
Population Based Average Parotid Gland Volume and Prevalence of Incidental Tumors in T1-MRI
 , , , , , and
, , , , , and
Abstract
:1. Introduction
1.1. Anatomy and Imaging of the Parotid Gland
1.2. Study of Health in Pomerania: An Epidemiological Cohort Employing MRI Scans
2. Materials and Methods
2.1. Cohort and Selected Modalities of the Study of Health in Pommerania
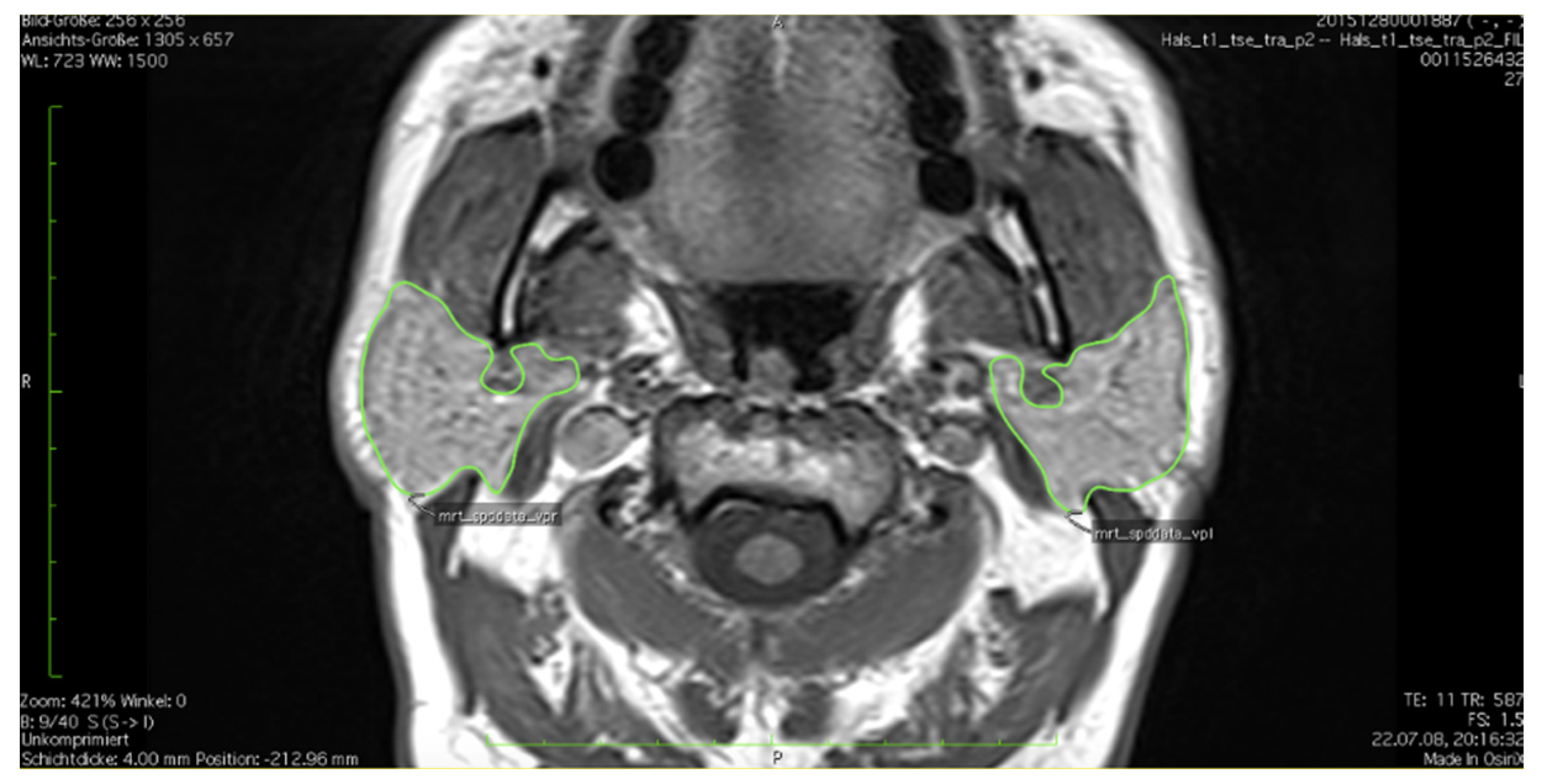
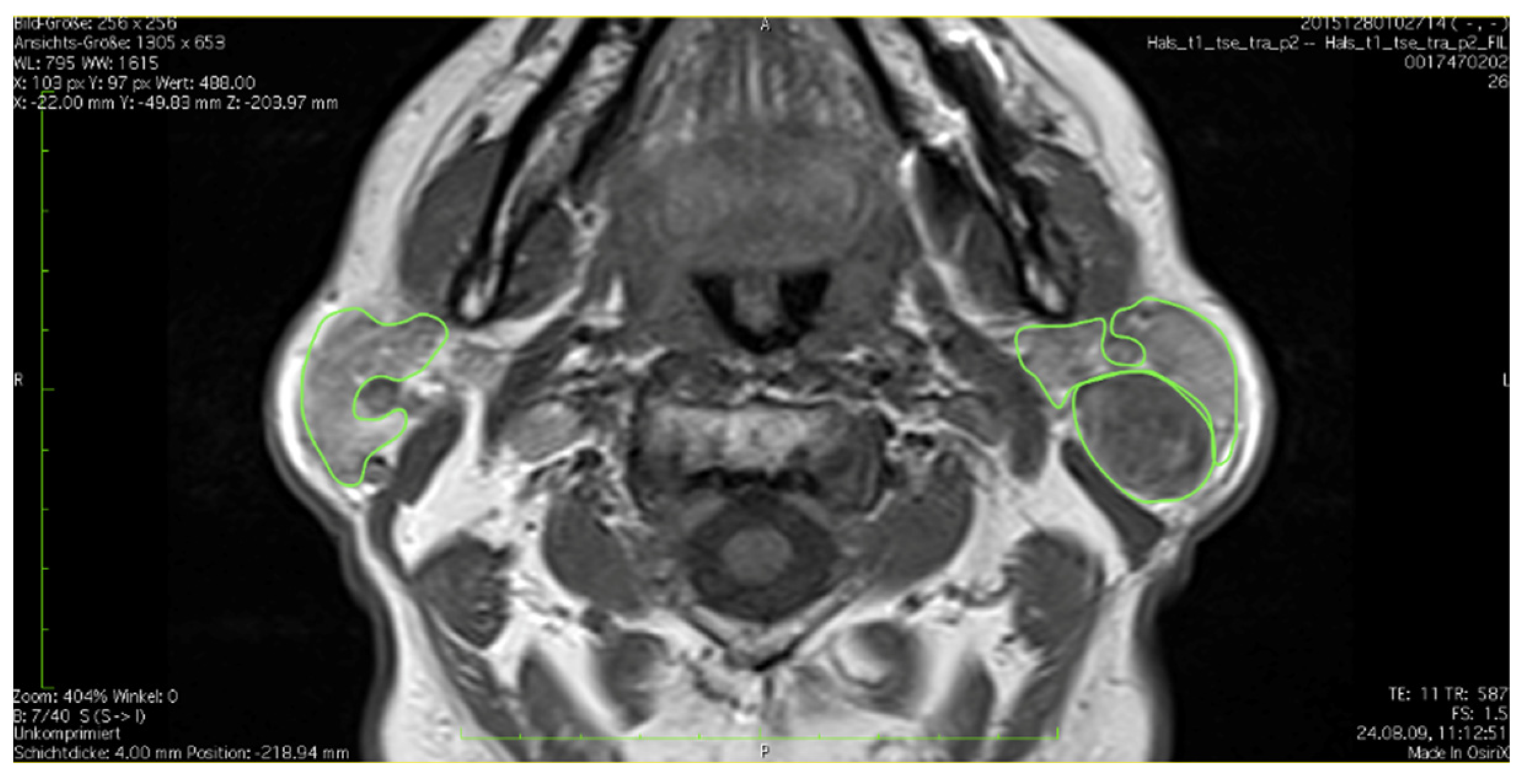
2.2. Standard Operating Procedure
2.3. Statistic Tools
3. Results
3.1. Analysis of Cohort
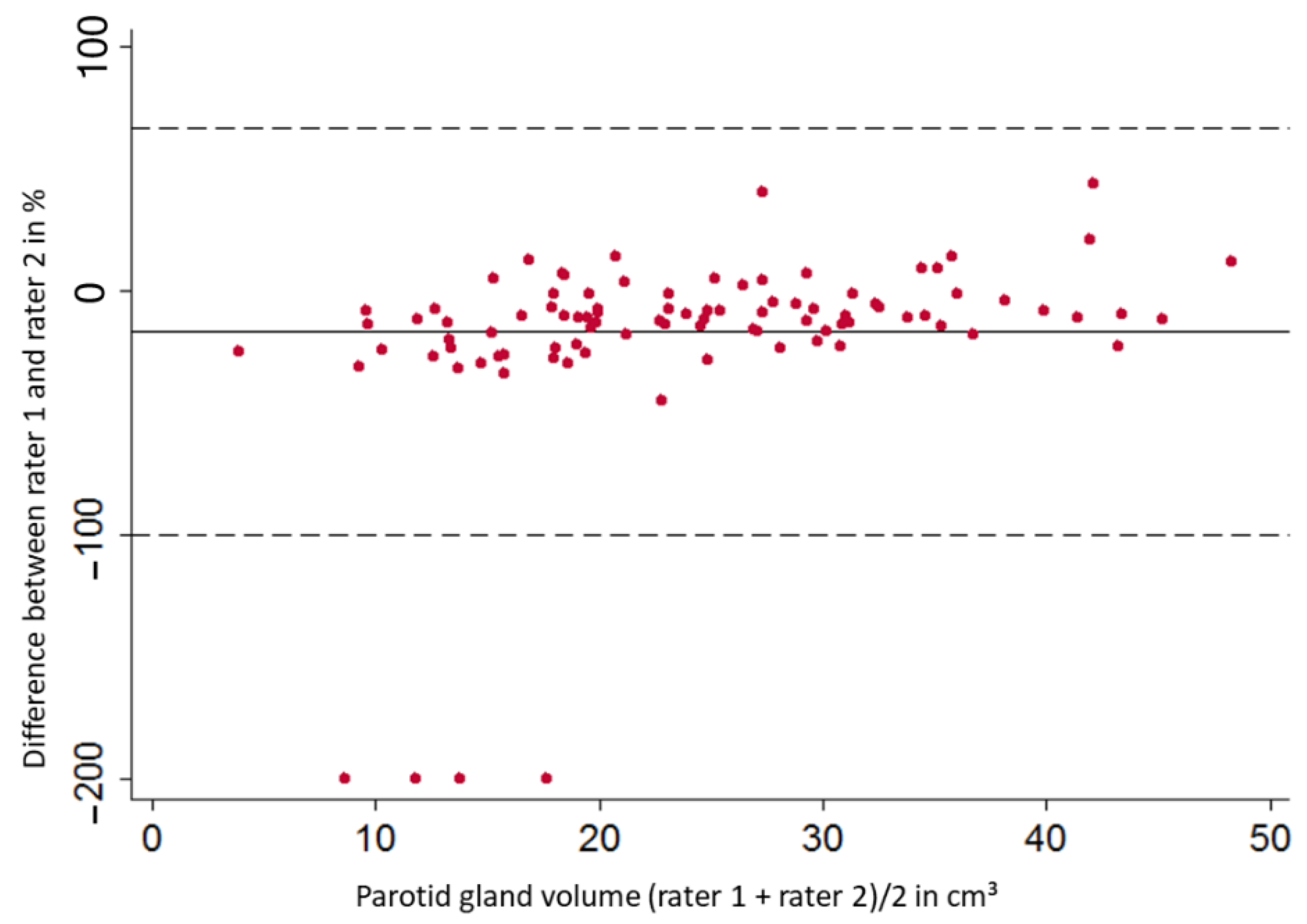
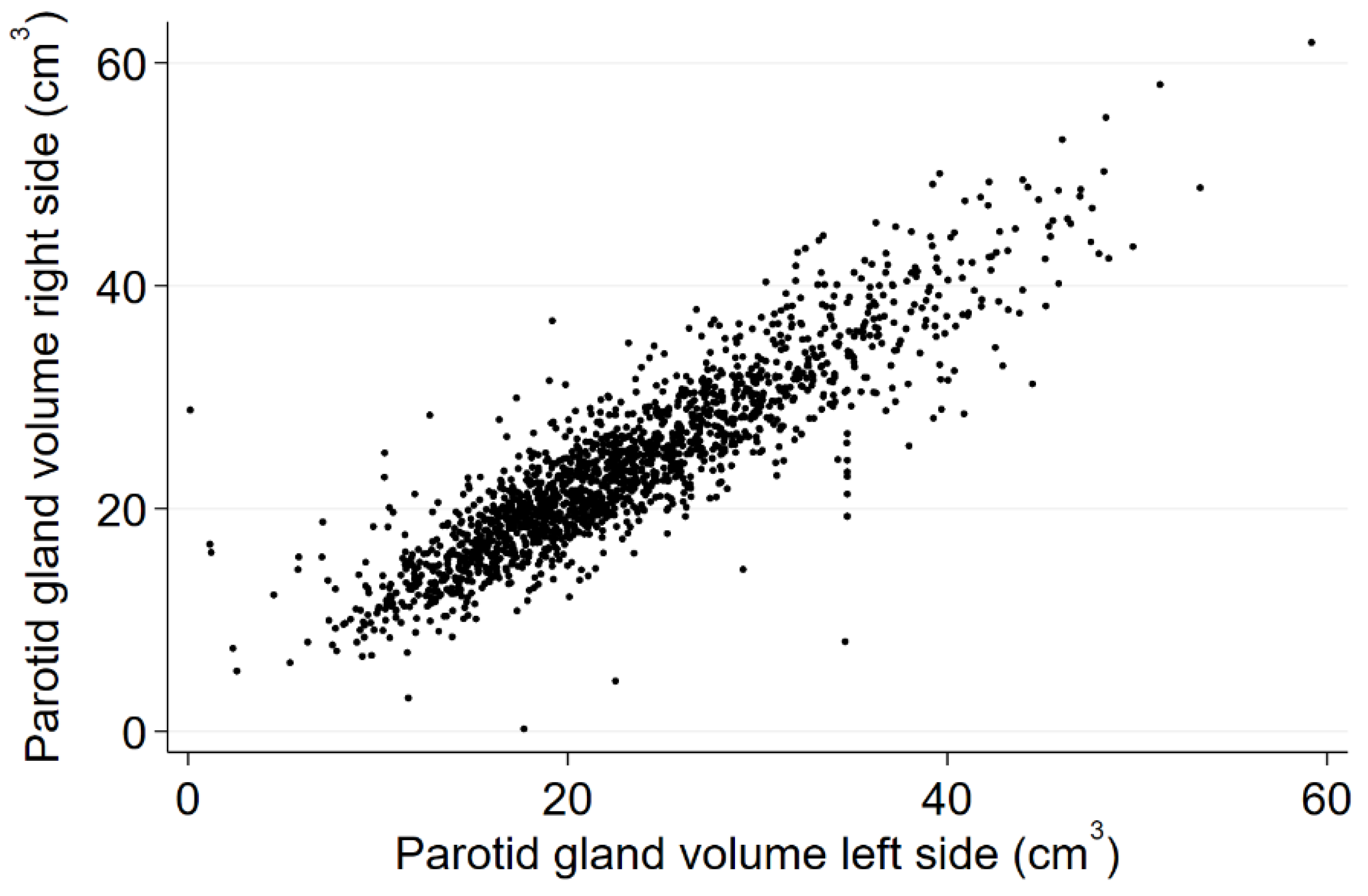
3.2. Analysis of Methods
3.3. Volume of the Parotid Gland and Association to Sex, Age, BMI and Selected Comorbidities
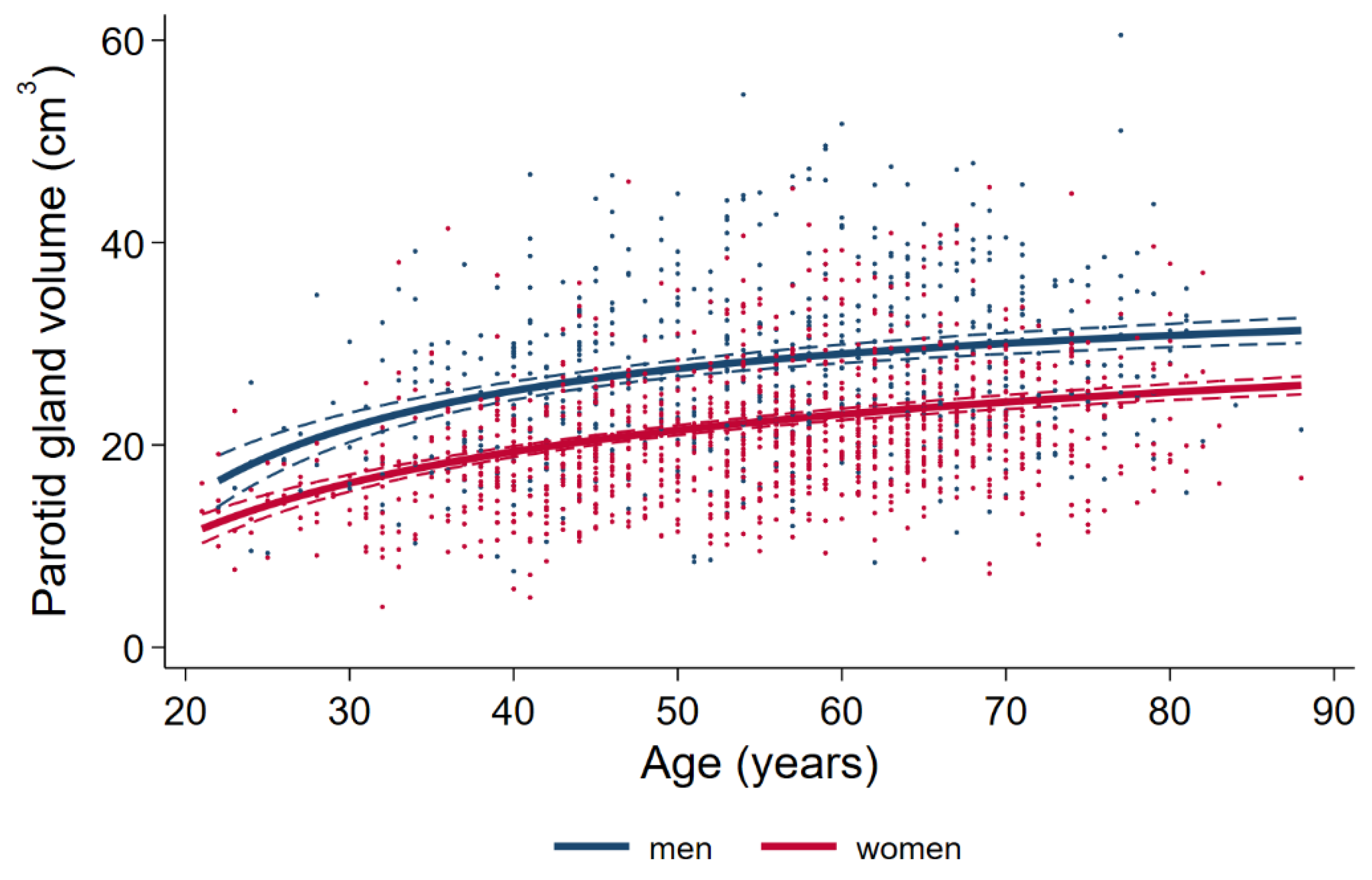
3.3.1. Associations of Sex and Age with Parotid Volume
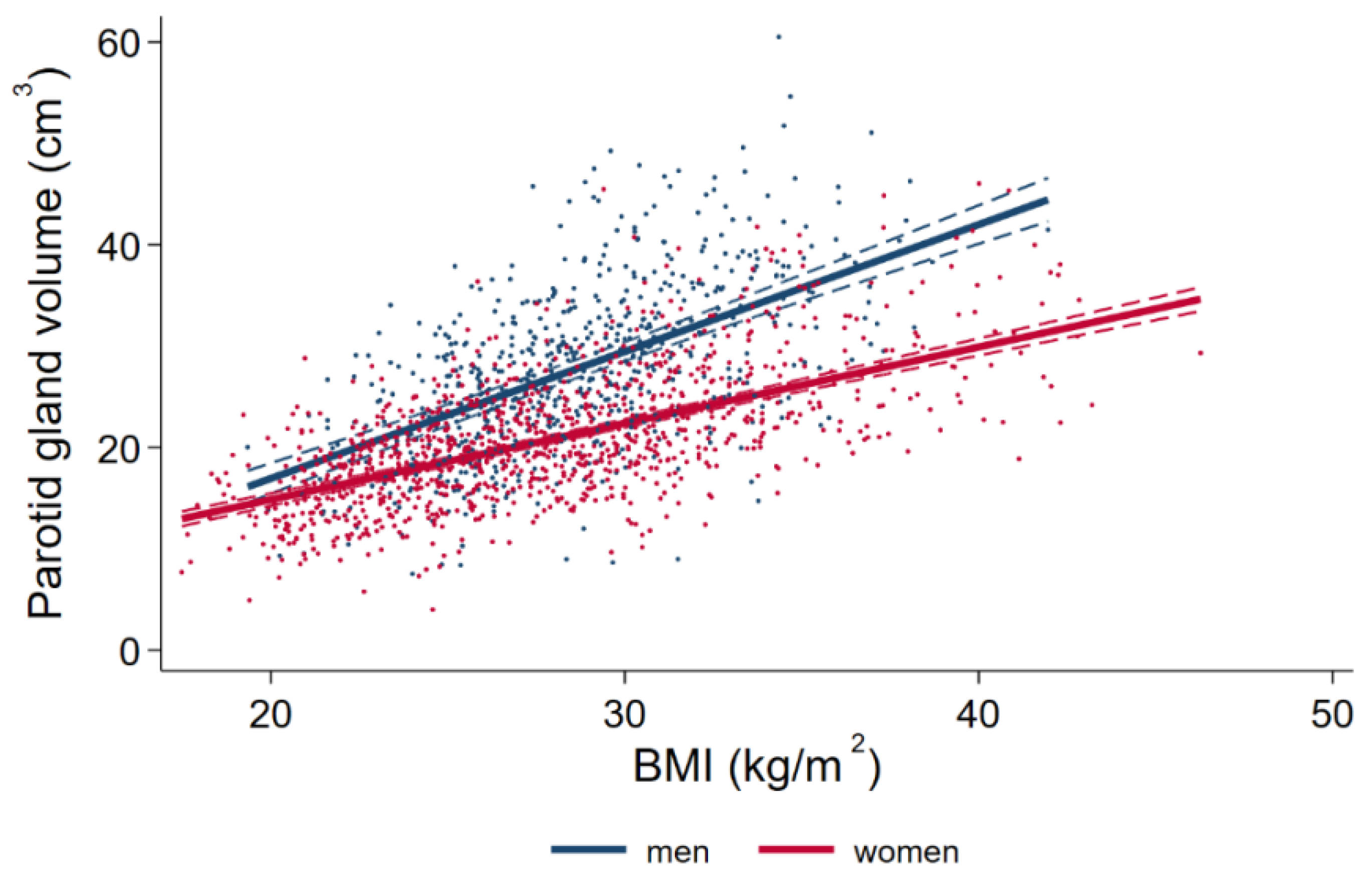
3.3.2. Associations of BMI with Parotid Volume
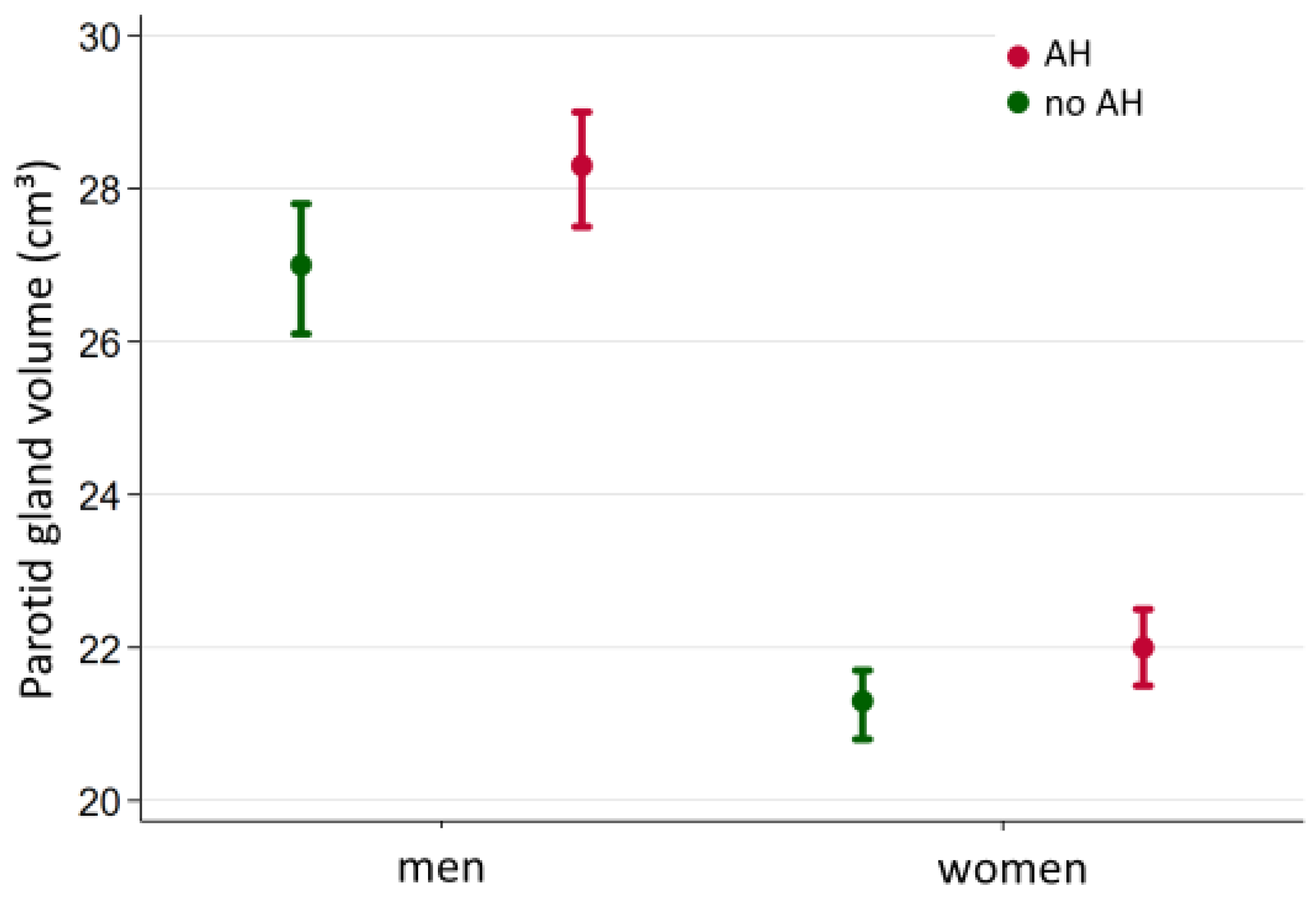
3.3.3. Associations of Diabetes Mellitus and Arterial Hypertension with Parotid Volume
3.4. Prevalence of Tumors of the Parotid Gland
4. Discussion
4.1. Cohort and Imaging Modalities
4.2. Comparison of Results in Different Studies
4.3. Associations between Sex, Age, BMI, Arterial Hypertension and Diabetes Mellitus and Gland Volume
4.3.1. Influence of Sex on Parotid Volume
4.3.2. Influence of Age on Parotid Volume
4.3.3. Influence of BMI on Parotid Volume
4.3.4. Discussion of Parotid Volumes in Relation to Selected Comorbidities
4.4. Significance of the Detection of Parotid Lesions
4.5. Stength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AH | Arterial Hypertension |
| BMI | Body Mass Index |
| CA | Contrast Agent |
| CI | Confidence Interval |
| CT | Computed Tomography |
| F | Female |
| ICC | Intraclass Correlation Coefficient |
| M | Male |
| MRI | Magnetic Resonance Imaging |
| N.E. | Not Evaluated |
| PET-CT | Positron Emission Tomography-Computed Tomography |
| ROI | Region of Interest |
| SD | Standard Deviation |
| SEM | Standard Error of the Mean |
| SHIP | Study of Health in Pomerania |
| T | Tesla |
| T2DM | Type 2 Diabetes Mellitus |
| Vs. | Versus |
References
- Dodds, M.W.; Johnson, D.A.; Yeh, C.K. Health benefits of saliva: A review. J. Dent. 2005, 33, 223–233. [Google Scholar] [CrossRef]
- Lima, D.L.F.; Carneiro, S.D.R.M.; Barbosa, F.T.S.; Saintrain, M.V.L.; Moizan, J.A.H.; Doucet, J. Salivary flow and xerostomia in older patients with type 2 diabetes mellitus. PLoS ONE 2017, 12, e0180891. [Google Scholar] [CrossRef] [Green Version]
