
COVID-19 Depression and Infection Prevention Behavior among College Students: A Health Belief Perspective

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Data Collection
2.3. Ethics Approval
2.4. Measuring Instruments
2.4.1. Depression
2.4.2. Health Belief
2.4.3. Infection Prevention Behavior
2.5. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of Participants
3.2. Correlational and Descriptive Statistics
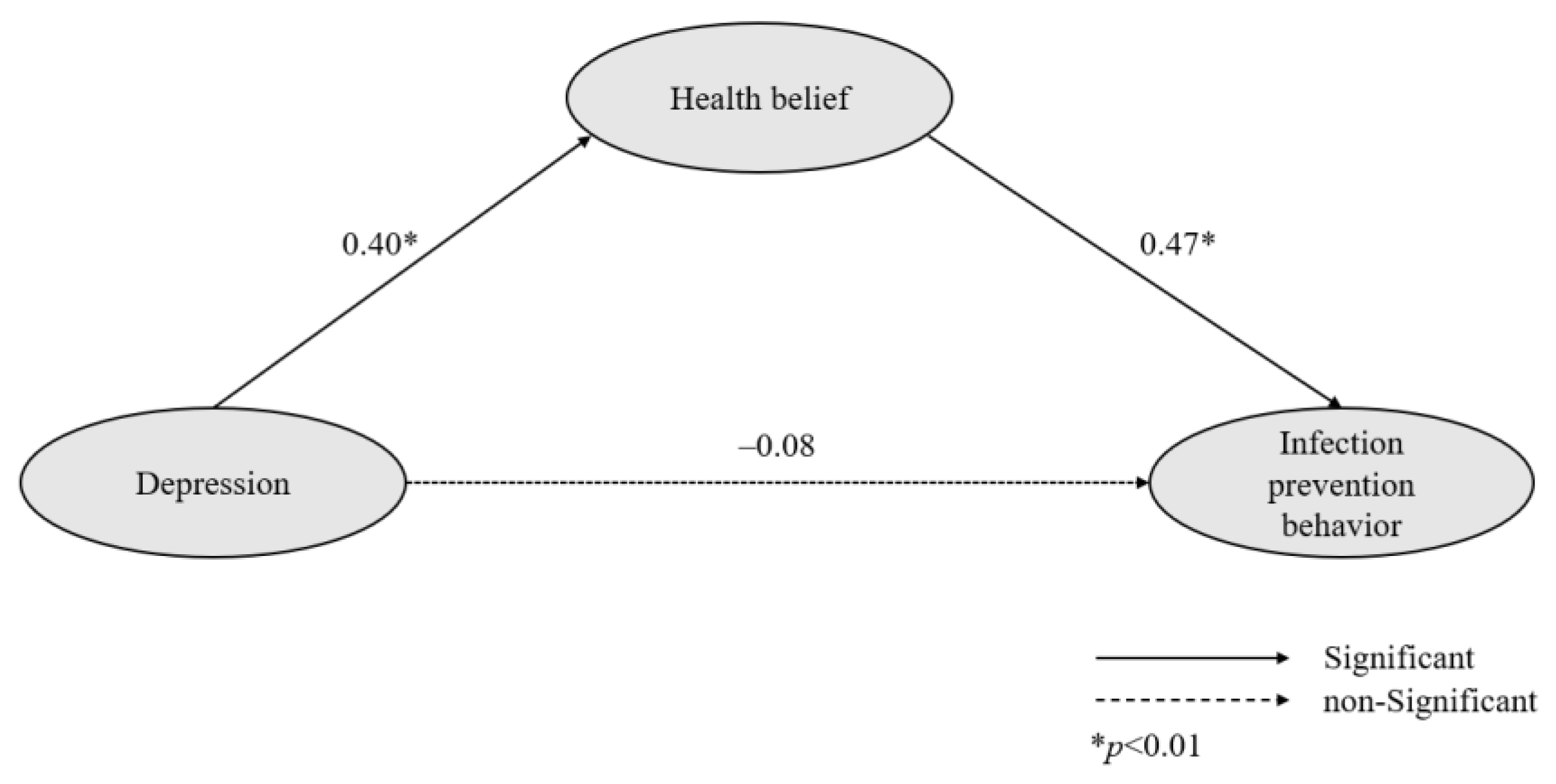
3.3. Model Fitness and Path Analysis
4. Discussion
4.1. Depression among College Students
4.2. Mediating Effect of Health Belief
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tong, K.K.; Chen, J.H.; Yu, E.W.; Wu, A.M.S. Adherence to COVID-19 precautionary measures: Applying the health belief model and generalised social beliefs to a probability community sample. Appl. Psychol. Health Well Being 2020, 12, 1205–1223. [Google Scholar] [CrossRef] [PubMed]
- Maier, B.F.; Brockmann, D. Effective containment explains subexponential growth in recent confirmed COVID-19 cases in China. Science 2020, 368, 742–746. [Google Scholar] [CrossRef] [Green Version]
- De-Diego-Cordero, R.; Martínez-Del-Carmen, C.; Sierra, P.B.; Vargas-Martínez, A.-M. Impact of the COVID-19 pandemic and psychosocial coping strategies in health sciences students at the University of Seville: A pilot study. Healthcare 2021, 9, 1661. [Google Scholar] [CrossRef] [PubMed]
- Nuggerud-Galeas, S.; Blázquez, B.O.; Yus, M.C.P.; Valle-Salazar, B.; Aguilar-Latorre, A.; Botaya, R.M. Factors associated with depressive episode recurrences in primary care: A retrospective, descriptive study. Front. Psychol. 2020, 11, 1230. [Google Scholar] [CrossRef] [PubMed]
- Morganstein, J.C.; Ursano, R.J. Ecological disasters and mental health: Causes, consequences, and interventions. Front. Psychiatry 2020, 11, 1. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Rodríguez-Hidalgo, A.J.; Pantaleón, Y.; Dios, I.; Falla, D. Fear of COVID-19, stress, and anxiety in university undergraduate students: A predictive model for depression. Front. Psychol. 2020, 11, 591797. [Google Scholar] [CrossRef]
- Fawaz, M.; Samaha, A. E-learning: Depression, anxiety, and stress symptomatology among Lebanese university students during COVID-19 quarantine. Nurs. Forum 2021, 56, 52–57. [Google Scholar] [CrossRef]
- Guo, K.; Zhang, X.; Bai, S.; Minhat, H.S.; Nazan, A.I.N.M.; Feng, J.; Li, X.; Luo, G.; Zhang, X.; Feng, J.; et al. Assessing social support impact on depression, anxiety, and stress among undergraduate students in Shaanxi province during the COVID-19 pandemic of China. PLoS ONE 2021, 16, e0253891. [Google Scholar] [CrossRef]
- Bressington, D.T.; Cheung, T.C.C.; Lam, S.C.; Suen, L.K.P.; Fong, T.K.H.; Ho, H.S.W.; Xiang, Y.-T. Association between depression, health beliefs, and face mask use during the COVID-19 pandemic. Front. Psychiatry 2020, 11, 571179. [Google Scholar] [CrossRef]
