
What Do We Know So Far about Ofatumumab for Relapsing Multiple Sclerosis? A Meta-Analytical Study

 , and
, and
Abstract
:1. Introduction
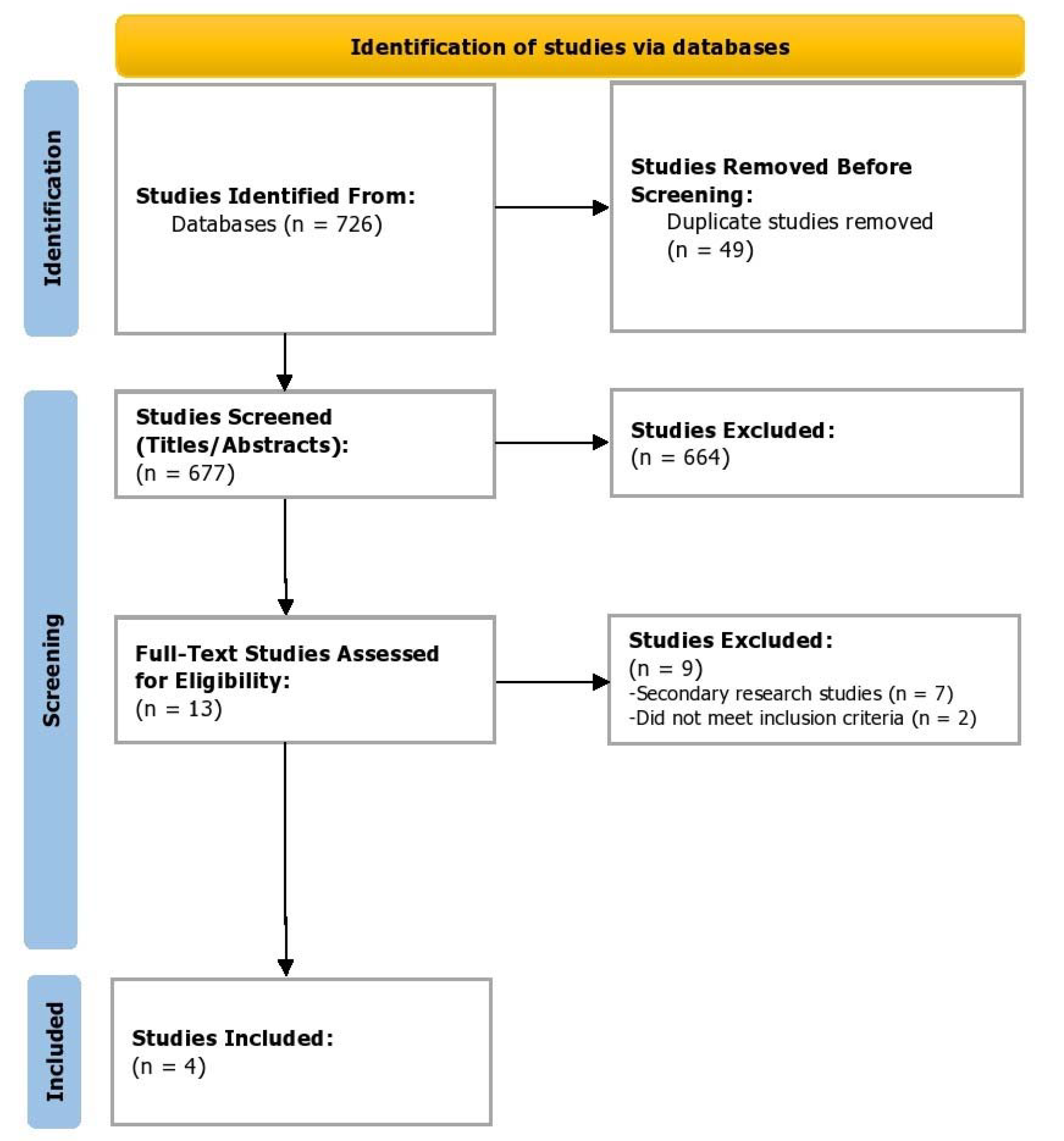
2. Methods
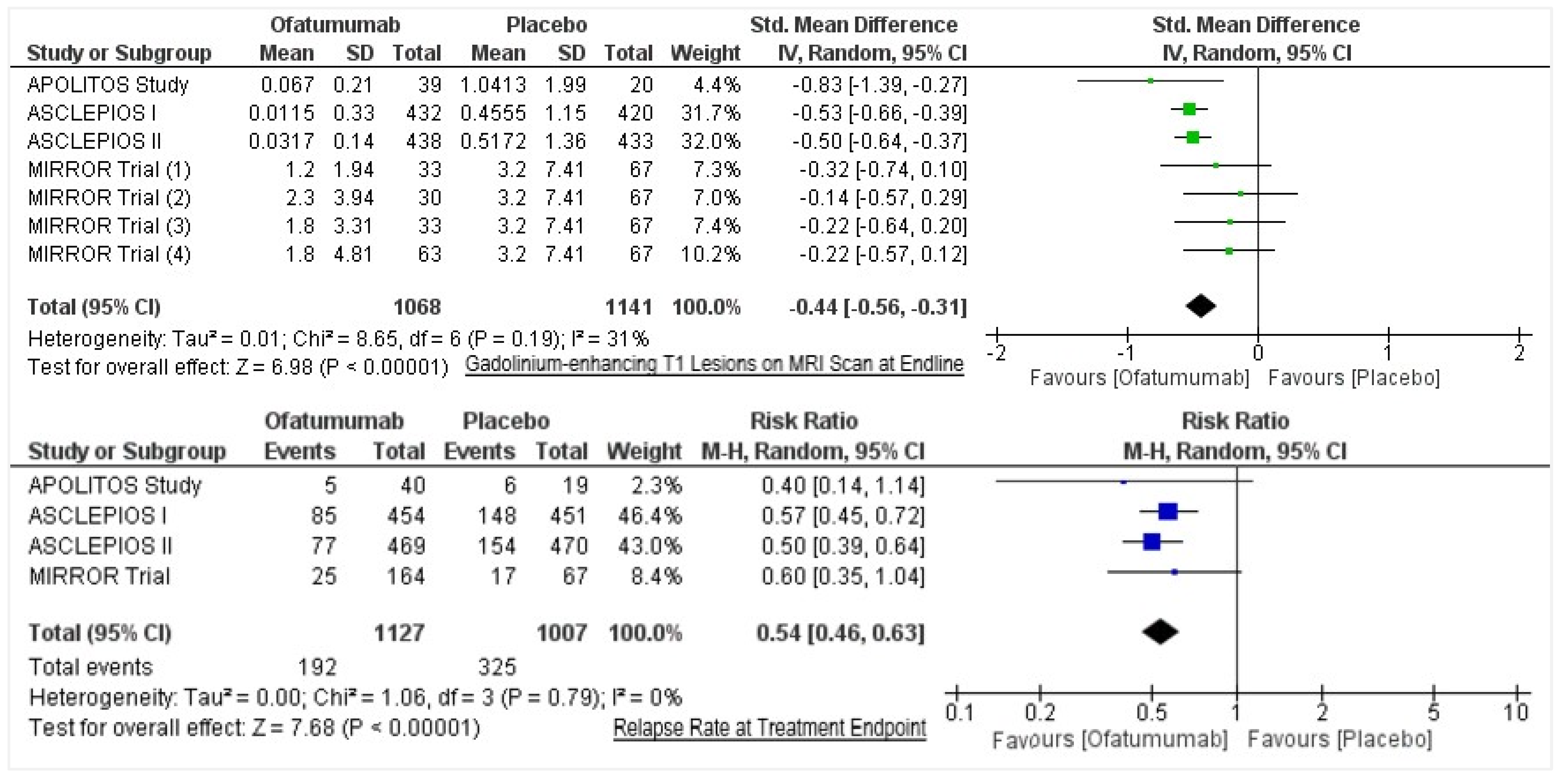
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang, C.; Blair, H.A. Ofatumumab: A Review in Relapsing Forms of Multiple Sclerosis. Drugs 2021, 82, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Samjoo, I.A.; Klotz, L.; Giovannoni, G.; Drudge, C.; Haltner, A.; Worthington, E.; Zhao, M.; Brennan, R.; Häring, D.A.; Cameron, C. Simulated Treatment Comparison of Efficacy Outcomes for Ofatumumab in ASCLEPIOS I/II versus Ocrelizumab in OPERA I/II for the Treatment of Patients with Relapsing Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 66, 104031. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration KESIMPTA® (Ofatumumab) Injection, for Subcutaneous Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125326s070lbl.pdf (accessed on 24 August 2022).
