
Referral Compliance Following a Diabetes Screening in a Dental Setting: A Scoping Review

Abstract
:1. Introduction
- the rates of referral compliance following diabetes screening in the dental setting
- the barriers and facilitators to patients’ referral compliance following diabetes screening in the dental setting
- behavioural models that have been developed to explain patient compliance to referral recommendations from OHPs following diabetes screening.
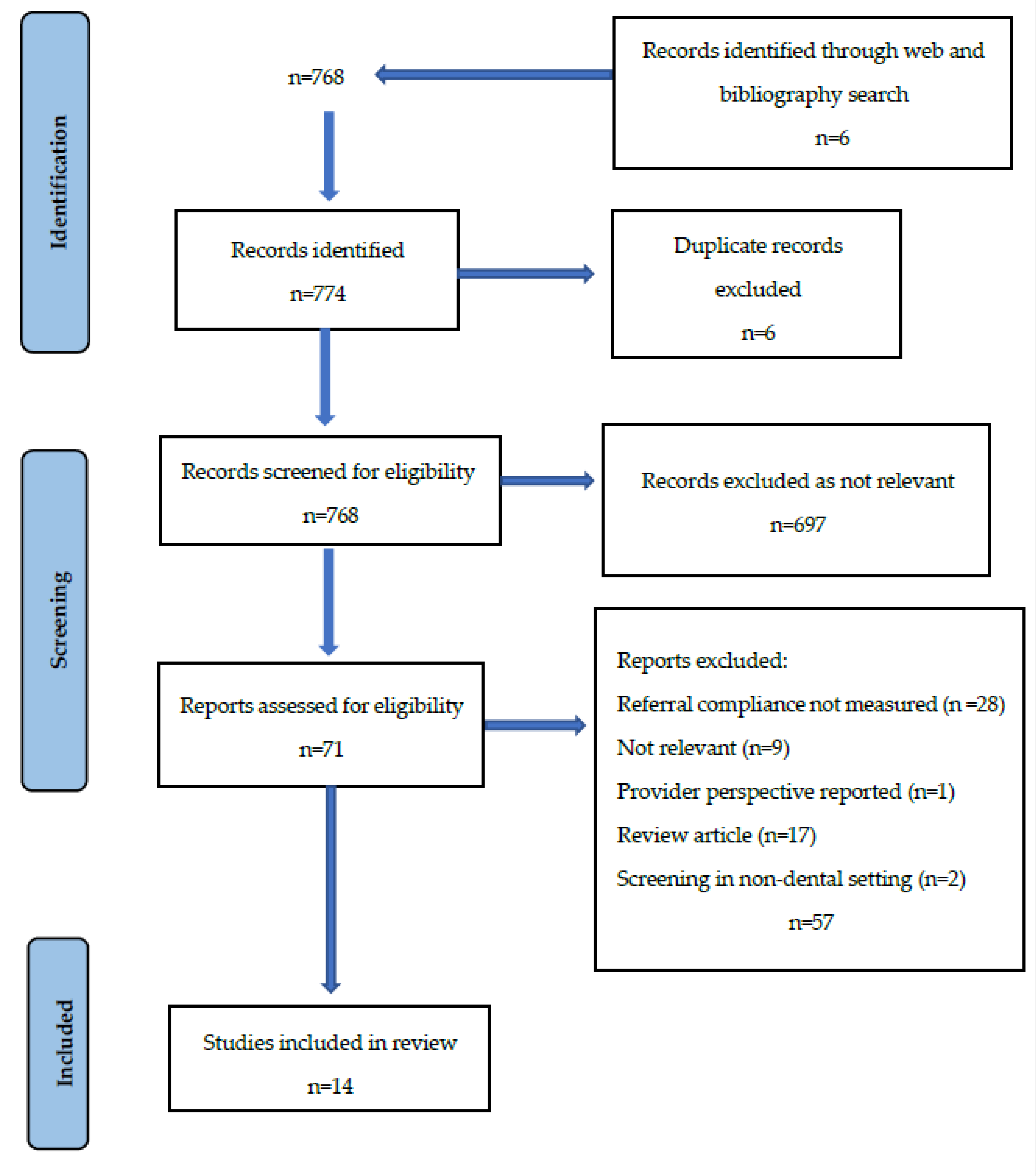
2. Methodology
- dysglycaemia or dysglyc* or type 2 diabetes or type two diabetes or diabetes mellitus type 2 or diabetes mellitus type two or type II diabetes or prediabetes or pre-diabetes or prediabetic or prediabetic state
- screen* or detect* or test or testing or diagnos* or assess*
- oral or dental or dentist* or oral hygienist* or dental hygienist* of oral health therapist* or dental therapist*
- refer* or follow-up
- comply or adhere* or attend*
3. Results
3.1. Rates of Referral Compliance following Diabetes Screening in the Dental Setting
3.2. Barriers and Facilitators to Patients’ Referral Compliance following Diabetes Screening in the Dental Setting
3.3. Behavioural Models Developed to Explain Patient’s Compliance to Referral Recommendations from OHPs following Diabetes Screening
4. Discussion
4.1. Rates of Referral Compliance
4.2. Barriers and Facilitators to Referral Compliance in the Dental Setting (Patient Factors)
4.3. Barriers and Facilitators to Referral Compliance in the Dental Setting (OHP Factors)
4.4. Behavioural Model That Explains Patient’s Compliance to Referral Recommendations
4.5. Strengths and Limitations of This Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| IDF | International Diabetes Federation |
| GP | General Medical Professional |
| AUSDRISK | Australian Type 2 Diabetes Risk Assessment Tool |
| HbA1c | glycosylated haemoglobin |
| OHP | oral health care professional, which includes dentist, dental hygienist, dental therapist and oral health therapist |
| HCP | healthcare professional |
| BCRA | breast cancer risk assessment |
References
- IDF Diabetes Atlas—2017. Available online: https://diabetesatlas.org/resources/2017-atlas.html (accessed on 5 July 2020).
- Sainsbury, E.; Shi, Y.; Flack, J.; Colagiuri, S. The diagnosis and management of diabetes in Australia: Does the “Rule of Halves” apply? Diabetes Res Clin Pract. 2020, 170, 108524. [Google Scholar] [CrossRef] [PubMed]
- Davis, W.A.; Peters, K.E.; Makepeace, A.; Griffiths, S.; Bundell, C.; Grant, S.F.A.; Ellard, S.; Hattersley, A.T.; Chubb, S.A.P.; Bruce, D.G.; et al. Prevalence of diabetes in Australia: Insights from the Fremantle Diabetes Study Phase II. Intern. Med. J. 2018, 48, 803–809. [Google Scholar] [CrossRef]
- Twigg, S.M.; Kamp, M.C.; Davis, T.M.; Neylon, E.K.; Flack, J.R. Prediabetes: A position statement from the Australian Diabetes Society and Australian Diabetes Educators Association. Med. J. Aust. 2007, 186, 461–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twigg, S.; Wong, J. The imperative to prevent diabetes complications: A broadening spectrum and an increasing burden despite improved outcomes. Med. J. Aust. 2015, 202, 300–304. