
Gender-Specific Effect of Couple-Based Intervention on Behavioral and Psychological Outcomes of Older Adults with Type 2 Diabetes during the COVID-19 Partial Lockdown in Guangzhou, China
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Study Participants
2.3. Measures
2.3.1. Lifestyle-Related Behavior Changes
2.3.2. Diabetes Self-Care Activities
2.3.3. Depressive Symptoms
2.3.4. Covariates
2.4. Statistical Analysis
3. Results
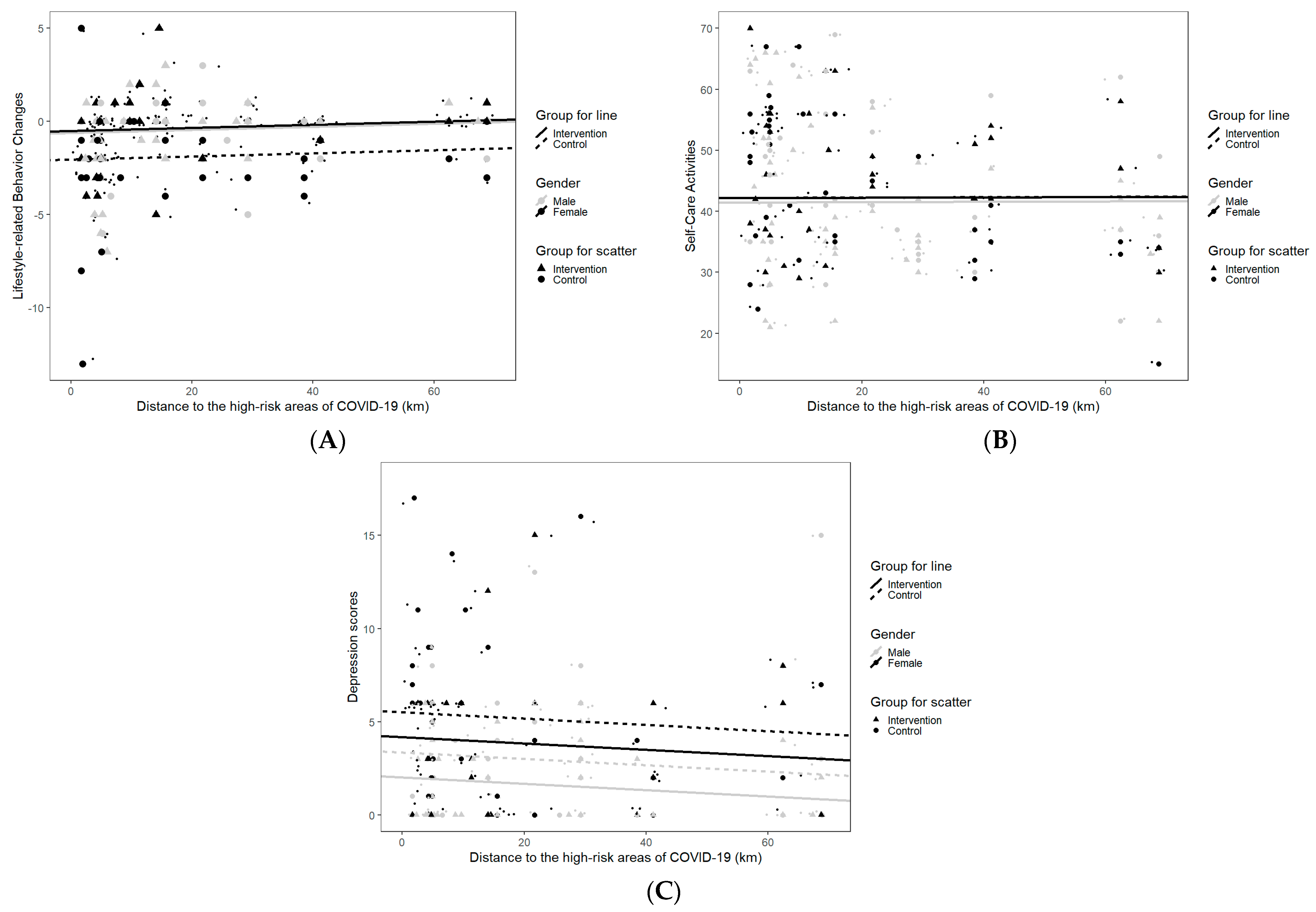
3.1. Gender-Specific Differences in Outcomes between Intervention Groups by Distance to the High-Risk Areas for the Cross-Sectional COVID-19 Survey
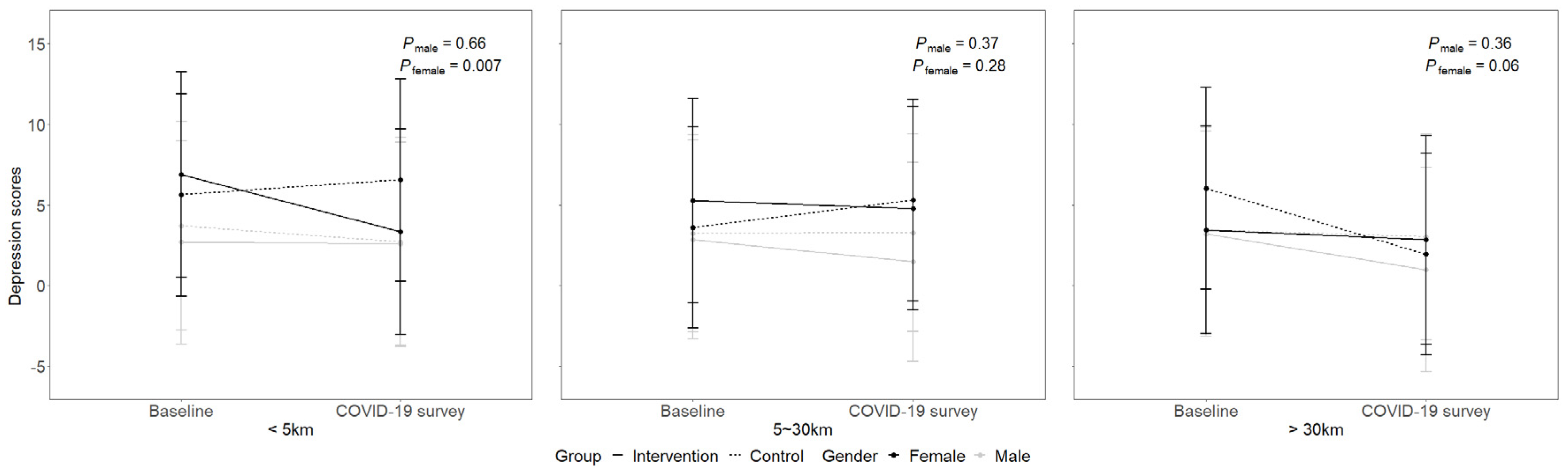
3.2. Longitudinal Changes of the Gender-Specific Differences in Outcomes between Intervention Groups by Distance to the High-Risk Areas
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef] [PubMed]
- Valabhji, J.; Barron, E.; Gorton, T.; Bakhai, C.; Kar, P.; Young, B.; Khunti, K.; Holman, N.; Sattar, N.; Wareham, N.J. Associations between reductions in routine care delivery and non-COVID-19-related mortality in people with diabetes in England during the COVID-19 pandemic: A population-based parallel cohort study. Lancet Diabetes Endocrinol. 2022, 10, 561–570. [Google Scholar] [CrossRef]
- State Council of the PRC. The Prevention and Control of 2019 Novel Coronavirus Pneumonia, 8th ed; 2021. Available online: http://www.gov.cn/xinwen/2021-05/14/content_5606469.htm (accessed on 27 May 2022).
- Zhong, N. Guangzhou Summed up Five Experiences in Dealing with SARS-CoV-2 Variant Delta for the First Time. 2021. Available online: https://m.thepaper.cn/baijiahao_13322445 (accessed on 1 June 2022).
