
Close Contacts, Infected Cases, and the Trends of SARS-CoV-2 Omicron Epidemic in Shenzhen, China

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Source of Data
2.2. Definitions of Infected Cases, Close Contacts, and Medical Observation
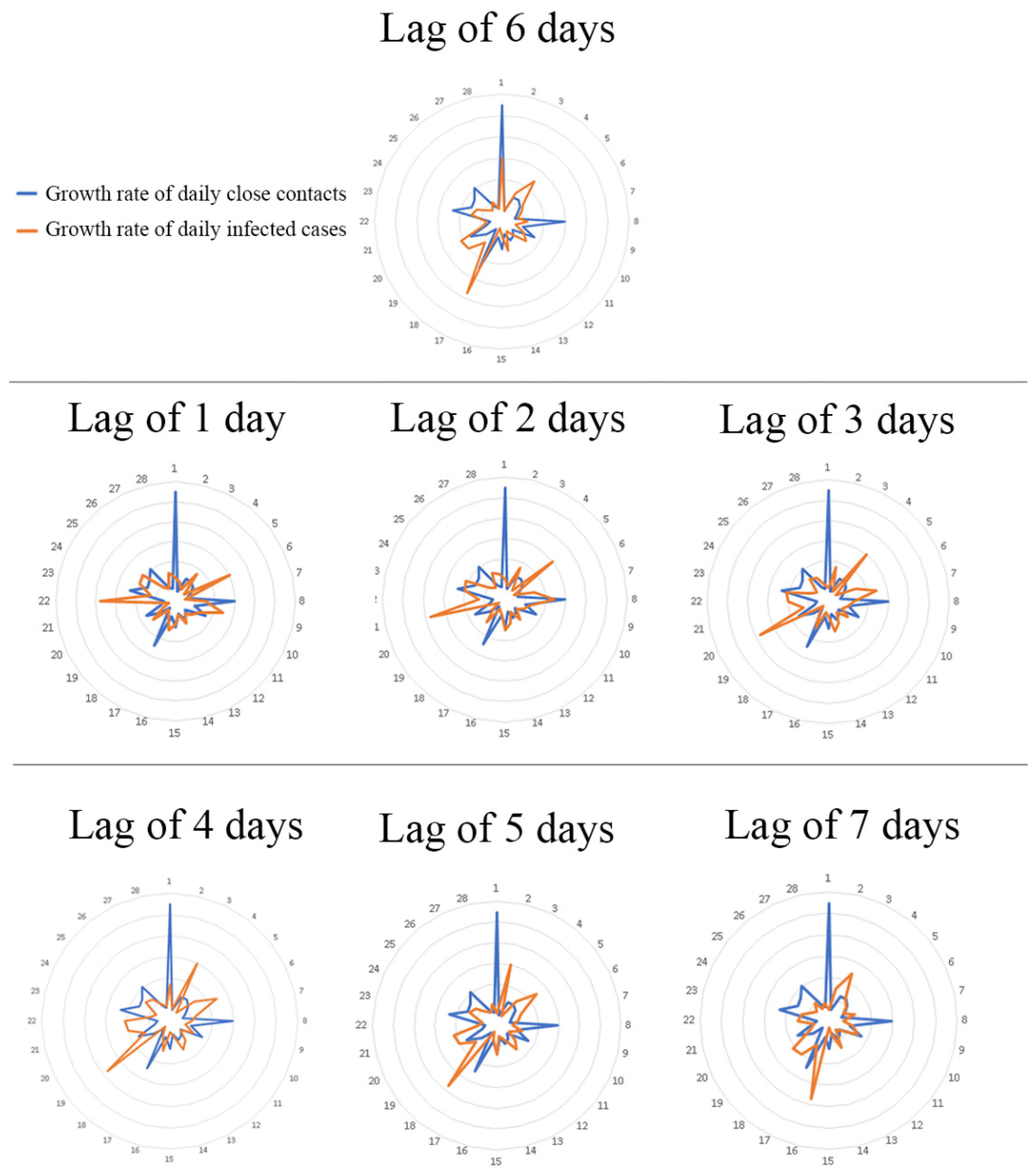
2.3. Statistical Analysis: Analyzing the Progress of the Epidemic Based on the Growth Rate of Close Contacts
- (1)
- Growth rate of close contacts = (number of new close contacts on day t + 1 − number of new close contacts on day t)/number of new close contacts on day t.