- Janssen, H.S.A.; Turowski, B. Bildgebung der Kopfspeicheldrüsen; Georg Thieme Verlag: Stuttgart, NY, USA, 2010; Volume 10, pp. 163–179. [Google Scholar]
- Cohnen, M.; Andersen, K. Kopf-Hals-Radiologie; Thieme: New York, NY, USA, 2012; p. 349. [Google Scholar]
- Myers, E.N.; Ferris, R.L. Salivary Gland Disorders; Springer: Berlin/Heidelberg, Germany, 2007; pp. 17–104. [Google Scholar]
- Waldeyer, A.; Fanghänel, J. Waldeyer Anatomie des Menschen; de Gruyter-Verlag: Berlin, Gremany; New York, NY, USA, 2003; p. 1334. [Google Scholar]
- Strutz, J.; Arndt, O. Praxis der HNO-Heilkunde, Kopf- und Halschirurgie; Georg Thieme Verlag: Stuttgart, NY, USA, 2010; p. 1071. [Google Scholar]
- Standring, S.E.A. Gray’s Anatomy—The Anatomical Basis of Clinical Practice, 41st ed.; Elsevier: Amsterdam, The Netherlands, 2016; p. 504. [Google Scholar]
- Peters, P.E.W.K.; Erlemann, R. Erkrankungen der Speicheldrüsen. In Gesichtsschädel Felsenbein · Speicheldrüsen · Pharynx · Larynx Halsweichteile; Klinische Radiologie (Diagnostik mit bildgebenden Verfahren); Mödder, U., Ed.; Springer: Berlin/Heidelberg, Germany, 1991. [Google Scholar]
- Ericson, S. The normal variation of the parotid size. Acta Otolaryngol. 1970, 70, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Flower, E.A.; Burns, J. A quantitative study of histological changes in the human parotid gland occurring with adult age. J. Oral Pathol. 1987, 16, 505–510. [Google Scholar] [CrossRef]
- Mahne, A.; El-Haddad, G.; Alavi, A.; Houseni, M.; Moonis, G.; Mong, A.; Hernandez-Pampaloni, M.; Torigian, D.A. Assessment of age-related morphological and functional changes of selected structures of the head and neck by computed tomography, magnetic resonance imaging, and positron emission tomography. Semin. Nucl. Med. 2007, 37, 88–102. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Sun, Z.P.; Liu, X.J.; Yu, G.Y. Volume measurements of human parotid and submandibular glands. Beijing Da Xue Xue Bao Yi Xue Ban 2014, 46, 288–293. [Google Scholar] [PubMed]
- Medbery, R.; Yousem, D.M.; Needham, M.F.; Kligerman, M.M. Variation in parotid gland size, configuration, and anatomic relations. Radiother. Oncol. 2000, 54, 87–89. [Google Scholar] [CrossRef]
- Heo, M.S.; Lee, S.C.; Lee, S.S.; Choi, H.M.; Choi, S.C.; Park, T.W. Quantitative analysis of normal major salivary glands using computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 240–244. [Google Scholar] [CrossRef]
- Hosten, N.; Bülow, R.; Völzke, H.; Domin, M.; Schmidt, C.O.; Teumer, A.; Ittermann, T.; Nauck, M.; Felix, S.; Dörr, M.; et al. SHIP-MR and Radiology: 12 Years of Whole-Body Magnetic Resonance Imaging in a Single Center. Healthcare 2021, 10, 33. [Google Scholar] [CrossRef]