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.M.Y.; Goode, B.; Nørtoft, E.; Shaw, J.E.; Magliano, D.J.; Colagiuri, S. The cost of diabetes and obesity in Australia. J. Med. Econ. 2018, 21, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International diabetes Federation and the European Federation of Periodontology. Diabetes Res. Clin. Pract. 2018, 137, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.S.; Yl€ostalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Periodontol. 2013, 84, S135–S152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, T.C.; Weldon, J.C.; Worthington, H.V.; Needleman, I.; Wild, S.H.; Moles, D.R.; Stevenson, B.; Furness, S.; Iheozor-Ejiofor, Z. Treatment of periodontal disease for glycaemic control in people with diabetes mellitus. Cochrane Database Syst. Rev. 2015, 11, CD004714. [Google Scholar] [CrossRef]
- Bell, K.; Shaw, J.E.; Maple-Brown, L.; Ferris, W.; Gray, S.; Murfet, G.; Flavel, R.; Maynard, B.; Ryrie, H.; Pritchard, B.; et al. A position statement on screening and management of prediabetes in adults in primary care in Australia. Diabetes Res. Clin. Pract. 2020, 164, 108188. [Google Scholar] [CrossRef]
- Huang, Y.; Cai, X.; Mai, W.; Li, M.; Hu, Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: Systematic review and meta-analysis. BMJ 2016, 355, i5953. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y.; Kiyohara, Y.; Kato, I.; Kubo, M.; Iida, M.; Koga, T. The severity of periodontal disease is associated with the development of glucose intolerance in non-diabetics: The Hisayama study. J. Dent. Res. 2004, 83, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Andriankaja, O.M.; Joshipura, K. Potential association between prediabetic conditions and gingival and/or periodontal inflammation. J. Diabetes Investig. 2014, 5, 108–114. [Google Scholar] [CrossRef]
- Roche, M.M.; Wang, P.P. Factors associated with a diabetes diagnosis and late diabetes diagnosis for males and females. J. Clin. Transl. Endocrinol. 2014, 1, 77–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization; Wilson, J.M.G.; Jungner, G. The Principles and Practice of Screening for Disease; World Health Organization: Geneva, Switzerland, 1966. [Google Scholar]
- The Royal Australian College of General Practitioners. Management of Type 2 Diabetes: A Handbook for General Practice; The Royal Australian College of General Practitioners: East Melbourne, Australia, 2020. [Google Scholar]
- Wong, K.C.; Brown, A.M.; Li, S.C.H. Ausdrisk: Application in General Practice. Aust. Fam. Physician 2011, 40, 524–526. [Google Scholar] [PubMed]
- Chen, L.; Magliano, D.J.; Balkau, B.; Colagiuri, S.; Zimmet, P.Z.; Tonkin, A.M.; Mitchell, P.; Phillips, P.J.; Shaw, J.E. AUSDRISK: An Australian Type 2 Diabetes Risk Assessment Tool based on demographic, lifestyle and simple anthropometric measures. Med. J. Aust. 2010, 192, 197–202. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Oral Health and Dental Care in Australia; AIHW: Canberra, Australia, 2020. [Google Scholar]
- Chrisopoulos, S.; Harford, J.E.; Ellershaw, A. Oral Health and Dental Care in Australia: Key Facts and Figures 2015; AIHW: Canberra, Australia, 2016. [Google Scholar]
- Bossart, M.; Calley, K.H.; Gurenlian, J.R.; Mason, B.; Ferguson, R.E.; Peterson, T. A pilot study of an HbA1c chairside screening protocol for diabetes in patients with chronic periodontitis: The dental hygienist’s role. Int. J. Dent. Hyg. 2016, 14, 98–107. [Google Scholar] [CrossRef]
