
Impact of Active Physiotherapy Rehabilitation on Pain and Global and Functional Improvement 1–2 Months after Lumbar Disk Surgery: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Methods
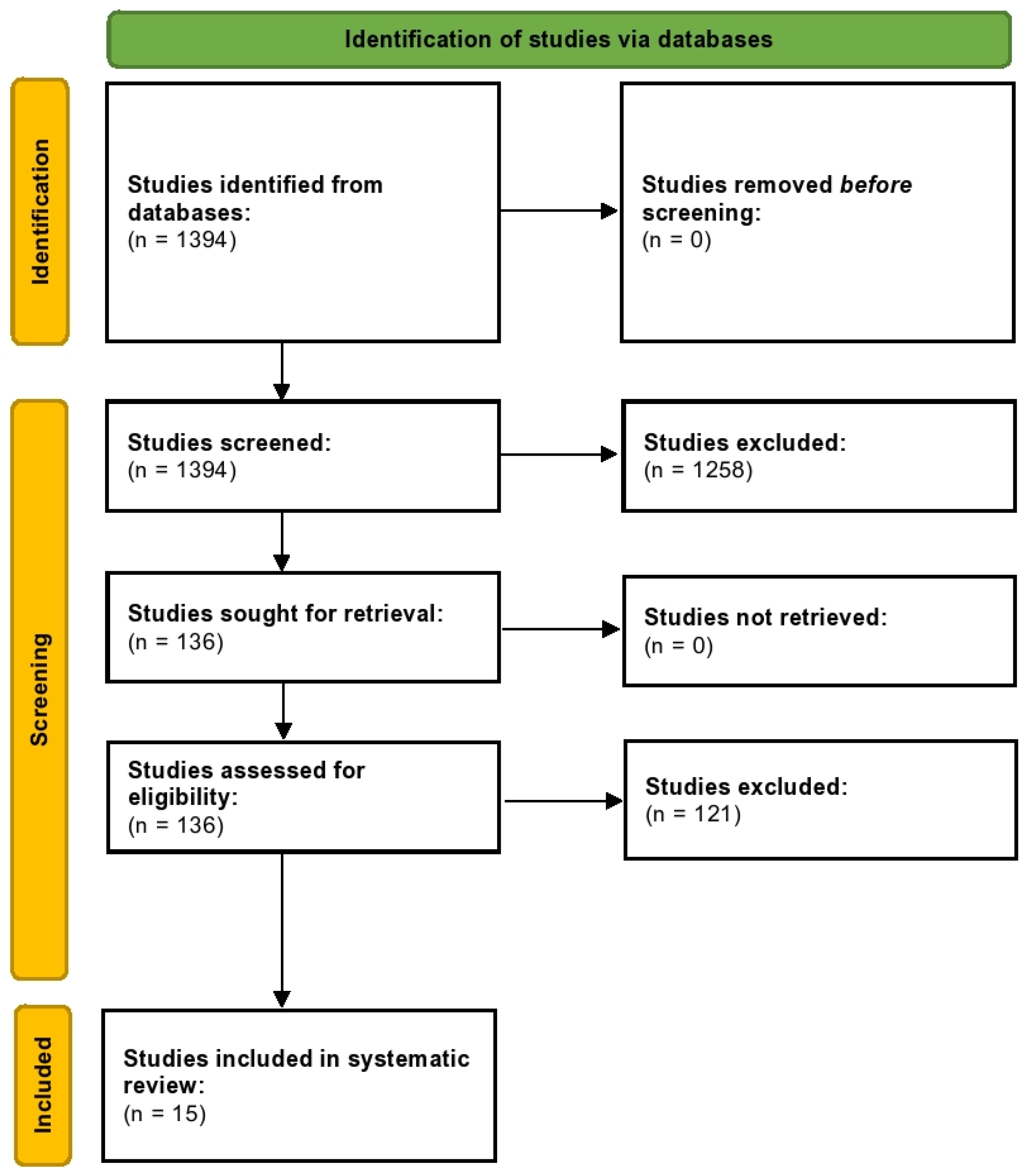
2.1. Search Strategy
2.2. Types of Studies Included
2.3. Data Extraction (Selection and Coding)
2.4. Risk of Bias (Quality) Assessment
2.5. Protocol Registration and Role of Funding
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sr. No. | Author, Year | Aim | Methodology | Participants | Interventions | Outcomes | GRADE Scores |
|---|---|---|---|---|---|---|---|
| 1 | Atlanta et al., 1986 [15] | To examine the one-year postoperative results in patients operated on for lumbar disc herniation with comprehensive rehabilitation and normal care facilities. | Randomization by age (>40 years) and sex stratification before the operation; N = 212 | Participants underwent first-time disc surgery for lumbar prolapse patients; the operation was carried out through an interlaminar trepanation and sequesters, and any loose nucleus pulposus material was removed. | IG = PR started four weeks after surgery (N = 106): multifactorial rehabilitation (physiatrist, physical and occupational therapists, psychologist, social worker) for two weeks, “Intensive Back School.” Encouraging physical activities; CG = Usual care. | At 1-year follow-up—Global perceived effect (five-point scale): ‘Much better or Better’-IG = 88%, CG = 83%. Occupational handicap (WHO scale) and total sick leave during a one-year follow-up period. No significant differences between groups. Reoperations: IG = 4/106, CG = 4/106. | Moderate-quality evidence |
| 2 | Donceel et al., 1999 [16] | To compare rehabilitation-oriented approaches focused on early mobilization and early resumption of professional activities. | Randomization was done by computer-generated number; N = 710 | The mean age of participants was 39.2 years and patients underwent open lumbar discectomy. Rehabilitative interventions started six weeks post-surgery. | IG = At first visit six weeks after surgery, functional evaluation, natural history, and expected work incapacity was discussed. Patients were encouraged and stimulated with personal activities and early mobilization—CG = Usual care. | On return to work at the 52nd week post-intervention, improvement was noted in 89.9% (IG) and 81.9% (CG) of patients; the differences were significant. | High-quality evidence |
| 3 | Danielsen et al., 2000 [17] | To assess the effect of an early regimen of vigorous medical exercise compared with an ordinary care program. | Randomization by a number table; N = 63. | The patients were aged 22 to 58 years, four weeks after the operation for lumbar disc herniation (arcotomy in 36 patients, microsurgical in 27 patients. | IG = Enrolled into the rehabilitation program from weeks 4–12, three times per week × 40 min per session exercise therapy; exclusively active, no manual intervention or physical therapist, strengthen muscles (various apparatus), participant tailored; N = 39. CG = weeks 1–3 comprised of standard programs, follow-up consultation for clinical course and clinical examination with a physical therapist every two weeks for eight weeks, with a mild home exercise program, relaxing and resting the back, and gradually resuming daily activities; N = 24. | Pain intensity (VAS) at 6 months: IG = 3.7 (95% CI: 2.7–4.7), CG = 2.0 (95% CI: 0.7–3.3). Functional status (RDQ): IG = 8.9 (7–10.8), CG = 5.4 (3–7.8). Pain at 12 months: IG = 3.2 (2.1–4.3), CG = 1.8 (0.5–3.1); (RDQ) IG = 8.7 (6.8–10.6), CG = 5.3 (2.6–8). Absolute RDQ values had a minor advantage for IG at 6 and 12 months. Pain scores were significantly better for IG at 6 months. A larger no. of participants in IG resumed daily activities (WONCA scale) at 6 months. | High-quality evidence |
