
Gait Characteristics of Dynapenia, Sarcopenia, and Presarcopenia in Community-Dwelling Japanese Older Women: A Cross-Sectional Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
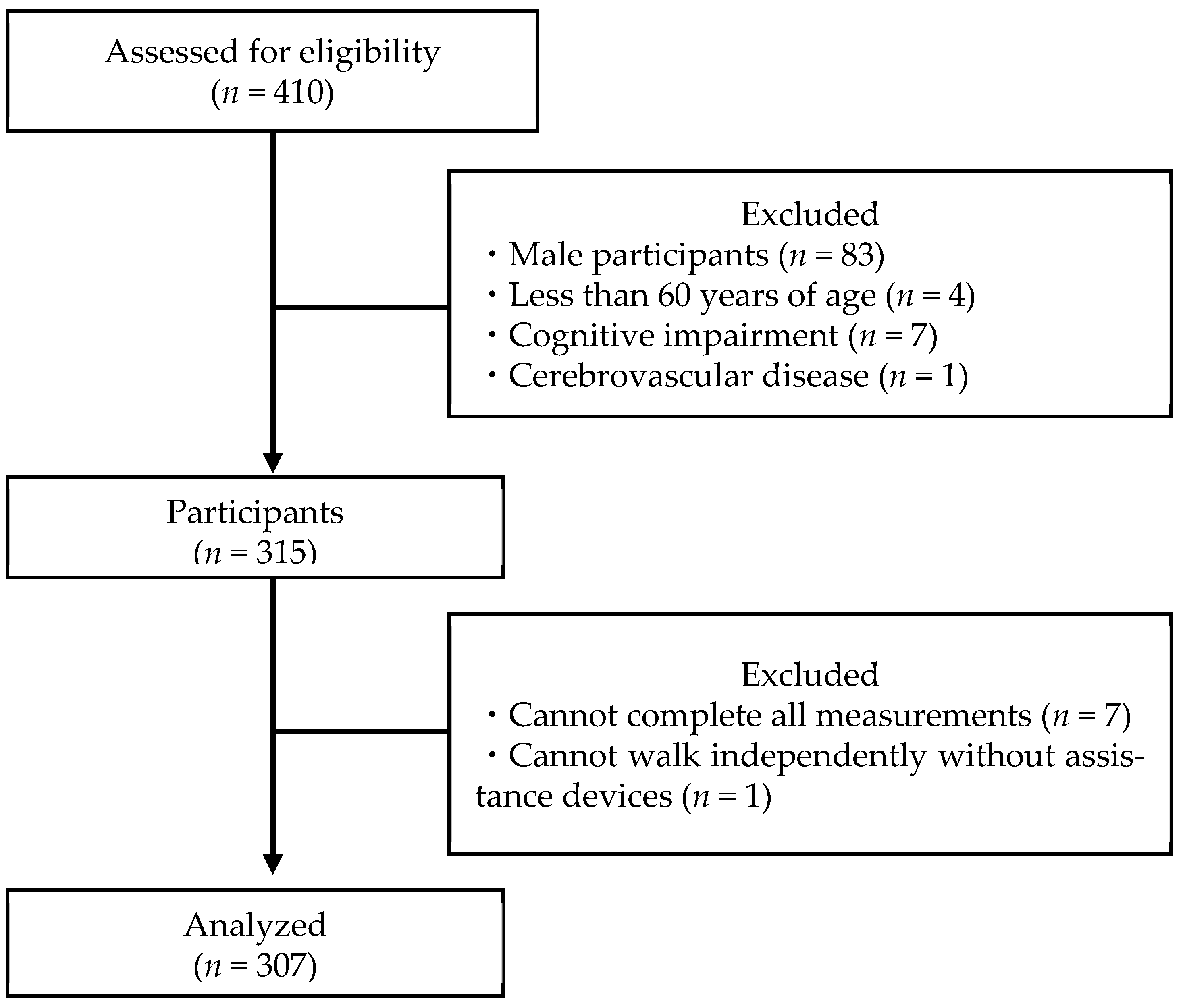
2.1. Participants
2.2. Measurements
2.2.1. Skeletal Muscle Mass
2.2.2. Muscle Strength
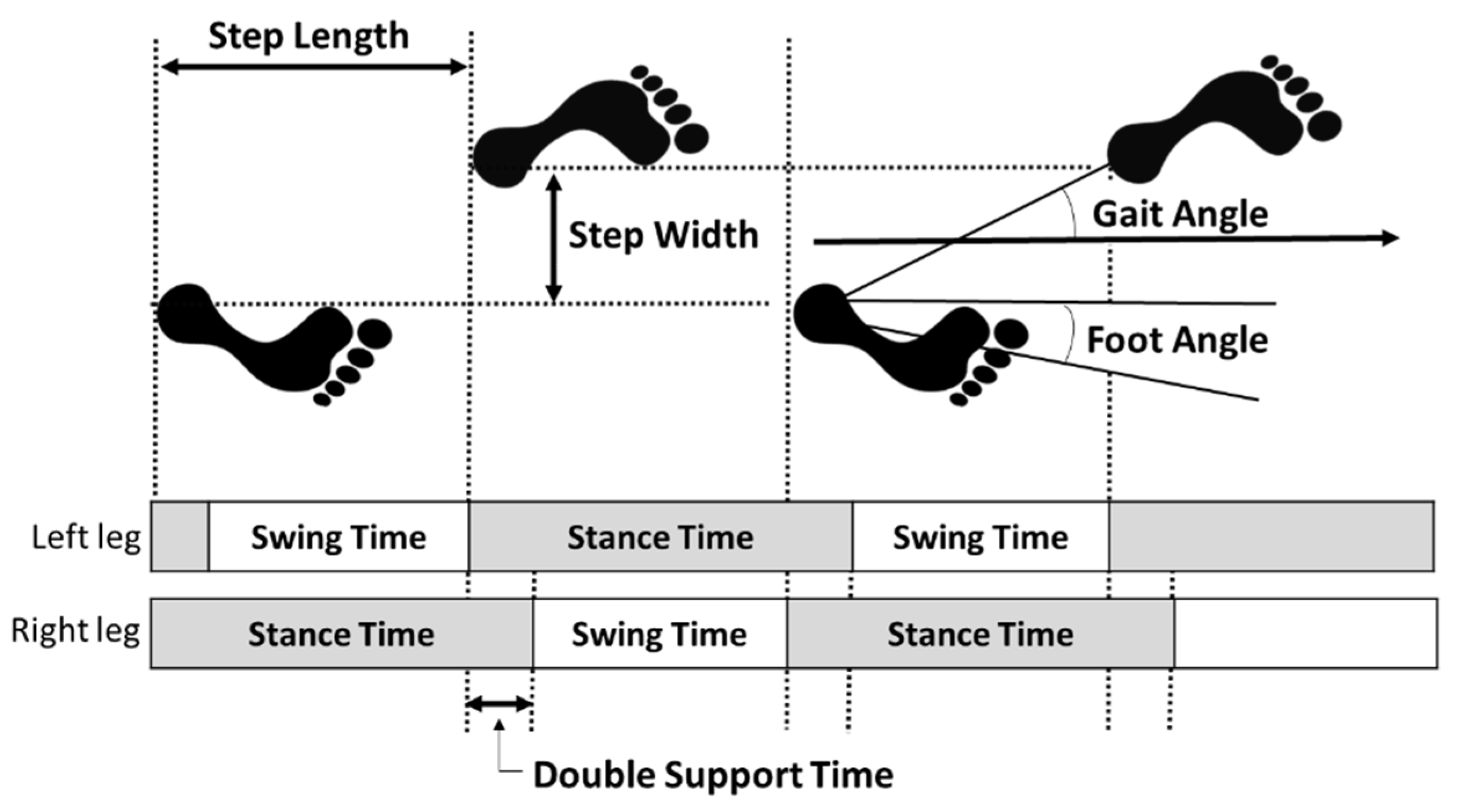
2.2.3. Gait Parameters
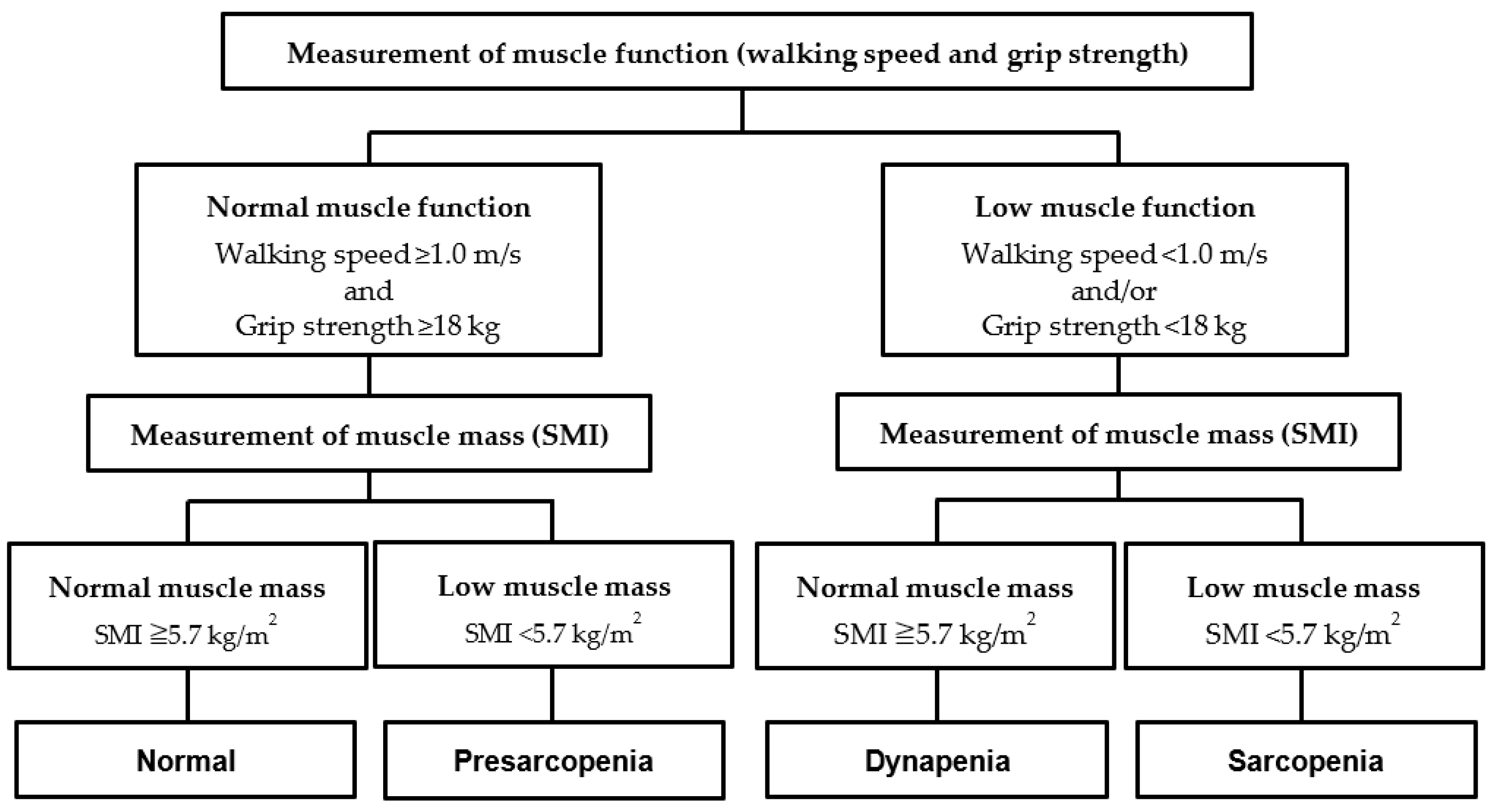
2.3. Assessing Presarcopenia, Dynapenia, and Sarcopenia
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perez-Sousa, M.A.; Venegas-Sanabria, L.C.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Izquierdo, M.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Gait speed as a mediator of the effect of sarcopenia on dependency in activities of daily living. J. Cachexia Sarcopenia Muscle 2019, 10, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, J.; Hughes, S.; Dunlop, D.; Chang, R.W. Predictors of change in walking velocity in older adults. J. Am. Geriatr. Soc. 1996, 44, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef]
- Jung, H.W.; Jang, I.Y.; Lee, C.K.; Yu, S.S.; Hwang, J.K.; Jeon, C.; Lee, Y.S.; Lee, E. Usual gait speed is associated with frailty status, institutionalization, and mortality in community-dwelling rural older adults: A longitudinal analysis of the Aging Study of Pyeongchang Rural Area. Clin. Interv. Aging 2018, 13, 1079–1089. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Lee, S.C.; Harada, K.; Hotta, R.; Nakakubo, S.; Bae, S.; et al. Age-dependent changes in physical performance and body composition in community-dwelling Japanese older adults. J. Cachexia Sarcopenia Muscle 2017, 8, 607–614. [Google Scholar] [CrossRef]
