
A Model for Effective Nonverbal Communication between Nurses and Older Patients: A Grounded Theory Inquiry

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Settings and Context
2.3. Study Participants and Sampling Methods
2.4. Data Collection
2.5. Data Analysis
2.6. Ethical Considerations
2.7. Rigor
3. Results and Discussion
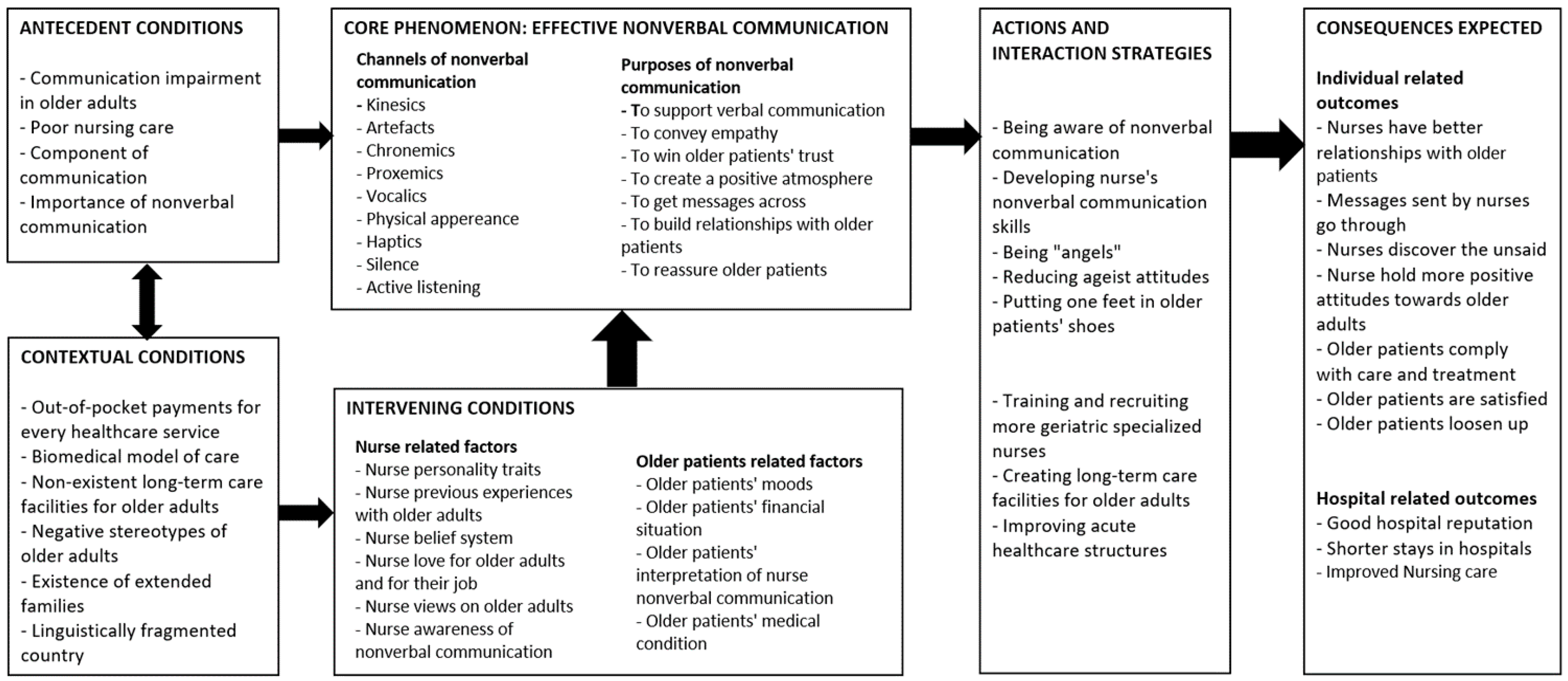
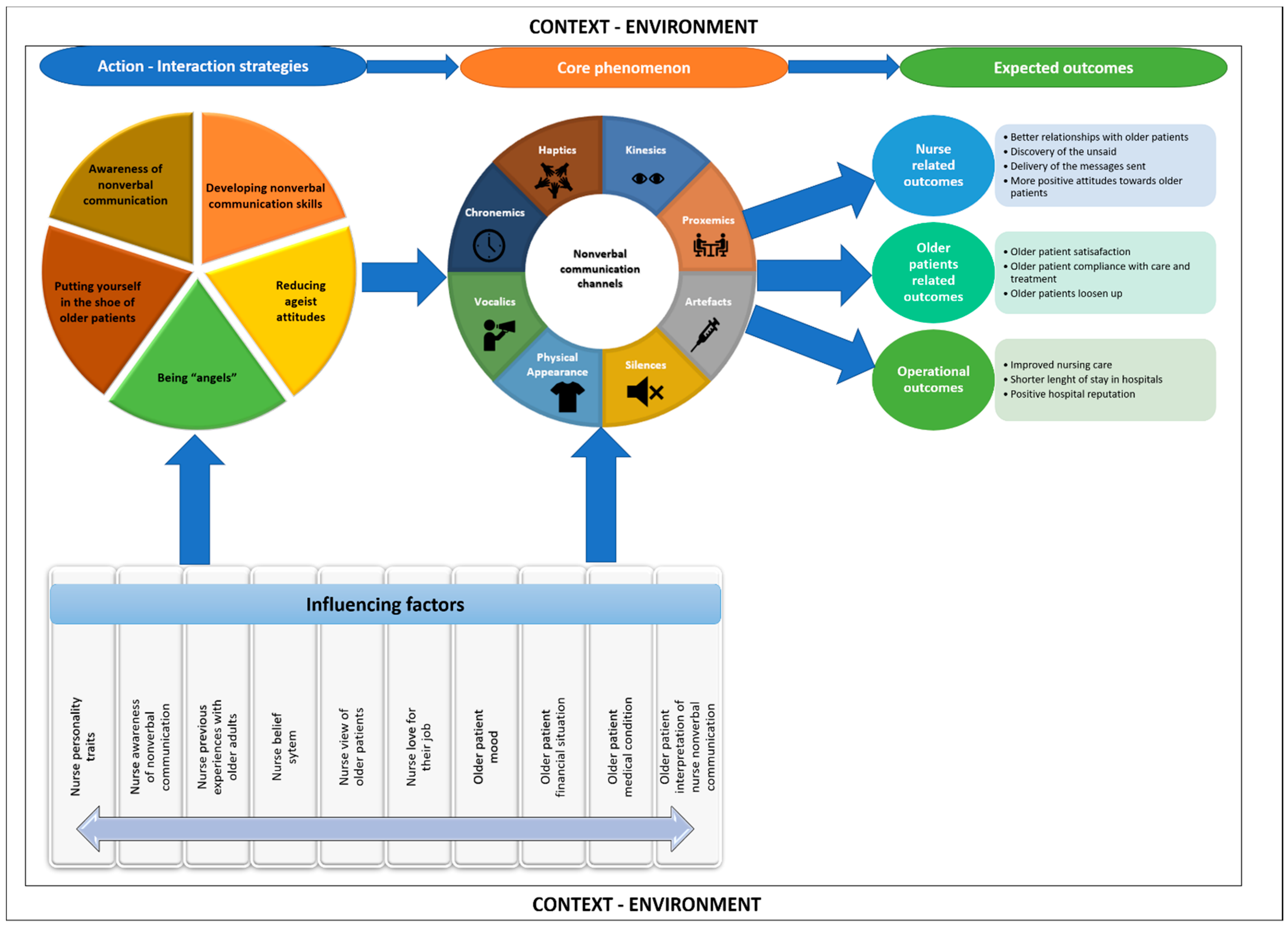
3.1. Purpose of the Model
3.2. Basic Assumptions of the Model
3.3. Concepts and Definitions
3.3.1. Core Concept
The Channels of Effective Nonverbal Communication
The Purposes of Effective Nonverbal Communication
3.3.2. Context and Environment
3.3.3. The Action and Interaction Strategies
3.3.4. The Pillars to Sustain Effective Nonverbal Communication between Nurses and Older Patients
3.3.5. The Outcomes of the Model
Individual-Related Outcomes
Operational Outcomes
3.4. Relationships between Concepts
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs Population Division. World Population Ageing 2019: Highlights (ST/ESA/SER.A/430); United Nations: New York, NY, USA, 2019.
