
The Optimal Cut-Off Point for Thai Diagnostic Autism Scale and Probability Prediction of Autism Spectrum Disorder Diagnosis in Suspected Children
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Settings
2.2. Assessment
2.3. Statistical Analysis
2.4. Ethical Approval and Consent for Participation
3. Results
3.1. The Characteristics of the Participants
3.2. The Optimal Cut-Off Point for TDAS According to the DSM-5 ASD Criteria
3.3. ASD Diagnosis Comparison between ADOS-2, TDAS, and TDAS ≥20 Points
3.4. The Predictive Model for the Probability of ASD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huerta, M.; Bishop, S.L.; Duncan, A.; Hus, V.; Lord, C. Application of DSM-5 criteria for autism spectrum disorder to three samples of children with DSM-IV diagnoses of pervasive developmental disorders. Am. J. Psychiatry 2012, 169, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global prevalence of autism: A systematic review update. Autism Res. 2022, 15, 778–790. [Google Scholar] [CrossRef] [PubMed]
- Hansakunachai, T.; Roongpraiwan, R.; Sombuntham, T.; Limprasert, P.; Ruangdaraganon, N. A new structured interview for children with autism spectrum disorder based on the DSM-IV. J. Med. Assoc. Thai. 2014, 97 (Suppl. 8), S7–S14. [Google Scholar] [PubMed]
- Plubrukarn, R.; Piyasil, V.; Moungnoi, P.; Tanprasert, S.; Chutchawalitsakul, V. Trend study of autistic spectrum disorders at Queen Sirikit National Institute of Child Health. J. Med. Assoc. Thai. 2005, 88, 891–897. [Google Scholar]
- Asia-Pacific Development Center on Disability. Autism at a Glance in ASEAN Under the Autism Mapping Project in the ASEAN Region: Part II Country Profiles; Asia-Pacific Development Center on Disability Foundation: Bangkok, Thailand, 2020; p. 428. [Google Scholar]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Lord, C.R.M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Schopler, E.; Reichler, R.; Renner, B. The Childhood Autism Rating Scale (CARS); Western Psychological Services: Los Angeles, CA, USA, 1988. [Google Scholar]
- Kaat, A.; Lecavalier, L. Childhood Autism Rating Scale. In Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer: New York, NY, USA, 2013; pp. 590–593. [Google Scholar]
- Randall, M.; Egberts, K.J.; Samtani, A.; Scholten, R.J.; Hooft, L.; Livingstone, N.; Sterling-Levis, K.; Woolfenden, S.; Williams, K. Diagnostic tests for autism spectrum disorder (ASD) in preschool children. Cochrane Database Syst. Rev. 2018, 7, Cd009044. [Google Scholar] [CrossRef]