- Mahlknecht, P.; Kiechl, S.; Bloem, B.R.; Willeit, J.; Scherfler, C.; Gasperi, A.; Rungger, G.; Poewe, W.; Seppi, K. Prevalence and burden of gait disorders in elderly men and women aged 60-97 years: A population-based study. PLoS ONE 2013, 8, e69627. [Google Scholar] [CrossRef]
- Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.; Newman, A.B.; Nevitt, M.; Rubin, S.M.; Simonsick, E.M.; Harris, T.B. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 324–333. [Google Scholar] [CrossRef]
- Rosemberg, I.H. Epidemiologic and methodologic problems in determining nutritional status of older persons. Am. J. Clin. Nutr. 1989, 50, 1121–1235. [Google Scholar]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Directors Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M. Sarcopenia =/= dynapenia. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, Y.; Watanabe, M.; Sun, W.; Sugiura, Y.; Hayashida, I.; Kusabiraki, T.; Tamaki, J. Sarcopenia and falls in community-dwelling elderly subjects in Japan: Defining sarcopenia according to criteria of the European Working Group on Sarcopenia in Older People. Arch. Gerontol. Geriatr. 2014, 59, 295–299. [Google Scholar] [CrossRef]
- Kao, T.W.; Peng, T.C.; Chen, W.L.; Han, D.S.; Chen, C.L.; Yang, W.S. Impact of adiposity on muscle function and clinical events among elders with dynapenia, presarcopenia and sarcopenia: A community-based cross-sectional study. Aging 2021, 13, 7247–7258. [Google Scholar] [CrossRef]
- Dos Santos, L.; Cyrino, E.S.; Antunes, M.; Santos, D.A.; Sardinha, L.B. Sarcopenia and physical independence in older adults: The independent and synergic role of muscle mass and muscle function. J. Cachexia Sarcopenia Muscle 2017, 8, 245–250. [Google Scholar] [CrossRef]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; et al. Sarcopenia: Prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30–38. [Google Scholar] [CrossRef]
