
Simulation Training Needs of Nurses for Nursing High-Risk Premature Infants: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Research Participants
2.3. Research Tool
2.3.1. The Importance of Nursing High-Risk Premature Babies
2.3.2. Performance in Nursing High-Risk Premature Babies
2.3.3. Importance-Performance Analysis (IPA) for Nursing High-Risk Premature Babies
2.3.4. Analysis of Nursing Training Needs for High-Risk Premature Babies
2.3.5. Priority Analysis of Nursing Training Needs for High-Risk Premature Babies
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. General Characteristics of Participants
3.2. Differences in the Importance of and Performance in Neonatal Intensive Care According to General Characteristics
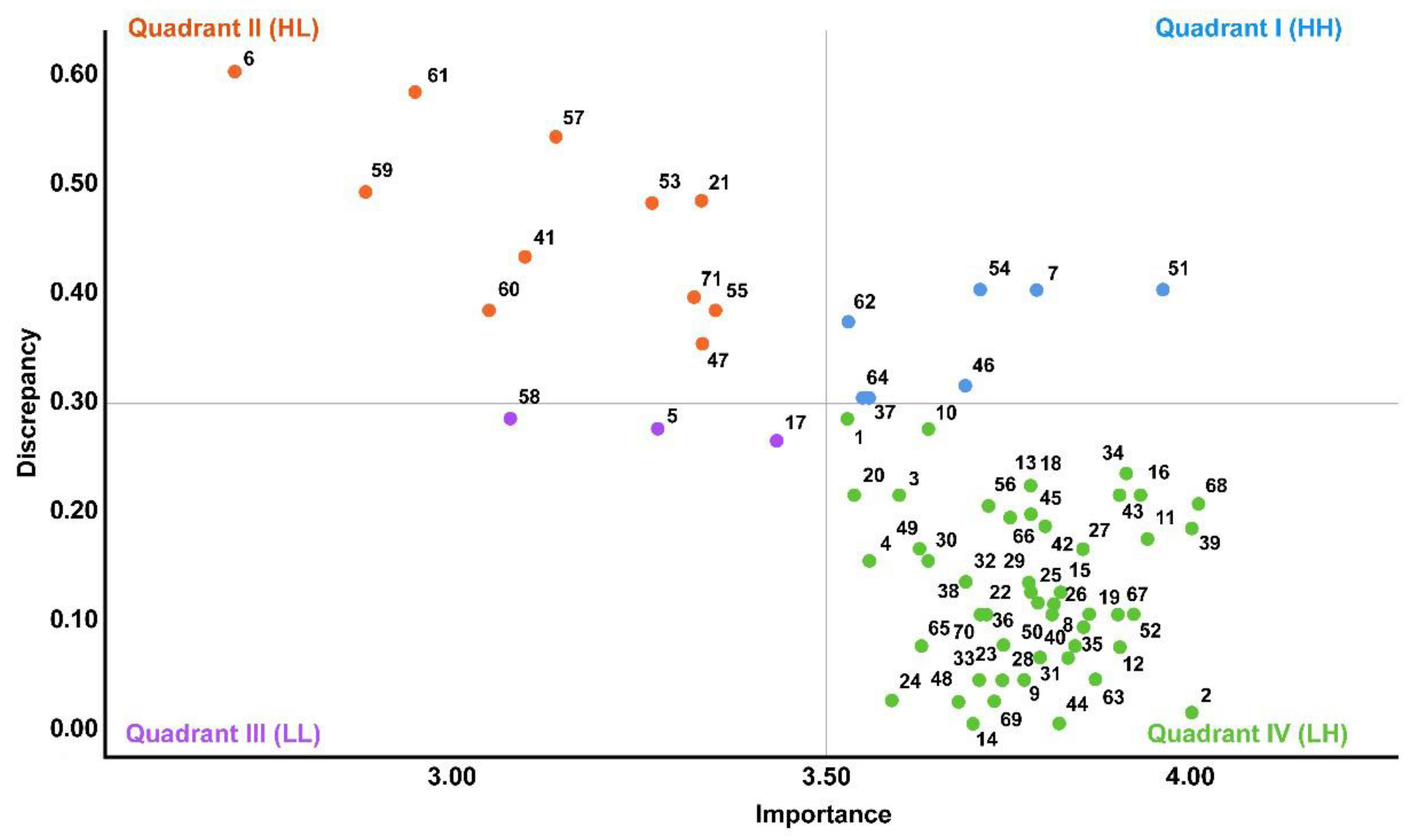
3.3. Importance-Performance Analysis (IPA) for Nursery and NICU Nurses in Nursing High-Risk Premature Babies
3.4. Borich Analysis of Nursing Training Needs for High-Risk Premature Infants in NICU Nurses
3.5. Locus for Focus Model Analysis on the Nursing of High-Risk Premature Infants by NICU Nurses
3.6. Deriving Priorities in the Nursing Training Needs for High-Risk Premature Infants
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.; Lee, H.; Kim, E.; Kim, H.; Jang, E. Analysis of the importance of nursing care and performance confidence perceived by nurses in the neonatal intensive care unit. J. Korean Acad. Soc. Nurs. Educ. 2022, 28, 5–14. [Google Scholar] [CrossRef]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Zamani, P.; Dehnad, A.; Haghani, H.; Borimnejad, L. Effect of web-based education on knowledge, attitude, and practice of nurses in neonatal intensive care unit. Interdiscip. J. Virtual Learn. Med. Sci. 2019, 10, 10–20. [Google Scholar] [CrossRef]
- Boskabadi, H.; Mamoori, G.; Khatami, S.F.; Faramarzi, R. Serum level of vitamin D in preterm infants and its association with premature-related respiratory complications: A case-control study. Electron. Physician 2018, 10, 6208–6214. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.; Bamber, D.; Bountziouka, V.; Clayton, S.; Cragg, L.; Gilmore, C. Improving developmental and educational support for children born preterm: Evaluation of an e-learning resource for education professionals. BMJ Open 2019, 9, e029720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cengiz, Z.; Gurdap, Z.; Işik, K. Challenges experienced by nursing students during the COVID-19 pandemic. Perspect. Psychiatr. Care 2022, 58, 47–53. [Google Scholar] [CrossRef]
- Kim, M.; Kim, S. Development and effects a simulation-based emergency airway management education program for nurses in a neonatal intensive care unit. Child Health Nurs. Res. 2019, 25, 518–527. [Google Scholar] [CrossRef]
- Shaw, C.; Gallagher, K.; Petty, J.; Mancini, A.; Boyle, B. Neonatal nursing during the COVID-19 global pandemic: A thematic analysis of personal reflections. J. Neonatal Nurs. 2021, 27, 165–171. [Google Scholar] [CrossRef]
