
Translation, Adaptation and Validation of the Pandemic Fatigue Scale (PFS) in the Greek Language
 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population/Sample
2.2. Ethical Considerations
2.3. Survey Instruments
2.3.1. Pandemic Fatigue Scale (PFS)
2.3.2. Generalized Anxiety Disorder Assessment (GAD-7)
2.3.3. Patient Health Questionnaire (PHQ-9)
2.4. Data Analysis
3. Results
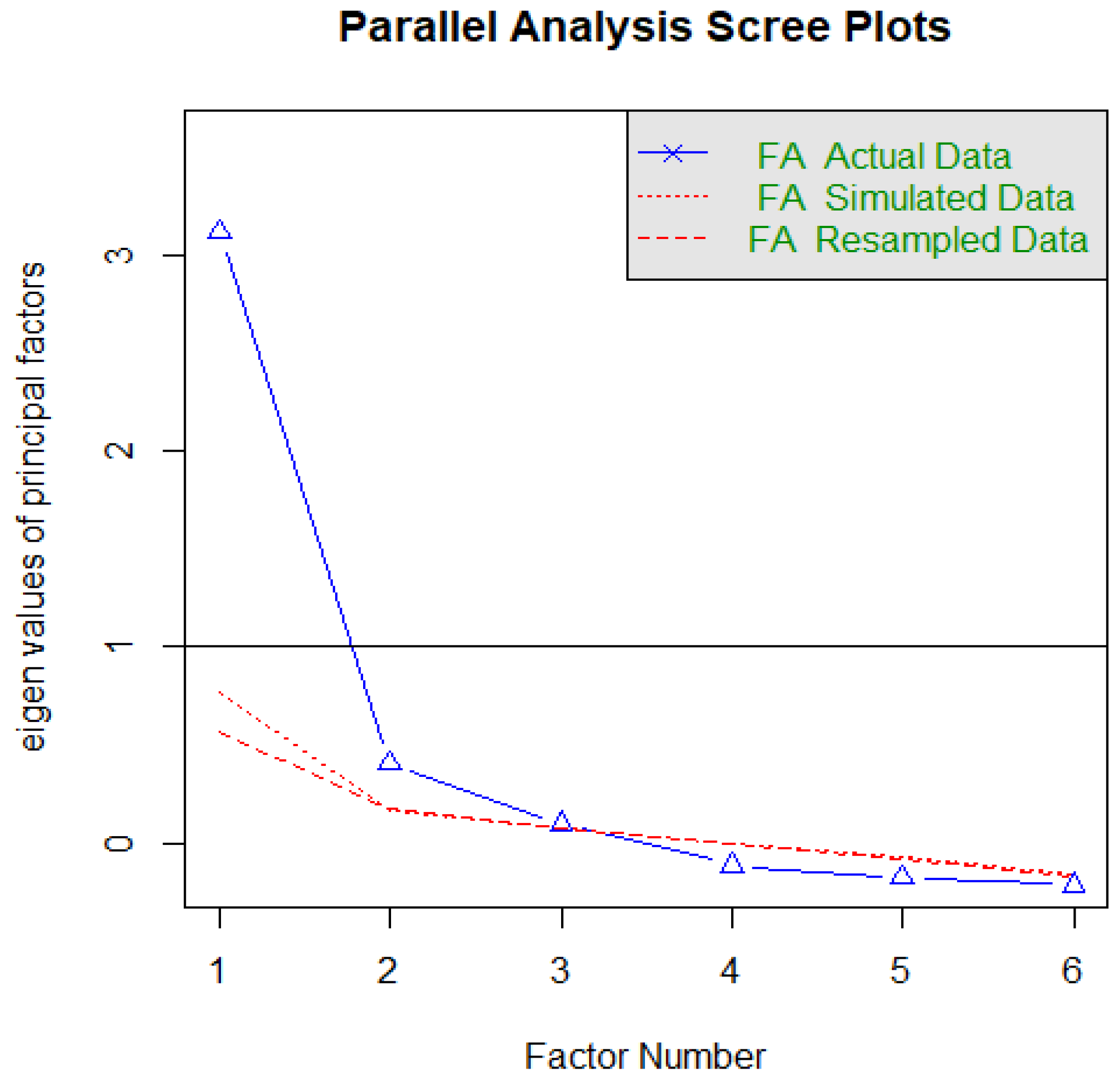
3.1. Exploratory Factor Analysis
3.2. Confirmatory Factor Analysis
3.3. Concurrent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Galanis, P.; Andreadaki, E.; Kleanthous, E.; Georgiadou, A.; Evangelou, E.; Kallergis, G.; Kaitelidou, D. Determinants of psychological distress during the COVID-19 pandemic and the lockdown measures: A nationwide on-line survey in Greece and Cyprus. Int. J. Caring Sci. 2021, 14, 837–853. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 October 2022).