- Schipf, S.; Werner, A.; Tamayo, T.; Holle, R.; Schunk, M.; Maier, W.; Meisinger, C.; Thorand, B.; Berger, K.; Mueller, G.; et al. Regional differences in the prevalence of known Type 2 diabetes mellitus in 45–74 years old individuals: Results from six population-based studies in Germany (DIAB-CORE Consortium). Diabet Med. 2012, 29, e88–e95. [Google Scholar] [CrossRef]
- Meisinger, C.; Strassburger, K.; Heier, M.; Thorand, B.; Baumeister, S.E.; Giani, G.; Rathmann, W. Prevalence of undiagnosed diabetes and impaired glucose regulation in 35-59-year-old individuals in Southern Germany: The KORA F4 Study. Diabet Med. 2010, 27, 360–362. [Google Scholar] [CrossRef] [PubMed]
- Stöckl, D.; Rückert-Eheberg, I.M.; Heier, M.; Peters, A.; Schipf, S.; Krabbe, C.; Völzke, H.; Tamayo, T.; Rathmann, W.; Meisinger, C. Regional Variability of Lifestyle Factors and Hypertension with Prediabetes and Newly Diagnosed Type 2 Diabetes Mellitus: The Population-Based KORA-F4 and SHIP-TREND Studies in Germany. PLoS ONE 2016, 11, e0156736. [Google Scholar] [CrossRef]
- Völzke, H.; Fung, G.; Ittermann, T.; Yu, S.; Baumeister, S.E.; Dörr, M.; Lieb, W.; Völker, U.; Linneberg, A.; Jørgensen, T.; et al. A new, accurate predictive model for incident hypertension. J. Hypertens 2013, 31, 2142–2150, discussion 2150. [Google Scholar] [CrossRef] [PubMed]
- Meisinger, C.; Heier, M.; Völzke, H.; Löwel, H.; Mitusch, R.; Hense, H.W.; Lüdemann, J. Regional disparities of hypertension prevalence and management within Germany. J. Hypertens 2006, 24, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, F.N.; Carvalho, R.A. Metabolic remodeling triggered by salivation and diabetes in major salivary glands. NMR Biomed. 2017, 30. in press. [Google Scholar] [CrossRef]
- Dodds, M.W.; Yeh, C.K.; Johnson, D.A. Salivary alterations in type 2 (non-insulin-dependent) diabetes mellitus and hypertension. Community Dent. Oral Epidemiol. 2000, 28, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Carda, C.; Mosquera-Lloreda, N.; Salom, L.; Gomez de Ferraris, M.E.; Peydró, A. Structural and functional salivary disorders in type 2 diabetic patients. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, E309–E314. [Google Scholar]
- Puls, R.; Völzke, H. Ganzkörper-MRT in der “Study of Health in Pomerania”. Radiologe 2011, 51, 379–383. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Völzke, H.; Schössow, J.; Schmidt, C.O.; Jürgens, C.; Richter, A.; Werner, A.; Werner, N.; Radke, D.; Teumer, A.; Ittermann, T.; et al. Cohort Profile Update: The Study of Health in Pomerania (SHIP). Int. J. Epidemiol. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Burke, C.J.; Thomas, R.H.; Howlett, D. Imaging the major salivary glands. Br. J. Oral Maxillofac. Surg. 2011, 49, 261–269. [Google Scholar] [CrossRef]