- Prullage, G.S.; Kenner, C.; Uwingabire, F.; Ndayambaje, A.; Boykova, M.; Walker, K. Survey of neonatal nursing: Staffing, education, and equipment availability in Rwanda. J. Neonatal Nurs. 2022, 28, 192–199. [Google Scholar] [CrossRef]
- Taghinejad, F.; Nikfarid, L.; Monfared, M.N.; Hoseini, N.; Habibi, S. Nursing diagnoses of preterm infants in the neonatal intensive care unit: A cross sectional study. J. Neonatal Nurs. 2021, 27, 451–458. [Google Scholar] [CrossRef]
- Huang, J.; Tang, Y.; Tang, J.; Shi, J.; Wang, H.; Xiong, T.; Xia, B.; Zhang, L.; Qu, Y.; Mu, D. Educational efficacy of high-fidelity simulation in neonatal resuscitation training: A systematic review and meta-analysis. BMC Med. Educ. 2019, 19, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricci, S.; Mobilio, G.A.; Calandrino, A.; Pescio, M.; Issa, E.; Rossi, P.; Chessa, M.; Solari, F.; Chirico, M.; Casadio, M. RiNeo MR: A mixed-reality tool for newborn life support training. In Proceedings of the 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 5043–5046. [Google Scholar] [CrossRef]
- Zhao, S.; Xiao, X.; Wang, Q.; Zhang, X.; Li, W.; Soghier, L.; Hahn, J. An intelligent augmented reality training framework for neonatal endotracheal intubation. In Proceedings of the International Symposium on Mixed and Augmented Reality IEEE International Symposium on Mixed and Augmented Reality (ISMAR), Porto de Galinhas, Brazil, 9–13 November 2020; pp. 672–681. [Google Scholar] [CrossRef]
- Park, S.J.; Ji, E.S. Clinical competence according to experiences on the neonatal nursing care in nursing students and educational needs of the nursing simulation. J. Learn. Cent. Curric. Instr. 2016, 16, 97–112. [Google Scholar]
- Yu, J.H.; Chang, H.J.; Kim, S.S.; Park, J.E.; Chung, W.Y.; Lee, S.K.; Kim, M.; Lee, J.H.; Jung, Y.J. Effects of high-fidelity simulation education on medical students’ anxiety and confidence. PLoS ONE 2021, 16, e0251078. [Google Scholar] [CrossRef] [PubMed]
- Ji, E.A. Educational needs in the development of simulation-based program on extremely low birth weight infants nursing care for nurses in the neonatal care unit. J. Korea Soc. Simul. Nurs. 2020, 8, 17–29. [Google Scholar] [CrossRef]
- Alreshidi, N.M.; Garcia, M.; Al Aseeri, R.M.; Al Reshedi, T.M. Assessing the impact of nursing training on patient safety in neonatal intensive care unit at maternity and Children’s Hospital in the K.S.A. J. Nurs. Educ. Pract. 2020, 10, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Mbekenga, C.; Pallangyo, E.; Mwansisya, T.; Isangula, K.; Mwasha, L. Training needs assessment of health care professionals in reproductive, maternal and newborn health in a low-income setting in Tanzania. J. Nurs. Sci. Pract. Res. Square 2020, 11, 1–20. [Google Scholar] [CrossRef]