- Wright, A.; Salazar, A.; Mirica, M.; Volk, L.A.; Schiff, G.D. The Invisible Epidemic: Neglected Chronic Disease Management During COVID-19. J. Gen. Intern. Med. 2020, 35, 2816–2817. [Google Scholar] [PubMed]
- Huang, L.; Zhang, L.; Jiang, S.; Liang, B.; Xu, N.; Li, J.; Zhang, X.; Zhang, Z. Association of the Coronavirus Disease 2019 Outbreak on the Diabetes Self-Management in Chinese Patients: An Analytical Cross-Sectional Study. Diabetes Metab. Syndr. Obesity Targets Ther. 2022, 15, 1413–1422. [Google Scholar]
- Yan, A.F.; Sun, X.; Zheng, J.; Mi, B.; Zuo, H.; Ruan, G.; Hussain, A.; Wang, Y.; Shi, Z. Perceived risk, behavior changes and Health-related outcomes during COVID-19 pandemic: Findingsamong adults with and without diabetesin China. Diabetes Res. Clin. Pract. 2020, 167, 108350. [Google Scholar] [CrossRef]
- Ruissen, M.M.; Regeer, H.; Landstra, C.P.; Schroijen, M.; Jazet, I.; Nijhoff, M.F.; Pijl, H.; Ballieux, B.E.P.B.; Dekkers, O.; Huisman, S.D.; et al. Increased stress, weight gain and less exercise in relation to glycemic control in people with type 1 and type 2 diabetes during the COVID-19 pandemic. BMJ Open Diabetes Res. Care 2021, 9, e002035. [Google Scholar] [CrossRef]
- Moradian, S.; Teufel, M.; Jahre, L.; Musche, V.; Fink, M.; Dinse, H.; Schweda, A.; Weismüller, B.; Dörrie, N.; Tan, S.; et al. Mental health burden of patients with diabetes before and after the initial outbreak of COVID-19: Predictors of mental health impairment. BMC Public Health 2021, 21, 2068. [Google Scholar]
- Li, Y.; Su, S.; Luo, B.; Wang, J.; Liao, S. Physical activity and depressive symptoms among community-dwelling older adults in the COVID-19 pandemic era: A three-wave cross-lagged study. Int. J. Disaster Risk Reduct. 2022, 70, 102793. [Google Scholar]
- Lebow, J.L. Family in the Age of COVID-19. Fam. Process 2020, 59, 309–312. [Google Scholar]
- Cobb, L.K.; McAdams-DeMarco, M.A.; Gudzune, K.A.; Anderson, C.A.; Demerath, E.; Woodward, M.; Selvin, E.; Coresh, J. Changes in Body Mass Index and Obesity Risk in Married Couples Over 25 Years: The ARIC Cohort Study. Am. J. Epidemiol. 2016, 183, 435–443. [Google Scholar] [CrossRef] [Green Version]
- Shih, D.-P.; Wen, C.-T.; Kuo, H.-W.; Liang, W.-M.; Liu, L.-F.; Su, C.-T.; Wang, J.-Y. Spousal Concordance in Dietary Behaviors and Metabolic Components, and Their Association: A Cross-Sectional Study. Nutrients 2020, 12, 3332. [Google Scholar]
- Cobb, L.K.; Godino, J.G.; Selvin, E.; Kucharska-Newton, A.; Coresh, J.; Koton, S. Spousal Influence on Physical Activity in Middle-Aged and Older Adults: The ARIC Study. Am. J. Epidemiol. 2016, 183, 444–451. [Google Scholar] [PubMed] [Green Version]
- Pereira, M.G.; Machado, J.C.; Sousa, M.R.; Pedras, S. A study of a couple with type 2 diabetes: Dyadic adjustment and psychological morbidity. Rev. Assoc. Med. Bras. 2014, 60, 318–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidel, A.; Franks, M.M.; Stephens, M.A.P.; Rook, K.S. Spouse Control and Type 2 Diabetes Management: Moderating Effects of Dyadic Expectations for Spouse Involvement. Fam. Relat. 2012, 61, 698–709. [Google Scholar] [PubMed]