- Lilleholt, L.; Zettler, I.; Betsch, C.; Böhm, R. Pandemic fatigue: Measurement, correlates, and consequences. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Patelarou, E.; Galanis, P.; Mechili, E.A.; Argyriadi, A.; Argyriadis, A.; Asimakopoulou, E.; Kicaj, E.; Bucaj, J.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I. Assessment of COVID-19 fear in five European countries before mass vaccination and key predictors among nurses and nursing students. Vaccines 2022, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Solomou, I.; Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef]
- Martini, M.; Gazzaniga, V.; Bragazzi, N.L.; Barberis, I. The Spanish Influenza Pandemic: A lesson from history 100 years after 1918. J. Prev. Med. Hyg. 2019, 60, E64. [Google Scholar] [CrossRef]
- World Health Organization. Pandemic Fatigue Reinvigorating the Public to Prevent COVID-19. Available online: https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf (accessed on 8 October 2022).
- Wang, D.; Marmo-Roman, S.; Krase, K.; Phanord, L. Compliance with preventative measures during the COVID-19 pandemic in the USA and Canada: Results from an online survey. Soc. Work Health Care 2021, 60, 240–255. [Google Scholar] [CrossRef]
- Kim, H.J.; Meeker, T.J.; Tulloch, I.K.; Mullins, J.; Park, J.-H.; Bae, S.H. Pandemic Fatigue and Anxiety Sensitivity as Associated Factors With Posttraumatic Stress Symptoms Among University Students in South Korea During the Prolonged COVID-19 Pandemic. Int. J. Public Health 2022, 67, 1604552. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Chutiyami, M.; Bello, U.M.; Salihu, D.; Ndwiga, D.; Kolo, M.A.; Maharaj, R.; Naidoo, K.; Devar, L.; Pratitha, P.; Kannan, P. COVID-19 pandemic-related mortality, infection, symptoms, complications, comorbidities, and other aspects of physical health among healthcare workers globally: An umbrella review. Int. J. Nurs. Stud. 2022, 129, 104211. [Google Scholar] [CrossRef]
- Pullen, M.F.; Skipper, C.P.; Hullsiek, K.H.; Bangdiwala, A.S.; Pastick, K.A.; Okafor, E.C.; Lofgren, S.M.; Rajasingham, R.; Engen, N.W.; Galdys, A. Symptoms of COVID-19 outpatients in the United States. Open Forum Infect. Dis. 2020, 7, ofaa271. [Google Scholar] [CrossRef] [PubMed]
- Maben, J.; Conolly, A.; Abrams, R.; Rowland, E.; Harris, R.; Kelly, D.; Kent, B.; Couper, K. ‘You can’t walk through water without getting wet’UK nurses’ distress and psychological health needs during the Covid-19 pandemic: A longitudinal interview study. Int. J. Nurs. Stud. 2022, 131, 104242. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Chen, L.; Feng, F.; Okoli, C.T.C.; Tang, P.; Zeng, L.; Jin, M.; Zhang, Y.; Wang, J. The prevalence of compassion satisfaction and compassion fatigue among nurses: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2021, 120, 103973. [Google Scholar] [CrossRef] [PubMed]
- Ream, E.; Richardson, A. Fatigue: A concept analysis. Int. J. Nurs. Stud. 1996, 33, 519–529. [Google Scholar] [CrossRef]