| 4 | Dolan et al., 2000 [18] | To determine the effects of a postoperative exercise program on pain, disability, psychological status, and spinal function. | Blind randomization; N = 20. | The patients were aged between 18 and 60 with radiological evidence of disc prolapse associated with sciatica of fewer than 12 months duration; they underwent microdiscectomy, followed by six weeks of routine postoperative care. In the exercise group, the IG underwent a 4-week exercise program concentrating on improving strength and endurance of the back and abdominal muscles and mobility of the spine and hips. | IG = Underwent an exercise program by an experienced physiotherapist, two one-hour sessions per week for four weeks (commenced six weeks after surgery); there were general aerobic exercises, stretching exercises, extension exercises, strength and endurance exercises (back and abdominal); N = 9. CG = acquired no further treatment; N = 11 | Pain intensity (VAS): Reductions were noted in both CG and IG 6 weeks after surgery, but IG showed a further decrease. Between IG and CG, at 12 months, pain (diary): was significantly less in IG (p < 0.05). Functional status (ranging from 0–75) was improved in both groups: IG = 54 ± 24, CG = 50 ± 25. Little behavioral outcome changes in IG and CG, with no differences in muscle endurance and ROM. | Low-quality evidence |
| 5 | Ostelo et al., 2003 [19] | To note the effectiveness of behavioral graded activity provided by physiotherapists for patients after first-time lumbar disc surgery. | Randomization was done a-priori; N = 105. | The patients were aged 18 to 65, still suffering complaints six weeks post-surgery, which had restrictions in normal activities of daily living. | IG: Using graded activity and positive reinforcement with time contingency management, the patients underwent behavioral graded activity (operant therapy); N = 52. Using baseline measurements, the individual-graded exercise training program was tailored. There was a total of 18 × 30-min sessions over three months. CG = Usual care with exercise trunk muscles, mobilization exercises with 18 × 30 sessions; N = 53. | Global perceived effect: 65% in IG recovered compared to 62% in CG. Functional status (24-item RDQ): mean (SD); −6.4 (5.8) ~IG vs. −6.1 (5.6) ~CG. Pain back (VAS): −13.7 (31.4) vs. −20.9 (31.6). | Moderate-quality evidence |
| 6 | Yilmaz et al., 2003 [20] | To determine the efficacy of dynamic lumbar stabilization exercises in patients with lumbar microdiscectomy. | Patients were randomized into three groups; N = 42. | The patients were between 20 and 60 years old, including one month after first-time lumbar disc surgery. The follow-up was short-term. | IG-1 = Underwent dynamic lumbar stabilization exercise for eight weeks under supervision; N = 14. IG-2 = Partook in the flexion–extension (Williams–McKenzie) home program for eight weeks; N = 14. CG = No treatment. | Pain (VAS scores): IG-1 = 1.14 ± 0.86, IG-2 = 2.93 ± 2.02, CG = 4.29 ± 1.9. Functional status (scores on Modified Oswestry at post-treatment): IG-1 = 8.5 ± 4.8, IG-2 = 12.93 ± 4.23, CG = 17.71 ± 6.23. | Low-quality evidence |