- Rahimi, R.; Javed, Z.; Abbas, K.; Khan, B.A.A.; Kauser, N.; Soomro, R. Impact of training on nurses performance and productivity at Neonatal Intensive Care Unit (NICU). JOJ Nurs. Health Care 2018, 9, 555758. [Google Scholar] [CrossRef]
- Martilla, J.A.; James, J.C. Importance-performance analysis. J. Mark. 1977, 41, 77–79. [Google Scholar] [CrossRef]
- Borich, G.D. A needs assessment model for conducting follow-up studies. J. Teach. Educ. 1980, 31, 39–42. [Google Scholar] [CrossRef]
- Mink, O.G.; Shultz, J.M.; Mink, B.P.; Formosa, A.R. Developing and Managing Open Organizations: A Model and Method for Maximizing Organizational Potential; Somerset Consulting Group: Austin, TX, USA, 1991. [Google Scholar]
- Holloway, K.; Arcus, K.; Orsborn, G. Training needs analysis: The essential first step for continuing professional development design. Nurse Educ. Pract. 2018, 28, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.M. Educational needs analysis for developing an occupational education program for nursing students: Focusing on nursing students and nursing professionals. Korean J. Adult Nurs. 2018, 30, 136–148. [Google Scholar] [CrossRef] [Green Version]
- Shin, D.A.; Bang, K.S. Analysis of the educational needs of nurses in the neonatal intensive care unit for developmental supportive care. J. Korean Acad. Soc. Nurs. Educ. 2021, 27, 261–273. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Park, S.N.; Kim, Y.; Im, Y.S. Educational needs assessment in pediatric nursing handoff for nursing students. Child Health Nurs. Res. 2015, 21, 204–215. [Google Scholar] [CrossRef]
- Yu, M.; Kim, D.Y.; Yoo, C. Development of Korean patient classification system for neonatal care nurses. J. Korean Clin. Nurs. Res. 2016, 22, 205–216. [Google Scholar] [CrossRef]
- Park, K.O.; Lee, Y.Y. Developing a performance appraisal tool for neonatal intensive care unit registered nurses. J. Korean Acad. Soc. Nurs. Educ. 2011, 17, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Hong, H.; Son, H.M. Factors influencing developmental care performance among neonatal intensive care units nurses. Child Health Nurs. Res. 2020, 26, 131–139. [Google Scholar] [CrossRef]
- Karami, A.; Farokhzadian, J.; Foroughameri, G. Nurses’ professional competency and organizational commitment: Is it important for human resource management? PLoS ONE 2017, 12, e0187863. [Google Scholar] [CrossRef]
- Poorchangizi, B.; Farokhzadian, J.; Abbaszadeh, A.; Mirzaee, M.; Borhani, F. The importance of professional values from clinical nurses’ perspective in hospitals of a medical university in Iran. BMC Med. Ethics 2017, 18, 20. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.S. Moving forward to improve safety and quality of neonatal intensive care in Korea. J. Korean Med. 2018, 33, e89. [Google Scholar] [CrossRef] [PubMed]
- Farzi, S.; Shahriari, M.; Farzi, S. Exploring the challenges of clinical education in nursing and strategies to improve it: A qualitative study. J. Educ. Health Promot. 2018, 7, 115. [Google Scholar] [CrossRef] [PubMed]