- (2)
- Growth rate of infected cases = (number of new infected cases on day t + 1 − number of new infected cases on day t)/number of new infected cases on day t.
3. Results
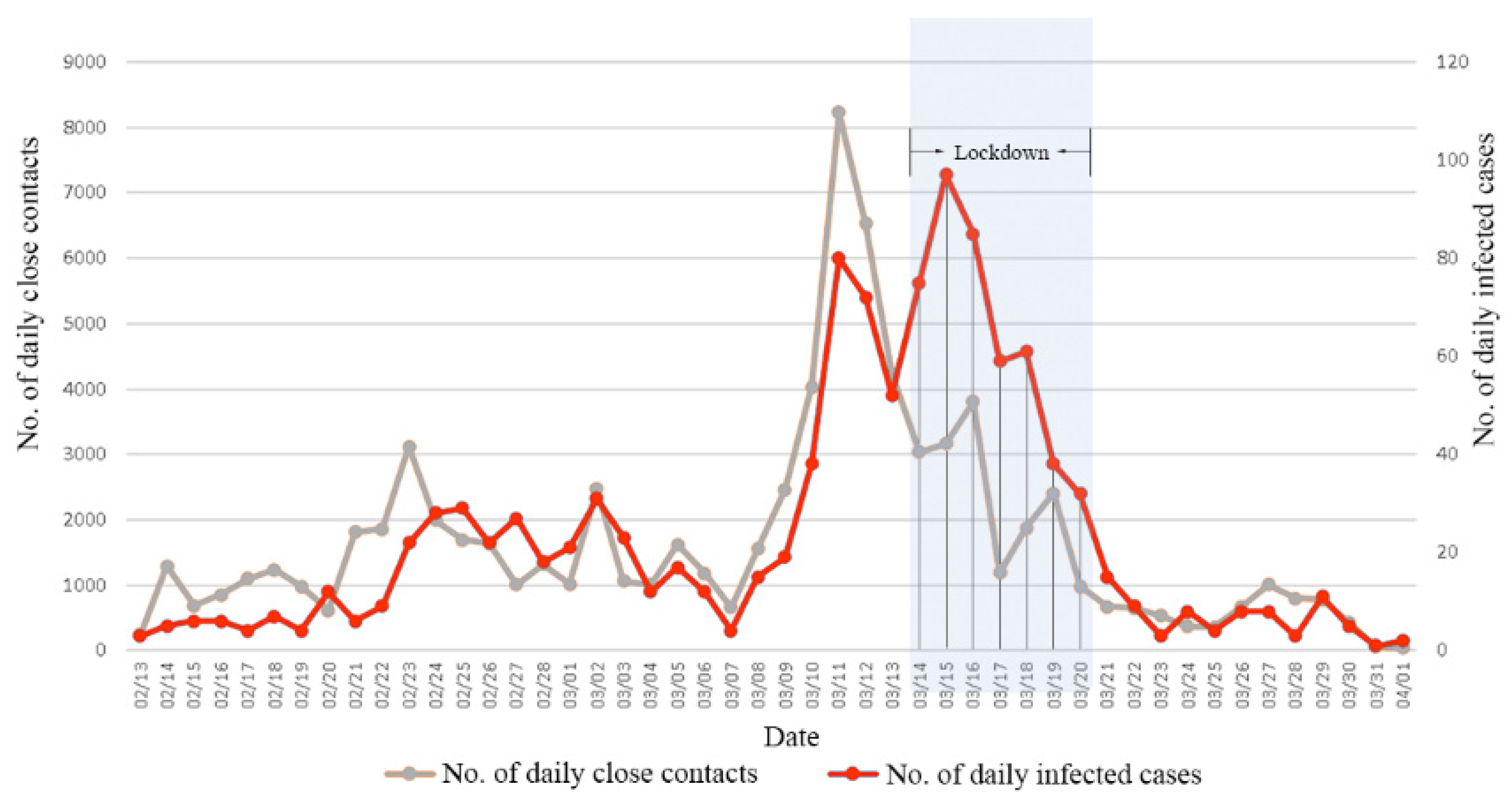
3.1. Number of New Close Contacts and Infected Cases by Days or Stages
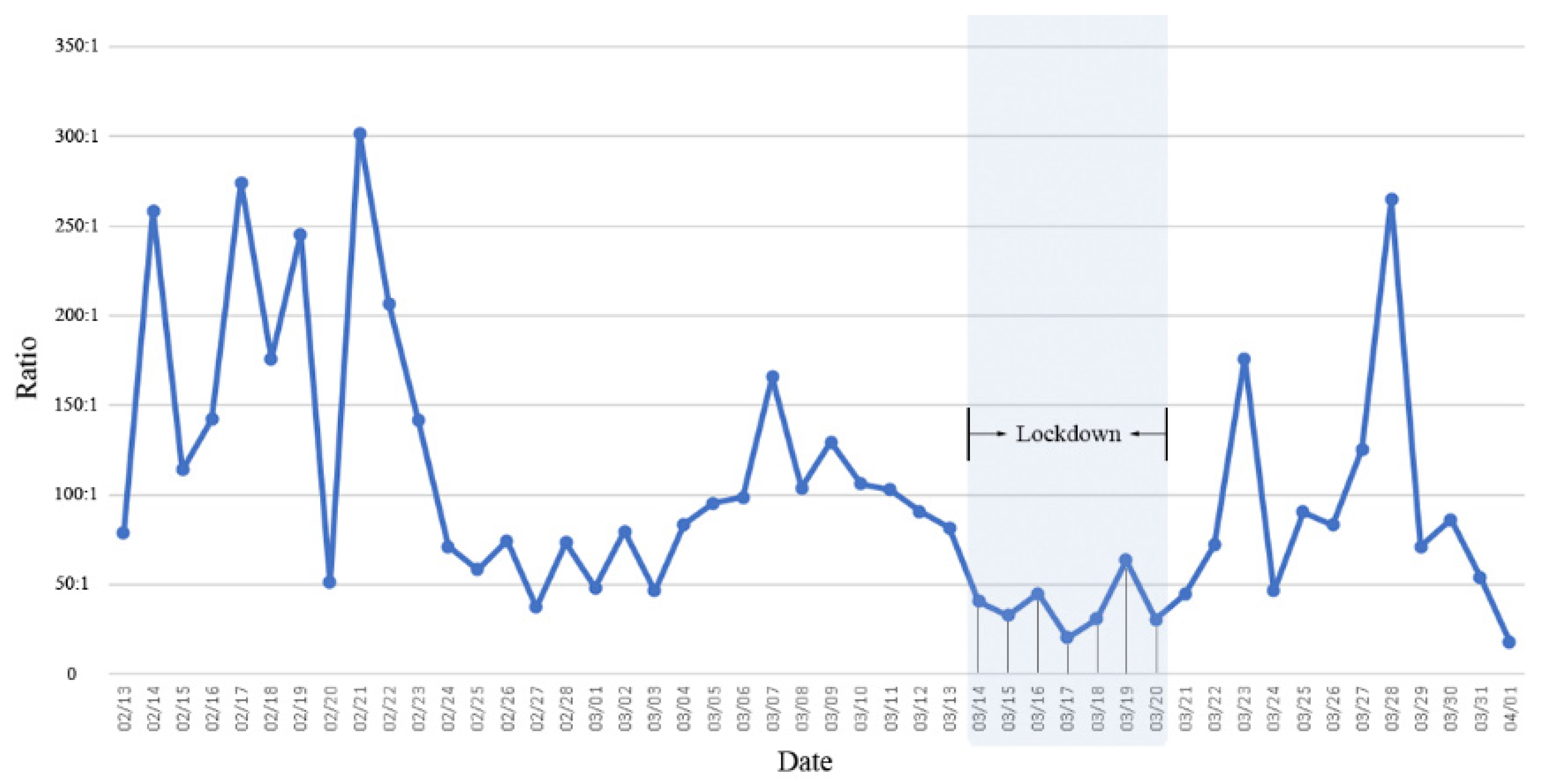
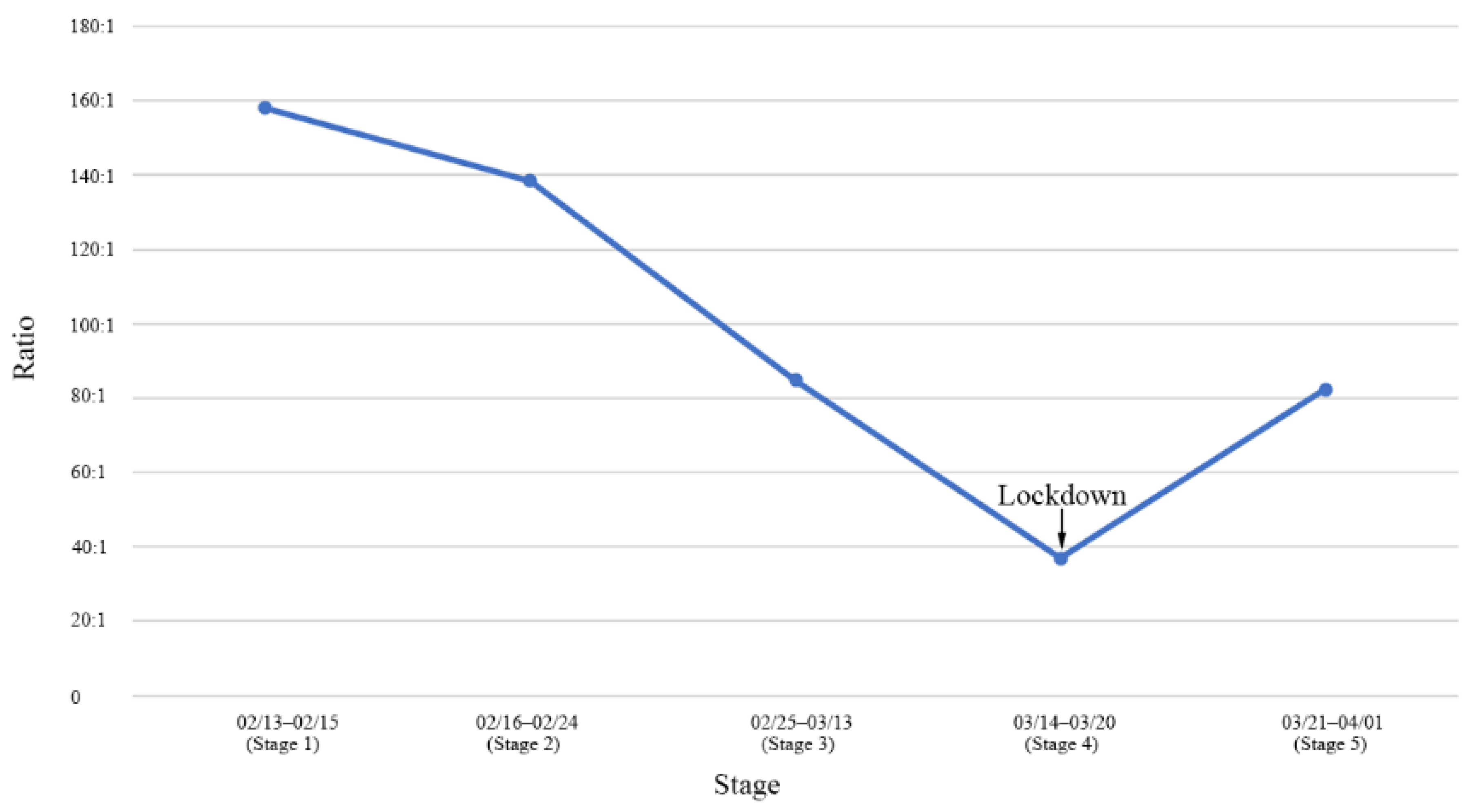
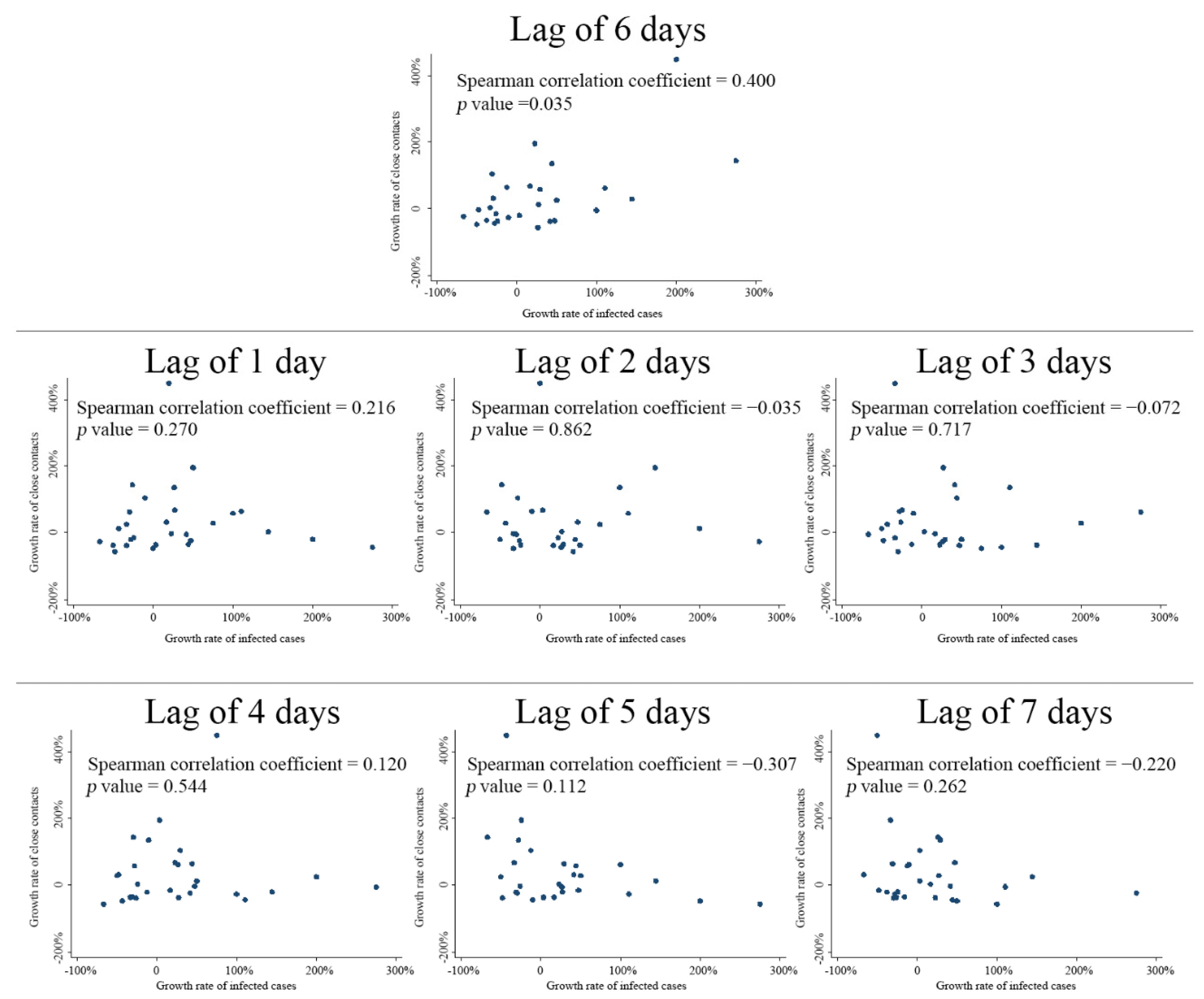
3.2. Predicting the Trajectory of the Epidemic Based on the Growth Rate of Close Contacts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dyer, O. COVID-19: Lockdowns spread in China as omicron tests “zero covid” strategy. BMJ 2022, 376, o859. [Google Scholar] [CrossRef] [PubMed]
- Ma, A.; Parry, J. When Hong Kong’s “dynamic zero” COVID-19 strategy met omicron, low vaccination rates sent deaths soaring. BMJ 2022, 377, o980. [Google Scholar] [CrossRef] [PubMed]