- Alexandre, T.d.S.; Duarte, Y.A.; Santos, J.L.; Wong, R.; Lebrão, M.L. Sarcopenia according to the European Working Group on Sarcopenia in Older People (EWGSOP) versus dynapenia as a risk factor for mortality in the elderly. J. Nutr. Health Aging 2014, 18, 751–756. [Google Scholar] [CrossRef]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative spatiotemporal gait parameters in older adults. Gait. Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Bassey, E.J.; Fiatarone, M.A.; O’Neill, E.F.; Kelly, M.; Evans, W.J.; Lipsitz, L.A. Leg extensor power and functional performance in very old men and women. Clin. Sci. 1992, 82, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; Di Iorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851–1860. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, I.; Tanimoto, Y.; Takahashi, Y.; Kusabiraki, T.; Tamaki, J. Correlation between muscle strength and muscle mass, and their association with walking speed, in community-dwelling elderly Japanese individuals. PLoS ONE 2014, 9, e111810. [Google Scholar] [CrossRef] [PubMed]
- Dufour, A.B.; Hannan, M.T.; Murabito, J.M.; Kiel, D.P.; McLean, R.R. Sarcopenia definitions considering body size and fat mass are associated with mobility limitations: The Framingham Study. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 168–174. [Google Scholar] [CrossRef]