- Holle, R.; Happich, M.; Löwel, H.; Wichmann, H.E.; Group, M.K.S. KORA–Eine Forschungsplattform für bevölkerungsbezogene Gesundheitsforschung. Gesundheitswesen 2005, 67 (Suppl. S1), S19–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COCHRAN, W.G. Modern methods in the sampling of human populations. Am. J. Public Health Nations Health 1951, 41, 647–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhauser, H.; Kuhnert, R.; Born, S. 12-Monats-Prävalenz von Bluthochdruck in Deutschland. J. Health Monit. 2017. [Google Scholar] [CrossRef]
- Christin, H.; Ronny, K.; Born, S.; Christa, S.-N. 12-Monats-Prävalenz des bekannten. Diabetes mellitus in Deutschland. J. Health Monit. 2017. [Google Scholar] [CrossRef]
- Müller, R.; Büttner, P. A critical discussion of intraclass correlation coefficients. Stat. Med. 1994, 13, 2465–2476. [Google Scholar] [CrossRef]
- Saito, N.; Sakai, O.; Bauer, C.M.; Norbash, A.M.; Jara, H. Age-related relaxo-volumetric quantitative magnetic resonance imaging of the major salivary glands. J. Comput. Assist. Tomogr. 2013, 37, 272–278. [Google Scholar] [CrossRef]
- Dos Santos, W.P.; Perez Gomes, J.P.; Nussi, A.D.; Altemani, J.M.; Botti Rodrigues Dos Santos, M.T.; Hasseus, B.; Giglio, D.; Braz-Silva, P.H.; Ferreira Costa, A.L. Morphology, Volume, and Density Characteristics of the Parotid Glands before and after Chemoradiation Therapy in Patients with Head and Neck Tumors. Int. J. Dent. 2020, 2020, 8176260. [Google Scholar] [CrossRef] [Green Version]
- Ono, K.; Morimoto, Y.; Inoue, H.; Masuda, W.; Tanaka, T.; Inenaga, K. Relationship of the unstimulated whole saliva flow rate and salivary gland size estimated by magnetic resonance image in healthy young humans. Arch. Oral Biol. 2006, 51, 345–349. [Google Scholar] [CrossRef]
- Niendorf, S.; Koch, C.; Völzke, H.; Langner, S.; Hosemann, W.; Beule, A.G. Results of the volume of the submandibular gland in an epidemiologic cohort. Abstr. Imaging/Sonogr. Laryngo-Rhino-Otol. 2020, 99, 48. [Google Scholar] [CrossRef]
- Hegedüs, L. Thyroid size determined by ultrasound. Influence of physiological factors and non-thyroidal disease. Dan Med. Bull 1990, 37, 249–263. [Google Scholar]
