVID-19 screenings and COVID-19 -elated deliveries, as there were no such cases in 2019.
To show how the screenings and deliveries are related to the four COVID-19 waves, we calculated the beginning and end of each wave in Hungary. There is an ongoing debate on how to define the start and the end of any given COVID-19 wave [
21,
22]. Two methods were considered by our research team. We determined that adopting the method used in Chile might be subject to limitations in Hungary, as this approach assumes that the two countries have a similar population density [
21]. Therefore, we opted to use the method that considers the reproduction rate (R) of the virus [
22]. Based on this approach—with the exception of the very first case identified in Hungary—the start of a COVID-19 wave was defined by an R value of more than 1 for two consecutive weeks, and the end of a COVID-19 wave was marked two weeks before the R value increased to more than 1. The R values regarding the COVID-19 pandemic in Hungary were obtained from the Our World in Data website [
23]. As the earliest data were from 22 March 2022, we decided that the first confirmed COVID-19 case in Hungary would be the start of the first COVID-19 wave [
8].
Microsoft Excel was used for the descriptive statistical analysis and to create the tables and figures. Intercooled STATA v13 was used to evaluate the normality of continuous variables and for all comparative statistical analysis.
3. Results
From January 2019 to December 2021, NAS delivered 2,798,348 patients aged 15 years or older (including 190,734 with COVID-19) and performed 1,557,388 COVID-19 screenings. The distribution of these activities based on gender and age are shown in
Table 1 and
Table 2.
Similarly, when comparing the distribution of gender and age regarding COVID-19 screenings and COVID-19-related ambulance deliveries (
Table 2), the differences between 2020 and 2021 were always significant (
p < 0.001).
Table 3 shows that the number of deliveries involving acute myocardial infarction significantly increased between the 2019/2020 (
p < 0.001) and the 2019/2021 (
p < 0.001) data. However, no significant change was observed between 2020 and 2021 (