- Essomba, M.J.N.; Atsa, D.; Noah, D.Z.; Zingui-Ottou, M.; Paula, G.; Nkeck, J.R.; Noubiap, J.J.; Ashuntantang, G. Geriatric syndromes in an urban elderly population in Cameroon: A focus on disability, sarcopenia and cognitive impairment. Pan Afr. Med. J. 2020, 37, 229. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, K.; Van Wyk, J. Protocol for a scoping review of age-related health conditions among geriatric populations in sub-Saharan Africa. Syst. Rev. 2019, 8, 133. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Towards Long-Term Care Systems in Sub-Saharan Africa; World Health Organization: Geneva, Switzerland, 2017; ISBN 9241513381.
- Forsgren, E.; Skott, C.; Hartelius, L.; Saldert, C. Communicative barriers and resources in nursing homes from the enrolled nurses’ perspective: A qualitative interview study. Int. J. Nurs. Stud. 2015, 54, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Skoglund, K.; Holmström, I.; Sundler, A.; Hammar, L. Previous work experience and age do not affect final semester nursing student self-efficacy in communication skills. Nurse Educ. Today 2018, 68, 182–187. [Google Scholar] [CrossRef]
- Hafskjold, L.; Sundler, A.; Holmström, I.; Sundling, V.; van Dulmen, S.; Eide, H. A cross-sectional study on person-centred communication in the care of older people: The COMHOME study protocol. BMJ Open 2015, 5, e007864. [Google Scholar] [CrossRef]
- Velentzas, J.; Broni, G. Communication cycle: Definition, process, models and examples. Recent Adv. Financ. Plan. Prod. Dev. 2014, 17, 117–131. [Google Scholar]
- de Guzman, A.; Jaurigue, K.; Jimenez, A. A comparison of the nurse–patient interaction criteria among geriatric clients in home health care and community settings: A trade-off analysis. Educ. Gerontol. 2019, 45, 176–190. [Google Scholar] [CrossRef]
- Blanch-Hartigan, D.; Ruben, M.A.; Hall, J.A.; Mast, M.S. Measuring nonverbal behavior in clinical interactions: A pragmatic guide. Patient Educ. Couns. 2018, 101, 2209–2218. [Google Scholar] [CrossRef]
- Hall, J.; Horgan, T.; Murphy, N. Nonverbal communication. Annu. Rev. Psychol. 2019, 70, 271–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kee, J.W.; Khoo, H.S.; Lim, I.; Koh, M.Y. Communication Skills in Patient-Doctor Interactions: Learning from Patient Complaints. Health Prof. Educ. 2018, 4, 97–106. [Google Scholar] [CrossRef]
- Lorié, Á.; Reinero, D.A.; Phillips, M.; Zhang, L.; Riess, H. Culture and nonverbal expressions of empathy in clinical settings: A systematic review. Patient Educ. Couns. 2017, 100, 411–424. [Google Scholar] [CrossRef]
- Tran, T.V.; Tran, T.D.; Nguyen, A.Q.; Dinh, T.T.; Le, A.T.K.; Tran, H.B.; Vu, P.T.; Nguyen, H.T.; Dang, L.V.P. Nurse–patient communication: A quality assessment in public hospital. Int. J. Healthc. Manag. 2021, 14, 1127–1133. [Google Scholar] [CrossRef]
- Yazew, K.G.; Gebrie, M.H.; Aynalem, Z.B. Nurses’ communication skills and determinant factors in Amhara Region Referral Hospitals, Northwest Ethiopia, 2019. Int. J. Afr. Nurs. Sci. 2021, 14, 100310. [Google Scholar]
- Güner, P.; Hiçdurmaz, D.; Yıldırım, N.K.; Inci, F. Psychosocial care from the perspective of nurses working in oncology: A qualitative study. Eur. J. Oncol. Nurs. 2018, 34, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Egan, G. The Skilled Helper: A Systematic Approach to Effective Helping; Thomson Brooks/Cole Publishing Co.: Pacific Groce, CA, USA, 1990. [Google Scholar]