- Kromrey, M.L.; Ittermann, T.; vWahsen, C.; Plodeck, V.; Seppelt, D.; Hoffmann, R.T.; Heiss, P.; Kühn, J.P. Reference values of liver volume in Caucasian population and factors influencing liver size. Eur. J. Radiol. 2018, 106, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Naeem, M.; Markus, M.R.P.; Mousa, M.; Schipf, S.; Dörr, M.; Steveling, A.; Aghdassi, A.; Kühn, J.P.; Kromrey, M.L.; Nauck, M.; et al. Associations of liver volume and other markers of hepatic steatosis with all-cause mortality in the general population. Liver Int. 2022, 42, 575–584. [Google Scholar] [CrossRef]
- Konttinen, Y.T.; Stegaev, V.; Mackiewicz, Z.; Porola, P.; Hänninen, A.; Szodoray, P. Salivary glands—“an unisex organ”? Oral Dis. 2010, 16, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Porcheri, C.; Mitsiadis, T.A. Physiology, Pathology and Regeneration of Salivary Glands. Cells 2019, 8, 976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagler, R.M. Salivary glands and the aging process: Mechanistic aspects, health-status and medicinal-efficacy monitoring. Biogerontology 2004, 5, 223–233. [Google Scholar] [CrossRef]
- Waterhouse, J.P.; Chisholm, D.M.; Winter, R.B.; Patel, M.; Yale, R.S. Replacement of functional parenchymal cells by fat and connective tissue in human submandibular salivary glands: An age-related change. J. Oral Pathol. 1973, 2, 16–27. [Google Scholar] [CrossRef]
- Stang, A.; Döring, A.; Völzke, H.; Moebus, S.; Greiser, K.H.; Werdan, K.; Berger, K.; Ellert, U.; Neuhauser, H. Regional differences in body fat distributions among people with comparable body mass index: A comparison across six German population-based surveys. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 106–114. [Google Scholar] [CrossRef]
- Ghezzi, E.M.; Ship, J.A. Aging and secretory reserve capacity of major salivary glands. J. Dent. Res. 2003, 82, 844–848. [Google Scholar] [CrossRef]
- Su, G.Y.; Wang, C.B.; Hu, H.; Liu, J.; Ding, H.Y.; Xu, X.Q.; Wu, F.Y. Effect of laterality, gender, age and body mass index on the fat fraction of salivary glands in healthy volunteers: Assessed using iterative decomposition of water and fat with echo asymmetry and least-squares estimation method. Dentomaxillofac. Radiol. 2019, 48, 20180263. [Google Scholar] [CrossRef]
- Chang, H.C.; Juan, C.J.; Chiu, H.C.; Cheng, C.C.; Chiu, S.C.; Liu, Y.J.; Chung, H.W.; Hsu, H.H. Effects of gender, age, and body mass index on fat contents and apparent diffusion coefficients in healthy parotid glands: An MRI evaluation. Eur. Radiol. 2014, 24, 2069–2076. [Google Scholar] [CrossRef]