p = 0.815). Regarding haemorrhagic stroke, a similar pattern is shown but with a negative correlation. A significant decrease was detected when comparing the 2019/2020 (
p < 0.001) and the 2019/2021 data (
p < 0.001), but no significant difference was found when comparing the 2020 and 2021 data (
p = 0.268). The deliveries of ischemic stroke cases consistently and significantly rose each year (
p < 0.001). As the majority of stroke cases were recorded as ischemic, all stroke deliveries also significantly increased each year (
p < 0.001). Overall non-COVID-19 deliveries significantly rose from 817,857 cases in 2019 to 841,427 cases in 2020 (
p < 0.001) and continued to increase significantly to 948,330 cases in 2021 (
p = 0.005). Both the number of COVID-19 screenings and COVID-19-related ambulance deliveries increased significantly from 2020 to 2021 (
p < 0.001).
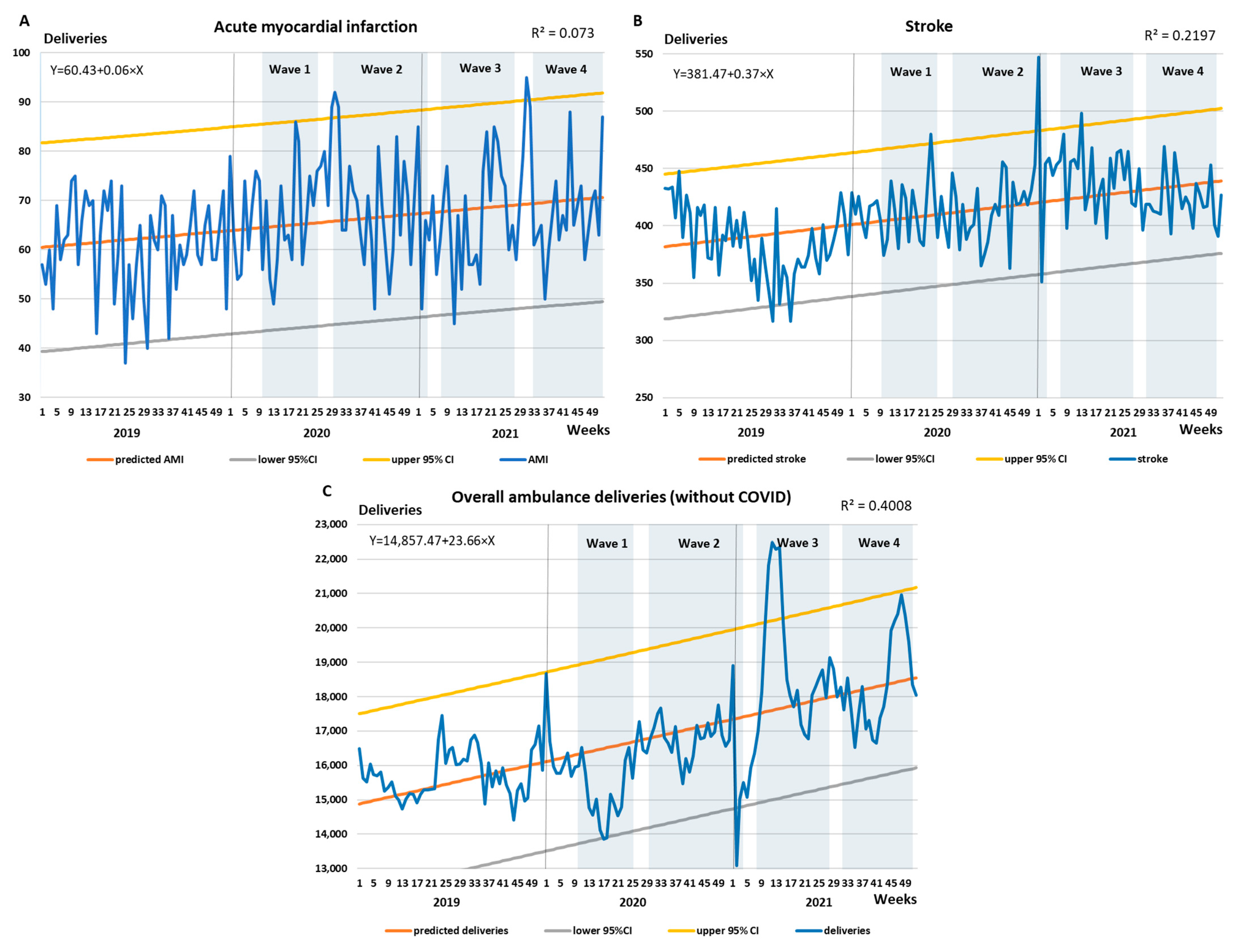
Figure 1A shows that the weekly average of deliveries involving acute myocardial infarction rose steadily during the three years and peaked at the beginning of the second COVID-19 wave. During this peak, the upper 95% standard deviation threshold was also breached. The R-squared value was only 0.073, partly because the number of deliveries between 2020 and 2021 did not differ significantly (see
Table 3).
Figure 1B shows that the increase in the weekly average of deliveries regarding stroke increased more considerably. The peak occurred during the third wave, during which the upper 95% standard deviation threshold was breached multiple times. With an R-squared value of 0.2197, the linear trend better matched the data points compared to acute myocardial infarction. The weekly moving average of overall non-COVID-19-related ambulance deliveries are shown in
Figure 1C. The lower 95% standard deviation threshold was almost surpassed during the lockdown of the first COVID-19 wave, after which the weekly moving average of deliveries increased consistently. The peak occurred during the third wave, after which the deliveries did fall below the upper 95% standard deviation threshold. The R-squared value of the linear trend was 0.4008. Low degree of all the R-squared values for the weekly variations may have also played a role.