| 7 | Choi et al., 2005 [21] | To identify the effects of postoperative early isolated lumbar extension muscle-strengthening program on pain, disability, return to work, and back muscle power after operation for the herniated lumbar disc. | Patients were randomized; N = 75. | The mean age of the patients was 46.09 years; they had leg pain not responding to conservative treatment, and had undergone discectomy. | IG = Advice, lumbar extension handout, home exercise for six weeks, and intensive training for 12 weeks (N = 35). MedX system, which restricts hip and pelvic motion. CG = Advice, lumbar extension handout, six weeks of home-based exercise, continued for another 12 weeks (N = 40). | Pain intensity (VAS) largely decreased in both IG (2.51) and CG (4.3) after 12 weeks of extension exercise (p < 0.05). Functional status (ODI): Postoperative ODI scores were improved compared with preoperative ODI scores IG = 24.6 and CG = 30.6 post-treatment (non-significant). Return to work: More than 92% returned to work within six months after surgery; within four months, 87% from IG and 24% from CG returned to work. | Moderate-quality evidence |
| 8 | Filiz et al., 2005 [22] | To compare two different exercise programs versus a control group, after lumbar disc surgery. | Randomized into three groups based on a blinded envelop-based system; N = 60. | Across all three arms, patients were included one month after first-time lumbar disc surgery, aged between 20 and 50 years. The follow-up was short-term in nature. | IG-1 = Underwent an intensive exercise program and back school education under supervision for eight weeks, three days a week with sessions of 1.5 h each, N = 20; IG-2 = were given back education and trained on McKenzie and Williams exercise with a home program for eight weeks to practice, N = 20; CG = No treatment, N = 20. | Pain (post-treatment score on VAS): IG-1 = 4.5 ± 1.6, IG-2 = 12 ± 3.7, CG = 13.3 ± 7.3. Functional status (post-treatment scores on Modified Oswestry): IG-1 = 7.1 ± 4.9, IG-2 = 11.7, CG = 15.1 ± 8.6. RTW (in days): IG-1 = 56.07 ± 18.66, IG-2 = 75 ± 24.9, CG = 86.2 ± 27.1. | Moderate-quality evidence |
| 9 | Hakkinen et al., 2005 [23] | To assess the adherence to and effects of a 12-month combined strength and stretching home exercise regimen versus stretching alone on patient outcome after lumbar disc surgery. | Patients were randomly assigned to IG and CG; N = 126. | The patients were enrolled two months after their first lumbar disc surgery; they were not pain-free (VAS > 10 mm). | IG = Placed with a home-based exercise program for 12 months. The patients were instructed to stretch and stabilize three times, with strength training, instructed to perform two sets of exercises twice a week. CG = Was instructed on regular stretching and stabilization three times. | At 12 months, improvement in back pain (100-mm VAS) was noted in IG = 4 mm (−11 to 5), CG = 1 mm (−7 to 9), leg pain (100-mm VAS), IG = −2 (−7 to 7), CG = −2 (−7 to 3). Improvement in disability (ODI) was IG = 3 mm (−6 to 1), CG = −2 (−5 to 1). | High-quality evidence |
