
Association between Antihypertensive Therapy and Risk of Acute Lower Respiratory Infections (ALRI): A Retrospective Cohort Study
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Database
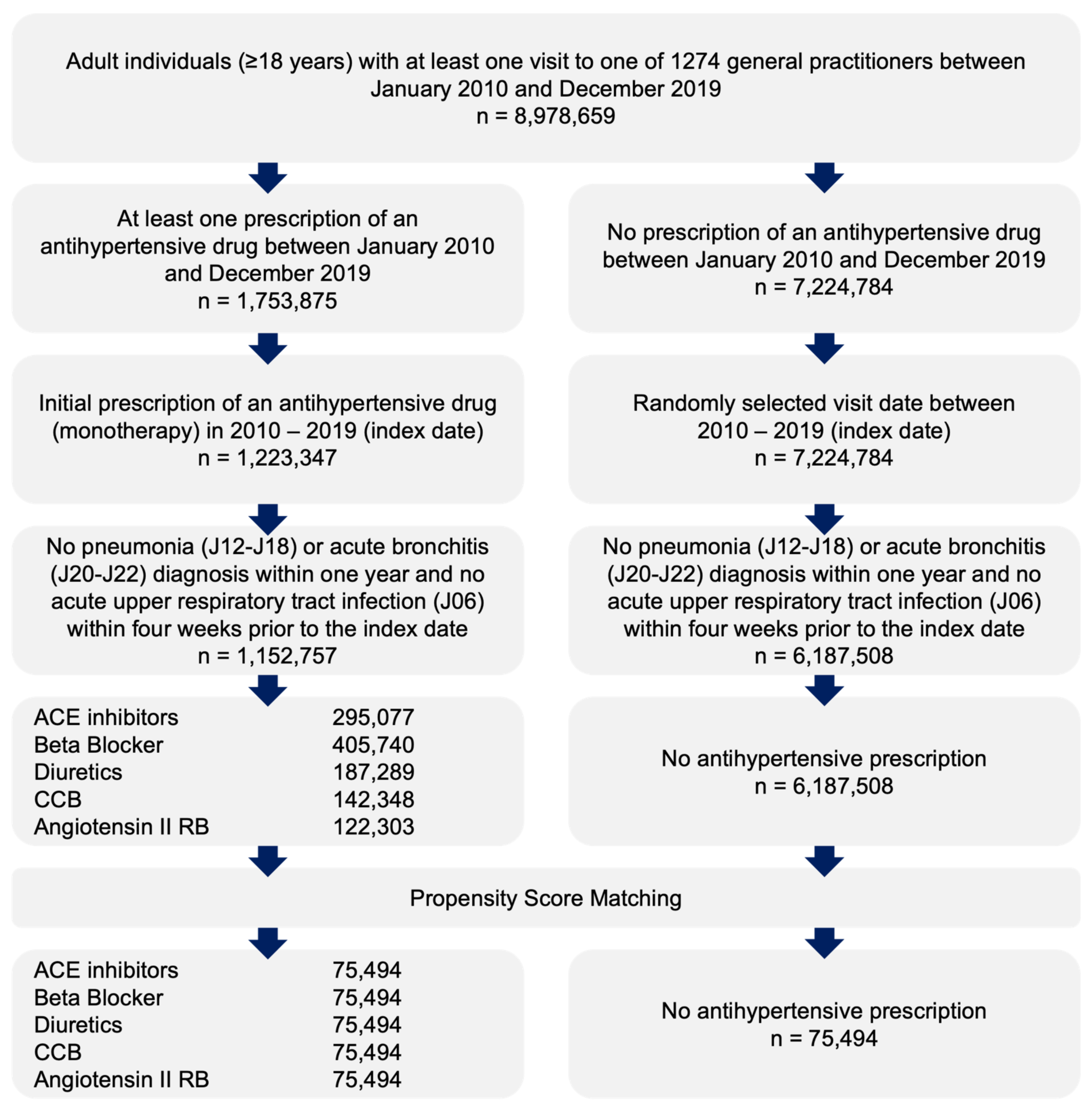
2.2. Study Population
2.3. Study Outcomes and Covariates
2.4. Statistical Analyses
2.5. Ethical Statement
3. Results
3.1. Basic Characteristics of the Study Sample
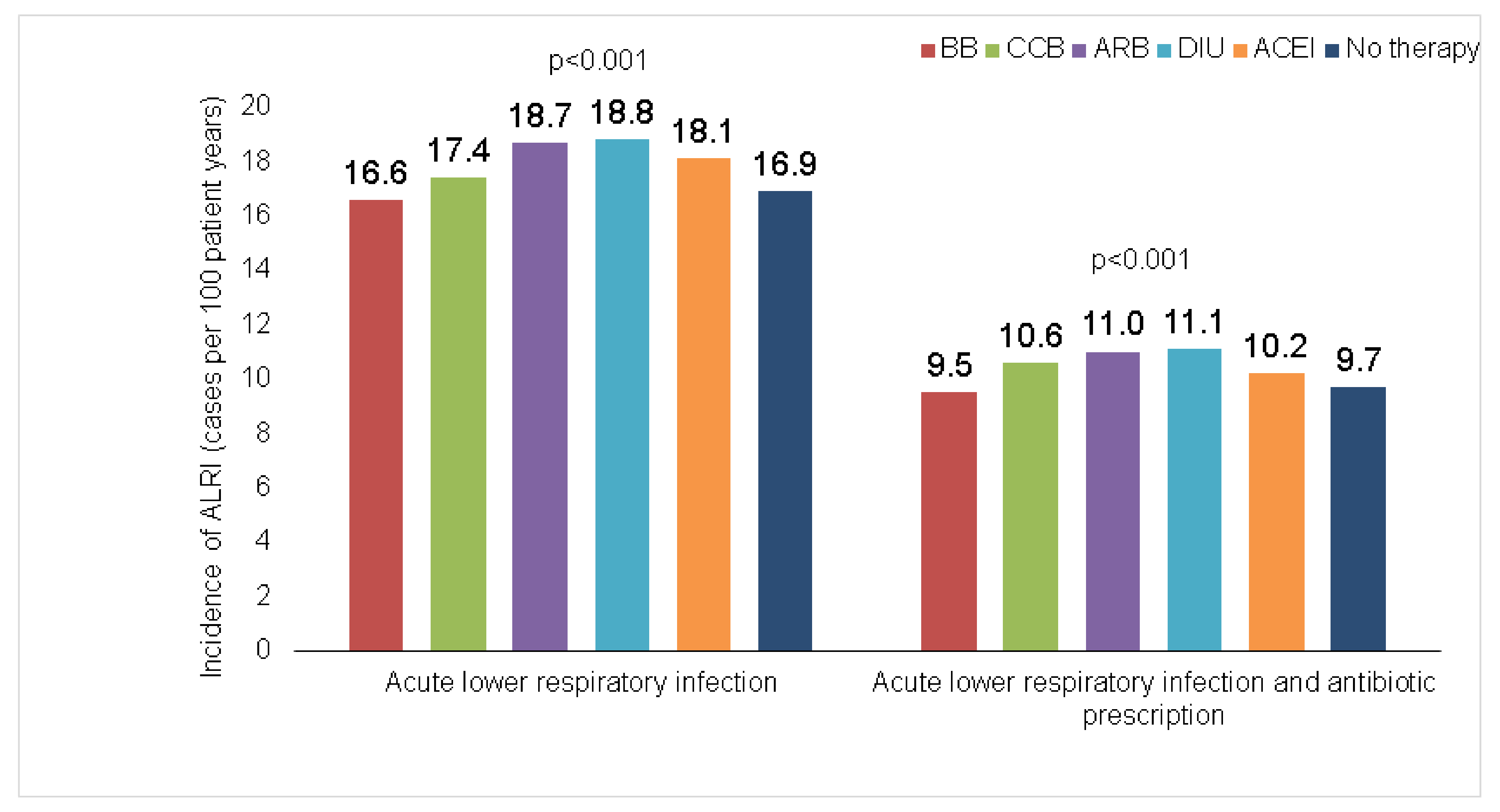
3.2. Cumulative Incidence of ALRI Diagnoses
3.3. Association between Antihypertensive Therapy and Incidence of ALRI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Egan, B.M.; Kjeldsen, S.E.; Grassi, G.; Esler, M.; Mancia, G. The global burden of hypertension exceeds 1.4 billion people. J. Hypertens. 2019, 37, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Salem, H.; Hasan, D.M.; Eameash, A.; El-Mageed, H.A.; Hasan, S.; Ali, R. Worldwide Prevalence of Hypertension: A Pooled Meta-Analysis of 1670 Studies In 71 Countries with 29.5 Million Participants. J. Am. Coll. Cardiol. 2018, 71, A1819. [Google Scholar] [CrossRef]
- Khalil, H.; Zeltser, R. Antihypertensive Medications; StatPearls Publishing LLC: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Jackson, R.E.; Bellamy, M.C. Antihypertensive drugs. Contin. Educ. Anaesth. Crit. Care Pain 2015, 15, 280–285. [Google Scholar] [CrossRef] [Green Version]
- Sarganas, G.; Knopf, H.; Grams, D.; Neuhauser, H.K. Trends in Antihypertensive Medication Use and Blood Pressure Control Among Adults with Hypertension in Germany. Am. J. Hypertens 2016, 29, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Vangen-Lønne, A.M.; Wilsgaard, T.; Johnsen, S.H.; Løchen, M.L.; Njølstad, I.; Mathiesen, E.B. Declining Incidence of Ischemic Stroke: What Is the Impact of Changing Risk Factors? The Tromsø Study 1995 to 2012. Stroke 2017, 48, 544–550. [Google Scholar] [CrossRef]
- Pore, P.; Ghattargi, C.H.; Rayate, M.R. Study of Risk Factors of Acute Respiratory Infection (ARI) in Underfives in Solapur. Natl. J. Community Med. 2010, 1, 64–67. [Google Scholar]
- Avendaño Carvajal, L.; Perret Pérez, C. Epidemiology of Respiratory Infections. In Pediatric Respiratory Diseases; Springer: Cham, Switzerland, 2020; pp. 263–272. [Google Scholar] [CrossRef] [Green Version]