- Kuraoka, Y. Effect of an experiential learning-based programme to foster competence among nurse managers. J. Nurs. Manag. 2018, 26, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Ali, W. Online and remote learning in higher education institutes: A necessity in light of COVID-19 pandemic. High Educ. Stud. 2020, 10, 16–25. [Google Scholar] [CrossRef]
- Islam, M.S.; Rahman, K.M.; Sun, Y.; Qureshi, M.O.; Adbi, I.; Chughtai, A.A.; Seale, H. Current knowledge of COVID-19 and infection prevention and control strategies in healthcare settings: A global analysis. Infect. Control Hosp. Epidemiol. 2020, 41, 1196–1206. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Categories | n (%) | Importance | t or F | p-Value | Performance | t or F | p-Value |
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||||||
| Age group (years) | 20s | 12 (12.1) | 3.75 (0.48) a | 9.87 | <0.001 | 3.76 (0.53) a | 10.35 | <0.001 |
| 30s | 68 (68.7) | 3.48 (0.45) b | c, d > b | 3.59 (0.61) b | c > a, b, d | |||
| 40s | 13 (13.1) | 4.08 (0.59) c | (Scheffé) | 4.47 (0.51) c | (Scheffé) | |||
| 50s | 6 (6.1) | 4.22 (0.30) d | 4.33 (0.44) d | |||||
| Final academic degree | Bachelor | 82 (82.8) | 3.53 (0.47) | −4.69 | <0.001 | 3.63 (0.60) | −5.36 | <0.001 |
| Master | 17 (17.2) | 4.13 (0.52) | 4.46 (0.46) | |||||
| Clinical experience (years) | More than 1~less than 3 | 2 (2.0) | 3.43 (0.17) | 14.67 | <0.001 | 3.43 (0.33) | 19.284 | <0.001 |
| More than 3~less than 5 | 5 (5.1) | 3.42 (0.50) | b > a | 3.69 (0.52) | b > a | |||
| More than 5~less than 7 | 52 (52.5) | 3.40 (0.31) a | (Scheffé) | 3.42 (0.40) a | (Scheffé) | |||
| More than 7 | 40 (40.4) | 4.00 (0.57) b | 4.25 (0.66) b | |||||
| Clinical experience in the nursery/NICU (year) | less than 1 | 3 (3.0) | 3.50 (0.17) a | 15.61 | <0.001 | 3.67 (0.48) a | 17.74 | <0.001 |
| More than 1~less than 3 | 22 (22.2) | 3.54 (0.44) b | e > a, b, c, d | 3.61 (0.57) b | e > a, b, c, d | |||
| More than 3~less than 5 | 33 (33.3) | 3.39 (0.27) c | (Scheffé) | 3.46 (0.43) c | (Scheffé) | |||
| More than 5~less than 7 | 17 (17.2) | 3.48 (0.41) d | 3.52 (0.53) d | |||||
| More than 7 | 24 (24.3) | 4.21 (0.55) e | 4.52 (0.53) e | |||||
| Number of assigned patients | 1~3 | 62 (62.6) | 3.70 (0.56) | 1.36 | 0.177 | 3.85 (0.68) | 1.72 | 0.089 |
| More than 4 | 37 (37.4) | 3.55 (0.44) | 3.63 (0.60) | |||||
| Working unit | Nursery | 45 (45.5) | 3.38 (0.26) | −5.26 | <0.001 | 3.39 (0.35) | −6.45 | <0.001 |
| NICU | 54 (54.5) | 3.85 (0.59) | 4.08 (0.69) | |||||
| Experience in clinical nursing training for high-risk premature infants | Yes | 90 (90.9) | 3.62 (0.52) b | −1.04 | 0.300 | 3.81 (0.53) | 3.40 | 0.069 |
| No | 9 (9.1) | 3.81 (0.51) | 3.70 (0.63) | |||||
| Training site for the clinical nursing of high-risk premature infants † | On-site | 48 (53.3) | 3.69 (0.57) | 1.29 | 0.199 | 3.76 (0.65) | 0.97 | 0.336 |