- Engstrom, S.; Berne, C.; Gahnberg, L.; Svardsudd, K. Effectiveness of screening for diabetes mellitus in dental health care. Diabet. Med. 2013, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Franck, S.D.; Stolberg, R.L.; Bilich, L.A.; Payne, L.E. Point-of-care HbA1c screening predicts diabetic status of dental patients. J. Dent. Hyg. 2014, 88, 42–52. [Google Scholar] [PubMed]
- Bould, K.; Scott, S.E.; Dunne, S.; Asimakopoulou, K. Uptake of screening for type 2 diabetes risk in general dental practice; an exploratory study. Br. Dent. J. 2017, 222, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Muirhead, V.; Weston-Price, S.; Fortunesurgeries, F. Type 2 diabetes risk screening in dental practice settings: A pilot study. Br. Dent. J. 2014, 216, E15. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Reiss, L.; Schmalz, G.; Krause, F.; Haak, R.; Mausberg, R.F. Different views of dentists and general medical practitioners on dental care for patients with diabetes mellitus and coronary heart diseases: Results of a questionnaire-based survey in a district of Germany. Int. Dent. J. 2018, 68, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Biethman, R.K.; Pandarakalam, C.; Garcia, M.N.; Whitener, S.; Hildebolt, C.F. Screening for Diabetes in a Dental School Clinic to Assess Interprofessional Communication Between Physicians and Dental Students. J. Dent. Educ. 2017, 81, 1062–1067. [Google Scholar] [CrossRef] [Green Version]
- Rosedale, M.T.; Strauss, S.M.; Kaur, N.; Knight, C.; Malaspina, D. Follow-up with primary care providers for elevated glycated haemoglobin identified at the dental visit. Int. J. Dent. Hyg. 2017, 15, e52–e60. [Google Scholar] [CrossRef] [PubMed]
- Herman, W.H.; Ye, W.; Griffin, S.J.; Simmons, R.K.; Davies, M.J.; Khunti, K.; Rutten, G.E.H.M.; Sandbaek, A.; Lauritzen, T.; Borch-Johnsen, K.; et al. Early Detection and Treatment of Type 2 Diabetes Reduce Cardiovascular Morbidity and Mortality: A Simulation of the Results of the Anglo-Danish-Dutch Study of Intensive Treatment in People With Screen-Detected Diabetes in Primary Care (ADDITION-Europe). Diabetes Care 2015, 38, 1449–1455. [Google Scholar] [CrossRef] [Green Version]
- Genco, R.J.; Schifferle, R.E.; Dunford, R.G.; Falkner, K.L.; Hsu, W.C.; Balukjian, J. Screening for diabetes mellitus in dental practices: A field trial. J. Am. Dent. Assoc. 2014, 145, 57–64. [Google Scholar] [CrossRef] [PubMed]
- AlGhamdi, A.S.T.; Merdad, K.; Sonbul, H.; Bukhari, S.M.N.; Elias, W.Y. Dental Clinics as Potent Sources for Screening Undiagnosed Diabetes and Prediabetes. Am. J. Med. Sci. 2013, 345, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Mariño, R.; Priede, A.; King, M.; Adams, G.G.; Sicari, M.; Morgan, M. Oral health professionals screening for undiagnosed type-2 diabetes and prediabetes: The iDENTify study. BMC Endocr Disord. 2022, 18, 22–183. [Google Scholar] [CrossRef]
- Montero, E.; Matesanz, P.; Nobili, A.; Luis Herrera-Pombo, J.; Sanz, M.; Guerrero, A.; Bujaldón, A.; Herrera, D.; SEPA Research Network of Dental Clinics; Campos, L.; et al. Screening of undiagnosed hyperglycaemia in the dental setting: The DiabetRisk study. A field trial. J. Clin. Periodontol. 2020, 48, 378–388. [Google Scholar] [CrossRef]