- Sekizawa, K.; Matsui, T.; Nakagawa, T.; Nakayama, K.; Sasaki, H. ACE inhibitors and pneumonia. Lancet 1998, 352, 1069. [Google Scholar] [CrossRef]
- Van de Garde, E.M.W.; Souverein, P.C.; Hak, E.; Deneer, V.H.M.; van den Bosch, J.M.M.; Leufkens, H.G.M. Angiotensin-converting enzyme inhibitor use and protection against pneumonia in patients with diabetes. J. Hypertens 2007, 25, 235–239. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.C.; Wang, Y.H.; Wang, C.Y.; Wang, H.C.; Yu, C.J.; Chen, L. Comparative effects of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on the risk of pneumonia and severe exacerbations in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 867. [Google Scholar] [CrossRef]
- Mukamal, K.J.; Ghimire, S.; Pandey, R.; O’Meara, E.S.; Gautam, S. Antihypertensive medications and risk of community-acquired pneumonia. J. Hypertens. 2010, 28, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Westendorp, W.F.; Vermeij, J.D.; Brouwer, M.C.; Roos, Y.B.W.E.M.; Nederkoorn, P.J.; van de Beek, D. Pre-Stroke Use of Beta-Blockers Does Not Lower Post-Stroke Infection Rate: An Exploratory Analysis of the Preventive Antibiotics in Stroke Study. Cerebrovasc. Dis. 2016, 42, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Maier, I.L.; Becker, J.C.; Leyhe, J.R.; Schnieder, M.; Behme, D.; Psychogios, M.N.; Liman, J. Influence of beta-blocker therapy on the risk of infections and death in patients at high risk for stroke induced immunodepression. PLoS ONE 2018, 13, e0196174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic characteristics and representativeness of the German Disease Analyzer database. Int. J. Clin. Pharm. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Jacob, L.; Kostev, K. Persistence with antihypertensive drugs in patients with depression in Germany. Int. J. Clin. Pharmacol. Ther. 2018, 56, 162–168. [Google Scholar] [CrossRef]
- Warda, A.; Reese, J.P.; Tanislav, C.; Kostev, K. The association between antihypertensive therapy and the incidence of Parkinson’s disease in patients followed in general practices in Germany. Int. J. Clin. Pharmacol. Ther. 2019, 57, 483–488. [Google Scholar] [CrossRef]