- Emmelin, N. Nerve interactions in salivary glands. J. Dent. Res. 1987, 66, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Schwenzer, N.F.; Schraml, C.; Martirosian, P.; Boss, A.; Claussen, C.D.; Schick, F. MR measurement of blood flow in the parotid gland without contrast medium: A functional study before and after gustatory stimulation. NMR Biomed. 2008, 21, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Baum, B.J. Evaluation of stimulated parotid saliva flow rate in different age groups. J. Dent. Res. 1981, 60, 1292–1296. [Google Scholar] [CrossRef]
- Islas Andrade, S.A.; Frati Munari, A.C.; González Angulo, J.; Iturralde, P.; Llanos Vega, L.M. Increase in neuroendocrine secretion granules in submaxillary and parotid glands in patients with non-insulin dependent diabetes mellitus. Gac. Med. Mex. 1992, 128, 411–414. [Google Scholar] [PubMed]
- Matczuk, J.; Zalewska, A.; Łukaszuk, B.; Knaś, M.; Maciejczyk, M.; Garbowska, M.; Ziembicka, D.M.; Waszkiel, D.; Chabowski, A.; Żendzian-Piotrowska, M.; et al. Insulin Resistance and Obesity Affect Lipid Profile in the Salivary Glands. J. Diabetes Res. 2016, 2016, 8163474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebsregisterdaten, Z.F. Krebs in Deutschland für 2015/2016, 12th ed.; Zentrum für Krebsregisterdaten, Gesellschaft der epidemiologischen Krebsregister in Deutschland; Robert Koch-Institute: Berlin, Germany, 2019. [Google Scholar]
- Pinkston, J.A.; Cole, P. Incidence rates of salivary gland tumors: Results from a population-based study. Otolaryngol. Head Neck Surg. 1999, 120, 834–840. [Google Scholar] [CrossRef]
- Speight, P.M.; Barrett, A.W. Salivary gland tumours. Oral Dis. 2002, 8, 229–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinheimer, A.; Vieira, D.S.; Cordeiro, M.M.; Rivero, E.R. Retrospective study of 124 cases of salivary gland tumors and literature review. J. Clin Exp. Dent. 2019, 11, e1025–e1032. [Google Scholar] [CrossRef]
- Grosheva, M.; Pick, C.; Granitzka, T.; Sommer, B.; Wittekindt, C.; Klussmann, J.P.; Guntinas-Lichius, O.; Beutner, D. Impact of extent of parotidectomy on early and long-term complications: A prospective multicenter cohort trial. Head Neck 2019, 41, 1943–1951. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Excluded Subjects (n = 1481) | Included Subjects (n = 1725) | p * | |
|---|---|---|---|
| Age; years | 49 (40; 60) | 56 (45; 65) | <0.001 |
| Male; % | 867 (60.5%) | 654 (37.9%) | <0.001 |
| Status of Smoking Never Formerly Presently | 517 (35.0%) 577 (39.1%) 383 (25.9%) | 742 (43.1%) 650 (37.8%) 330 (19.2%) | <0.001 |
| Body Mass Index | 26.8 (24.0; 29.8) | 27.8 (24.8; 30.9) | <0.001 |
| Body Weight; kg | 80.7 (70.4; 92.3) | 77.6 (67.9; 88.4) | |
| Body Height; cm | 173 (167; 180) | 167 (161; 173) | |
| Waist Circumference; cm | 90 (80; 99) | 90 (80; 100) | 0.569 |
| HDL-Cholesterol; mmol/L | 1.39 (1.14; 1.67) | 1.43 (1.21; 1.70) | 0.010 |