- Lalla, E.; Cheng, B.; Kunzel, C.; Burkett, S.; Ferraro, A.; Lamster, I.B. Six-month outcomes in dental patients identified with hyperglycaemia: A randomized clinical trial. J. Clin. Periodontol. 2015, 42, 228–235. [Google Scholar] [CrossRef]
- Khatib, R.; Schwalm, J.D.; Yusuf, S.; Haynes, R.B.; McKee, M.; Khan, M.; Nieuwlaat, R. Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: A systematic review and meta-analysis of qualitative and quantitative studies. PLoS ONE 2014, 9, e84238. [Google Scholar] [CrossRef]
- Willis, A.R.P.; Gray, L.J.; Davies, M.; Khunti, K. The Effectiveness of Screening for Diabetes and Cardiovascular Disease Risk Factors in a Community Pharmacy Setting. PLoS ONE 2014, 9, e91157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginde, A.A.; Delaney, K.E.; Lieberman, R.M.; Vanderweil, S.G.; Camargo, C.A., Jr. Estimated risk for undiagnosed diabetes in the emergency department: A multicenter survey. Acad. Emerg. Med. 2007, 14, 492–495. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.M.; Vallipuram, J.; Baswick, B. Incidental findings of elevated random plasma glucose in the ED as a prompt for outpatient diabetes screening: A retrospective study. BMJ Open. Dec. 2013, 3, e003486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saglam-Aydinatay, B.; Uysal, S.; Taner, T. Facilitators and barriers to referral compliance among dental patients with increased risk of obstructive sleep apnea. Acta Odontol. Scand. 2018, 76, 86–91. [Google Scholar] [CrossRef]
- Dillow, K.; Essick, G.; Sanders, A.; Sheats, R.; Brame, J. Patient response to sleep apnea screening in a dental practice. J. Public Health Dent. 2016, 77, 13–20. [Google Scholar] [CrossRef]
- Sia, J.T.; Gan, A.T.L.; Soh, B.P.; Fenwick, E.; Quah, J.; Sahil, T.; Tao, Y.; Tan, N.C.; Sabanayagam, C.; Lamoureux, E.L.; et al. Rates and Predictors of Nonadherence to Postophthalmic Screening Tertiary Referrals in Patients with Type 2 Diabetes. Transl. Vis. Sci. Technol. 2020, 9, 15. [Google Scholar] [CrossRef]
- Maiman, L.A.; Hildreth, N.G.; Cox, C.; Greenland, P. Improving referral compliance after public cholesterol screening. Am. J. Public Health 1992, 82, 804–809. [Google Scholar] [CrossRef] [Green Version]
- Khanna, N.; Phillips, M.D. Adherence to care plan in women with abnormal Papanicolaou smears: A review of barriers and interventions. J. Am. Board Fam. Pract. 2001, 14, 123–130. [Google Scholar]
- Hui, S.K.; Miller, S.M.; Wen, K.Y.; Fang, Z.; Li, T.; Buzaglo, J.; Hernandez, E. Psychosocial barriers to follow-up adherence after an abnormal cervical cytology test result among low-income, inner-city women. J. Prim. Care Community Health 2014, 5, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Paek, H.-J.; Hove, T. Risk Perceptions and Risk Characteristics; Springer: Berlin, Germany, 2017. [Google Scholar]
- Eborall, H.; Stone, M.; Aujla, N.; Taub, N.; Davies, M.; Khunti, K.; Eborall, H.; Stone, M.; Aujla, N.; Taub, N.; et al. Influences on the uptake of diabetes screening: A qualitative study in primary care. Br. J. Gen. Pract. 2012, 62, 204–211. [Google Scholar] [CrossRef]