- Wing, R.R.; Marcus, M.D.; Epstein, L.H.; Jawad, A. A “family-based” approach to the treatment of obese type II diabetic patients. J. Consult. Clin. Psychol. 1991, 59, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.; Wu, X.; Wang, C.; Xiao, X.; Cai, Y.; Wu, M.; Liu, Y.; Chen, X.; Wu, S.; Yang, Y.J.; et al. Couple-based collaborative management model of type 2 diabetes mellitus for community-dwelling older adults in China: Protocol for a hybrid type 1 randomized controlled trial. BMC Geriatr. 2020, 20, 123. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.J.; Zhan, Z.; Xue, M.; Zheng, P.; Lyu, J.; Ma, J.; Zhang, X.D.; Luo, W.; Huang, H.; Zhang, Y.; et al. Public Health Measures and the Control of COVID-19 in China. Clin. Rev. Allergy Immunol. 2021, 1–16. [Google Scholar] [CrossRef]
- Kumari, A.; Ranjan, P.; Vikram, N.K.; Kaur, D.; Sahu, A.; Dwivedi, S.N.; Baitha, U.; Goel, A. A short questionnaire to assess changes in lifestyle-related behaviour during COVID 19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1697–1701. [Google Scholar] [CrossRef]
- Chopra, S.; Ranjan, P.; Singh, V.; Kumar, S.; Arora, M.; Hasan, M.S.; Kasiraj, R.; Suryansh; Kaur, D.; Vikram, N.K.; et al. Impact of COVID-19 on lifestyle-related behaviours—A cross-sectional audit of responses from nine hundred and ninety-five participants from India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2021–2030. [Google Scholar] [CrossRef]
- Berens, C. Volunteerism during the COVID-19 Pandemic: A look at Risk Perceptions, Health Behaviors, and Quality of Life. Doctoral Dissertation, University of Missouri, Kansas City, MI, USA, 2021. [Google Scholar]
- Saadeh, D.; Hajj, A.; Malaeb, D.; Sacre, H.; Haddad, C.; Salameh, P. Assessing Changes in Lifestyle and Health-Related Behaviors During the COVID-19 Pandemic: A Cross Sectional Web-Based Survey Among Lebanese Adults. 8 April 2021. preprint (Version 1). Available online: https://doi.org/10.21203/rs.3.rs-376219/v1 (accessed on 27 May 2022).
- Toobert, D.J.; Hampson, S.E.; Glasgow, R.E. The summary of diabetes self-care activities measure: Results from 7 studies and a revised scale. Diabetes Care 2000, 23, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Boey, K.W. Cross-validation of a short form of the CES-D in Chinese elderly. Int. J. Geriatr. Psychiatry 1999, 14, 608–617. [Google Scholar] [CrossRef]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale:A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Grund, S.; Lüdtke, O.; Robitzsch, A. Multiple Imputation of Missing Data for Multilevel Models. Organ. Res. Methods 2017, 21, 111–149. [Google Scholar]
- Yang, Q.; Wang, Y.; Tian, C.; Chen, Y.; Mao, J. The Experiences of Community-dwelling older adults during the COVID-19 Lockdown in Wuhan: A qualitative study. J. Adv. Nurs. 2021, 77, 4805–4814. [Google Scholar] [CrossRef]
- Ding, S.; Lei, Q.; Wu, W.; Xiao, Z.; Wu, Z.; Chen, M.; Chen, L. Changes in lifestyle, mood, and disease management among community-dwelling older adults during the COVID-19 pandemic in China. Aging Health Res. 2022, 2, 100059. [Google Scholar] [CrossRef]
- State Council of the PRC. Guidelines on Promoting “Internet Plus” Health Care Services during COVID-19 Prevention and Control. 2020. Available online: http://www.gov.cn/zhengce/zhengceku/2020-03/03/content_5486256.htm (accessed on 27 May 2022).
