
A Predictable Approach of a Rare and Frequently Misdiagnosed Entity: Laryngeal Nerve Schwannoma



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
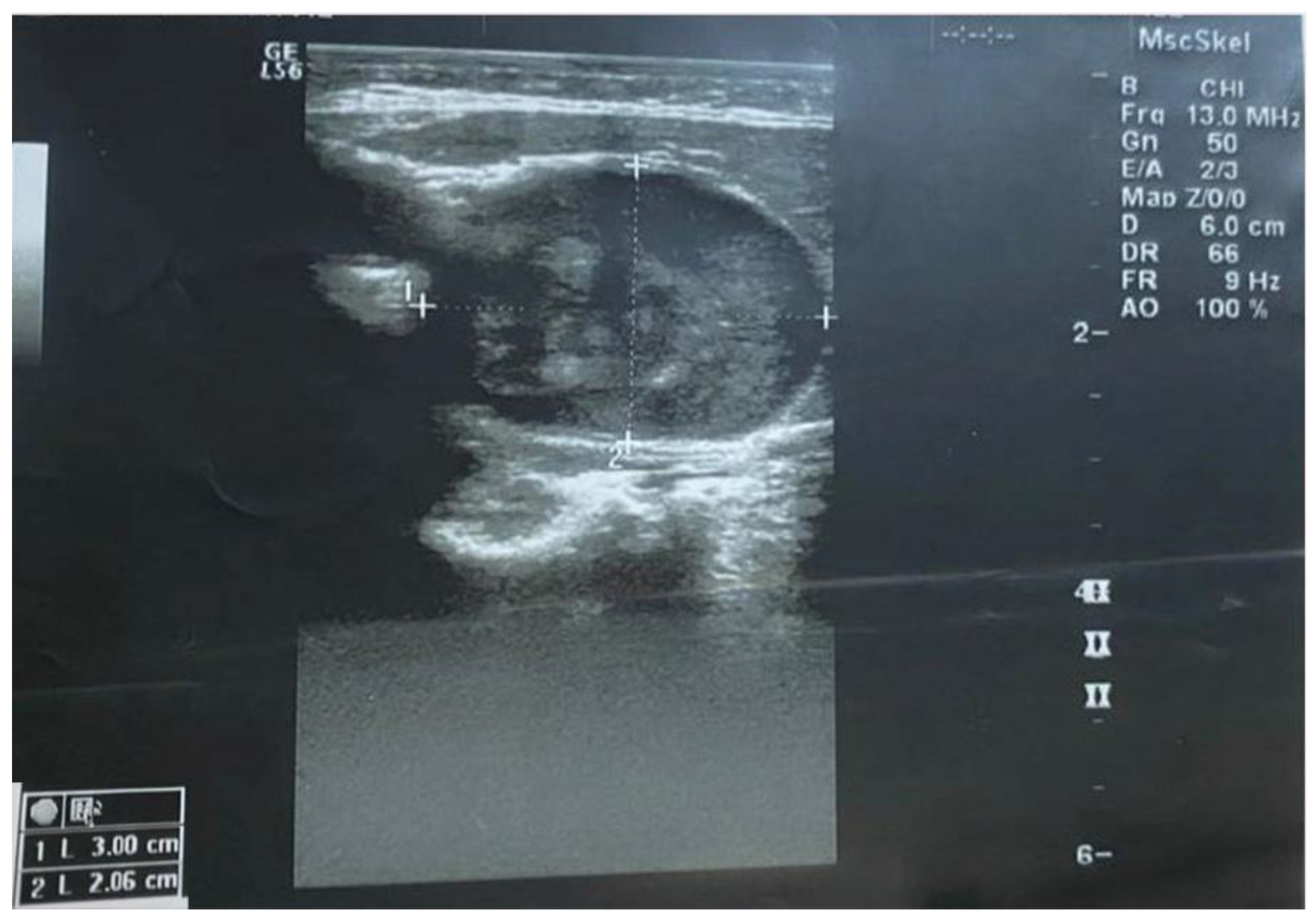
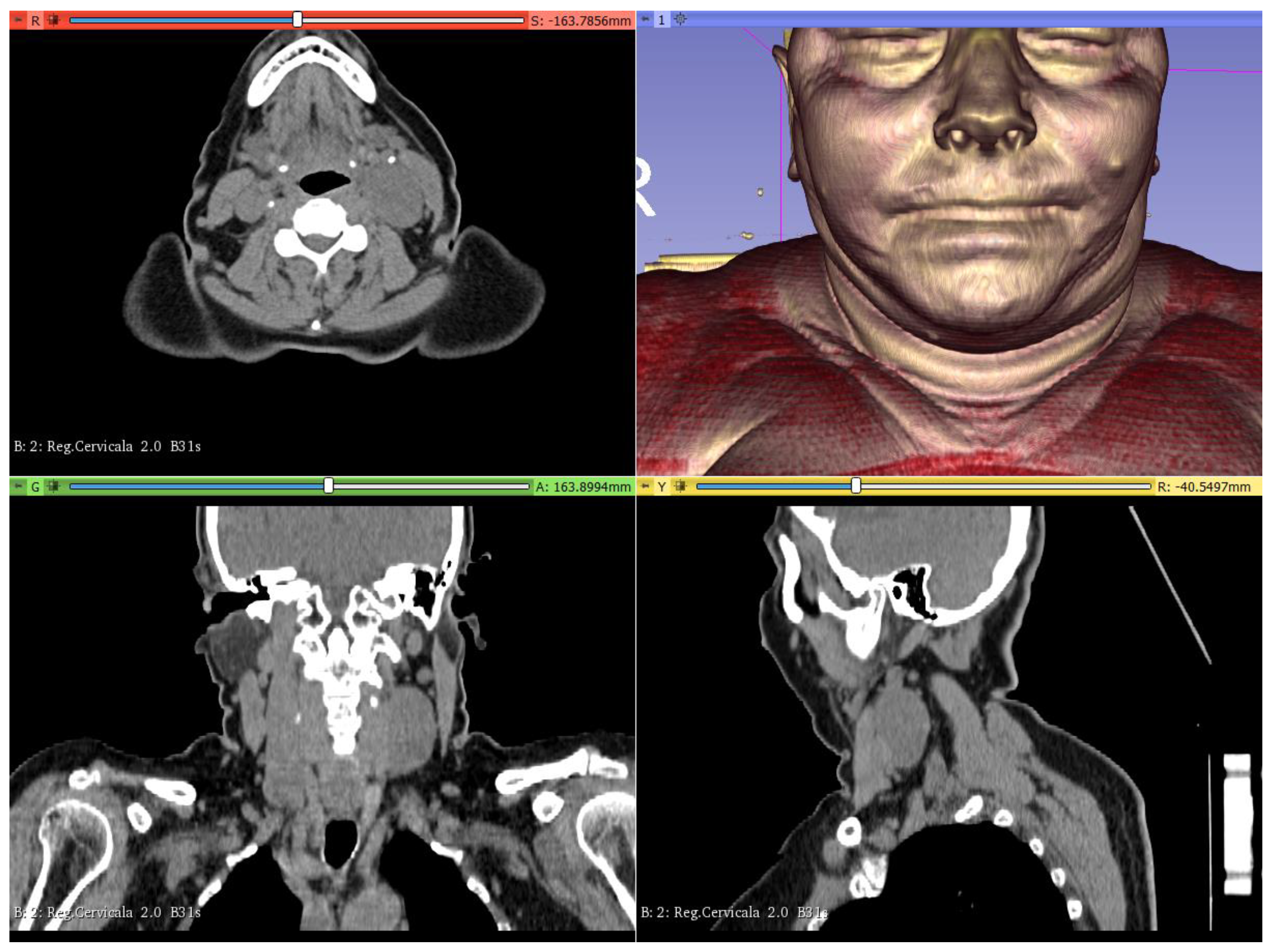
2.1. Diagnostic and Virtual Planning
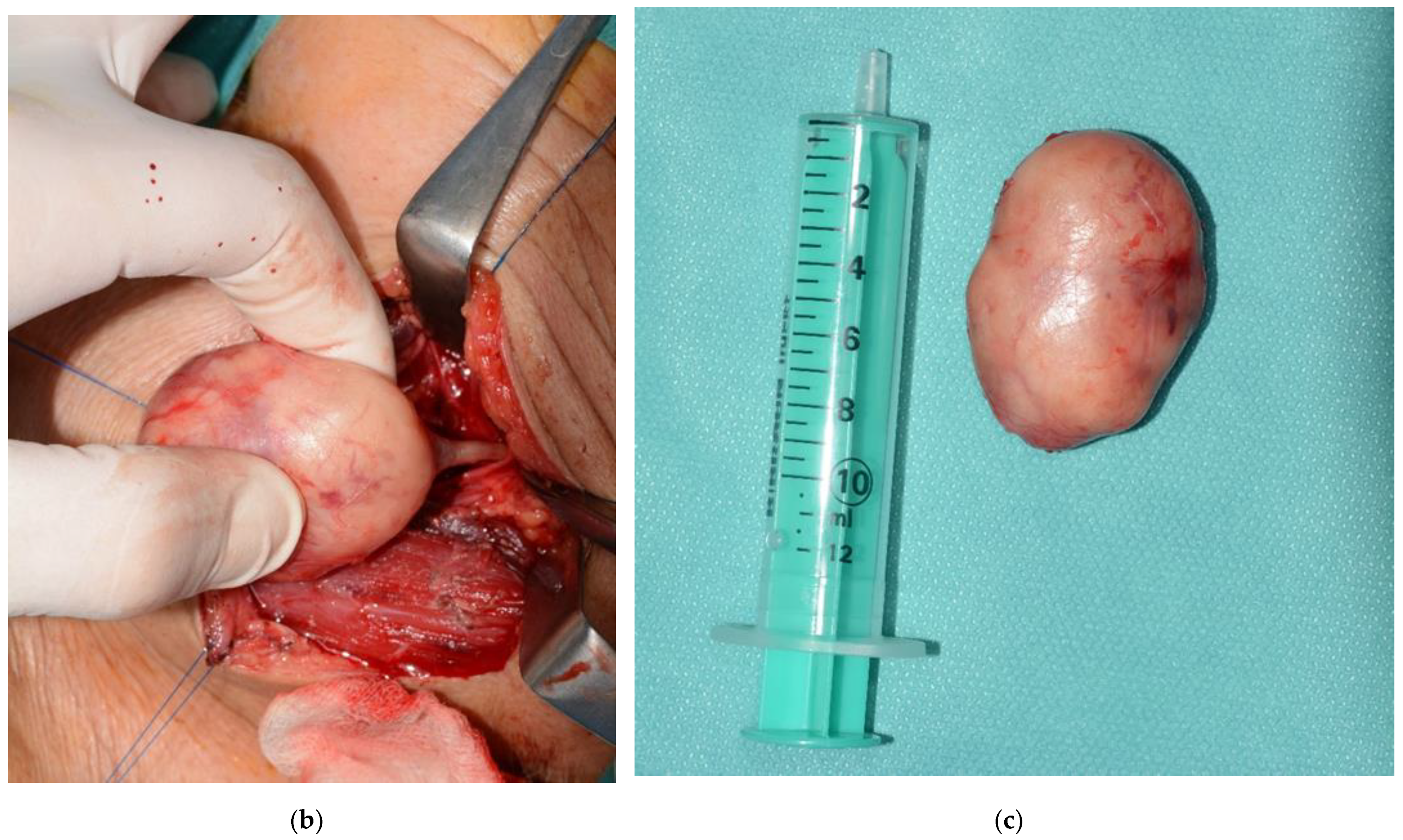
2.2. Surgical Procedures
2.3. Postoperative Care and Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Verocay, J. Zur kenntnis der’Neurofibrome’. Beitr. Path. Anat. 1910, 48, 1–60. [Google Scholar]