| 10 | Donaldson et al., 2006 [24] | To compare the outcomes of formal post-surgical exercise-based rehabilitation to usual post-procedural surgical advice. | Randomization was carried out into two groups; N = 93. | The patients had a mean age of 41 and had standard open lumbar discectomy via the Spengler technique. | IG = Intervened at six weeks post-op and underwent 6-months of progressive training with 3sets of repetitions per exercise. There were 3 phases: conditioning, hypertrophy, and strength; N = 47. CG = Was given surgical advice; N = 46. | All values were noted at 58 weeks. Functional status (ODI): IG = 11.66 ± 2.25, CG = 12 ± 1.84. Functional status (RMDQ): IG = 4.03 ± 0.91, CG = 4.53 ± 0.74. The differences in SF36 [physical and mental category] were non-significant. Median time to return to work IG = 35 days and CG = 37 days. | Moderate-quality evidence |
| 11 | Erdogmus et al., 2007 [25] | To test the effectiveness of physiotherapy-based rehabilitation after lumbar disc surgery. | Randomized into three groups; N = 120. | The patients had a mean age of 41.3 years; they underwent standard laminectomy and micro-discectomy. | IG-1 = Underwent physiotherapy-based rehabilitative program starting 4–6 weeks postoperatively for a total of 12 weeks; N = 40. IG-2 = Underwent sham therapy ‘neck massage’ for 30 min per session; N = 40. CG = standard care; N = 40. | Post-treatment scores on functional status (LBPRS): IG-1 = −15.98 (−18.02 to −13.9), IG-2 = −13.23 (−15.35 to −11.1), CG = −12.15 (−14.59 to −9.71). | High-quality evidence |
| 12 | Kulig et al., 2009 [26] | To examine the effectiveness of a new interventional protocol to improve functional performance in patients who have undergone a single-level lumbar microdiscectomy. | Patients were randomly allocated to receive education only or exercise and education; N = 98. | The participants had a mean age of 40.3 years and underwent microdiscectomy. | IG = Enrolled into the USC Spine Exercise Program and a ‘back care education session. The intervention started 4–6 weeks after surgery, with three months of training sessions per week. The sessions involved back extensor strength and endurance training (using a variable-angle Roman chair) and mat and therapeutic exercise training; N = 51. CG = had a one-hour back care education single session; N = 47. | Functional status (ODI): IG = −18.4 (−22.5 to −14.3), CG = −9.4 (−13.0 to −5.8). | Moderate-quality evidence |
| 13 | McGregor et al., 2011 [27] | To evaluate the benefits of rehabilitation and an education booklet in the postoperative management of patients undergoing discectomy or lateral nerve root decompression, compared to standard of care. | The patients were randomized into four groups; N = 338. | The overall mean age of all participants was 53.75 years. The patients underwent routine discectomy to confirm root symptoms using signs and MRI results of lumbar disc herniation. | IG-1 = Intervention started at 6–8 weeks post-op, consisting of twelve, 1-h classes including aerobic fitness, stability exercises, stretching, stability exercises, endurance and strengthening training for the back, abdominal, and leg muscles, ergonomic training, and advice on living and setting targets; N = 86. IG-2 = Underwent rehabilitation and booklets; N = 91: IG-3 = Were intervened with educational booklets ‘Your Back Operation’; N = 70. CG = routine practice; N = 91. | Functional status (12-month scores on ODI). IG-1 = 24 ± 21, IG-2 = 26 ± 22, IG-3 = 25 ± 20, CG = 27 ± 23. Pain intensity (VAS). IG-1 = 72 ± 24, IG-2 = 71 ± 26, IG-3 = 72 ± 23, CG = 67 ± 26. | High-quality evidence |