- Tanislav, C.; Kostev, K. Investigation of the prevalence of non-COVID-19 infectious diseases during the COVID-19 pandemic. Public Health 2022, 203, 53–57. [Google Scholar] [CrossRef]
- Kern, W.V.; Kostev, K. Prevalence of and Factors Associated with Antibiotic Prescriptions in Patients with Acute Lower and Upper Respiratory Tract Infections—A Case-Control Study. Antibiotics 2021, 10, 455. [Google Scholar] [CrossRef]
- Kikuchi, R.; Watabe, N.; Konno, T.; Mishina, N.; Sekizawa, K.; Sasaki, H. High incidence of silent aspiration in elderly patients with community-acquired pneumonia. Am. J. Respir. Crit. Care Med. 1994, 150, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Arai, T.; Yoshimi, N.; Fujiwara, H.; Sekizawa, K. Serum substance P concentrations and silent aspiration in elderly patients with stroke. Neurology 2003, 61, 1625–1626. [Google Scholar] [CrossRef]
- Van de Garde, E.M.W.; Souverein, P.C.; van den Bosch, J.M.M.; Deneer, V.H.M.; Leufkens, H.G.M. Angiotensin-converting enzyme inhibitor use and pneumonia risk in a general population. Eur. Respir. J. 2006, 27, 1217–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.Y.; Chang, S.S.; Lin, C.L.; Lin, C.C.; Hsu, W.H.; Chou, C.H.; Chi, C.Y.; Lin, C.D.; Tu, C.Y.; Hsu, C.Y.; et al. Association between angiotensin-converting enzyme inhibitors or angiotensin receptor blockers and community-acquired pneumonia: A nationwide population propensity-score matching study. Int. J. Clin. Pract. 2021, 75, e14476. [Google Scholar] [CrossRef] [PubMed]
- Caldeira, D.; Alarcão, J.; Vaz-Carneiro, A.; Costa, J. Risk of pneumonia associated with use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers: Systematic review and meta-analysis. BMJ 2012, 345, e4260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.L.; Shau, W.Y.; Wu, C.S.; Lai, M.S. Angiotensin-converting enzyme inhibitor/angiotensin II receptor blockers and pneumonia risk among stroke patients. J. Hypertens. 2012, 30, 2223–2229. [Google Scholar] [CrossRef]
- Ohkubo, T.; Chapman, N.; Neal, B.; Woodward, M.; Omae, T.; Chalmers, J. Effects of an Angiotensin-converting Enzyme Inhibitor-based Regimen on Pneumonia Risk. Am. J. Respir. Crit. Care Med. 2012, 169, 1041–1045. [Google Scholar] [CrossRef]