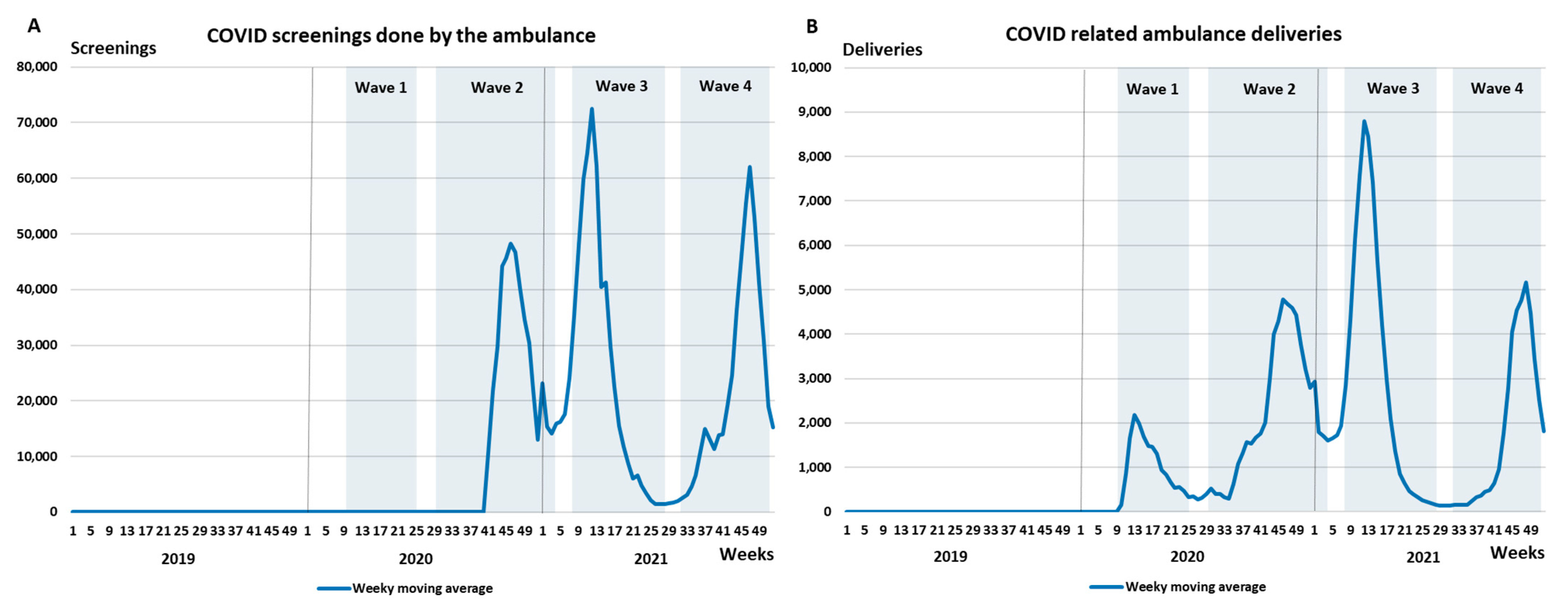
Figure 2A,B illustrate the weekly moving average of COVID-19 screenings and COVID-19-related ambulance deliveries, respectively. The intensity of these activities is consistent with the COVID-19 waves. In terms of acute myocardial infarction, the gender and age distribution did not change significantly over a three-year period (see
Supplementary Material Table S1). For haemorrhagic stroke, only the age distribution changed significantly (
p = 0.045) between 2019 and 2020, and for ischemic stroke a significant difference was observed with respect to age between 2019 and 2021 (
p = 0.016). After merging the two types of strokes, the significant difference persisted for age when comparing 2019 and 2020 data (
p = 0.015) and when comparing 2019 and 2021 data (
p = 0.006). For all non-COVID-19-related deliveries, the distribution for both gender and age was significant across all three years (
p < 0.05).
4. Discussion
In general, the rescue activities of the NAS showed a significant increase during the periods of the COVID-19 pandemic. Of the four pandemic waves that have taken place to date in Hungary, the third COVID-19 wave required the greatest effort from the NAS. AMI and stroke are primary issues from a public health point of view [
24,
25], so it is important for the healthcare system that the ambulance service prioritizes the organization and execution of such rescues [
13,
26]. A previous British study did not report increased STEMI and stroke rescue activity during the period of the COVID-19 epidemic, but only the effect of the first wave was analyzed in their study [
16]. This research result was also confirmed by our study, as during the first wave of COVID, we did not observe a significant increase in the rescue activity tasks, possibly because the additional rescue tasks caused by COVID-19 may have been offset by the reduced rescue burden as a consequence of the lockdown (e.g., reduced number of injuries from motor vehicle collisions and sports-related activities) [
27].