- Kerr, C.C.; Mistry, D.; Stuart, R.M.; Rosenfeld, K.; Hart, G.R.; Núñez, R.C.; Cohen, J.A.; Selvaraj, P.; Abeysuriya, R.G.; Jastrzębski, M.; et al. Controlling COVID-19 via test-trace-quarantine. Nat. Commun. 2021, 12, 2993. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: A retrospective cohort study. Lancet Infect. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- Ge, Y.; Martinez, L.; Sun, S.; Chen, Z.; Zhang, F.; Li, F.; Sun, W.; Chen, E.; Pan, J.; Li, C.; et al. COVID-19 Transmission Dynamics Among Close Contacts of Index Patients With COVID-19: A Population-Based Cohort Study in Zhejiang Province, China. JAMA Intern. Med. 2021, 181, 1343–1350. [Google Scholar] [CrossRef]
- Luo, L.; Liu, D.; Liao, X.; Wu, X.; Jing, Q.; Zheng, J.; Liu, F.; Yang, S.; Bi, H.; Li, Z.; et al. Contact Settings and Risk for Transmission in 3410 Close Contacts of Patients With COVID-19 in Guangzhou, China: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 879–887. [Google Scholar] [CrossRef]
- Crawford, F.W.; Jones, S.A.; Cartter, M.; Dean, S.G.; Warren, J.L.; Li, Z.R.; Barbieri, J.; Campbell, J.; Kenney, P.; Valleau, T.; et al. Impact of close interpersonal contact on COVID-19 incidence: Evidence from 1 year of mobile device data. Sci. Adv. 2022, 8, eabi5499. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, W.; Chen, S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet 2022, 399, 2011–2012. [Google Scholar] [CrossRef]
- Fan, X.; Lu, S.; Bai, L.; Liu, H.; Fu, J.; Jin, X.; He, Y.; Lu, J.; Dong, X. Preliminary Study of the Protectiveness of Vaccination Against the COVID-19 in the Outbreak of VOC Omicron BA.2-Jilin City, Jilin Province, China, 3 March–12 April 2022. China CDC Wkly. 2022, 4, 377–380. [Google Scholar] [PubMed]
- Burki, T. Dynamic zero COVID policy in the fight against COVID. Lancet Respir. Med. 2022, 10, e58–e59. [Google Scholar] [CrossRef]
- Wang, X.; Wang, J.; Shen, J.; Ji, J.S.; Pan, L.; Liu, H.; Zhao, K.; Li, L.; Ying, B.; Fan, L.; et al. Facilities for Centralized Isolation and Quarantine for the Observation and Treatment of Patients with COVID-19. Engineering 2021, 7, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Tsang, T.K.; Fang, L.Q.; Zhang, A.; Jiang, F.C.; Ruan, S.M.; Liu, L.Z.; Cowling, B.J.; Liu, W.; Yang, Y. Variability in transmission risk of SARS-CoV-2 in close contact settings: A contact tracing study in Shandong Province, China. Epidemics 2022, 39, 100553. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zheng, H. From blanket quarantine in Wuhan to distant centralized quarantine in Shijiazhuang: The evolution of China’s COVID-19 quarantine approach. Infection 2021, 49, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Wu, H.; Zhou, D.; Li, K.; Zhang, Y.; Ji, H.; Tong, Z.; Lou, S.; Liu, Z. Application of Big Data and Artificial Intelligence in COVID-19 Prevention, Diagnosis, Treatment and Management Decisions in China. J. Med. Syst. 2021, 45, 84. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.; Wang, C. Big Data Technology Applications and the Right to Health in China during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7325. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Li, X.; Zhu, B.; Zhao, W.; Huang, J.; Liu, G.; Gu, D. Effect of Lockdown and Mass Testing for the SARS-CoV-2 Omicron Epidemic on Reducing New Infections in Shenzhen, China. Healthcare 2022, 10, 1725. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Deng, X.; Yang, J.; Sun, K.; Liu, H.; Chen, Z.; Peng, C.; Chen, X.; Wu, Q.; Zou, J.; et al. Modeling transmission of SARS-CoV-2 Omicron in China. Nat. Med. 2022, 28, 1468–1475. [Google Scholar] [CrossRef]
- Koc, H.C.; Xiao, J.; Liu, W.; Li, Y.; Chen, G. Long COVID and its Management. Int. J. Biol. Sci. 2022, 18, 4768–4780. [Google Scholar] [CrossRef] [PubMed]
- Ceban, F.; Ling, S.; Lui, L.M.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2021, 101, 93–135. [Google Scholar] [CrossRef] [PubMed]
- Montani, D.; Savale, L.; Noel, N.; Meyrignac, O.; Colle, R.; Gasnier, M.; Corruble, E.; Beurnier, A.; Jutant, E.M.; Pham, T.; et al. Post-acute COVID-19 syndrome. Eur. Respir. Rev. 2022, 31, 210185. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Date | No. of Daily Infected Cases | No. of Daily Close Contacts |