- Shaw, K. Exploring beliefs and attitudes of personal service practitioners towards infection control education, based on the health belief model. Environ. Health Rev. 2016, 59, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.F. Health belief model for coronavirus infection risk determinants. Rev. Saude Publica 2020, 54, 47. [Google Scholar] [CrossRef]
- Lam, S.C.; Arora, T.; Grey, I.; Suen, L.K.P.; Huang, E.Y.-Z.; Li, D.; Lam, K.B.H. Perceived risk and protection from infection and depressive symptoms among healthcare workers in mainland China and Hong Kong during COVID-19. Front. Psychiatry 2020, 11, 686. [Google Scholar] [CrossRef] [PubMed]
- Bialek, S.; CDC COVID-19 Response Team. Severe outcomes among patients with coronavirus disease 2019 (COVID-19)—United States, February 12–March 16 2020. Morb. Mortal Wkly. Rep. 2020, 69, 343–346. [Google Scholar]
- American Psychological Association. Stress in America 2020: A National Mental Health Crisis. 2020. Available online: https://www.apa.org/news/press/releases/stress/2020/report-october (accessed on 22 March 2022).
- Varma, P.; Junge, M.; Meaklim, H.; Jackson, M.L. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2021, 109, 110236. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.J. Path Analysis. In Design and Analysis of Ecological Experiments; Scheiner, S.M., Gurevitch, J., Eds.; Oxford University Press: Oxford, UK, 2001; pp. 217–234. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Park, S.J. Reliability and validity of the Korean version of the Patient Health Questionnaire-9 (PHQ-9). Anxiety Mood 2010, 6, 119–124. [Google Scholar]
- Kim, N.Y.; Jeong, S.Y. Perception on and behaviors for blood-borne infection prevention among operating room nurses. J. Korean Clin. Nurs. Res. 2016, 22, 276–284. [Google Scholar] [CrossRef]
- Kwak, S.J.; Kim, N.Y. Media dependence of nursing students on COVID-19-related infection prevention behavior: Mediating effect of risk perception. Korean J. Adult Nurs. 2021, 33, 630–638. [Google Scholar] [CrossRef]
- Bae, B.R. Structural Equation Modeling with Amos 24; Chenngram Books: Seoul, Korea, 2017; pp. 76–309. [Google Scholar]
- Zhang, Y.-L.; Liang, W.; Chen, Z.-M.; Zhang, H.-M.; Zhang, J.-H.; Weng, X.-Q.; Yang, S.-C.; Zhang, L.; Shen, L.-J.; Zhang, Y.-L. Validity and reliability of Patient Health Questionnaire-9 and Patient Health Questionnaire-2 to screen for depression among college students in China. Asia Pac. Psychiatry 2013, 5, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Sidana, S. Prevalence of depression in students of a medical college in New Delhi: A cross-sectional study. Australas Med. J. 2012, 5, 247–250. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Alias, H.; Wong, L.P. Knowledge, attitudes, impact, and anxiety regarding COVID-19 infection among the public in China. Front. Public Health 2020, 8, 236. [Google Scholar] [CrossRef] [PubMed]
- Jose, R.; Narendran, M.; Bindu, A.; Beevi, N.; Manju, L.; Benny, P.V. Public perception and preparedness for the pandemic COVID 19: A health belief model approach. Clin. Epidemiol. Glob. Health 2021, 9, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Hwang, J.S. A study on the types of online community participants and their distinguishing factors: Focused on individual factors. J. Cybercommunication Acad. Soc. 2020, 37, 137–210. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Category | n (%) | Mean ± SD | Skewness | Kurtosis |