The NAS has several instruments at their disposal to perform at the highest possible level. One of the most often-used tools is business intelligence (BI). “BI is a technology-driven process for analyzing data and delivering actionable information that helps executives, managers and workers make informed business decisions” [
28]. In Hungary, with the help of this system, the management of the NAS is able to monitor—at a national level on a daily basis—whether the number of rescue units is sufficient to perform the tasks at hand. As other studies have demonstrated, the appropriate use of BI serve as an effective tool for decision makers, even during a pandemic [
29,
30,
31]. Therefore, it can be assumed that the NAS also benefited from using BI.
For healthcare providers around the world, in order to perform the extra tasks that arose during the COVID-19 pandemic in a professional and timely manner, additional human resources were needed. This brought about a change not only in the number of employees but also in their composition, in addition to the need to ensure that staff did not become infected [
32,
33,
34,
35]. For the NAS, this meant that medical and health science university students (e.g., physiotherapy and public health students) were also involved in the execution of tasks according to their knowledge and skills. Furthermore, a procedure for sampling required by general practitioners was established, for which the work of the Red Cross and volunteers was organized. Additionally, consultations were held several times a week with the institutions providing inpatient COVID-19 care with respect to the number of beds available.
A limitation of our study is that we were only able to define one year as a baseline before the onset of the COVID-19 pandemic. The number of haemorrhagic stroke cases appeared to be exiguous during our investigation because the ambulance service is not able to clearly separate cases of stroke, so the two types of strokes were combined in our analysis. However, the strength of our study is that we were able to examine 3 years of data provided directly by the domestic ambulance service. The authentic and professionally relevant data were ensured by the NAS and verified, with the help of BI, from the point of view of a medical professional. However, as the ambulance staff was responsible for the initial data recording, in cases of severe emergency there, was not enough time to enter all supplementary data, which might explain why approximately 10% of gender and approximately 1% of age data were not recorded. Finally, in the case of AMI and stroke, because the distribution did not differ significantly according to age and gender, we could rule out that the increase in the number of rescues was the result of a change in the composition of those who required ambulance delivery.
5. Conclusions
As a significant increase in ambulance deliveries was identified, the study results confirm that the emergence of a pandemic puts a heavy burden on emergency services, although the degree of variation may depend on the type of disease. The increase in activities coincided with the pandemic waves; however, our study does not provide an explanation of why the deliveries related to acute myocardial infarction and stroke responded differently. For example, a possible explanation for the fewer haemorrhagic stroke deliveries is that during the lockdown of the first wave, there were fever road accidents. However, without additional data, this cannot be confirmed or rejected. Thus, future studies should investigate this enigma. Furthermore, we recommend that future studies expand the timeframe and investigate how ambulance deliveries changed after the fourth wave of the COVID-19 pandemic, in addition to broadening the scope of the investigated diseases to determine which other types of deliveries are most affected by the pandemic. The aforementioned limitations must also be considered when interpreting the results of the present study, and future studies should address these limitations to provide more robust evidence. This can be achieved by including at least two years of baseline data for comparison and clearly separating the two types of strokes with diagnostic imaging.
Finally, emergency services must also prepare for the next global pandemic; to this end, it is important to rethink capacity organization and rescue activities. The Hungarian example highlights that in a pandemic situation, it can be beneficial to organize the emergency care of a country or a larger region under a single provider with a single decision-maker, and BI can provide assistance in monitoring critical indicators. Finally, we suggest that, similar to the NAS, the emergency services of various countries share their strategies by which they were able to cope with the increased burden during the pandemic.
Author Contributions
Conceptualization, K.B. (Klára Bíró), M.S.D., A.N. and V.D.; methodology, K.B. (Klára Bíró), M.S.D., A.N. and V.D.; formal analysis, K.B. (Klára Bíró), M.S.D., A.N. and V.D.; resources, G.P. and G.C.; data curation, G.P. and G.C.; writing—original draft preparation, K.B. (Klára Bíró), M.S.D., A.N. and V.D.; writing—review and editing, G.P., G.C., K.B. (Klára Boruzs), G.B. and G.T.S.; visualization, V.D.; supervision, K.B. (Klára Bíró) and G.C. All authors have read and agreed to the published version of the manuscript.