| Off-site | 42 (46.7) | 3.55 (0.47) | 3.63 (0.61) | |||||
| High-risk preterm infant clinical nursing Training method for the clinical nursing of high-risk premature infants † | Lecture | 29 (32.2) | 3.99 (0.61) a | 11.18 | <0.001 | 3.85 (0.65) | 18.13 | 0.121 |
| Simulation | 27 (30.0) | 3.57 (0.42) b | a > b, c, d | 3.59 (0.51) | ||||
| Case-based learning | 24 (26.7) | 3.35 (0.31) c | (Scheffé) | 3.33 (0.35) | ||||
| Problem-based learning | 10 (11.1) | 3.33 (0.24) d | 3.31 (0.24) | |||||
| Desired training site | On-site | 66 (66.7) | 3.58 (0.47) | −1.41 | 0.164 | 3.71 (0.62) | −1.10 | 0.274 |
| Off-site | 33 (33.3) | 3.75 (0.61) | 3.88 (0.73) | |||||
| Confidence in clinical nursing for high-risk premature infants | Lack | 4 (4.0) | 3.75 (0.09) | 0.13 | 0.876 | 3.77 (0.28) | 0.01 | 0.993 |
| Moderate | 26 (26.3) | 3.61 (0.46) | 3.76 (0.66) | |||||
| High | 69 (69.7) | 3.64 (0.52) | 3.77 (0.68) | |||||
| Need XR training on neonatal care | Yes | 96 (97.0) | 4.34 (0.51) | −2.40 | 0.018 | 3.81 (0.17) | −1.31 | 0.121 |
| No | 3 (3.0) | 3.62 (0.52) | 3.74 (0.65) |
| No. | Contents | Importance | Performance | Gap | Paired t-Test | p-Value | Borich Needs | Rank |
|---|---|---|---|---|---|---|---|---|
| Total | 3.78 (0.67) | 3.69 (0.57) | 0.09 (0.29) | 3.31 | 0.001 | 3.63 | ||
| Monitoring and measuring | 3.71 (0.68) | 3.56 (0.50) | 0.15 (0.43) | 3.45 | 0.001 | 0.56 | 2 | |
| 1 | Measurement of body temperature, respiration, and heart rate | 3.81 (1.27) | 3.53 (1.37) | 0.28 (1.20) | 2.35 | 0.021 | 1.07 | 19 |
| 2 | Device monitoring | 4.01 (0.97) | 4.00 (0.98) | 0.01 (1.04) | 0.10 | 0.928 | 0.04 | 69 |
| 3 | Invasive pressure monitoring | 3.81 (1.35) | 3.60 (1.38) | 0.21 (1.79) | 1.18 | 0.240 | 0.80 | 30 |
| 4 | Monitoring others | 3.71 (1.11) | 3.56 (1.10) | 0.15 (1.40) | 1.08 | 0.283 | 0.56 | 41 |
| 5 | Installation of a monitor for pressure measurement | 3.55 (1.17) | 3.27 (1.12) | 0.27 (1.34) | 2.03 | 0.045 | 0.96 | 22 |
| 6 | Maintenance of IABP or ECMO | 3.28 (1.44) | 2.69 (1.38) | 0.60 (1.76) | 3.37 | 0.001 | 1.97 | 3 |
| 7 | Intake & output check | 3.79 (1.32) | 3.75 (1.34) | 0.40 (1.41) | 0.29 | 0.776 | 1.52 | 9 |
| 8 | Weighing high-risk premature infants | 3.85 (1.30) | 3.76 (1.28) | 0.09 (1.46) | 0.62 | 0.536 | 0.35 | 55 |
| 9 | Body measurements | 3.77 (1.17) | 3.73 (1.19) | 0.04 (1.14) | 0.35 | 0.726 | 0.15 | 64 |
| Physical examination and lab test | 3.82 (0.66) | 3.78 (0.62) | 0.04 (0.38) | 1.03 | 0.306 | 0.15 | 8 | |
| 10 | State of consciousness observation | 3.91 (1.15) | 3.64 (1.24) | 0.27 (1.41) | 1.92 | 0.058 | 1.06 | 20 |
| 11 | Auscultation and recording of breath and heart sounds | 4.11 (1.04) | 3.94 (1.06) | 0.17 (1.20) | 1.42 | 0.159 | 0.70 | 36 |
| 12 | Circulation/sensation/motion check | 3.90 (1.06) | 3.83 (1.16) | 0.07 (1.33) | 0.53 | 0.597 | 0.27 | 56 |