| 14 | Oestergaard et al., 2013 [28] | To examine the effect of early initiation of rehabilitation after instrumented lumbar spinal fusion. | Block randomized; two groups intervened at 6 and 12 weeks post-surgery with no control group; N = 82. | The mean age of all participants was 52 years; all patients planned for an instrumented lumbar spinal fusion due to degenerative disc disease or spondylolisthesis grade I or II were randomized at 6 or 12 weeks after surgery. | IG = Enrolled at 6 or 12 weeks post-surgery, with each session targeting pain and physical incapacity, problems, and solutions in performing ADL. The physiotherapist advised home exercises, focusing on active stability training of the truncus and large muscle groups. | Functional status (ODI) at 6-month follow-up. IG-1, the 6-week group, had achieved a reduction of 6 points; IG-2, the 12-week group, achieved a decrease of 15 points. At 1-year follow-up, IG-1 had a decrease of 5 points, and IG-2 had a reduction of 20 points. | Low-quality evidence |
| 15 | Demir et al., 2014 [29] | To investigate the effects of supervised dynamic lumbar stabilization exercises during postoperative rehabilitation on pain, spinal mobility, and functional status among patients undergoing lumbar microdiscectomy for the first time. | Randomization into two groups; N = 44 | The mean age of all patients was 41.1 years. They were randomly divided into two equal groups (N = 22), with the IG focusing on dynamic lumbar stabilization and home exercises. CG underwent home exercises only for four weeks in total. | IG = Partook in home exercises and DLA at the 4th week post-operation and the activities continued for four weeks. CG = Was part of the home exercise program comprising stretching, pelvic tilt, extension, and flexion strengthening of the trunk and abdomen. | Functional status (ODI) at 1-month follow-up. IG = 17.5 (IQR = 15.2), CG = 23 (IQR = 11.5). Back Pain (VAS) in 1st month. IG = 10 (IQR = 20), CG = 10 (IQR = 20) | Moderate-quality evidence |
3.1. Meta-Analytical Findings
3.1.1. Back Pain Functional Status Post-Treatment
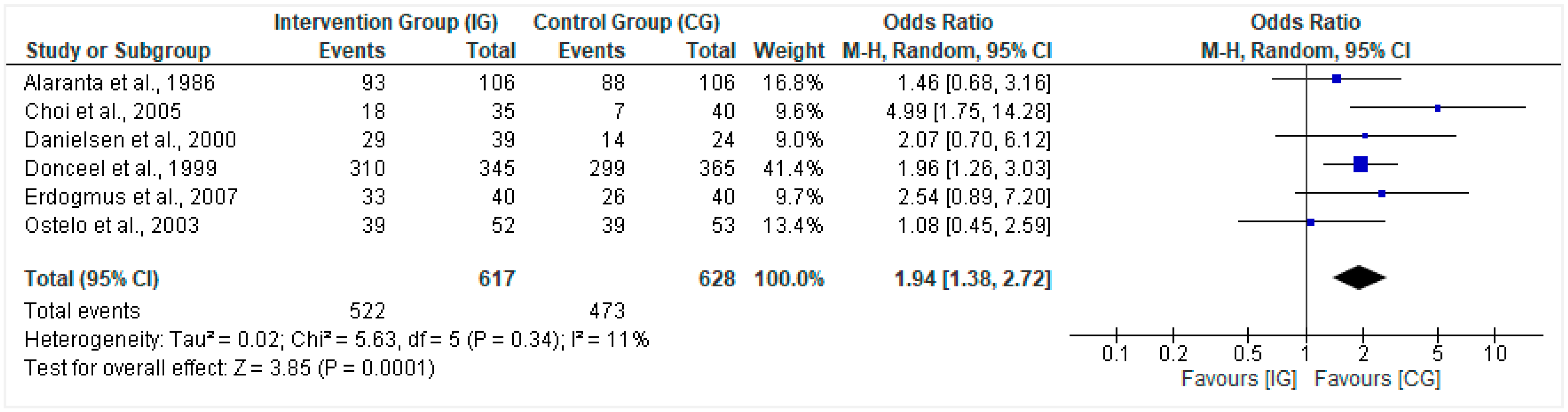
3.1.2. Global Measure of Improvement
3.1.3. Pain Scores Post-Treatment
3.2. Funnel Plot
3.3. Risk of Bias Synthesis
4. Discussion
4.1. Current Evidence and Key Underpinnings
4.2. Clinical Significance
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deyo, R.A.; Mirza, S.K. Herniated lumbar intervertebral disk. N. Engl. J. Med. 2016, 374, 1763–1772. [Google Scholar] [CrossRef] [PubMed]
- Saal, J.A.; Saal, J.S. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study. Spine 1989, 14, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Watters, W.C., III; McGirt, M.J. An evidence-based review of the literature on the consequences of conservative versus aggressive discectomy for the treatment of primary disc herniation with radiculopathy. Spine J. 2009, 9, 240–257. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; Weiner, B.K. Treatment of lumbar disc herniation: Evidence-based practice. Int. J. Gen. Med. 2010, 3, 209–214. [Google Scholar] [PubMed] [Green Version]
- Dohrmann, G.J.; Mansour, N. Long-term results of various operations for lumbar disc herniation: Analysis of over 39,000 patients. Med. Princ. Pract. 2015, 24, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Donceel, P.; Du Bois, M. Fitness for work after surgery for lumbar disc herniation: A retrospective study. Eur. Spine J. 1998, 7, 29–35. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rehabilitation. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed on 29 January 2022).