- Stickley, T. From SOLER to SURETY for effective non-verbal communication. Nurse Educ. Pract. 2011, 11, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Atieno Wagoro, M.; Duma, S. Nurses’ perspectives of an environment of optimum mental health: A grounded theory study. J. Res. Nurs. 2021, 26, 557–571. [Google Scholar] [CrossRef] [PubMed]
- Batalden, M.; Batalden, P.; Margolis, P.; Seid, M.; Armstrong, G.; Opipari-Arrigan, L.; Hartung, H. Coproduction of healthcare service. BMJ Qual. Saf. 2016, 25, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Emeh, A.N.; Che, F.L.; Gilbert, T.N.; Ashu, A.H. Health Status of Elderly Population in the Buea Health District, Cameroon. J. Clin. Gerontol. Geriatr. 2020, 11, 10–19. [Google Scholar] [CrossRef]
- Gallo, V. Ageism in nursing education: A review of the literature. Teach. Learn. Nurs. 2019, 14, 208–215. [Google Scholar] [CrossRef]
- Chiatoh, B.A.-A. The Cameroonian experience in mother tongue education planning: The community response framework. Curr. Issues Lang. Plan. 2014, 15, 376–392. [Google Scholar] [CrossRef]
- Salmon, P.; Young, B. Creativity in clinical communication: From communication skills to skilled communication. Med. Educ. 2011, 45, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Gorawara-Bhat, R.; Cook, M.A. Eye contact in patient-centered communication. Patient Educ. Couns. 2011, 82, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 4th ed.; Sage Publications: Los Angeles, CA, USA, 2015. [Google Scholar]
- McCann, T.V.; Clark, E. Grounded theory in nursing research: Part 1—Methodology. Nurse Res. 2003, 11, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Ngwakongnwi, E.; Atanga, M.B.S.; Quan, H. Challenges to Implementing a National Health Information System in Cameroon: Perspectives of Stakeholders. J. Public Health Afr. 2014, 5, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, A.L.; Corbin, J. Basics of Qualitative Research: Grounded Theory Procedures and Techniques; Sage Publications: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory; Sage: Thousands Oaks, CA, USA, 2014. [Google Scholar]
- NVivo Qualitative Data Analysis Software; Version 12; QSR International Pty Ltd.: Doncaster, Australia, 2018.
- Corbin, J.; Strauss, A. The Basics of Qualitative Research, 3rd ed.; Sage: Los Angeles, CA, USA, 2008. [Google Scholar]
- Goulding, C. Grounded Theory: A practical Guide for Management, Buiseness, and Market Researchers; SAGE: London, UK, 2002. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G. Establishing trustworthiness. Nat. Inq. 1985, 289, 289–327. [Google Scholar]
- Keutchafo, E.L.W.; Kerr, J. Older Adults’ Interpretation of Nurses’ Nonverbal Communication in Cameroon: A Grounded Theory Inquiry. Inq. J. Health Care Organ. Provis. Financ. 2022, 59, 00469580211056194. [Google Scholar] [CrossRef]
- Keutchafo, E.L.W.; Kerr, J.; Baloyi, O.B.; Duma, S.E. Conditions Influencing Effective Nurse Nonverbal Communication With Hospitalized Older Adults in Cameroon. Glob. Qual. Nurs. Res. 2022, 9, 2333393622109875. [Google Scholar] [CrossRef]
- Chinn, P.; Kramer, M. Integrated Theory & Knowledge Development in Nursing; Elsevier Health Sciences: Riverport Lane, MO, USA, 2013. [Google Scholar]
- Kourkouta, L.; Papathanasiou, I. Communication in nursing practice. Mater. Socio-Med. 2014, 26, 65–67. [Google Scholar] [CrossRef] [Green Version]
- United Nations Population Fund. World Population Aging. New-York UNPF. Available online: http://www.unfpa.org/ageing (accessed on 12 October 2022).