- Whitehead, L. The Measurement of Fatigue in Chronic Illness: A Systematic Review of Unidimensional and Multidimensional Fatigue Measures. J. Pain Symptom Manag. 2009, 37, 107–128. [Google Scholar] [CrossRef]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Prevalence and determinants of fatigue after COVID-19 in non-hospitalized subjects: A population-based study. Int. J. Environ. Res. Public Health 2021, 18, 2030. [Google Scholar] [CrossRef]
- Liu, C.; Liu, Y. Media exposure and anxiety during COVID-19: The mediation effect of media vicarious traumatization. Int. J. Environ. Res. Public Health 2020, 17, 4720. [Google Scholar] [CrossRef]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef]
- World Health Organization. Process of Translation and Adaptation of Instruments. Available online: https://cir.nii.ac.jp/crid/1572543025674509568 (accessed on 8 October 2022).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Group, P.H.Q.P.C.S.; Group, P.H.Q.P.C.S. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Jama 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cyprus Ministry of Education, Sport and Youth. Available online: https://archeia.moec.gov.cy/mc/916/chartografisi_2020_2021.pdf (accessed on 8 October 2022).
- Hatcher, L.; O’Rourke, N. A Step-by-Step Approach to Using SAS for Factor Analysis and Structural Equation Modeling, 2nd ed.; SAS Institute Inc.: Cary, NC, USA, 2013. [Google Scholar]
- Nunnally, J.C. An Overview of Psychological Measurement. In Clinical Diagnosis of Mental Disorders: A Handbook; Wolman, B.B., Ed.; Springer US: Boston, MA, USA, 1978; pp. 97–146. [Google Scholar] [CrossRef]
- Hyphantis, T.; Kotsis, K.; Voulgari, P.V.; Tsifetaki, N.; Creed, F.; Drosos, A.A. Diagnostic accuracy, internal consistency, and convergent validity of the Greek version of the patient health questionnaire 9 in diagnosing depression in rheumatologic disorders. Arthritis Care Res. 2011, 63, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: Pearson New International Edition; Pearson Education Limited: Essex, UK, 2014; Volume 1. [Google Scholar]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M.L. Chi-square for model fit in confirmatory factor analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238. [Google Scholar] [CrossRef]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Steiger, J.H. Structural model evaluation and modification: An interval estimation approach. Multivar. Behav. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Joreskog, K.; Sorbom, D. LISREL 8 User’s Reference Guide; Science Software: Chicago, IL, USA, 1993. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford publications: New York, NY, USA, 2015. [Google Scholar]
- Gao, H.; Du, Z.; Tsang, T.K.; Xiao, J.; Shan, S.; Liao, Q.; Wu, P.; Leung, G.M.; Cowling, B.J. Pandemic fatigue and attenuated impact of avoidance behaviours against COVID-19 transmission in Hong Kong by cross-sectional telephone surveys. BMJ Open 2021, 11, e055909. [Google Scholar] [CrossRef]
- Ford, J.L.; Douglas, M.; Barrett, A.K. The Role of Pandemic Fatigue in Seeking and Avoiding Information on COVID-19 Among Young Adults. Health Commun. 2022, 5, 1–14. [Google Scholar] [CrossRef]