- Carr, T. Autism Diagnostic Observation Schedule. In Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer: New York, NY, USA, 2013; pp. 349–356. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Pornnoppadol, C.; Thongngen, A.; Gaevalin, A.; Sangratanayont, D. Development of the Pervasive Developmental Disorders Screening Questionnaires. J. Psychiatr. Assoc. Thail. 2002, 47, 75–96. [Google Scholar]
- Panyayong, B. The validation of the pervasive developmental. J. Ment. Health Thail. 2012, 18, 36–44. [Google Scholar] [CrossRef]
- Bernier, R.; Mao, A.; Yen, J. Psychopathology, families, and culture: Autism. Child Adolesc. Psychiatr. Clin. N. Am. 2010, 19, 855–867. [Google Scholar] [CrossRef]
- Sirithongthaworn, S. The development of developmental surveillance and promotion manual; DSPM. J. Psychiatr. Assoc. Thail. 2018, 63, 3–12. [Google Scholar]
- Tangviriyapaiboon, D.; Sirithongthaworn, S.; Apikomonkon, H.; Suyakong, C.; Srikummoon, P.; Kawilapat, S.; Traisathit, P. Development and psychometric evaluation of a Thai Diagnostic Autism Scale for the early diagnosis of Autism Spectrum Disorder. Autism Res. 2021, 15, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Buderer, N.M. Statistical methodology: I. Incorporating the prevalence of disease into the sample size calculation for sensitivity and specificity. Acad. Emerg. Med. 1996, 3, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Liu, X. Classification accuracy and cut point selection. Stat. Med. 2012, 31, 2676–2686. [Google Scholar] [CrossRef]
- Cleves, M.A. From the Help Desk: Comparing Areas under Receiver Operating Characteristic Curves from Two or more Probit or Logit Models. Stata J. 2002, 2, 301–313. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Parikh, R.; Mathai, A.; Parikh, S.; Chandra Sekhar, G.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian J. Ophthalmol. 2008, 56, 45–50. [Google Scholar] [CrossRef]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef]
- Cicchetti, D.V.; Sparrow, S.A. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am. J. Ment. Defic. 1981, 86, 127–137. [Google Scholar]
- Nagelkerke, N.J.D. A note on a general definition of the coefficient of determination. Biometrika 1991, 78, 691–692. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.S.; Singh, V.; Kalb, L.; Ashkar, A.; Landa, R. Replication study of ADOS-2 Toddler Module cut-off scores for autism spectrum disorder classification. Autism Res. 2021, 14, 1284–1295. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.H.; Xie, X.F.; Dai, J.J.; Yu, Y.; Zhang, Y.; Cheng, Q. Value of autism screening checklists in the early identification of autism spectrum disorder. Zhongguo Dang Dai Er Ke Za Zhi (Chin. J. Contemp. Pediatr.) 2021, 23, 343–349. [Google Scholar] [CrossRef]