| 13 | Other circumstances (fall, pain, sores, sedation, etc.) | 3.91 (1.15) | 3.68 (1.26) | 0.23 (1.38) | 1.68 | 0.096 | 0.90 | 24 |
| 14 | Blood sugar test | 3.70 (1.27) | 3.70 (1.29) | 0.00 (1.45) | 0.00 | 1.000 | 0.00 | 70 |
| 15 | Emergency lab test (Stat) | 3.94 (1.10) | 3.82 (1.17) | 0.12 (1.15) | 1.05 | 0.299 | 0.47 | 44 |
| 16 | Collecting other samples (sputum, urine, feces, etc.) | 3.93 (1.10) | 3.72 (1.13) | 0.21 (1.18) | 1.79 | 0.077 | 0.83 | 27 |
| 17 | 3-lead ECG recording | 3.70 (1.15) | 3.43 (1.16) | 0.26 (1.42) | 1.84 | 0.068 | 0.96 | 21 |
| Respiratory care | 3.81 (0.78) | 3.70 (0.67) | 0.11 (0.42) | 2.55 | 0.012 | 0.42 | 5 | |
| 18 | Maintain O2 therapy | 4.00 (1.18) | 3.78 (1.18) | 0.22 (1.27) | 1.74 | 0.086 | 0.88 | 25 |
| 19 | Initiation and exchange O2 therapy | 3.86 (1.15) | 3.76 (1.27) | 0.10 (1.40) | 0.72 | 0.473 | 0.39 | 51 |
| 20 | Maintain NO therapy | 3.75 (1.26) | 3.54 (1.21) | 0.21 (1.72) | 1.23 | 0.223 | 0.79 | 31 |
| 21 | Initiation and exchange NO therapy | 3.82 (1.23) | 3.33 (1.22) | 0.48 (1.42) | 3.39 | 0.001 | 1.83 | 4 |
| 22 | Apnea care | 3.81 (1.29) | 3.71 (1.26) | 0.10 (1.33) | 0.76 | 0.451 | 0.38 | 53 |
| 23 | Chest physiotherapy | 3.81 (1.16) | 3.74 (1.16) | 0.07 (1.40) | 0.50 | 0.617 | 0.27 | 57 |
| 24 | Apply nebulizer | 3.57 (1.20) | 3.59 (1.18) | 0.02 (1.45) | 0.14 | 0.890 | 0.07 | 68 |
| 25 | Airway aspiration | 3.90 (1.20) | 3.78 (1.18) | 0.12 (1.23) | 0.98 | 0.330 | 0.47 | 45 |
| 26 | Maintaining ventilator (invasive and non-invasive) | 3.91 (1.17) | 3.81 (1.18) | 0.10 (1.40) | 0.72 | 0.476 | 0.39 | 49 |
| 27 | Ventilator setting and application | 4.01 (1.18) | 3.85 (1.13) | 0.16 (1.34) | 1.20 | 0.232 | 0.64 | 38 |
| 28 | Intubation | 3.78 (1.33) | 3.74 (1.16) | 0.04 (1.53) | 0.26 | 0.793 | 0.15 | 63 |
| 29 | Extubation | 3.78 (1.16) | 3.65 (1.21) | 0.13 (1.47) | 0.89 | 0.376 | 0.49 | 43 |
| 30 | Artificial airway (endotracheal tube) care | 3.79 (1.26) | 3.64 (1.13) | 0.15 (1.33) | 1.14 | 0.259 | 0.57 | 40 |
| Mobility | 3.85 (1.00) | 3.76 (1.07) | 0.10 (1.13) | 0.84 | 0.402 | 0.39 | 6 | |
| 31 | Position change | 3.89 (1.18) | 3.83 (1.32) | 0.06 (1.35) | 0.45 | 0.657 | 0.23 | 60 |
| 32 | Rehabilitation | 3.82 (1.17) | 3.69 (1.20) | 0.13 (1.50) | 0.87 | 0.385 | 0.50 | 42 |
| Hygiene and infection control | 3.79 (0.78) | 3.76 (0.79) | 0.03 (0.11) | 0.60 | 0.547 | 0.11 | 10 | |
| 33 | Bathing | 3.75 (1.24) | 3.71 (1.26) | 0.04 (1.40) | 0.29 | 0.774 | 0.15 | 65 |
| 34 | Exchange linen | 3.68 (1.18) | 3.91 (1.16) | 0.23 (1.34) | 1.73 | 0.087 | 0.85 | 26 |
| 35 | Incubator management | 3.77 (1.21) | 3.84 (1.27) | 0.07 (1.37) | 0.51 | 0.609 | 0.26 | 58 |
| 36 | Contact quarantine and counter-isolation nursing | 3.90 (1.17) | 3.79 (1.22) | 0.11 (1.26) | 0.88 | 0.383 | 0.43 | 48 |
| 37 | Droplet and air containment nursing | 3.86 (1.16) | 3.56 (1.31) | 0.30 (1.52) | 1.98 | 0.050 | 1.16 | 17 |
| Feeding | 3.89 (1.11) | 3.86 (1.04) | 0.03 (0.50) | 0.31 | 0.758 | 0.12 | 9 | |