|---|---|---|---|
| Stage 1 | 2/13–2/15 | 14 | 2212 |
| Stage 2 | 2/16–2/24 | 98 | 13,562 |
| Stage 3 | 2/25–3/13 | 492 | 41,715 |
| Stage 4 | 3/14–3/20 | 447 | 16,458 |
| Stage 5 | 3/21–4/01 | 77 | 6341 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, F.; Liang, F.; Zhu, B.; Han, X.; Fang, S.; Huang, J.; Zou, X.; Gu, D. Close Contacts, Infected Cases, and the Trends of SARS-CoV-2 Omicron Epidemic in Shenzhen, China. Healthcare 2022, 10, 2126. https://doi.org/10.3390/healthcare10112126
Li F, Liang F, Zhu B, Han X, Fang S, Huang J, Zou X, Gu D. Close Contacts, Infected Cases, and the Trends of SARS-CoV-2 Omicron Epidemic in Shenzhen, China. Healthcare. 2022; 10(11):2126. https://doi.org/10.3390/healthcare10112126
Chicago/Turabian StyleLi, Furong, Fengchao Liang, Bin Zhu, Xinxin Han, Shenying Fang, Jie Huang, Xuan Zou, and Dongfeng Gu. 2022. "Close Contacts, Infected Cases, and the Trends of SARS-CoV-2 Omicron Epidemic in Shenzhen, China" Healthcare 10, no. 11: 2126. https://doi.org/10.3390/healthcare10112126