- Keutchafo, E.L.W.; Kerr, J.; Jarvis, M.A. Evidence of nonverbal communication between nurses and older adults: A scoping review. BMC Nurs. 2020, 19, 53. [Google Scholar] [CrossRef]
- McCabe, C.; Timmins, F. Communication Skills for Nursing Practice; Macmillan International Higher Education; Bloomsbury Publishing: London, UK, 2013. [Google Scholar]
- Jack, K.; Ridley, C.; Turner, S. Effective communication with older people. Nurs. Older People 2019, 33, 40–48. [Google Scholar] [CrossRef]
- Mast, M.S.; Kadji, K.K. How female and male physicians’ communication is perceived differently. Patient Educ. Couns. 2018, 101, 1697–1701. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.A.; Tsang, P.L.; Ching, S.S.Y.; Wong, F.Y.; Lam, W. Nurses’ perspectives on their communication with patients in busy oncology wards: A qualitative study. PLoS ONE 2019, 14, e0224178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, P.A.; Watson, R. Language barriers and their impact on provision of care to patients with limited English proficiency: Nurses’ perspectives. J. Clin. Nurs. 2017, 27, e1152–e1160. [Google Scholar] [CrossRef]
- Dima, I.; Teodorescu, M.; Gifu, D. New communication approaches vs. traditional communication. Int. Lett. Soc. Humanist. Sci. 2014, 31, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Barratt, J. Developing clinical reasoning and effective communication skills in advanced practice. Nurs. Stand. 2019, 34, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Daly, L. Effective communication with older adults. Nurs. Stand. 2017, 31, 55–63. [Google Scholar] [CrossRef]
- Webb, L. Exploring the characteristics of effective communicators in healthcare. Nurs. Stand. 2018, 33, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Keutchafo, E.; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban 4001, South Africa; Kerr, J.; School of Nursing and Public Health, College of Health Sciences, University of KwaZulu-Natal, Durban 4001, South Africa. Nurses’ nonverbal communication strategies with older patients in two hospital settings. Unpublished. 2022. [Google Scholar]
- Alforque, J.M.L.; Meneses, R.C.; Sorronda, M.; Locsin, R.C. Development of the Emerging Theory of Encountering Nursing in a Nurse-Nursed Dyadic Relationship (ThENNDyR). Open J. Nurs. 2020, 10, 777–809. [Google Scholar] [CrossRef]
- Madula, P.; Kalembo, F.W.; Yu, H.; Kaminga, A.C. Healthcare provider-patient communication: A qualitative study of women’s perceptions during childbirth. Reprod. Health 2018, 15, 135. [Google Scholar] [CrossRef]
- Guvenc, G.; Unver, V.; Basak, T.; Yuksel, C.; Ayhan, H.; Kok, G.; Konukbay, D.; Kose, G.; Aslan, O.; Tastan, S.; et al. Turkish Senior Nursing Students’ Communication Experience with English-Speaking Patients. J. Nurs. Educ. 2016, 55, 73–81. [Google Scholar] [CrossRef]
- Gorawara-Bhat, R.; Hafskjold, L.; Gulbrandsen, P.; Eide, H. Exploring physicians’ verbal and nonverbal responses to cues/concerns: Learning from incongruent communication. Patient Educ. Couns. 2017, 100, 1979–1989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arkorful, V.E.; Hammond, A.; Basiru, I.; Boateng, J.; Doku, F.; Pokuaah, S.; Agyei, E.K.; Baoteng, J.A.; Lugu, B.K. A Cross-Sectional Qualitative Study of Barriers to Effective Therapeutic Communication among Nurses and Patients. Int. J. Public Adm. 2020, 44, 500–512. [Google Scholar] [CrossRef]
- Yoo, H.J.; Lim, O.B.; Shim, J.L. Critical care nurses’ communication experiences with patients and families in an intensive care unit: A qualitative study. PLoS ONE 2020, 15, e0235694. [Google Scholar] [CrossRef] [PubMed]
- Attafuah, P.Y.; Amertil, N.P.; Abuosi, A.A.; Nyonator, D. Nurses knowledge and attitude towards care of older patients: A cross-sectional study. Int. J. Afr. Nurs. Sci. 2022, 16, 100413. [Google Scholar] [CrossRef]
- Andersen, R.S.; Risør, M.B. The importance of contextualization. Anthropological reflections on descriptive analysis, its limitations and implications. Anthr. Med. 2014, 21, 345–356. [Google Scholar] [CrossRef]
- Barker, H.R.; Griffiths, P.; Mesa-Eguiagaray, I.; Pickering, R.; Gould, L.; Bridges, J. Quantity and quality of interaction between staff and older patients in UK hospital wards: A descriptive study. Int. J. Nurs. Stud. 2016, 62, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwame, A.; Petrucka, P.M. Communication in nurse-patient interaction in healthcare settings in sub-Saharan Africa: A scoping review. Int. J. Afr. Nurs. Sci. 2020, 12, 100198. [Google Scholar] [CrossRef]