- Dublin, S.; Walker, R.L.; Jackson, M.L.; Nelson, J.C.; Weiss, N.S.; Jackson, L.A. Angiotensin-converting enzyme inhibitor use and pneumonia risk in community-dwelling older adults: Results from a population-based case-control study. Pharm. Drug Saf. 2012, 21, 1173. [Google Scholar] [CrossRef] [Green Version]
- Cao, D.Y.; Giani, J.F.; Veiras, L.C.; Bernstein, E.A.; Okwan-Duodu, D.; Ahmed, F.; Bresee, C.; Tourtellotte, W.G.; Karumanchi, S.A.; Bernstein, K.E.; et al. An ACE inhibitor reduces bactericidal activity of human neutrophils in vitro and impairs mouse neutrophil activity in vivo. Sci. Transl. Med. 2021, 13, eabj2138. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.K.; Heo, E.Y.; Chung, H.S.; Kim, D.K. The association of renin-angiotensin system blockades and pneumonia requiring admission in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2159. [Google Scholar] [CrossRef]
- Liu, C.L.; Shau, W.Y.; Chang, C.H.; Wu, C.S.; Lai, M.S. Pneumonia risk and use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers. J. Epidemiol. 2013, 23, 344–350. [Google Scholar] [CrossRef] [Green Version]
- Henry, C.; Zaizafoun, M.; Stock, E.; Ghamande, S.; Arroliga, A.C.; White, H.D. Impact of angiotensin-converting enzyme inhibitors and statins on viral pneumonia. Bayl. Univ. Med. Cent. Proc. 2018, 31, 419–423. [Google Scholar] [CrossRef]
- Arai, T.; Sekizawa, K.; Ohrui, T.; Fujiwara, H.; Yoshimi, N.; Matsuoka, H.; Sasaki, H. ACE inhibitors and protection against pneumonia in elderly patients with stroke. Neurology 2005, 64, 573–574. [Google Scholar] [CrossRef] [PubMed]
- Nanni, G.; Panocchia, N.; Tacchino, R.; Foco, M.; Piccioni, E.; Castagneto, M. Increased incidence of infection in verapamil-treated kidney transplant recipients. Transpl. Proc. 2000, 32, 551–553. [Google Scholar] [CrossRef]
- Zheng, L.; Hunter, K.; Gaughan, J.; Poddar, S. Preadmission Use of Calcium Channel Blockers and Outcomes After Hospitalization with Pneumonia: A Retrospective Propensity-Matched Cohort Study. Am. J. Ther. 2017, 24, e30–e38. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Proportion Affected among Patients Treated with ACE Inhibitors (%) | Proportion Affected among Patients Treated with Beta Blockers (%) | Proportion Affected among Patients Treated with Diuretics (%) | Proportion Affected among Patients Treated with CCB (%) | Proportion Affected among Patients Treated with ARB (%) | p-Value |