- Yu, H.; Graham, G.; David, O.J.; Kahn, J.M.; Savelieva, M.; Pigeolet, E.; Das Gupta, A.; Pingili, R.; Willi, R.; Ramanathan, K. Population Pharmacokinetic–B Cell Modeling for Ofatumumab in Patients with Relapsing Multiple Sclerosis. CNS Drugs 2022, 36, 283–300. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.; Lammens, A.; Schäfer, W.; Georges, G.; Schwaiger, M.; Mössner, E.; Hopfner, K.-P.; Umaña, P.; Niederfellner, G. Epitope Interactions of Monoclonal Antibodies Targeting CD20 and Their Relationship to Functional Properties. In Proceedings of the MAbs; Taylor & Francis: Oxfordshire, UK, 2013; Volume 5, pp. 22–33. [Google Scholar]
- Roach, C.A.; Cross, A.H. Anti-CD20 B Cell Treatment for Relapsing Multiple Sclerosis. Front. Neurol. 2021, 11, 595547. [Google Scholar] [CrossRef] [PubMed]
- Hemstedt, T.; Kugler, F. Ofatumumab as a Potential First-Line Therapy for Relapsing Multiple Sclerosis in Germany. Neurology 2021, 96, 4093. [Google Scholar]
- Kalincik, T. Multiple Sclerosis Relapses: Epidemiology, Outcomes and Management. A Systematic Review. Neuroepidemiology 2015, 44, 199–214. [Google Scholar] [CrossRef] [PubMed]
- Derfuss, T.; Ontaneda, D.; Nicholas, J.; Meng, X.; Hawker, K. Relapse Rates in Patients with Multiple Sclerosis Treated with Fingolimod: Subgroup Analyses of Pooled Data from Three Phase 3 Trials. Mult. Scler. Relat. Disord. 2016, 8, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Hauser, S.L.; Bar-Or, A.; Cohen, J.A.; Comi, G.; Correale, J.; Coyle, P.K.; Cross, A.H.; De Seze, J.; Leppert, D.; Montalban, X. Ofatumumab versus Teriflunomide in Multiple Sclerosis. N. Engl. J. Med. 2020, 383, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Bar-Or, A.; Grove, R.A.; Austin, D.J.; Tolson, J.M.; VanMeter, S.A.; Lewis, E.W.; Derosier, F.J.; Lopez, M.C.; Kavanagh, S.T.; Miller, A.E. Subcutaneous Ofatumumab in Patients with Relapsing-Remitting Multiple Sclerosis: The MIRROR Study. Neurology 2018, 90, e1805–e1814. [Google Scholar] [CrossRef] [PubMed]
- Kira, J.; Nakahara, J.; Sazonov, D.V.; Kurosawa, T.; Tsumiyama, I.; Willi, R.; Zalesak, M.; Pingili, R.; Häring, D.A.; Ramanathan, K. Effect of Ofatumumab versus Placebo in Relapsing Multiple Sclerosis Patients from Japan and Russia: Phase 2 APOLITOS Study. Mult. Scler. J. 2022, 28, 1229–1238. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Hauser et al. (2020) [11] | Bar-or et al. (2018) [12] | Kira et al. (2021) [13] | |
|---|---|---|---|---|
| Names | ASCLEPIOS I | ASCLEPIOS II | MIRROR Trial (OMS112831) | APOLITOS Study |
| Study type | Randomized, double-blind, double-dummy, parallel-group study (NCT02792218) | Randomized, double-blind, double-dummy, parallel-group study (NCT02792231) | Phase 2, randomized, double-blind, placebo-controlled, parallel-group, dose-ranging study (NCT01457924) | Phase 2, randomized, double-blind, placebo-controlled, parallel-group, multicenter study (NCT03249714) |
| Arms | Ofatumumab vs. active comparator (Teriflunomide)/placebo on days 1, 7, 14, week 4 and every 4 weeks thereafter | Ofatumumab every 4 or 12 weeks vs. placebo for a 24 week period | Randomized (2:1) to ofatumumab or matching placebo | |