- Doi, T.; Nakakubo, S.; Tsutsumimoto, K.; Kim, M.J.; Kurita, S.; Ishii, H.; Shimada, H. Spatio-temporal gait variables predicted incident disability. J. Neuroeng. Rehabil. 2020, 17, 11. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Sugishita, M.; Hemmi, I.; Takeuchi, T. Reexamination of the validity and reliability of the Japanese version of the Mini-Mental State Examination (MMSE-J). Jpn. J. Cogn. Neurosci. 2016, 18, 4. [Google Scholar]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef]
- Nonaka, K.; Murata, S.; Shiraiwa, K.; Abiko, T.; Nakano, H.; Iwase, H.; Naito, K.; Horie, J. Physical Characteristics Vary According to Body Mass Index in Japanese Community-Dwelling Elderly Women. Geriatrics 2018, 3, 87. [Google Scholar] [CrossRef]
- Abe, T.; Yaginuma, Y.; Fujita, E.; Thiebaud, R.S.; Kawanishi, M.; Akamine, T. Associations of sit-up ability with sarcopenia classification measures in Japanese older women. Interv. Med. Appl. Sci. 2016, 8, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Ishii, K.; Makizako, H.; Ishiwata, K.; Oda, K.; Suzukawa, M. Effects of exercise on brain activity during walking in older adults: A randomized controlled trial. J. Neuroeng. Rehabil. 2017, 14, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makino, K.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Hotta, R.; Nakakubo, S.; Suzuki, T.; Shimada, H. Fear of falling and gait parameters in older adults with and without fall history. Geriatr. Gerontol. Int. 2017, 17, 2455–2459. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Nishio, N.; Abe, Y.; Kakehi, T.; Fujimoto, J.; Tanaka, T.; Ohji, S.; Otobe, Y.; et al. Differential characteristics of skeletal muscle in community-dwelling older adults. J. Am. Med. Dir. Assoc. 2017, 18, 807.e9–807.e16. [Google Scholar] [CrossRef]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef]