|---|---|---|---|---|---|---|
| N | 75,494 | 75,494 | 75,494 | 75,494 | 75,494 | |
| Age (Mean, SD) | 65.3 (14.0) | 65.3 (14.0) | 65.3 (14.0) | 65.3 (14.0) | 65.3 (14.0) | 1.000 |
| Age ≤ 60 | 36.2 | 36.2 | 36.2 | 36.2 | 36.2 | 1.000 |
| Age 61–70 | 23.3 | 23.3 | 23.3 | 23.3 | 23.3 | |
| Age 71–80 | 26.4 | 26.4 | 26.4 | 26.4 | 26.4 | |
| Age > 80 | 14.1 | 14.1 | 14.1 | 14.1 | 14.1 | |
| Female | 56.9 | 56.9 | 56.9 | 56.9 | 56.9 | 1.000 |
| Male | 43.1 | 43.1 | 43.1 | 43.1 | 43.1 | |
| Diabetes | 13.2 | 13.2 | 13.2 | 13.2 | 13.2 | 1.000 |
| Ischemic heart diseases | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 | 1.000 |
| Heart failure | 1.7 | 1.7 | 1.7 | 1.7 | 1.7 | 1.000 |
| Renal failure | 2.0 | 2.0 | 2.0 | 2.0 | 2.0 | 1.000 |
| COPD | 3.7 | 3.7 | 3.7 | 3.7 | 3.7 | 1.000 |
| Asthma | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | 1.000 |
| Cohort | BB versus Rest | CCB versus Rest | ARB versus Rest | DIU versus Rest | ACEI versus Rest |
|---|---|---|---|---|---|
| Total | |||||
| Diagnosis | 0.96 (0.93–0.99) | 0.93 (0.90–0.96) | 1.08 (1.05–1.12) | 1.02 (0.99–1.05) | 1.02 (0.98–1.05) |
| Diagnosis + antibiotic prescription | 0.95 (0.90–0.99) | 0.96 (0.92–1.00) | 1.09 (1.94–1.13) | 1.03 (0.99–1.07) | 0.99 (0.94–1.03) |
| Age ≤ 60 | |||||
| Diagnosis | 0.96 (0.91–1.02) | 0.89 (0.85–0.95) | 1.08 (1.03–1.14) | 0.96 (0.91–1.02) | 1.11 (1.05–1.17) |
| Diagnosis + antibiotic prescription | 0.96 (0.89–1.03) | 0.90 (0.84–0.96) | 1.10 (1.03–1.17) | 1.00 (0.94–1.07) | 1.06 (0.99–1.13) |
| Age 61–70 | |||||
| Diagnosis | 1.01 (0.94–1.09) | 0.97 (0.90–1.04) | 1.06 (0.99–1.14) | 0.94 (0.87–1.029 | 1.02 (0.95–1.10) |
| Diagnosis + antibiotic prescription | 0.96 (0.87–1.06) | 0.99 (0.90–1.09) | 1.04 (0.95–1.14) | 1.01 (0.91–1.10) | 1.01 (0.92–1.11) |
| Age 71–80 | |||||
| Diagnosis | 0.95 (0.89–1.03) | 0.93 (0.87–1.00) | 1.12 (1.05–1.20) | 1.06 (0.99–1.13) | 0.94 (0.88–1.01) |