| Intervention arm sample size | N = 465 | N = 481 | N = 164 | N = 43 |
| Control arm sample size | N = 462 | N = 474 | N = 67 | N = 21 |
| Duration of intervention and follow-up | Up to 2.5 years | 6 months, with follow-up until 12 months | 6 months, with follow-up until 12 months | |
| Country | Argentina, Australia, Belgium, Bulgaria, Canada, Croatia, Czechia, Denmark, Estonia, France, Germany, Greece, Hungary, India, Israel, Italy, Mexico, Netherlands, Poland, Puerto Rico, Russian Federation, Slovakia, Spain, Sweden, Switzerland, Thailand, Turkey, United Kingdom, United States | Argentina, Australia, Austria, Belgium, Bulgaria, Canada, Croatia, Czechia, Finland, France, Germany, Hungary, India, Italy, Latvia, Lithuania, Mexico, Norway, Peru, Poland, Portugal, Russian Federation, Slovakia, South Africa, Spain, Switzerland, Taiwan, Turkey, United Kingdom, United States | Bulgaria, Canada, Czechia, Denmark, Germany, Italy, Netherlands, Norway, Russian Federation, Spain, United States | Japan and Russia |
| Year | 20 September 2016–5 July 2019 | 26 August 2016–10 July 2019 | 1 November 2011–23 August 2013 | 15 March 2018–26 December 2019 |
| Primary outcome measure | To identify the annualized relapse rate in different arms at baseline up to 2.5 years | To identify the cumulative number of new gadolinium-enhancing (GdE) brain lesions at week 12 (based on T1-weighted MRI scans at weeks 4, 8, and 12) | To identify the number of gadolinium-enhancing T1 lesions per scan over 24 weeks | |
| Secondary outcome measure(s) | To identify the (i) disability worsening at 3 months or 6 months, (ii) disability improvement at 6 months, (iii) the number of gadolinium-enhancing lesions per T1-weighted magnetic resonance imaging scan, (iv) the annualized rate of new or enlarging lesions on T2-weighted MRI, (v) serum neurofilament light chain levels at month 3, and (vi) change in brain volume | To identify the (i) cumulative number of new GdE lesions at week 24, (ii) cumulative number and total volume of new and new plus persisting GdE lesions, (iii) new and/or newly enlarging T2 lesions, and (iv) T1-hypointense lesions at weeks 12 and 24 | To identify the (i) number of gadolinium-enhancing T1 lesions per MRI Scan (Japan vs. Non-Japan), (ii) number of new or enlarging T2 lesions on MRI Scans (annualized T2 lesion rate), (iii) annualized relapse rate (ARR), (iv) pharmacokinetic (PK) concentrations of ofatumumab, (v) B-cell counts | |
| Key inclusion criteria | (I) Diagnosis of MS; (II) Relapsing MS: relapsing–remitting MS (RRMS) or secondary progressive MS (SPMS); (III) At least one relapse during the previous 1 year or two relapses during the previous 2 years, or a positive gadolinium-enhancing MRI scan in the previous year; (IV) Expanded disability status scale (EDSS) score of 0 to 5.5; (V) Neurologically stable within 1 month prior to randomization | (I) Definite diagnosis of MS according to the 2010 revisions of the McDonald diagnostic criteria for MS; (II) No manifestation of another type of MS other than RRMS; (III) Expanded Disability