Funding
Project no. TKP2020-NKA-04 was implemented with support provided by the National Research, Development and Innovation Fund of Hungary, financed under the 2020-4.1.1-TKP2020 funding scheme.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Hungarian Scientific Research and Ethics Committee of the Medical Research Council (protocol code: ETT-TUKEB IV/5553-2/2020/EKU; date of approval: 30 June 2020).
Informed Consent Statement
Patient consent was waived due to the nature of the data provided by both the Hungarian Central Statistical Office and the Hungarian National Ambulance Service. Only aggregated data were provided; thus, the identification of individual cases is not possible.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available at the request of the board members of the Hungarian National Ambulance Service.
Conflicts of Interest
Gábor Csató (G.C.) and György Pápai (G.P.) are board members of the Hungarian National Ambulance Services. The other authors have no potential conflict of interest to declare.
References
- Riou, M.; Marcot, C.; Canuet, M.; Renaud-Picard, B.; Chatron, E.; Porzio, M.; Dégot, T.; Hirschi, S.; Metz-Favre, C.; Kassegne, L.; et al. Clinical Characteristics of and Outcomes for Patients with COVID-19 and Comorbid Lung Diseases Primarily Hospitalized in a Conventional Pulmonology Unit: A Retrospective Study. Respir. Med. Res. 2021, 79, 100801. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zeng, L.; Li, Z.; Mao, Q.; Liu, D.; Zhang, L.; Zhang, H.; Xie, Y.; Liu, G.; Gan, X.; et al. Emergency Trauma Care during the Outbreak of Corona Virus Disease 2019 (COVID-19) in China. World J. Emerg. Surg. 2020, 15, 33. [Google Scholar] [CrossRef] [PubMed]
- Wachira, B.W.; Mwai, M. A Baseline Review of the Ability of Hospitals in Kenya to Provide Emergency and Critical Care Services for COVID-19 Patients. Afr. J. Emerg. Med. 2021, 11, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Al-Wathinani, A.; Hertelendy, A.J.; Alhurishi, S.; Mobrad, A.; Alhazmi, R.; Altuwaijri, M.; Alanazi, M.; Alotaibi, R.; Goniewicz, K. Increased Emergency Calls during the COVID-19 Pandemic in Saudi Arabia: A National Retrospective Study. Healthcare 2020, 9, 14. [Google Scholar] [CrossRef]
- Prezant, D.J.; Lancet, E.A.; Zeig-Owens, R.; Lai, P.H.; Appel, D.; Webber, M.P.; Braun, J.; Hall, C.B.; Asaeda, G.; Kaufman, B.; et al. System Impacts of the COVID-19 Pandemic on New York City’s Emergency Medical Services. J. Am. Coll Emerg. Physicians Open 2020, 1, 1205–1213. [Google Scholar] [CrossRef]
- Al Amiry, A.; Maguire, B.J. Emergency Medical Services (EMS) Calls During COVID-19: Early Lessons Learned for Systems Planning (A Narrative Review). Open Access Emerg. Med. 2021, 13, 407–414. [Google Scholar] [CrossRef]
- Bilotta, C.; Zerbo, S.; Perrone, G.; Malta, G.; Argo, A. The medico-legal implications in medical malpractice claims during COVID-19 pandemic: Increase or trend reversal? Med. Leg J. 2020, 88, 35–37. [Google Scholar] [CrossRef]
- Kemenesi, G.; Zeghbib, S.; Somogyi, B.A.; Tóth, G.E.; Bányai, K.; Solymosi, N.; Szabo, P.M.; Szabó, I.; Bálint, Á.; Urbán, P.; et al. Multiple SARS-CoV-2 Introductions Shaped the Early Outbreak in Central Eastern Europe: Comparing Hungarian Data to a Worldwide Sequence Data-Matrix. Viruses 2020, 12, 1401. [Google Scholar] [CrossRef]
- Hungarian Government Official COVID-19 Information Site. The First Hungarian Patient Died. Available online: https://koronavirus.gov.hu/cikkek/meghalt-az-elso-magyar-beteg (accessed on 8 September 2022).