- King, M.D.; Fountain, C.; Dakhlallah, D.; Bearman, P.S. Estimated autism risk and older reproductive age. Am. J. Public Health 2009, 99, 1673–1679. [Google Scholar] [CrossRef]
- Lyall, K.; Song, L.; Botteron, K.; Croen, L.A.; Dager, S.R.; Fallin, M.D.; Hazlett, H.C.; Kauffman, E.; Landa, R.; Ladd-Acosta, C.; et al. The Association Between Parental Age and Autism-Related Outcomes in Children at High Familial Risk for Autism. Autism Res. 2020, 13, 998–1010. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic (n (%) or Median (IQR)) | All | DSM-5 | ||
|---|---|---|---|---|
| Non-ASD (n = 51) | ASD (n =105) | p-Value a | ||
| Gender (n = 155) | 0.005 | |||
| Boys | 124 (80.0%) | 34 (66.7%) | 90 (86.5%) | |
| Girls | 21 (20.0%) | 17 (33.3%) | 14 (13.5%) | |
| Age (months) (n = 152) | 34 (27–41) | 28 (24–40) | 36 (31–41) | 0.001 |
| ADOS-2 score | 20 (14–25) | 14 (10–20) | 22 (18–25) | <0.001 |
| TDAS score | 25 (16–32) | 14 (9–19) | 30 (22–26) | <0.001 |
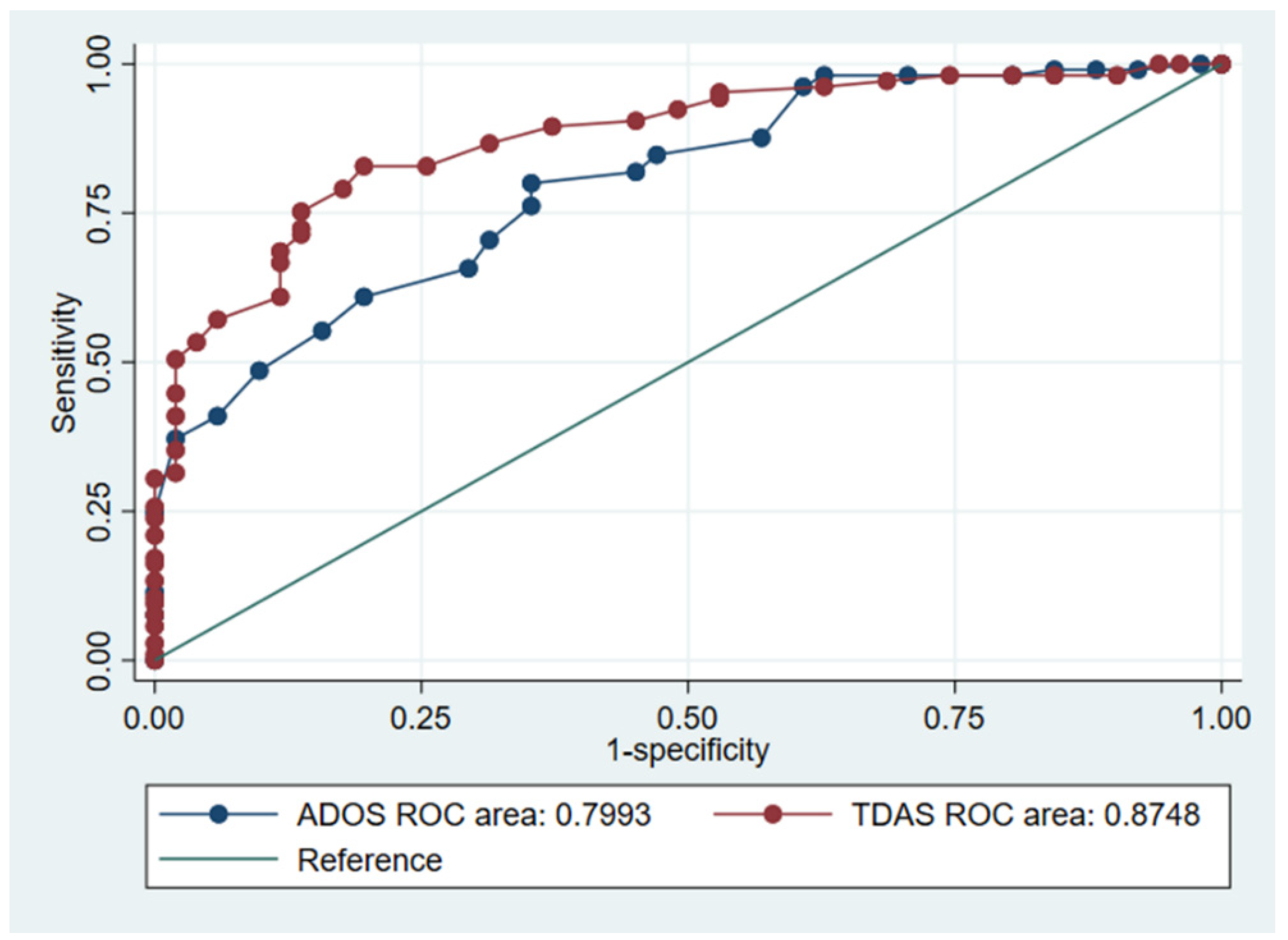
| Tools | ROC AUC | SE | 95% CI | p-Value a |
|---|---|---|---|---|
| ADOS-2 (gold standard) b | 0.7993 | 0.0359 | (0.7289–0.8698) | |
| TDAS b | 0.8748 | 0.0283 | (0.8193–0.9303) | 0.033 |
| Cut-Off Point | Sensitivity | Specificity | Accuracy |
|---|---|---|---|
| ≥2 | 100.00% | 0.00% | 67.31% |
| ≥4 | 100.00% | 3.92% | 68.59% |
| ≥6 | 100.00% | 5.88% | 69.23% |
| ≥7 | 98.10% | 9.80% | 69.23% |
| ≥8 | 98.10% | 15.69% | 71.15% |
| ≥9 | 98.10% | 19.61% | 72.44% |
| ≥10 | 98.10% | 25.49% | 74.36% |
| ≥11 | 97.14% | 31.37% | 75.64% |
| ≥12 | 96.19% | 37.25% | 76.92% |
| ≥13 | 95.24% | 47.06% | 79.49% |
| ≥14 | 94.29% | 47.06% | 78.85% |
| ≥15 | 92.38% | 50.98% | 78.85% |
| ≥16 | 90.48% | 54.90% | 78.85% |
| ≥17 | 89.52% | 62.75% | 80.77% |
| ≥18 | 86.67% | 68.63% | 80.77% |
| ≥19 | 82.86% | 74.51% | 80.13% |
| ≥20 | 82.86% | 80.39% | 82.05% |
| ≥21 | 79.05% | 82.35% | 80.13% |
| ≥22 | 75.24% | 86.27% | 78.85% |
| ≥23 | 72.38% | 86.27% | 76.92% |
| ≥24 | 71.43% | 86.27% | 76.28% |
| ≥25 | 68.57% | 88.24% | 75.00% |
| ≥26 | 66.67% | 88.24% | 73.72% |
| ≥27 | 60.95% | 88.24% | 69.87% |
| ≥28 | 57.14% | 94.12% | 69.23% |
| ≥29 | 53.33% | 96.08% | 67.31% |
| ≥30 | 50.48% | 98.04% | 66.03% |
| ≥31 | 44.76% | 98.04% | 62.18% |