| Diagnosis + antibiotic prescription | 0.98 (0.89–1.08) | 0.96 (0.87–1.05) | 1.14 (1.04–1.24) | 1.01 (0.93–1.11) | 0.93 (0.81–0.99) |
| Age > 80 | |||||
| Diagnosis | 0.92 (0.83–1.00) | 0.94 (0.85–1.03) | 1.08 (0.98–1.18) | 1.10 (1.00–1.20) | 0.99 (0.90–1.08) |
| Diagnosis + antibiotic prescription | 0.88 (0.77–1.00) | 1.09 (0.96–1.24) | 1.08 (0.95–1.24) | 1.02 (0.90–1.15) | 0.95 (0.84–1.08) |
| Women | |||||
| Diagnosis | 0.96 (0.92–1.00) | 0.91 (0.87–0.95) | 1.06 (1.02–1.11) | 1.05 (1.01–1.10) | 1.02 (0.98–1.06) |
| Diagnosis + antibiotic prescription | 0.96 (0.91–1.02) | 0.94 (0.89–1.00) | 1.05 (0.99–1.11) | 1.08 (1.02–1.14) | 0.97 (0.91–1.02) |
| Men | |||||
| Diagnosis | 0.95 (0.91–1.00) | 0.94 (0.89–0.99) | 1.12 (1.06–1.18) | 0.98 (0.93–1.04) | 1.02 (0.97–1.08) |
| Diagnosis + antibiotic prescription | 0.91 (0.85–0.98) | 0.96 (0.90–1.03) | 1.14 (1.07–1.23) | 0.97 (0.90–1.04) | 1.02 (0.95–1.10) |
| Cohort | BB versus No Therapy | CCB versus No Therapy | ARB versus No Therapy | DIU versus No Therapy | ACEI versus No Therapy |
|---|---|---|---|---|---|
| Total | |||||
| Diagnosis | 0.95 (0.91–1.00) | 0.98 (0.93–1.00) | 1.10 (1.05–1.15) | 1.06 (1.01–1.11) | 1.05 (1.00–1.10) |
| Diagnosis + antibiotic prescription | 0.95 (0.89–1.01) | 1.03 (0.97–1.10) | 1.12 (1.05–1.19) | 1.08 (1.02–1.15) | 1.02 (0.96–1.09) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heidemann, J.; Konrad, M.; Roderburg, C.; Loosen, S.H.; Kostev, K. Association between Antihypertensive Therapy and Risk of Acute Lower Respiratory Infections (ALRI): A Retrospective Cohort Study. Healthcare 2022, 10, 2318. https://doi.org/10.3390/healthcare10112318
Heidemann J, Konrad M, Roderburg C, Loosen SH, Kostev K. Association between Antihypertensive Therapy and Risk of Acute Lower Respiratory Infections (ALRI): A Retrospective Cohort Study. Healthcare. 2022; 10(11):2318. https://doi.org/10.3390/healthcare10112318
Chicago/Turabian StyleHeidemann, Jana, Marcel Konrad, Christoph Roderburg, Sven H. Loosen, and Karel Kostev. 2022. "Association between Antihypertensive Therapy and Risk of Acute Lower Respiratory Infections (ALRI): A Retrospective Cohort Study" Healthcare 10, no. 11: 2318. https://doi.org/10.3390/healthcare10112318