- Flynn, D.M.; McQuinn, H.; Fairchok, A.; Eaton, L.H.; Langford, D.J.; Snow, T.; Doorenbos, A.Z. Enhancing the Success of Functional Restoration Using Complementary and Integrative Therapies: Protocol and Challenges of a Comparative Effectiveness Study in Active Duty Service Members with Chronic Pain. Contemp. Clin. Trials Commun. 2019, 13, 100311. [Google Scholar] [CrossRef] [PubMed]
- Roche-Leboucher, G.; Petit-Lemanac’h, A.; Bontoux, L.; Dubus-Bausière, V.; Parot-Shinkel, E.; Fanello, S.; Penneau-Fontbonne, D.; Fouquet, N.; Legrand, E.; Roquelaure, Y. Multidisciplinary intensive functional restoration versus outpatient active physiotherapy in chronic low back pain: A randomized controlled trial. Spine 2011, 36, 2235–2242. [Google Scholar] [CrossRef] [Green Version]
- Williamson, E.; White, L.; Rushton, A. A survey of post-operative management for patients following first time lumbar discectomy. Eur. Spine J. 2007, 16, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Oosterhuis, T.; Costa, L.O.P.; Maher, C.G.; de Vet, H.C.W.; van Tulder, M.W.; Ostelo, R.W.J.G. Rehabilitation after lumbar disc surgery. Cochrane Database Syst. Rev. 2014, 3. [Google Scholar] [CrossRef]
- Ostelo, R.W.J.G.; Costa, L.O.P.; Maher, C.G.; De Vet, H.C.W.; Van Tulder, M.W. Rehabilitation after lumbar disc surgery: An update Cochrane review. Spine 2009, 34, 1839–1848. [Google Scholar] [CrossRef] [PubMed]
- Anon. GRADE in Cochrane Handbook | Cochrane Training. Available online: https://training.cochrane.org/online-learning/cochrane-methodology/grade-approach/grade-cochrane-handbook (accessed on 7 August 2022).
- Anon. RoB 2: A Revised Cochrane Risk-of-Bias Tool for Randomized Trials | Cochrane Bias. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 7 August 2022).
- Alaranta, H.; Hurme, M.; Einola, S.; Kallio, V.; Knuts, L.-R.; Törmä, T. Rehabilitation after surgery for lumbar disc herniation: Results of a randomized clinical trial. Int. J. Rehabil. Res. 1986, 9, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Donceel, P.; Du Bois, M.; Lahaye, D. Return to work after surgery for lumbar disc herniation: A rehabilitation-oriented approach in insurance medicine. Spine 1999, 24, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, J.M.; Johnsen, R.; Kibsgaard, S.K.; Hellevik, E. Early aggressive exercise for postoperative rehabilitation after discectomy. Spine 2000, 25, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Dolan, P.; Greenfield, K.; Nelson, R.J.; Nelson, I.W. Can exercise therapy improve the outcome of microdiscectomy? Spine 2000, 25, 1523–1532. [Google Scholar] [CrossRef]
- Ostelo, R.W.J.G.; De Vet, H.C.W.; Vlaeyen, J.W.S.; Kerckhoffs, M.R.; Berfelo, W.M.; Wolters, P.M.J.C.; Van den Brandt, P.A. Behavioral graded activity following first-time lumbar disc surgery: 1-year results of a randomized clinical trial. Spine 2003, 28, 1757–1765. [Google Scholar] [CrossRef]
- Yılmaz, F.; Yılmaz, A.; Merdol, F.; Parlar, D.; Sahin, F.; Kuran, B. Efficacy of dynamic lumbar stabilization exercise in lumbar microdiscectomy. J. Rehabil. Med. 2003, 35, 163–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, G.; Raiturker, P.P.; Kim, M.-J.; Chung, D.J.; Chae, Y.-S.; Lee, S.-H. The effect of early isolated lumbar extension exercise program for patients with herniated disc undergoing lumbar discectomy. Neurosurgery 2005, 57, 764–772. [Google Scholar] [CrossRef]
- Filiz, M.; Cakmak, A.; Ozcan, E. The effectiveness of exercise programmes after lumbar disc surgery: A randomized controlled study. Clin. Rehabil. 2005, 19, 4–11. [Google Scholar] [CrossRef]
- Häkkinen, A.; Ylinen, J.; Kautiainen, H.; Tarvainen, U.; Kiviranta, I. Effects of home strength training and stretching versus stretching alone after lumbar disk surgery: A randomized study with a 1-year follow-up. Arch. Phys. Med. Rehabil. 2005, 86, 865–870. [Google Scholar] [CrossRef]