| ≥32 | 40.95% | 98.04% | 59.62% |
| ≥33 | 35.24% | 98.04% | 55.77% |
| ≥34 | 31.43% | 98.04% | 53.21% |
| ≥35 | 30.48% | 100.00% | 53.21% |
| ≥36 | 25.71% | 100.00% | 50.00% |
| ≥37 | 23.81% | 100.00% | 48.72% |
| ≥38 | 20.95% | 100.00% | 46.79% |
| ≥39 | 17.14% | 100.00% | 44.23% |
| ≥40 | 16.19% | 100.00% | 43.59% |
| ≥41 | 13.33% | 100.00% | 41.67% |
| ≥42 | 10.48% | 100.00% | 39.74% |
| ≥43 | 9.52% | 100.00% | 39.10% |
| ≥44 | 7.62% | 100.00% | 37.82% |
| ≥45 | 5.71% | 100.00% | 36.54% |
| ≥46 | 2.86% | 100.00% | 34.62% |
| ≥48 | 0.95% | 100.00% | 33.33% |
| >48 | 0.00% | 100.00% | 32.69% |
| Criteria | DSM-5 | |||
|---|---|---|---|---|
| Non-ASD (n = 51) | ASD (n = 105) | Agreement | p-Value a | |
| ADOS-2 | 113 (72.44%) | <0.001 | ||
| Non-ASD | 9 (17.65%) | 1 (0.95%) | ||
| ASD | 42 (82.35%) | 104 (99.05%) | ||
| TDAS b | 118 (75.64%) | <0.001 | ||
| Non-ASD | 22 (43.14%) | 9 (8.57%) | ||
| ASD | 29 (56.86%) | 96 (91.43%) | ||
| TDAS ≥ 20 points | 128 (82.05%) | <0.001 | ||
| Non-ASD | 41 (80.39%) | 18 (17.14%) | ||
| ASD | 10 (19.61%) | 87 (82.86%) | ||
| Variables | Coefficient (95% CI) | p-Value a | Nagelkerke r2 |
|---|---|---|---|
| Constant | −5.341 (−7.678, −3.003) | <0.001 | 0.529 |
| TDAS score | 0.179 (0.119, 0.240) | <0.001 | |
| Age (months) | 0.068 (0.014, 0.122) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tangviriyapaiboon, D.; Kawilapat, S.; Sirithongthaworn, S.; Apikomonkon, H.; Suyakong, C.; Srikummoon, P.; Thumronglaohapun, S.; Traisathit, P. The Optimal Cut-Off Point for Thai Diagnostic Autism Scale and Probability Prediction of Autism Spectrum Disorder Diagnosis in Suspected Children. Healthcare 2022, 10, 1868. https://doi.org/10.3390/healthcare10101868
Tangviriyapaiboon D, Kawilapat S, Sirithongthaworn S, Apikomonkon H, Suyakong C, Srikummoon P, Thumronglaohapun S, Traisathit P. The Optimal Cut-Off Point for Thai Diagnostic Autism Scale and Probability Prediction of Autism Spectrum Disorder Diagnosis in Suspected Children. Healthcare. 2022; 10(10):1868. https://doi.org/10.3390/healthcare10101868
Chicago/Turabian StyleTangviriyapaiboon, Duangkamol, Suttipong Kawilapat, Samai Sirithongthaworn, Hataichanok Apikomonkon, Chidawan Suyakong, Pimwarat Srikummoon, Salinee Thumronglaohapun, and Patrinee Traisathit. 2022. "The Optimal Cut-Off Point for Thai Diagnostic Autism Scale and Probability Prediction of Autism Spectrum Disorder Diagnosis in Suspected Children" Healthcare 10, no. 10: 1868. https://doi.org/10.3390/healthcare10101868