| LDL-Cholesterol; mmol/L | 3.32 (2.71; 3.90) | 3.40 (2.75; 4.04) | 0.110 |
| Triglycerides; mmol/L | 1.31 (0.92; 2.01) | 1.43 (0.98; 2.01) | <0.001 |
| Glucose; mmol/L | 5.3 (4.9; 5.8) | 5.4 (5.0; 5.9) | 0.142 |
| HbA1c; % | 5.2 (4.8; 5.6) | 5.3 (5.0; 5.7) | <0.001 |
| Systolic Blood Pressure; mmHg | 128 (116; 139) | 128 (115; 140) | 0.833 |
| Diastolic Blodd Pressure; mmHg | 78 (71; 84) | 78 (72; 85) | 0.585 |
| Arterial Hypertension | 634 (42.9%) | 837 (48.8%) | 0.001 |
| Type 2 Diabetes Mellitus | 108 (7.3%) | 188 (10.9%) | <0.001 |
| All Subjects (n = 1725) | Men (n = 654) | Women (n = 1071) | |
|---|---|---|---|
| Status of Smoking | |||
| Formerly vs. Never | 0.60 (−0.08; 1.40) | 0.57 (−0.85; 1.99) | 0.70 (−0.15; 1.54) |
| Presently vs. Never | −0.05 (−0.97; 0.87) | −1.07 (−2.86; 0.72) | 0.60 (−0.43; 1.63) |
| Body Mass Index; kg/m2 | 0.87 (0.81; 0.93) * | 1.25 (1.11; 1.40) * | 0.75 (0.69; 0.81) * |
| Waist Circumference; cm | 0.36 (0.33; 0.38) * | 0.43 (0.38; 0.48) * | 0.32 (0.30; 0.35) * |
| HDL Cholesterol; mmol/L | −1.01 (−1.84; −0.18) | −0.77 (−2.53; 0.99) | −1.16 (−2.02;−0.31) |
| LDL Cholesterol; mmol/L | 0.37 (0.08; 0.66) * | 0.19 (−0.36; 0.75) | 0.57 (0.25; 0.89) * |
| Triglycerides; mmol/L | 0.70 (0.44; 0.97) * | 0.55 (0.16; 0.94) * | 0.83 (0.45; 1.21) * |
| Type 2 Diabetes Mellitus | 1.27 (0.38; 2.16) | 1.63 (−0.02; 3.28) | 1.02 (0.04; 2.00) |
| Glucose; mmol/L | 0.50 (0.30; 0.70) * | 0.55 (0.20; 0.89) * | 0.40 (0.17; 0.63) * |
| HbA1c; % | 0.67 (0.29; 1.04) * | 0.37 (−0.26; 1.00) | 0.88 (0.43; 1.33) * |
| Systolic Blood Pressure; mmHg | 0.02 (0.01; 0.04) * | 0.02 (−0.01; 0.06) | 0.02 (−0.01; 0.04) |
| Diastolic Blood Pressure; mmHg | 0.04 (0.01; 0.07) * | 0.03 (−0.02; 0.08) | 0.02 (−0.01; 0.06) |
| Arterial Hypertension | 1.04 (0.42; 1.66) * | 1.14 (−0.03; 2.31) * | 0.75 (0.07; 1.44) |
| Tumors | N | Median Volume (cm3) | Mean (cm3) | Standard Deviation | Variance | Kurtosis |
|---|---|---|---|---|---|---|
| Right parotid gland | 41 | 0.161 | 0.299 | 0.333 | 0.111 | 5.95 |
| Left parotid gland | 34 | 0.214 | 0.56 | 1.346 | 1.811 | 26.91 |
| Dos Santos et al. (2020) [35] | Heo et al. (2001) [15] | Li et al. (2014) [13] | Mahne et al. (2007) [12] | Medbery et al. (2000) [14] | Ono et al. (2006) [36] | Saito et al. (2013) [34] | Present Study (2022) | ||
|---|---|---|---|---|---|---|---|---|---|
| Imaging (plane, layer thickness) | CT with CA | CT (5 mm) | CT (axial, 1.25 mm) | MRI, 1.5 T (axial, 5 mm) | PET-CT (axial, 5 mm) | MRI, 1.5 T (7 mm) | MRI, 1.5 T (axial, 7 mm) | MRI, 1.5 T | MRI, 1.5 T (axial, 4 mm) |