- Morman, N.A.; Byrne, L.; Collins, C.; Reynolds, K.; Bell, J.G. Breast Cancer Risk Assessment at the Time of Screening Mammography: Perceptions and Clinical Management Outcomes for Women at High Risk. J. Genet. Couns. 2017, 26, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Goto, E.; Ishikawa, H.; Okuhara, T.; Kato, M.; Okada, M.; Kiuchi, T. Factors associated with adherence to recommendations to visit a physician after annual health checkups among Japanese employees: A cross-sectional observational study. Ind. Health 2018, 56, 155–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, E.B.; Ostroff, J.S.; DuHamel, K.N.; D’Agostino, T.A.; Hernandez, M.; Canzon, M.R.; Byland, C.L. Impact of provider-patient communication on cancer screening adherence: A systematic review. Prev. Med. 2016, 93, 96–105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Main Author Date | Objectives | Country | Screening Instruments Used | % Referral Compliance | Barriers and Facilitators to Referral Compliance | Results and Conclusions |
|---|---|---|---|---|---|---|
| Bossart et al., 2015 [21] | Assess the effectiveness, convenience and cost of POC diabetes screenings performed by a dental hygienist for patients with periodontitis. | USA | Periodontal exam, risk assessment and POC-Hb A1c | 53% | Waiting for next GP visit and time constraints | 34% (n = 17) participants screened positive for dysglycaemia. Diabetes screening by dental hygienists is effective and convenient for identifying dyglycaemia. |
| Engstrom et al., 2013 [22] | Test the effectiveness of diabetes screening in a collaborative framework between oral and primary health care. | Sweden | Risk assessment using BMI, RCBG, and RPG. | 90% | Not reported | 9 individuals were diagnosed with T2D. Diabetes screening was successful in terms of response rate and referral compliance. |
| Franck et al., 2014 [23] | To investigate the ability to screen dental patients for T2D or PD. | USA | Risk assessment Survey. High-risk received POC and labor Hb A1c | 55% | Not reported | 28 participants had prediabetes. identified patients with dysglycaemia. |
| Bould et al., 2016 [24] | To determine dental patients’ uptake of two screening tools FR and POC-HbA1c. in general dental practice. | UK | FR screening tool and POC-HbA1c | 60% | Significant association between number of ‘at risk’ screening results received and whether or not patient attended follow-up. | 258 participants identified as at risk of diabetes. A two-step method of diabetes screening was acceptable to patients, and the majority complied with referral advice. Patients were three times more likely to contact their GP if they received a positive risk result on both screening tools. |
| Wright et al., 2013 [25] | To assess the feasibility of implementing a T2D diabetes risk assessment screening in dental settings using the NICE guidance tool | UK | Risk assessment | 26% (30.6% moderate-risk and 20% of high-risk patients attended follow-up) | Barriers to medical follow-up: misplacing the referral letter, being too busy, being away, delaying the appointment until after Ramadan and perception condition was not ‘serious enough’ to visit their GP. | Diabetes screening is feasible in dental settings. Amongst the challenges to this approach for the OHPs are time constraints, limited manpower and low referral compliance |