- Doi, T.; Nakakubo, S.; Tsutsumimoto, K.; Kurita, S.; Ishii, H.; Shimada, H. Spatiotemporal gait characteristics and risk of mortality in community-dwelling older adults. Maturitas 2021, 151, 31–35. [Google Scholar] [CrossRef]
- Mortaza, N.; Abu Osman, N.A.; Mehdikhani, N. Are the spatio-temporal parameters of gait capable of distinguishing a faller from a non-faller elderly? Eur. J. Phys. Rehabil. Med. 2014, 50, 677–691. [Google Scholar]
- Schaap, L.A.; Koster, A.; Visser, M. Adiposity, muscle mass, and muscle strength in relation to functional decline in older persons. Epidemiol. Rev. 2013, 35, 51–65. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Normal (n = 187) | Presarcopenia (n = 79) | Sarcopenia (n = 25) | Dynapenia (n = 16) | ANOVA | ||
|---|---|---|---|---|---|---|
| Characteristic | F Value | p Value | ||||
| Age (y) | 73.0 ± 5.4 | 73.5 ± 5.6 | 77.8 ± 6.7 N,P | 75.8 ± 7.1 | 6.0 | <0.001 |
| Height (cm) | 152.3 ± 5.0 | 151.3 ± 5.1 | 146.0 ± 4.8 N,P | 149.3 ± 7.0 | 12.0 | <0.001 |
| Weight (kg) | 53.6 ± 7.0 | 45.4 ± 5.4 N,D | 44.5 ± 4.6 N,D | 51.0 ± 4.8 | 39.7 | <0.001 |
| BMI (kg/m2) | 23.1 ± 2.9 | 19.8 ± 2.3 N,D | 20.9 ± 2.4 N | 22.9 ± 1.7 | 30.1 | <0.001 |
| SMI (kg/m2) | 6.42 ± 0.58 | 5.34 ± 0.29 N,D | 5.19 ± 0.45 N,D | 6.04 ± 0.22 N | 111.8 | <0.001 |
| Grip strength (kg) | 25.2 ± 3.4 | 22.7 ± 2.6 N | 17.3 ± 3.5 N,P | 19.0 ± 3.7 N,P | 58.7 | <0.001 |
| Walking speed (m/s) | 1.34 ± 0.21 | 1.35 ± 0.20 | 1.19 ± 0.23 N,P | 1.01 ± 0.22 N,P,S | 16.1 | <0.001 |
| Normal (n = 187) | Presarcopenia (n = 79) | Sarcopenia (n = 25) | Dynapenia (n = 16) | ANCOVA | ||
|---|---|---|---|---|---|---|
| F Value | p Value | |||||
| Walking speed (m/s) | 1.34 ± 0.21 | 1.35 ± 0.20 | 1.19 ± 0.23 N | 1.01 ± 0.22 N,P,S | 13.53 | <0.001 |