| 38 | Gavage-tube feeding | 3.90 (1.22) | 3.78 (1.36) | 0.12 (1.28) | 0.94 | 0.348 | 0.47 | 46 |
| 39 | Bottle feeding | 4.00 (1.17) | 3.82 (1.18) | 0.18 (1.27) | 1.43 | 0.156 | 0.72 | 35 |
| Elimination | 3.66 (0.82) | 3.56 (0.70) | 0.10 (0.85) | 1.22 | 0.224 | 0.37 | 7 | |
| 40 | Diaper change | 3.85 (1.16) | 3.79 (1.22) | 0.06 (1.25) | 0.48 | 0.631 | 0.23 | 61 |
| 41 | Nelaton catheterization | 3.53 (1.24) | 3.09 (1.22) | 0.43 (1.55) | 2.78 | 0.006 | 1.52 | 8 |
| 42 | Enema | 3.80 (1.20) | 3.62 (1.21) | 0.18 (1.55) | 1.17 | 0.245 | 0.68 | 37 |
| Medication and transfusion | 3.81 (0.79) | 3.69 (0.63) | 0.12 (0.54) | 2.18 | 0.032 | 0.46 | 4 | |
| 43 | Insert IV route or arterial line | 3.90 (1.01) | 3.69 (1.28) | 0.21 (1.25) | 1.69 | 0.094 | 0.82 | 28 |
| 44 | Continuous fluid infusion via infusion/syringe pump | 3.82 (1.26) | 3.82 (1.18) | 0.00 (1.26) | 0.00 | 1.000 | 0.00 | 71 |
| 45 | Intravenous injection | 3.97 (1.18) | 3.78 (1.23) | 0.19 (1.38) | 1.38 | 0.170 | 0.75 | 33 |
| 46 | Blood transfusion | 4.00 (1.20) | 3.69 (1.20) | 0.31 (1.54) | 2.02 | 0.046 | 1.24 | 16 |
| 47 | Exchange transfusion | 3.69 (1.14) | 3.33 (1.27) | 0.35 (1.68) | 2.09 | 0.039 | 1.29 | 15 |
| 48 | surfactant administration (Intratracheal) | 3.70 (1.24) | 3.68 (1.19) | 0.02 (1.57) | 0.13 | 0.898 | 0.07 | 67 |
| 49 | Non-intravenous medication | 3.79 (1.26) | 3.63 (1.24) | 0.16 (1.39) | 1.16 | 0.250 | 0.61 | 39 |
| Treatment and procedure | 3.70 (0.66) | 3.43 (0.54) | 0.27 (0.67) | 4.06 | <0.001 | 1.00 | 1 | |
| 50 | Tube insertion | 3.92 (1.22) | 3.81 (1.21) | 0.11 (1.50) | 0.74 | 0.462 | 0.43 | 47 |
| 51 | Simple dressing | 3.96 (1.07) | 3.92 (1.08) | 0.40 (1.25) | 0.32 | 0.747 | 1.58 | 7 |
| 52 | Tube irrigation and instillation | 3.71 (1.26) | 3.92 (1.08) | 0.10 (1.23) | 1.71 | 0.090 | 0.37 | 54 |
| 53 | Prepare puncture | 3.75 (1.15) | 3.26 (1.16) | 0.48 (1.50) | 3.21 | 0.002 | 1.80 | 5 |
| 54 | Maintenance of various tubes | 3.71 (1.18) | 3.68 (1.19) | 0.40 (1.41) | 0.29 | 0.776 | 1.48 | 10 |
| 55 | Complex dressing | 3.74 (1.22) | 3.35 (1.29) | 0.38 (1.56) | 2.44 | 0.016 | 1.42 | 13 |
| 56 | Phototherapy | 3.92 (1.12) | 3.72 (1.25) | 0.20 (1.28) | 1.57 | 0.119 | 0.78 | 32 |
| 57 | Preparing and nursing for tracheostomy insertion | 3.67 (1.26) | 3.13 (1.36) | 0.54 (1.88) | 2.84 | 0.005 | 1.98 | 2 |
| 58 | Observe intracranial pressure monitoring device | 3.35 (1.22) | 3.07 (1.27) | 0.28 (1.69) | 1.67 | 0.099 | 0.94 | 23 |
| 59 | Preparing for CRRT insertion | 3.36 (1.32) | 2.87 (1.37) | 0.49 (1.80) | 2.73 | 0.007 | 1.65 | 6 |
| 60 | CRRT maintenance care | 3.42 (1.28) | 3.04 (1.38) | 0.38 (1.68) | 2.28 | 0.025 | 1.30 | 14 |
| 61 | Perform peritoneal dialysis | 3.52 (1.35) | 2.94 (1.31) | 0.58 (1.77) | 3.24 | 0.002 | 2.04 | 1 |
| 62 | Therapeutic thermoregulation | 3.90 (1.11) | 3.53 (1.22) | 0.37 (1.45) | 2.56 | 0.012 | 1.44 | 12 |