- Hungarian Government Official COVID-19 Information Site. The Number of Patients Infected with the New Coronavirus Has Increased to 58. Available online: https://koronavirus.gov.hu/cikkek/58-ra-nott-az-uj-koronavirussal-fertozott-betegek-szama (accessed on 8 September 2022).
- WHO COVID-19 Official Information Site. Available online: https://covid19.who.int/region/euro/country/hu (accessed on 8 September 2022).
- Hungarian Government Official Law Promulgation Site. Available online: https://net.jogtar.hu/jogszabaly?docid=A21K0223.EGK (accessed on 8 September 2022).
- Deák, M.S.; Csató, G.; Pápai, G.; Dombrádi, V.; Nagy, A.; Nagy, C.; Juhász, A.; Bíró, K. Investigating the Geographic Disparities of Amenable Mortality and Related Ambulance Services in Hungary. Int. J. Environ. Res. Public Health 2021, 18, 1065. [Google Scholar] [CrossRef]
- Jánosi, A.; Pach, F.P.; Erdős, G.; Csató, G.; Pápai, G.; Andréka, P. Incidence, Pre-Hospital Delay and Prognosis of Acute Myocardial Infarction in Big Regions of Hungary: Population Data from the Hungarian Myocardial Infarction Registry. Int. J. Clin. Pract. 2021, 75, e14831. [Google Scholar] [CrossRef]
- OECD Official Health Data Site. Available online: https://data.oecd.org/healthstat/potential-years-of-life-lost.htm#indicator-chart (accessed on 8 September 2022).
- Holmes, J.L.; Brake, S.; Docherty, M.; Lilford, R.; Watson, S. Emergency Ambulance Services for Heart Attack and Stroke during UK’s COVID-19 Lockdown. Lancet 2020, 395, e93–e94. [Google Scholar] [CrossRef]
- Bell, F.; Pilbery, R.; Connell, R.; Fletcher, D.; Leatherland, T.; Cottrell, L.; Webster, P. The Acceptability and Safety of Video Triage for Ambulance Service Patients and Clinicians during the COVID-19 Pandemic. Br. Paramed. J. 2021, 6, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Vinci, A.; Pasquarella, A.; Corradi, M.P.; Chatzichristou, P.; D’Agostino, G.; Iannazzo, S.; Trani, N.; Parafati, M.A.; Palombi, L.; Ientile, D.A. Emergency Medical Services Calls Analysis for Trend Prediction during Epidemic Outbreaks: Interrupted Time Series Analysis on 2020–2021 COVID-19 Epidemic in Lazio, Italy. Int. J. Environ. Res. Public Health 2022, 19, 5951. [Google Scholar] [CrossRef]
- Masterson, S.; Heffernan, E.; Keegan, D.; Clarke, B.; Deasy, C.; O’Donnell, C.; Crowley, P.; Breen, R.; Kelly, M.E.; Murphy, A.W. Rapid Response and Learning for Later: Establishing High Quality Information Networks and Evaluation Frameworks for the National Ambulance Service Response to COVID-19—The ENCORE COVID Project Protocol. HRB Open Res. 2020, 3, 68. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, D.; Duncan, E.A.S.; Moore, M.; Best, C.; Andreis, F.; Esposito, M.; Dobbie, R.; Corfield, A.R.; Lowe, D.J. Epidemiology of Emergency Ambulance Service Calls Related to COVID-19 in Scotland: A National Record Linkage Study. Scand. J. Trauma Resusc. Emerg. Med. 2022, 30, 9. [Google Scholar] [CrossRef]
- Ayala, A.; Villalobos Dintrans, P.; Elorrieta, F.; Castillo, C.; Vargas, C.; Maddaleno, M. Identification of COVID-19 Waves: Considerations for Research and Policy. Int. J. Environ. Res. Public Health 2021, 18, 11058. [Google Scholar] [CrossRef]
- Zhang, S.X.; Arroyo Marioli, F.; Gao, R.; Wang, S. A Second Wave? What Do People Mean by COVID Waves—A Working Definition of Epidemic Waves. Risk Manag. Health Policy 2021, 14, 3775–3782. [Google Scholar] [CrossRef]
- Coronavirus Pandemic (COVID-19) Information Site. Available online: https://ourworldindata.org/coronavirus (accessed on 8 September 2022).