| Cadence (steps/min) | 129.05 ± 11.55 | 129.84 ± 9.88 | 127.73 ± 11.42 | 120.34 ± 10.64 N,P | 3.16 | 0.025 |
| Step length (cm) | 62.35 ± 7.74 | 62.37 ± 7.51 | 56.17 ± 9.19 N | 50.15 ± 9.22 N,P | 13.55 | <0.001 |
| Step width (cm) | 7.53 ± 2.79 | 6.84 ± 2.69 | 7.04 ± 2.87 | 9.66 ± 2.84 N,P,S | 3.38 | 0.019 |
| Gait angle (°) | 7.04 ± 2.74 | 6.38 ± 2.68 | 7.49 ± 3.71 | 11.31 ± 3.86 N,P,S | 10.91 | <0.001 |
| Foot angle (°) | 2.53 ± 4.46 | 2.72 ± 5.19 | 2.27 ± 5.52 | 1.74 ± 5.14 | 0.29 | 0.832 |
| Stance time (s) | 0.60 ± 0.07 | 0.59 ± 0.07 | 0.63 ± 0.08 | 0.65 ± 0.10 N | 3.39 | 0.018 |
| Swing time (s) | 0.33 ± 0.07 | 0.33 ± 0.06 | 0.32 ± 0.06 | 0.34 ± 0.07 | 0.37 | 0.777 |
| Double stance time (s) | 0.13 ± 0.05 | 0.12 ± 0.05 | 0.15 ± 0.06 | 0.15 ± 0.06 | 1.81 | 0.145 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, K.; Murata, S.; Goda, A.; Kikuchi, Y.; Shiraiwa, K.; Horie, J.; Nakano, H. Gait Characteristics of Dynapenia, Sarcopenia, and Presarcopenia in Community-Dwelling Japanese Older Women: A Cross-Sectional Study. Healthcare 2022, 10, 1905. https://doi.org/10.3390/healthcare10101905
Mori K, Murata S, Goda A, Kikuchi Y, Shiraiwa K, Horie J, Nakano H. Gait Characteristics of Dynapenia, Sarcopenia, and Presarcopenia in Community-Dwelling Japanese Older Women: A Cross-Sectional Study. Healthcare. 2022; 10(10):1905. https://doi.org/10.3390/healthcare10101905
Chicago/Turabian StyleMori, Kohei, Shin Murata, Akio Goda, Yuki Kikuchi, Kayoko Shiraiwa, Jun Horie, and Hideki Nakano. 2022. "Gait Characteristics of Dynapenia, Sarcopenia, and Presarcopenia in Community-Dwelling Japanese Older Women: A Cross-Sectional Study" Healthcare 10, no. 10: 1905. https://doi.org/10.3390/healthcare10101905