- Msiska, G.; Smith, P.; Fawcett, T. The “lifeworld” of Malawian undergraduate student nurses: The challenge of learning in resource poor clinical settings. Int. J. Afr. Nurs. Sci. 2014, 1, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Vatandost, S.; Cheraghi, F.; Oshvandi, K. Facilitators of professional communication between nurse and opposite gender patient: A content analysis. Maedica 2020, 15, 45–52. [Google Scholar]
- Andriyanto, A. Communication Barrier between Nurse and Patient at the Hospital: A Systematic Review. J. Health Policy Manag. 2019, 4, 105–110. [Google Scholar] [CrossRef]
- Wamara, C.K.; Bennich, M.; Strandberg, T. Missing voices: Older people’s perspectives on being abused in Uganda. J. Elder Abus. Negl. 2021, 33, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Sudirman, I.; Sidin, I. Does demography matter in nonverbal communication between physician and patient. Res. J. Bus. Manag. 2016, 3, 1–10. [Google Scholar] [CrossRef]
- Junaid, A.; Shaban, M. Perceptions of patients on doctors’ and nurses’ non-verbal communication in Lahore, Pakistan: A Phenomenological study. Pak. Armed Forces Med. J. 2018, 68, 1731–1736. [Google Scholar]
- Tork, H.M.; Alatrash, A.S.; Alharbi, A.R.; Almansour, M.A.; Alolayqi, R.S. Understanding communication skills learning, behavior and attitude among students in three nursing colleges in Qassim region, Saudi Arabia. Clin. Nurs. Stud. 2018, 7, 19–28. [Google Scholar] [CrossRef]
- Van der Cingel, M. Compassion in care: A qualitative study of older people with a chronic disease and nurses. Nurs. Ethics 2011, 18, 672–685. [Google Scholar] [CrossRef]
- Ayalon, L.; Dolberg, P.; Mikulionienė, S.; Perek-Białas, J.; Rapolienė, G.; Stypinska, J.; Willińska, M.; de la Fuente-Núñez, V. A systematic review of existing ageism scales. Ageing Res. Rev. 2019, 54, 100919. [Google Scholar] [CrossRef]
- World Health Organization. Global Report on Ageism; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2021.
- Wyman, M.F.; Shiovitz-Ezra, S.; Bengel, J. Ageism in the Health Care System: Providers, Patients, and Systems. In Contemporary Perspectives on Ageism; Ayalon, L., Tesch-Römer, C., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 193–212. [Google Scholar]
- Inouye, S.K. Creating an anti-ageist healthcare system to improve care for our current and future selves. Nat. Aging 2021, 1, 150–152. [Google Scholar] [CrossRef]
- Dionigi, R.A. Stereotypes of Aging: Their Effects on the Health of Older Adults. J. Geriatr. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Sumijati, S.; Astuti, D.R.; Setiawan, A.I. Islamic Counseling Communication of Nurses on Cancer Patients in Islamic Hospital. Ilmu Dakwah Acad. J. Homilet. Stud. 2020, 14, 275–296. [Google Scholar] [CrossRef]
- Griffiths, J. Person-centred communication for emotional support in district nursing: SAGE and THYME model. Br. J. Community Nurs. 2017, 22, 593–597. [Google Scholar] [CrossRef]
- Chan, E.A.; Wong, F.; Cheung, M.Y.; Lam, W. Patients’ perceptions of their experiences with nurse-patient communication in oncology settings: A focused ethnographic study. PLoS ONE 2018, 13, e0199183. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; der Wal, J.T.G.-V.; Pereboom, M.T.; Spelten, E.R.; Hutton, E.K.; van Dulmen, S. Clients’ psychosocial communication and midwives’ verbal and nonverbal communication during prenatal counseling for anomaly screening. Patient Educ. Couns. 2016, 99, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sequeira, S.; D’Silva, P. Client Satisfaction and Preferences Towards Nonverbal Communication (NVC) of Health Care Providers in a Therapeutic Setting, Mangaluru. Med.-Leg. Update 2020, 20, 51–56. [Google Scholar]
- Moore, J.; Prentice, D.; Crawford, J. Collaboration among nurses when transitioning older adults between hospital and community settings: A scoping review. J. Clin. Nurs. 2021, 30, 2769–2785. [Google Scholar] [CrossRef] [PubMed]
- Huynh, E.; Basic, D.; Gonzales, R.; Shanley, C. Structured interdisciplinary bedside rounds do not reduce length of hospital stay and 28-day re-admission rate among older people hospitalised with acute illness: An Australian study. Aust. Health Rev. 2017, 41, 599–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosadeghrad, A.M. Patient choice of a hospital: Implications for health policy and management. Int. J. Health Care Qual. Assur. 2014, 27, 152–164. [Google Scholar] [CrossRef]