| Ziebolz et al., 2019 [26] | Investigate the efficacy of T2D screening based on questionnaire replies | Germany | FR-positive patients were referred to a specialist | 55% | Not reported | The survey tool identified patients with T2D and prediabetes and is suitable for diabetes screening in dental practices. Difficult to motivate individuals to attend medical follow-up |
| Biethman et al., [27] | To evaluate GPs’ responses to requests for information regarding follow-up results after diabetes screening in a dental setting. A secondary aim was to evaluate patients’ referral compliance. | USA | POC Hb A 1C | 59% | Unable to predict patients’ compliance with seeking follow-up with their GPs. | Most patients complied with their OHP’s advice to seek medical follow-up after diabetes screening. A single written request from an OHP to the GP to share the results may be insufficient and a phone call may be a more effective communication method. |
| Rosedale et al., 2017 [28] | To examine patient experiences after receiving positive diabetes screening results at a dental clinic, whether they attended medical follow-up and facilitators and barriers to referral compliance. | USA | Hb A1c | 54 % | Facilitators: positive screening result viewed as an opportunity to act, 3-month follow-up/ reminder call from OHP. Barriers: Positive screening results perceived as a burden, lack of knowledge about diabetes, not understanding the importance of follow-up, busyness, financial concerns, fear and denial. | Patients and OHPs believe the dental setting is an acceptable and feasible site for diabetes screening. A limitation of diabetes screening is the extent to which patients’ follow-up positive screening results with their GPs. |
| Herman et al., 2015 [29] | To develop and validate a tool to screen for PD and T2D in dental practices | USA | Risk assessment survey, RCBG and periodontal exam | 26% | Those that complied were significantly older than those who did not. More likely to comply if a previous history of tooth loss or dyslipidaemia | 30 % of patients ≥30 years old seen in general dental practices had dysglycaemia. Screening for dysglycaemia can be used to identify high-risk patients. |
| Genco et al., 2014 [30] | To assess patient compliance with referral to GPs for diabetes diagnosis | USA | Risk assessment and POC-HbA1c | 35% | 78.8 % of patients from community clinics and 21.5 % were referred from private dental clinics attended medical follow-ups. Patients reported they declined to seek follow-up without giving an explicit reason. | Patients and OHPs support diabetes screening in the dental setting. Low referral compliance occurred in the private dental setting and good compliance in the community health centre setting. The reasons for low referral compliance need to be investigated and addressed before screening for diabetes in the dental setting can be advocated. |
| Al Ghamadi et al., 2013 [31] | To assess the efficacy of the dental setting for T2D and PD screening | Saudi Arabia | Random blood glucose levels (RBGLs) were recorded. | 84% | Not reported | 16.4 % undiagnosed T2D and 15.8 % PD among patients visiting dental clinics |