Status Scale (EDSS) score of 0–5.5 (inclusive) at screening; (IV) Neurologically stable with no evidence of relapse for at least 30 days prior | (I) Diagnosis of multiple sclerosis (MS); (II) Relapsing MS; (III) At least one appearance of a new neurological abnormality or worsening of pre-existing neurological abnormality during the previous 2 years prior to screening AND an MRI activity (Gd-enhancing T1 lesions or new or enlarging T2 lesions) in the brain during the previous 1 year prior to randomization; (IV) EDSS score of 0 to 5.5 | |
| Intervention | Ofatumumab on days 1, 7, 14, week 4 and every 4 weeks thereafter OR placebo taken orally once daily OR teriflunomide taken once daily OR matching placebo of ofatumumab on days 1, 7, 14, week 4 and every 4 weeks thereafter | One dose of ofatumumab 3 mg over 24 weeks OR two doses of ofatumumab 3 mg over 24 weeks OR two doses of ofatumumab 30 mg over 24 weeks OR conditioning dose of ofatumumab 3 mg at randomization, two doses of ofatumumab 30 mg over 24 weeks OR two doses of ofatumumab 60 mg over 24 weeks OR conditioning dose of ofatumumab 3 mg at randomization, two doses of ofatumumab 60 mg over 24 weeks OR six doses of ofatumumab 60 mg over 24 weeks | Ofatumumab on Days 1,7, 14 and every 4 weeks for 24 weeks; all extension patients received dose every 4 weeks up to week 48. | |
| Author, Year | Hauser et al. (2020) [11] | Bar-or et al. (2018) [12] | Kira et al. (2021) [13] | |
|---|---|---|---|---|
| Names | ASCLEPIOS I | ASCLEPIOS II | MIRROR Trial (OMS112831) | APOLITOS Study |
| Dose and Mode of Administration | Ofatumumab 20 mg pre-filled syringes for subcutaneous injection OR placebo capsule OR teriflunomide 14 mg oral capsule OR matching placebo of ofatumumab subcutaneous injections | 3 mg OR 30 mg OR 60 mg, subcutaneous | 20 mg, (50 mg/mL, 0.4 mL content), subcutaneous | |
| Age (Mean SD) | 38.9 (8.77) vs. 37.8 (8.95) | 38.0 (9.28) vs. 38.2 (9.47) | 37.2 (9.39) vs. 37.7 (9.38) | 35.0 (9.49) vs. 35.5 (8.93) |
| Female (n, %) | 318/465 (68.4%) vs. 317/470 (68.6%) | 319 (66.3%) vs. 319 (67.3%) | 109/164 vs. 46/67 | 36 vs. 19 |
| Race (n, %) | Asian: 21 vs. 19; Black or African American: 15 vs. 20; White: 411 vs. 412; Other/Unknown: 24 vs. 14 | Asian: 21 vs. 19; Black or African American: 13 vs. 18; White: 418 vs. 417; Other/Unknown: 29 vs. 20 | White: 160/164 vs. 65/67 | Asian: 21 vs. 22; White: 22 vs. 10 |
| Gadolinium-enhancing T1 Lesions on MRI Scan at Endline (Mean, SD) | 0.0115 (SD = 0.33) (N = 432) vs. 0.4555 (SD = 1.15) (N = 420) | 0.0317 (SD = 0.14) (N = 438) vs. 0.5172 (SD = 1.36) (N = 433) | [Ofatumumab 3 mg q12w = 1.2 (1.94) N = 33; Ofatumumab 30 mg q12w = 2.3 (3.94) N = 30; Ofatumumab 60 mg q12w = 1.8 (3.31) N = 33; Ofatumumab 60 mg q4w = 1.8 (4.81) N = 63] vs. Placebo/Ofatumumab 3 mg = 3.2 (7.41) N = 67 | 0.0670 (SD = 0.21) (N = 39) vs. 1.0413 (SD = 1.99) (N = 20) |
| Relapse Rate at Treatment Endpoint (n/N) | 85/454 vs. 148/451 | 77/469 vs. 154/470 | 25/164 vs. 17/67 | 5/40 vs. 6/19 |
| No. | NCT Number | Title | Phase | Enrollment |
|---|---|---|---|---|