- Hall, S.; Longhurst, S.; Higginson, I. Living and dying with dignity: A qualitative study of the views of older people in nursing homes. Age Ageing 2009, 38, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Lam, F.M.; Chan, P.F.; Liao, L.R.; Woo, J.; Hui, E.; Lai, C.W.; Kwok, T.C.; Pang, M.Y.C. Effects of whole-body vibration on balance and mobility in institutionalized older adults: A randomized controlled trial. Clin. Rehabil. 2017, 32, 462–472. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participant | Age (Years) | Gender | Hospital | Position | Types of Nurses | Years of Experiences |
|---|---|---|---|---|---|---|
| P1 | 26–35 | Female | Hospital 1 | Staff nurse | Degree nurse | 4 |
| P2 | 46–55 | Female | Hospital 2 | Middle unit manager | Diploma nurse | 32 |
| P3 | 36–45 | Female | Hospital 2 | Staff nurse | Diploma nurse | 23 |
| P4 | 36–45 | Male | Hospital 2 | Staff nurse | Geriatric nurse | 11 |
| P5 | 46–55 | Female | Hospital 2 | Unit manager | Geriatric nurse | 30 |
| P6 | 46–55 | Female | Hospital 2 | Staff nurse | Diploma nurse | 11 |
| P7 | 36–45 | Female | Hospital 2 | Staff nurse | Diploma nurse | 9 |
| P8 | 26–35 | Female | Hospital 2 | Staff nurse | Geriatric nurse | 3 |
| P9 | 26–35 | Female | Hospital 2 | Staff nurse | Geriatric nurse | 6 |
| P10 | 26–35 | Female | Hospital 2 | Staff nurse | Nurse aid | 14 |
| P11 | 36–45 | Female | Hospital 1 | Staff nurse | Diploma nurse | 13 |
| P12 | 36–45 | Female | Hospital 2 | Staff nurse | Geriatric nurse | 5 |
| P13 | 26–35 | Female | Hospital 1 | Middle unit manager | Degree nurse | 10 |
| P14 | 18–25 | Female | Hospital 1 | Student nurse | Degree program | 2nd year |
| P15 | 18–25 | Female | Hospital 1 | Student nurse | Diploma program | 1st year |
| P16 | 26–35 | Female | Hospital 2 | Student nurse | Student nurse aid | 1st year |
| P17 | 26–35 | Female | Hospital 2 | Student nurse | Student nurse aid | 1st year |
| P18 | 78 | Female | Hospital 1 | N/A | N/A | N/A |
| P19 | 65 | Male | Hospital 2 | N/A | N/A | N/A |
| P20 | 64 | Female | Hospital 2 | N/A | N/A | N/A |
| P21 | 82 | Female | Hospital 2 | N/A | N/A | N/A |
| P22 | 67 | Male | Hospital 2 | N/A | N/A | N/A |
| P23 | 61 | Male | Hospital 1 | N/A | N/A | N/A |
| P24 | 92 | Male | Hospital 2 | N/A | N/A | N/A |
| P25 | 70 | Female | Hospital 2 | N/A | N/A | N/A |
| Context and environment | Linguistically fragmented country | … We have different mother tongues, for example, because we are in a diversity of languages here in Cameroon. (P2, middle unit manager, diploma in nursing) Many of those 60 years and older do not speak neither French nor English. It is often the foufouldé (tribe in Cameroon), the Makas (tribe in Cameroon) and all that. After school, you find yourself in a region where you perhaps speak French and your own mother tongue while the patients do not understand French nor your mother tongue. What do you do? You use nonverbal communication. (P1, staff nurse, degree in nursing) |
| Negative stereotypes on older adults | In Cameroon, we believe that older people want to cling to life. They do not want to die. When they feel that they are about to die, they can exchange their life with younger lives to increase their lifespan. That is why younger people do not want to be close to a dying older person. It is like the famous video game Mario. When your energy level gets low, you should collect coins to increase your lifespan to continue to run. It is the same with older people. (P23, older man, 61 years) For example, in my village, there is this belief that if you administer care to an old patient that is almost dying, that patient can recover and transfer his death to you. (P12, staff nurse, specialization in geriatric nursing) | |
| Inexistent long-term care facilities | I think it would be different because here (in the hospitals), younger patients are mixed with older patients to young ones. Whereas there (long-term care facilities), you only care for older patients. I think it will help them better to be among themselves. Unfortunately, we don’t have homes in Cameroon yet. (P11, staff nurse, diploma in nursing) I think other structures should be created because it seems that in Cameroon, a geriatric unit is only functional here. With the ageing population, we need private structures for older patients because some families tell us that they wish there was a place where they could send their parents there for three months. Here in the hospital, you cannot keep a patient for three months because of the shortage of beds. If the government could develop structures for older people, it would be great. (P7, staff nurse, diploma nurse) |