- Shi, C.-F.; So, M.C.; Stelmach, S.; Earn, A.; Earn, D.J.; Dushoff, J. From science to politics: COVID-19 information fatigue on YouTube. BMC Public Health 2022, 22, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Guan, M.; Li, Y.; Scoles, J.D.; Zhu, Y. COVID-19 Message Fatigue: How Does It Predict Preventive Behavioral Intentions and What Types of Information are People Tired of Hearing About? Health Commun. 2022, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N. Behavioral fatigue: Real phenomenon, naïve construct, or policy contrivance? Front. Psychol. 2020, 11, 589892. [Google Scholar] [CrossRef] [PubMed]
- Kvarnström, K.; Airaksinen, M.; Liira, H. Barriers and facilitators to medication adherence: A qualitative study with general practitioners. BMJ Open 2018, 8, e015332. [Google Scholar] [CrossRef] [PubMed]
- Khalid, A.; Younas, M.W.; Khan, H.; Khan, M.S.; Malik, A.R.; Butt, A.U.A.; Ali, B. Relationship between knowledge on COVID-19 and psychological distress among students living in quarantine: An email survey. AIMS Public Health 2021, 8, 90. [Google Scholar] [CrossRef]
- Patelarou, E.; Galanis, P.; Mechili, E.A.; Argyriadi, A.; Argyriadis, A.; Asimakopoulou, E.; Brokaj, S.; Bucaj, J.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I. Factors influencing nursing students’ intention to accept COVID-19 vaccination: A pooled analysis of seven European countries. Nurse Educ. Today 2021, 104, 105010. [Google Scholar] [CrossRef]
- Williams, S.N.; Armitage, C.J.; Tampe, T.; Dienes, K.A. Public perceptions of non-adherence to pandemic protection measures by self and others: A study of COVID-19 in the United Kingdom. PLoS ONE 2021, 16, e0258781. [Google Scholar] [CrossRef]
- Bodas, M.; Kaim, A.; Velan, B.; Ziv, A.; Jaffe, E.; Adini, B. Overcoming the effect of pandemic fatigue on vaccine hesitancy—Will belief in science triumph? J. Nurs. Scholarsh. 2022, 00, 1–10. [Google Scholar] [CrossRef]
- Labrague, L.J. Pandemic fatigue and clinical nurses’ mental health, sleep quality and job contentment during the COVID-19 pandemic: The mediating role of resilience. J. Nurs. Manag. 2021, 29, 1992–2001. [Google Scholar] [CrossRef]
- Wylie, G.R.; Pra Sisto, A.J.; Genova, H.M.; DeLuca, J. Fatigue across the lifespan in men and women: State vs. trait. Front. Hum. Neurosci. 2022, 16, 790006. [Google Scholar] [CrossRef]
- Avlund, K. Fatigue in older adults: An early indicator of the aging process? Aging Clin. Exp. Res. 2010, 22, 100–115. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Strongly Disagree | Disagree | Somewhat Disagree | Neutral/Neither Disagree nor Agree | Somewhat Agree | Agree | Strongly Agree | |
|---|---|---|---|---|---|---|---|
| I am tired of all the COVID-19 discussions in TV shows, newspapers, radio programs, etc. (item 1) | 25(7.5) | 27(8.1) | 15(4.5) | 27(8.1) | 51(15.3) | 59(17.7) | 130(38.9) |
| I feel strained from following all of the behavioural regulations and recommendations around COVID-19. (item 4) | 49(14.7) | 67(20.1) | 19(5.7) | 51(15.3) | 51(15.3) | 52(15.6) | 45(13.5) |
| I am sick of hearing about COVID-19. (item 2) | 31(9.3) | 32(9.6) | 18(5.4) | 47(14.1) | 48(14.4) | 52(15.6) | 106(31.7) |
| I am tired of restraining myself to save those who are most vulnerable to COVID-19. (item 5) | 101(30.2) | 71(21.3) | 20(6) | 43(12.9) | 30(9) | 33(9.9) | 36(10.8) |