| 1 | NCT05199571 | Study of Efficacy and Safety of Ofatumumab in Relapsing Multiple Sclerosis (RMS) Patients in China | Phase 4 | 100 |
| 2 | NCT04486716 | A Single-Arm Study Evaluating the Efficacy, Safety and Tolerability of Ofatumumab in Patients with Relapsing Multiple Sclerosis (OLIKOS) | Phase 3 | 100 |
| 3 | NCT03650114 | Long-Term Safety, Tolerability and Effectiveness Study of Ofatumumab in Patients with Relapsing MS (ALITHIOS) | Phase 3 | 2010 |
| 4 | NCT04353492 | An Open-Label Study Evaluating Ofatumumab Treatment Effectiveness and PROs in Subjects with RMS Transitioning from Fumarate-based RMS Approved Therapies or Fingolimod to Ofatumumab (ARTIOS) | Phase 3 | 555 |
| 5 | NCT04510220 | Nine-Month Study to Assess the Efficacy of Ofatumumab on Microglia in Patients with Relapsing Forms of Multiple Sclerosis | Phase 3 | 10 |
| 6 | NCT04667117 | A Multicenter Study to Assess Response to Influenza Vaccine in Multiple Sclerosis Participants Treated with Ofatumumab | Phase 4 | 66 |
| 7 | NCT04869358 | Exploring the Immune Response to SARS-CoV-2 COVID-19 Vaccines in Patients with Relapsing Multiple Sclerosis (RMS) Treated with Ofatumumab (KYRIOS) | Phase 4 | 34 |
| 8 | NCT04047628 | Best Available Therapy Versus Autologous Hematopoetic Stem Cell Transplant for Multiple Sclerosis (BEAT-MS) | Phase 3 | 156 |
| 9 | NCT05084638 | Study to Assess the Effect of Ofatumumab in Treatment Naive, Very Early RRMS Patients Benchmarked Against Healthy Controls (AGNOS) | Phase 4 | 168 |
| 10 | NCT05090371 | A Multicenter Study of Continued Current Therapy vs. Transition to Ofatumumab After Neurofilament (NfL) Elevation (SOSTOS) | Phase 4 | 150 |
| 11 | NCT04926818 | Efficacy and Safety of Ofatumumab and Siponimod Compared to Fingolimod in Pediatric Patients with Multiple Sclerosis (NEOS) | Phase 3 | 180 |
| 12 | NCT04788615 | Open Label Randomized Multicenter to Assess Efficacy & Tolerability of Ofatumumab 20 mg vs. First Line DMT in RMS (STHENOS) | Phase 3 | 236 |
| 13 | NCT03500328 | Traditional Versus Early Aggressive Therapy for Multiple Sclerosis Trial (TREAT-MS) | Not Applicable | 900 |
| 14 | NCT03535298 | Determining the Effectiveness of Early Intensive Versus Escalation Approaches for RRMS (DELIVER-MS) | Phase 4 | 800 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taj, H.M.; Talib, M.; Siddiqa, S.; Sarfraz, A.; Sarfraz, Z.; Robles-Velasco, K.; Cherrez-Ojeda, I. What Do We Know So Far about Ofatumumab for Relapsing Multiple Sclerosis? A Meta-Analytical Study. Healthcare 2022, 10, 2199. https://doi.org/10.3390/healthcare10112199
Taj HM, Talib M, Siddiqa S, Sarfraz A, Sarfraz Z, Robles-Velasco K, Cherrez-Ojeda I. What Do We Know So Far about Ofatumumab for Relapsing Multiple Sclerosis? A Meta-Analytical Study. Healthcare. 2022; 10(11):2199. https://doi.org/10.3390/healthcare10112199
Chicago/Turabian StyleTaj, Hafiza Munazza, Maryam Talib, Sania Siddiqa, Azza Sarfraz, Zouina Sarfraz, Karla Robles-Velasco, and Ivan Cherrez-Ojeda. 2022. "What Do We Know So Far about Ofatumumab for Relapsing Multiple Sclerosis? A Meta-Analytical Study" Healthcare 10, no. 11: 2199. https://doi.org/10.3390/healthcare10112199