|---|---|---|---|---|---|
| Age (years) | 21.55 ± 4.59 | ||||
| Gender | Men | 47 (21.4) | |||
| Women | 173 (78.6) | ||||
| Grade | Freshmen | 42 (19.1) | |||
| Sophomore | 64 (29.1) | ||||
| Junior | 54 (24.5) | ||||
| Senior | 60 (27.3) | ||||
| Major | Health sciences | 171 (77.7) | |||
| Others | 49 (22.3) | ||||
| Class format | Face to face | 34 (15.5) | |||
| Online | 186 (84.5) | ||||
| COVID-19 infection experience | Yes | 95 (43.2) | |||
| No | 125 (56.8) | ||||
| Isolation experience (COVID-19) | Yes | 120 (54.5) | |||
| No | 100 (45.5) | ||||
| Depression | Yes | 58 (26.4) | 6.65 ± 6.38 | 0.86 | 0.17 |
| (cut-off point = 10) | No | 162 (73.6) | |||
| Health belief | 3.55 ± 0.55 | 0.05 | 0.37 | ||
| Perceived benefits | 4.20 ± 0.70 | −0.77 | 0.45 | ||
| Perceived severity | 3.18 ± 0.97 | −0.15 | −0.35 | ||
| Perceived susceptibility | 3.74 ± 0.69 | −0.70 | 1.58 | ||
| Perceived barriers | 3.07 ± 0.92 | −0.15 | −0.29 | ||
| Infection prevention behavior | 3.61 ± 0.74 | −0.24 | −0.29 |
| Variable | DE | PBE | PSE | PSU | PBA | IPB | |
|---|---|---|---|---|---|---|---|
| R | r | ||||||
| (p) | (p) | ||||||
| Depression | 1 | ||||||
| Health belief | PBE | −0.02 | 1 | ||||
| (0.773) | |||||||
| PSE | 0.21 | 0.22 | 1 | ||||
| (0.002) | (0.001) | ||||||
| PSU | 0.22 | 0.19 | 0.29 | 1 | |||
| (0.001) | (0.006) | (<0.001) | |||||
| PBA | 0.24 | 0.05 | 0.42 | 0.30 | 1 | ||
| (<0.001) | (0.492) | (<0.001) | (<0.001) | ||||
| Infection prevention behavior | 0.05 | 0.36 | 0.25 | 0.22 | 0.16 | 1 | |
| (0.423) | (<0.001) | (<0.001) | 0.001 | 0.019 |
| Endogenous Variable | Exogenous Variable | SRW | SE | CR | p | Direct β (p) | Indirect β (p) |
|---|---|---|---|---|---|---|---|
| Health belief | Depression | 0.40 | 0.04 | 2.98 | 0.003 | 0.40 (0.002) | |
| Infection prevention behavior | Depression | −0.08 | 0.09 | −0.96 | 0.337 | −0.08 (0.537) | 0.20 (0.001) |
| Health belief | 0.47 | 0.55 | 3.08 | 0.002 | 0.47 (0.004) | ||
| Goodness-of-fit statistics | χ2/DF(p) = 2.64 (<0.001), GFI = 0.90, NFI = 0.89, TLI = 0.90, CFI = 0.92, SRMR = 0.06 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, Y.-M.; Park, J.-U.; Kim, N.-Y. COVID-19 Depression and Infection Prevention Behavior among College Students: A Health Belief Perspective. Healthcare 2022, 10, 2104. https://doi.org/10.3390/healthcare10102104
Jang Y-M, Park J-U, Kim N-Y. COVID-19 Depression and Infection Prevention Behavior among College Students: A Health Belief Perspective. Healthcare. 2022; 10(10):2104. https://doi.org/10.3390/healthcare10102104
Chicago/Turabian StyleJang, Yeong-Mi, Jong-Uk Park, and Nam-Yi Kim. 2022. "COVID-19 Depression and Infection Prevention Behavior among College Students: A Health Belief Perspective" Healthcare 10, no. 10: 2104. https://doi.org/10.3390/healthcare10102104