| When friends or family members talk about COVID-19, I try to change the subject because I do not want to talk about it anymore. (item 3) | 56(16.8) | 66(19.8) | 32(9.6) | 53(15.9) | 33(9.9) | 43(12.9) | 51(15.3) |
| I am losing my spirit to fight against COVID-19. (item 6) | 93(27.8) | 70(21) | 24(7.2) | 52(15.6) | 26(7.8) | 32(9.6) | 37(11.1) |
| PFS | ||||
|---|---|---|---|---|
| n (%) or Mean ± SD | Mean ± SD | Test | ||
| Gender | Male | 78(23.4) | 3.80 ± 1.41 | t332 = 0.327, p = 0.744 |
| Female | 256(76.6) | 3.74 ± 1.42 | ||
| Age | 28.04 ± 9.39 | r = 0.069, p = 0.206 | ||
| Level of education | Undergraduate | 172(51.5) | 3.52 ± 1.47 | t332 = −3.084, p = 0.002 |
| Postgraduate | 162(48.5) | 3.99 ± 1.32 | ||
| Infected with COVID-19 | yes | 106(31.7) | 4.22 ± 1.37 | t332 = −4.229, p < 0.001 |
| no | 228(68.3) | 3.53 ± 1.38 | ||
| Vaccinated against COVID-19 | yes | 279(83.5) | 3.61 ± 1.39 | t332 = 4.320, p < 0.001 |
| no | 55(16.5) | 4.49 ± 1.32 | ||
| Model (6 items) | ||
|---|---|---|
| Factors | ||
| Item | IF * | BF * |
| I am tired of all the COVID-19 discussions in TV shows, newspapers, radio programs, etc. (item 1) | 0.857 | 0.241 |
| I am sick of hearing about COVID-19. (item 2) | 0.900 | 0.155 |
| When friends or family members talk about COVID-19, I try to change the subject because I do not want to talk about it anymore. (item 3) | 0.675 | 0.482 |
| I feel strained from following all of the behavioural regulations and recommendations around COVID-19. (item 4) | 0.465 | 0.678 |
| I am tired of restraining myself to save those who are most vulnerable to COVID-19. (item 5) | 0.09 | 0.876 |
| I am losing my spirit to fight against COVID-19. (item 6) | 0.321 | 0.806 |
| % of variance | 59.76 | 15.56 |
| Cronbach’s alpha | 0.84 | 0.80 |
| Cronbach’s alpha overall | 0.86 | |
| KMO = 0.81, Bartlett’s Test of Sphericity = 446.47 (p < 0.001) | ||
| Model | χ2 | df | χ2/df | RMSEA | CFI | TLI | SRMS | |
|---|---|---|---|---|---|---|---|---|
| Model 1: | 6 items (one factor) | 86.33 | 9 | 9.59 | 0.22 | 0.88 | 0.80 | 0.07 |
| Model 2: | 6-item model (two factors) | 49.48 | 8 | 6.19 | 0.17 | 0.94 | 0.88 | 0.06 |
| Model 3: | 6-item model (two factors, correlated error– item 3 <-> item 5 and item 3 <-> item 6) | 15.42 | 6 | 2.57 | 0.09 | 0.99 | 0.96 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asimakopoulou, E.; Paoullis, P.; Shegani, A.; Argyriadis, A.; Argyriadi, A.; Patelarou, E.; Patelarou, A. Translation, Adaptation and Validation of the Pandemic Fatigue Scale (PFS) in the Greek Language. Healthcare 2022, 10, 2118. https://doi.org/10.3390/healthcare10112118
Asimakopoulou E, Paoullis P, Shegani A, Argyriadis A, Argyriadi A, Patelarou E, Patelarou A. Translation, Adaptation and Validation of the Pandemic Fatigue Scale (PFS) in the Greek Language. Healthcare. 2022; 10(11):2118. https://doi.org/10.3390/healthcare10112118
Chicago/Turabian StyleAsimakopoulou, Evanthia, Panagiotis Paoullis, Antonio Shegani, Alexandros Argyriadis, Agathi Argyriadi, Evridiki Patelarou, and Athina Patelarou. 2022. "Translation, Adaptation and Validation of the Pandemic Fatigue Scale (PFS) in the Greek Language" Healthcare 10, no. 11: 2118. https://doi.org/10.3390/healthcare10112118