| Marino et al., 2020 [32] | To develop and evaluate an innovative approach for identifying pre-diabetes and type 2 diabetes within the private oral health setting. | Australia | AUSDRISK risk assessment tool | 25% | Cost, personal issues, other health concerns taking priority and COVID-19, were named as barriers to attending medical follow-ups. | Six individuals were diagnosed with prediabetes. T2D screening in a dental setting is well-accepted and effective. However, developing referral pathways, both to and from GPs, as well as maximising follow-ups is required. |
| Montero et al., 2020 [33] | To evaluate the efficacy of different screening protocols for undiagnosed dysglycaemia in the dental setting | Spain | FR screening tool and periodontal exam and POC-HbA1c | Results of 23 referred patients were unknown, for some, this may be due to referral non-compliance. | Not reported | 8.5% of individuals were diagnosed with dysglycaemia. The screening protocol was feasible and effective in identifying participants with dysglycaemia in the dental setting. |
| Lalla et al., 2015 [34] | To assess an approach to improving behavioural and glycaemic outcomes in dental patients with diabetes risk factors and previously undiagnosed hyperglycaemia | USA | Risk assessment, periodontal exam, and Hb A1c | 84% | Not reported | At 6 months most of the participants reported having attended a GP and 49% reported at least one positive lifestyle change. In participants identified as at risk of diabetes, HbA1c was significantly reduced. |
| Barriers to Referral Compliance | Study |
|---|---|
| Referral pathway issues (e.g., negative perception of services losing the referral, no longer in the country) | [21,25,32] |
| Too busy to attend | [21,25,28] |
| Cultural/religious reasons (e.g Ramadan) | [25] |
| Lack of knowledge and awareness of the condition | [25,28] |
| Fears and distress about the results | [28] |
| Cost of follow-up appointment | [28,32] |
| Other health issues took priority | [32] |
| Patient perceived positive screening result as a burden | [28] |
| Facilitators to Referral Compliance | Study |
|---|---|
| Good HCP–patient interaction | [28] |
| Good interprofessional communication between dental and medical professional | [28] |
| Patient perceiving positive screening as an opportunity to act | [28] |
| Observing family members with diabetes or desire to be a role model for family members | [28] |
| History of tooth loss and dyslipidaemia | [28] |
| Location of screening; Community dental clinic | [30] |
| Receiving a reminder to follow-up | [28] |
| Multiple ‘at risk’ screening results received | [24] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priede, A.; Lau, P.; Darby, I.; Morgan, M.; Mariño, R. Referral Compliance Following a Diabetes Screening in a Dental Setting: A Scoping Review. Healthcare 2022, 10, 2020. https://doi.org/10.3390/healthcare10102020
Priede A, Lau P, Darby I, Morgan M, Mariño R. Referral Compliance Following a Diabetes Screening in a Dental Setting: A Scoping Review. Healthcare. 2022; 10(10):2020. https://doi.org/10.3390/healthcare10102020
Chicago/Turabian StylePriede, Andre, Phyllis Lau, Ivan Darby, Mike Morgan, and Rodrigo Mariño. 2022. "Referral Compliance Following a Diabetes Screening in a Dental Setting: A Scoping Review" Healthcare 10, no. 10: 2020. https://doi.org/10.3390/healthcare10102020