- Jánosi, A.; Ferenci, T.; Tomcsányi, J.; Andréka, P. Out-of-Hospital Cardiac Arrest in Patients Treated for ST-Elevation Acute Myocardial Infarction: Incidence, Clinical Features, and Prognosis Based on Population-Level Data from Hungary. Resusc. Plus 2021, 6, 100113. [Google Scholar] [CrossRef]
- Égi, C.; Horváth, J.; Hahn, K.; Kalman, B.; Betlehem, J.; Nagy, L. Improving Outcomes Achieved by a New Stroke Program in Hungary. Cereb. Dis. Extra 2015, 5, 132–138. [Google Scholar] [CrossRef]
- Ong, J.; O’Connell, F.; Mazer-Amirshahi, M.; Pourmand, A. An international perspective of out-of-hospital cardiac arrest and cardiopulmonary resuscitation during the COVID-19 pandemic. Am. J. Emerg. Med. 2021, 47, 192–197. [Google Scholar] [CrossRef]
- Keays, G.; Friedman, D.; Gagnon, I. Injuries in the Time of COVID-19. Health Promot. Chronic Dis. Prev. Can. 2020, 40, 336–341. [Google Scholar] [CrossRef] [PubMed]
- TechTarget. Business Intelligence (BI). Available online: https://www.techtarget.com/searchbusinessanalytics/definition/business-intelligence-BI (accessed on 19 September 2022).
- Davy, A.; Borycki, E.M. Business Intelligence Dashboards for Patient Safety and Quality: A Narrative Literature Review. Stud. Health Technol. Inf. 2022, 290, 438–441. [Google Scholar] [CrossRef]
- Escher, A.; Hainc, N.; Boll, D. Business Intelligence in Hospital Management. Radiol. Manag. 2016, 38, 47–52. [Google Scholar]
- Sechi, G.M.; Migliori, M.; Dassi, G.; Pagliosa, A.; Bonora, R.; Oradini-Alacreu, A.; Odone, A.; Signorelli, C.; Zoli, A.; AREU COVID-19 Response Team. Business Intelligence Applied to Emergency Medical Services in the Lombardy Region during SARS-CoV-2 Epidemic. Acta Biomed. 2020, 91, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Yusefi, A.R.; Sharifi, M.; Nasabi, N.S.; Rezabeigi Davarani, E.; Bastani, P. Health Human Resources Challenges during COVID-19 Pandemic; Evidence of a Qualitative Study in a Developing Country. PLoS ONE 2022, 17, e0262887. [Google Scholar] [CrossRef]
- Mohammadi, F.; Tehranineshat, B.; Bijani, M.; Khaleghi, A.A. Management of COVID-19-Related Challenges Faced by EMS Personnel: A Qualitative Study. BMC Emerg. Med. 2021, 21, 95. [Google Scholar] [CrossRef]
- Turner, S.; Niño, N.; Segura, C.; Botero-Tovar, N. Organisational Responses to Mitigate the Effects of COVID-19 on Healthcare Workers: A Qualitative Case Study from Bogotá, Colombia. BMC Health Serv. Res. 2021, 21, 792. [Google Scholar] [CrossRef]
- Cirrincione, L.; Plescia, F.; Ledda, C.; Rapisarda, V.; Martorana, D.; Lacca, G.; Argo, A.; Zerbo, S.; Vitale, E.; Vinnikov, D.; et al. COVID-19 Pandemic: New Prevention and Protection Measures. Sustainability 2022, 14, 4766. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 


{kind=link}
{kind=link}