| N-subjects (m; %m) | 49 (45; 92%) | 42 (21; 50%) | 240 (120; 50%) | 64 (25; 39%) | 35 (19; 54%) | 16 (n.e.) | 28 (23; 82%) | 35 (20; 57%) | 1725 (654; 38%) |
| Study design; specifics | Clinical, oncology study (pre-& post radiation) | Prospective; No volume estimation, measuring MCSA | Prospective; no exclusion of extra parenchymal structures | Retrospective; oncology setting; 2 separate collectives and modalities | Retrospective; oncology setting | Prospective; exclusion of extra parenchymal structures | Retrospective; clinical setting; exclusion of extra parenchymal structures | Prospective, epidemiological study; exclusion of extra parenchymal structures | |
| Mean parotid gland volume, (range), <SD> | 29 cm3 (11–55) <9.5> | {7.5–8.7 MCSA in cm2} | 25 cm3 m: 16.9–35.1 cm3 f: 13.9–34.9 cm3 | bilat.: m: 55 cm3 (20–96) <19> f: 36cm3 (13–72) <16> | m: 25 cm3 (3–42), <12> f: 17 cm3 (11–36), <9> | 25.3 (9–54) cm3 | bilat.: 80.2 cm3 (46–120) <SEM 3.3> | 5–38 cm3 | 23.9 cm3 <8.1> (4–61.8) m: 27.82 cm3 <8.23> f: 21.60 cm3 <6> |
| Inter- observer reliability; ICC | Automatic ROI marking according to thresholds | n.e. | n.e. | n.e. | n.e. | 4,8% | n.e. | n.e. | 7.9%/16.7%; ICC 0.78/0.72 |
| Laterality | r = l | r = l | r = l | r = l | r = l | r = l | r = l | n.e. | r = l |
| Association with sex (m > f) | n.e. | p > 0.05 | p < 0.05 | p < 0.001 | p = 0.15 | n.e. | n.e. | n.e. | p < 0.05 |
| Association with age (range of age in years) | n.e. | p < 0.05 (21–76) | p < 0.01 (25–60) | p = 0.06 (13–81) | p = 0.3 (10–76) | n.e. | n.e. | p < 0.05 for age-dependent fat saturation (0.5–87) | p < 0.05 (21–79) |
| Association with BMI | n.e. | p < 0.05 | n.e. | n.e. | n.e. | n.e. | Body weight: p < 0.001 | n.e. | p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzoska, T.; Ittermann, T.; Ihler, F.; Koch, C.; Blaurock, M.; Bülow, R.; Völzke, H.; Busch, C.-J.; Beule, A.G. Population Based Average Parotid Gland Volume and Prevalence of Incidental Tumors in T1-MRI. Healthcare 2022, 10, 2310. https://doi.org/10.3390/healthcare10112310
Brzoska T, Ittermann T, Ihler F, Koch C, Blaurock M, Bülow R, Völzke H, Busch C-J, Beule AG. Population Based Average Parotid Gland Volume and Prevalence of Incidental Tumors in T1-MRI. Healthcare. 2022; 10(11):2310. https://doi.org/10.3390/healthcare10112310
Chicago/Turabian StyleBrzoska, Tina, Till Ittermann, Friedrich Ihler, Carmela Koch, Markus Blaurock, Robin Bülow, Henry Völzke, Chia-Jung Busch, and Achim Georg Beule. 2022. "Population Based Average Parotid Gland Volume and Prevalence of Incidental Tumors in T1-MRI" Healthcare 10, no. 11: 2310. https://doi.org/10.3390/healthcare10112310