| 63 | Other treatment and exam (X-ray, ultrasound, etc.) | 3.87 (1.22) | 3.83 (1.15) | 0.04 (1.29) | 0.31 | 0.755 | 0.15 | 62 |
| 64 | NRP | 3.85 (1.26) | 3.55 (1.25) | 0.30 (1.69) | 1.78 | 0.078 | 1.16 | 18 |
| Emotional support, communication, and education | 3.82 (1.05) | 3.69 (1.02) | 0.13 (1.02) | 1.28 | 0.205 | 0.50 | 3 | |
| 65 | Family Counseling | 3.70 (1.22) | 3.63 (1.34) | 0.07 (1.44) | 0.39 | 0.697 | 0.26 | 59 |
| 66 | Developmental supportive care | 3.94 (1.19) | 3.75 (1.03) | 0.19 (1.31) | 1.21 | 0.228 | 0.75 | 34 |
| Admission and discharge management | 3.77 (0.87) | 3.74 (0.71) | 0.03 (0.63) | 0.54 | 0.588 | 0.11 | 11 | |
| 67 | Admission | 3.90 (1.24) | 3.80 (1.24) | 0.10 (1.39) | 0.72 | 0.471 | 0.39 | 50 |
| 68 | Discharge | 4.01 (0.92) | 3.81 (1.29) | 0.20 (1.35) | 1.49 | 0.139 | 0.80 | 29 |
| 69 | Transfer preparation | 3.73 (1.31) | 3.71 (1.26) | 0.02 (1.46) | 0.14 | 0.891 | 0.07 | 66 |
| 70 | Discharge education (for caregiver) | 3.82 (1.21) | 3.72 (1.24) | 0.10 (1.32) | 0.76 | 0.449 | 0.38 | 52 |
| 71 | Care of the dying patient | 3.72 (1.23) | 3.32 (1.30) | 0.39 (1.68) | 2.34 | 0.021 | 1.45 | 11 |
| Domain | Item | Contents | IPA | Borich Needs | The Locus for Focus | Priority |
|---|---|---|---|---|---|---|
| MM | 6 | Maintenance of IABP or extracorporeal membrane oxygenator (ECMO) | LP | 3 | HL | 3 |
| 7 | Intake & output check | KU | 9 | HH | 2 | |
| RC | 21 | Initiation and exchange NO therapy | PO | 4 | HL | 3 |
| HIC | 37 | Droplet and air containment nursing | KU | 17 | HH | 2 |
| EM | 41 | Nelaton catheterization | LP | 8 | HL | 3 |
| MTTP | 46 | Blood transfusion | KU | 16 | HH | 2 |
| 47 | Exchange transfusion | LP | 15 | HL | 3 | |
| TP | 51 | Simple dressing | KU | 7 | HH | 2 |
| 53 | Prepare puncture | PO | 5 | HL | 3 | |
| 54 | Maintenance of various tubes | CH | 10 | HH | 1 | |
| 55 | Complex dressing | PO | 13 | HL | 3 | |
| 57 | Preparing and nursing for tracheostomy insertion | LP | 2 | HL | 3 | |
| 59 | Preparing for CRRT insertion | LP | 6 | HL | 3 | |
| 60 | CRRT maintenance care | LP | 14 | HL | 3 | |
| 61 | Perform peritoneal dialysis | LP | 1 | HL | 3 | |
| 62 | Therapeutic thermoregulation | KU | 12 | HH | 2 | |
| 64 | NRP | KU | 18 | HH | 2 | |
| ADM | 71 | Care of the dying patient | PO | 11 | HL | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.-Y. Simulation Training Needs of Nurses for Nursing High-Risk Premature Infants: A Cross-Sectional Study. Healthcare 2022, 10, 2197. https://doi.org/10.3390/healthcare10112197
Yang S-Y. Simulation Training Needs of Nurses for Nursing High-Risk Premature Infants: A Cross-Sectional Study. Healthcare. 2022; 10(11):2197. https://doi.org/10.3390/healthcare10112197
Chicago/Turabian StyleYang, Sun-Yi. 2022. "Simulation Training Needs of Nurses for Nursing High-Risk Premature Infants: A Cross-Sectional Study" Healthcare 10, no. 11: 2197. https://doi.org/10.3390/healthcare10112197