| Core Phenomenon | Channel: Artifacts (use of objects) | When you want to know the time, you can show them a watch. So, we can use objects to pass a message, depending on what we want to tell the person. (P8, staff nurse, specialization in geriatric nursing) You put a bottle of water in front of them, so that they understand that you are giving them water, and they will drink. (P7, staff nurse, diploma in nursing) |
| Channel: Haptics | Yes, we touch the cheeks, we touch the hands. We greet, but touch his hand, so that he feels that we are here. (P10, staff nurse, nurse aid) Sometimes it takes a touch to make a change in them (older patients). (P17, student nurse, 1st year) When the person is sleeping, I touch him gently to wake him up. (P12, staff nurse, specialization in geriatric nursing) | |
| Purpose: Support verbal communication | You use hand gestures, facial expressions, eye gazes, all that to support what you are saying to him. (P1, staff nurse, degree in nursing) For me, nonverbal communication is anything we said or do without using words. For instance, it can be body language, smiling, frowning, a tap on a back, eye gazing, grumbling, and a lack of reaction when someone speaks to you. (P13, middle unit manager, degree in nursing) | |
| Purpose: Build relationships with older patients | As we said earlier, nonverbal communication is a form of exchange, a form of conversation with the older patients. The goal, I believe, is to establish a very good therapeutic relationship because we have to reassure the person, we put them at ease. I think nonverbal communication is to better establish a relationship with the older person and to encourage her to open up more. (P4, staff nurse, specialization in geriatric nursing) Often, nonverbal communication is to initiate the first contact in the relationship with older patients. Along the way, they notice that when the nurses come, they wave at them. So, even when the nurses forget to wave, the patients wave at the nurses. As time goes by, smiling with them, sitting on the bed close to them will help build the relationship. (P7, staff nurse, diploma in nursing) |
| Outcomes | Compliance with care | We had patients who were not talking when they first arrived, they totally refused to eat, but as we spent time with them, reassuring them all the time, touching them, they started to give in. That particular patient ended up taking his medication and eating by his own. That made us happy. (P8, staff nurse, specialization in geriatric nursing) … Even if she doesn’t like a particular drug, she will take it to please you in return. (P7, staff nurse, diploma in nursing) |
| Older patients’ satisfaction | When they smile with me or touch my hand, I am happy; I am pleased. I wish I could stay longer here. (P18, older woman, 78 years) So, the gestures play a lot because they bring joy in the unit, they bring joy to the family members as well as to the patients. The patients feel that we are willing to listen to them, that we are willing and are doing everything to help them. They are happy. (P10, staff nurse, nurse aid) | |
| Nurse messages go through | … When you gesture with them, they understand that you are giving them water for instance. They will drink it. Your message went through. Therefore, it (nonverbal communication) helps. (P7, staff nurse, diploma in nursing) Most of the times when they (nurses) use gestures, I understand what they mean. (P25, older woman, 70 years) Even if I speak in French and the patient does not understand, at least he feels that someone is speaking. Through my gestures, he understands what I mean. He interprets my gestures and understands, and my messages get through easily. (P8, staff nurse, specialization in geriatric nursing) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wanko Keutchafo, E.L.; Kerr, J.; Baloyi, O.B. A Model for Effective Nonverbal Communication between Nurses and Older Patients: A Grounded Theory Inquiry. Healthcare 2022, 10, 2119. https://doi.org/10.3390/healthcare10112119
Wanko Keutchafo EL, Kerr J, Baloyi OB. A Model for Effective Nonverbal Communication between Nurses and Older Patients: A Grounded Theory Inquiry. Healthcare. 2022; 10(11):2119. https://doi.org/10.3390/healthcare10112119
Chicago/Turabian StyleWanko Keutchafo, Esther L., Jane Kerr, and Olivia B. Baloyi. 2022. "A Model for Effective Nonverbal Communication between Nurses and Older Patients: A Grounded Theory Inquiry" Healthcare 10, no. 11: 2119. https://doi.org/10.3390/healthcare10112119