- Donaldson, B.L.; Shipton, E.A.; Inglis, G.; Rivett, D.; Frampton, C. Comparison of usual surgical advice versus a nonaggravating six-month gym-based exercise rehabilitation program post–lumbar discectomy: Results at one-year follow-up. Spine J. 2006, 6, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Erdogmus, C.B.; Resch, K.-L.; Sabitzer, R.; Müller, H.; Nuhr, M.; Schöggl, A.; Posch, M.; Osterode, W.; Ungersböck, K.; Ebenbichler, G.R. Physiotherapy-based rehabilitation following disc herniation operation: Results of a randomized clinical trial. Spine 2007, 32, 2041–2049. [Google Scholar] [CrossRef] [PubMed]
- Kulig, K.; Beneck, G.J.; Selkowitz, D.M.; Popovich, J.M., Jr.; Ge, T.T.; Flanagan, S.P.; Poppert, E.M.; Yamada, K.A.; Powers, C.M.; Azen, S. An intensive, progressive exercise program reduces disability and improves functional performance in patients after single-level lumbar microdiskectomy. Phys. Ther. 2009, 89, 1145–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGregor, A.H.; Doré, C.J.; Morris, T.P.; Morris, S.; Jamrozik, K. ISSLS prize winner: Function After Spinal Treatment, Exercise, and Rehabilitation (FASTER): A factorial randomized trial to determine whether the functional outcome of spinal surgery can be improved. Spine 2011, 36, 1711–1720. [Google Scholar] [CrossRef] [PubMed]
- Oestergaard, L.G.; Nielsen, C.V.; Bünger, C.E.; Svidt, K.; Christensen, F.B. The effect of timing of rehabilitation on physical performance after lumbar spinal fusion: A randomized clinical study. Eur. Spine J. 2013, 22, 1884–1890. [Google Scholar] [CrossRef] [PubMed]
- Demir, S.; Dulgeroglu, D.; Cakci, A. Effects of dynamic lumbar stabilization exercises following lumbar microdiscectomy on pain, mobility and return to work. Randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2014, 50, 627–640. [Google Scholar]
- Madera, M.; Brady, J.; Deily, S.; McGinty, T.; Moroz, L.; Singh, D.; Tipton, G.; Truumees, E. The role of physical therapy and rehabilitation after lumbar fusion surgery for degenerative disease: A systematic review. J. Neurosurg. Spine 2017, 26, 694–704. [Google Scholar] [CrossRef] [Green Version]
- Johansson, A.-C.; Linton, S.J.; Rosenblad, A.; Bergkvist, L.; Nilsson, O. A prospective study of cognitive behavioural factors as predictors of pain, disability and quality of life one year after lumbar disc surgery. Disabil. Rehabil. 2010, 32, 521–529. [Google Scholar] [CrossRef]
- Svensson, G.L.; Lundberg, M.; Östgaard, H.C.; Wendt, G.K. High degree of kinesiophobia after lumbar disc herniation surgery: A cross-sectional study of 84 patients. Acta Orthop. 2011, 82, 732–736. [Google Scholar] [CrossRef]
- Gordon, R.; Bloxham, S. A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. Healthcare 2016, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Harden, R.N.; Oaklander, A.L.; Burton, A.W.; Perez, R.S.G.M.; Richardson, K.; Swan, M.; Barthel, J.; Costa, B.; Graciosa, J.R.; Bruehl, S. Complex regional pain syndrome: Practical diagnostic and treatment guidelines. Pain Med. 2013, 14, 180–229. [Google Scholar] [CrossRef] [PubMed]
- McGregor, A.H.; Probyn, K.; Cro, S.; Doré, C.J.; Burton, A.K.; Balagué, F.; Pincus, T.; Fairbank, J. Rehabilitation following surgery for lumbar spinal stenosis: A Cochrane review. Spine 2014, 39, 1044–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGregor, A.H.; Probyn, K.; Cro, S.; Doré, C.J.; Burton, A.K.; Balagué, F.; Pincus, T.; Fairbank, J. Rehabilitation following surgery for lumbar spinal stenosis. Cochrane Database Syst. Rev. 2013, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shipton, E.A. Physical therapy approaches in the treatment of low back pain. Pain Ther. 2018, 7, 127–137. [Google Scholar] [CrossRef] [Green Version]