- National Health Commission of the PRC. Notice on Several Key Tasks in the Current Medical Service. 2021. Available online: http://www.nhc.gov.cn/xcs/zhengcwj/202103/89bdb7805e094e4da6fb244350bf3eb1.shtml (accessed on 1 June 2022).
- Kiecolt-Glaser, J.K.; Newton, T.L. Marriage and health: His and hers. Psychol. Bull. 2001, 127, 472–503. [Google Scholar] [CrossRef]
- Li, X.; Zhang, J. Confucian Doctrine’s Influence on the Socialization of Sex Equality. J. Dali Univ. 2008, 01, 53–57. [Google Scholar]
- Tripathee, S.; Sweeting, H.; Chambers, S.; Maclean, A. How men receive and utilise partner support when trying to change their diet and physical activity within a men’s weight management programme. BMC Public Health 2020, 20, 199. [Google Scholar] [CrossRef] [Green Version]
- Tu, J.; Liu, Y.; Wu, X.; Xu, D.; Liao, J. Dyadic appraisal and coping with illness among older Chinese adults with type 2 diabetes mellitus: A qualitative study. Age Ageing 2020, 50, 928–935. [Google Scholar] [CrossRef]
- Liao, J.; Zhang, J.; Xie, J.; Gu, J. Gender Specificity of Spousal Concordance in the Development of Chronic Disease among Middle-Aged and Older Chinese Couples: A Prospective Dyadic Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2886. [Google Scholar] [PubMed]
- Rosenman, R.; Tennekoon, V.; Hill, L.G. Measuring bias in self-reported data. Int. J. Behav. Healthc. Res. 2011, 2, 320–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boerma, T.; Hosseinpoor, A.R.; Verdes, E.; Chatterji, S. A global assessment of the gender gap in self-reported health with survey data from 59 countries. BMC Public Health 2016, 16, 675. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 156) | Control Group (n = 79) | Intervention Group (n = 77) | p-Value for Group Differences | |
|---|---|---|---|---|
| Response rate (%) | 75.4 | 78.2 | 72.6 | 0.38 |
| Age M (SD) | 66.0 (6.2) | 66.1 (6.13) | 66.0 (6.36) | 0.92 |
| Male (%) | 53.8 | 49.4 | 58.4 | 0.26 |
| Education (%) | 0.38 | |||
| Primary school or below | 30.8 | 38.0 | 23.4 | |
| Secondary school | 29.5 | 21.5 | 37.7 | |
| Tertiary education or above | 39.7 | 40.5 | 39.0 | |
| Retired (%) | 87.2 | 84.8 | 89.6 | 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, C.; Xu, Y.; Zhi, J.; Zheng, H.; Sun, Z.; Wu, X.; Liao, J. Gender-Specific Effect of Couple-Based Intervention on Behavioral and Psychological Outcomes of Older Adults with Type 2 Diabetes during the COVID-19 Partial Lockdown in Guangzhou, China. Healthcare 2022, 10, 2290. https://doi.org/10.3390/healthcare10112290
Yang C, Xu Y, Zhi J, Zheng H, Sun Z, Wu X, Liao J. Gender-Specific Effect of Couple-Based Intervention on Behavioral and Psychological Outcomes of Older Adults with Type 2 Diabetes during the COVID-19 Partial Lockdown in Guangzhou, China. Healthcare. 2022; 10(11):2290. https://doi.org/10.3390/healthcare10112290
Chicago/Turabian StyleYang, Conghui, Yingxin Xu, Jingyi Zhi, Huiqiong Zheng, Zhenhua Sun, Xueji Wu, and Jing Liao. 2022. "Gender-Specific Effect of Couple-Based Intervention on Behavioral and Psychological Outcomes of Older Adults with Type 2 Diabetes during the COVID-19 Partial Lockdown in Guangzhou, China" Healthcare 10, no. 11: 2290. https://doi.org/10.3390/healthcare10112290