- Goudman, L.; Huysmans, E.; Ickmans, K.; Nijs, J.; Moens, M.; Putman, K.; Buyl, R.; Louw, A.; Logghe, T.; Coppieters, I. A modern pain neuroscience approach in patients undergoing surgery for lumbar radiculopathy: A clinical perspective. Phys. Ther. 2019, 99, 933–945. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Stevens, S.; Hansen, D.; Demoulin, C.B.O.E.; Eijnde, B.O.; Vandenabeele, F.; Timmermans, A. Exercise intensity matters in chronic nonspecific low back pain rehabilitation. Med. Sci. Sports Exerc. 2019, 51, 2434–2442. [Google Scholar] [CrossRef]
- Semrau, J.; Hentschke, C.; Peters, S.; Pfeifer, K. Effects of behavioural exercise therapy on the effectiveness of multidisciplinary rehabilitation for chronic non-specific low back pain: A randomised controlled trial. BMC Musculoskelet. Disord. 2021, 22, 500. [Google Scholar] [CrossRef]
- Leung, G.C.N.; Cheung, P.W.H.; Lau, G.; Lau, S.T.; Luk, K.D.K.; Wong, Y.W.; Cheung, K.M.C.; Koljonen, P.A.; Cheung, J.P.Y. Multidisciplinary programme for rehabilitation of chronic low back pain–factors predicting successful return to work. BMC Musculoskelet. Disord. 2021, 22, 251. [Google Scholar] [CrossRef]






| Participants | Intervention | Comparator | Outcomes |
|---|---|---|---|
| Adult patients aged 18–65 that were undergoing first-time lumbar disc surgery due to prolapse of the lumbar disc were included. Any type of surgical technique, whether standard discectomy, laser discectomy, microdiscectomy, or chemonucleolysis, was included. Studies that pertained to non-first-time post-surgical patients or those aged < 18 years or > 65 years were excluded. | Post lumbar disc surgery active rehabilitation programs include strength and mobility training, exercise therapy, physiotherapy, and multidisciplinary treatment. These programs may be conducted one-to-one or in a group-based setting. Individuals who do not undergo active enlisted programs and do not acquire physiotherapeutic measures are excluded. | The active physiotherapeutic rehabilitation was compared to a control group that did not acquire active rehabilitative treatment. | The randomized controlled trials were required to pertain to at least one of the four primary outcome measures, including: 1. Pain (i.e., visual analog scale), 2. A global measure of improvement (i.e., overall improvement of health, proportion of sample size showing recovery, subjective test to quantify improvement), 3. Back pain functional status (i.e., Oswestry Disability Index, Roland Morris Disability Questionnaire), and 4. Return to work (i.e., days off work, return to work status). The secondary outcomes of the physical examination pertained to the spinal range of motion, muscle strength, and straight-leg raise range of motion; the behavioral outcomes include anxiety, depression, and pain behavior. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afzal, K.; Khattak, H.G.; Sajjad, A.G.; Hussain, S.A.; Sarfraz, Z.; Sarfraz, A.; Cherrez-Ojeda, I. Impact of Active Physiotherapy Rehabilitation on Pain and Global and Functional Improvement 1–2 Months after Lumbar Disk Surgery: A Systematic Review and Meta-Analysis. Healthcare 2022, 10, 1943. https://doi.org/10.3390/healthcare10101943
Afzal K, Khattak HG, Sajjad AG, Hussain SA, Sarfraz Z, Sarfraz A, Cherrez-Ojeda I. Impact of Active Physiotherapy Rehabilitation on Pain and Global and Functional Improvement 1–2 Months after Lumbar Disk Surgery: A Systematic Review and Meta-Analysis. Healthcare. 2022; 10(10):1943. https://doi.org/10.3390/healthcare10101943
Chicago/Turabian StyleAfzal, Kiran, Hafsah Gul Khattak, Abdul Ghafoor Sajjad, Syed Ali Hussain, Zouina Sarfraz, Azza Sarfraz, and Ivan Cherrez-Ojeda. 2022. "Impact of Active Physiotherapy Rehabilitation on Pain and Global and Functional Improvement 1–2 Months after Lumbar Disk Surgery: A Systematic Review and Meta-Analysis" Healthcare 10, no. 10: 1943. https://doi.org/10.3390/healthcare10101943