- Stout, A.P. The peripheral manifestations of the specific nerve sheath tumor (neurilemoma). Am. J. Cancer 1935, 24, 751–780. [Google Scholar] [CrossRef] [Green Version]
- Batsakis, J.G. Tumors of the peripheral nervous system. In Tumors Head Neck, 2nd ed.; Williams and Wilkins: Baltimore, MD, USA, 1979; pp. 313–333. [Google Scholar]
- Mohammad, A.; Iqbal, M.A.; Wadhwania, A. Schwannomas of the head and neck region: A report of two cases with a narrative review of the literature. Cancer Res. Stat. Treat. 2020, 3, 517. [Google Scholar]
- Adouly, T.; Adnane, C.; Oubahmane, T.; Rouadi, S.; Abada, R.; Roubal, M.; Mahtar, M. An unusual giant schwannoma of cervical sympathetic chain: A case report. J. Med. Case Rep. 2016, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- Kanatas, A.; Mücke, T.; Houghton, D.; Mitchell, D.A. Schwannomas of the head and neck. Oncol. Rev. 2009, 3, 107–111. [Google Scholar] [CrossRef]
- Wax, M.K.; Shiley, S.G.; Robinson, J.L.; Weissman, J.L. Cervical sympathetic chain schwannoma. Laryngoscope 2004, 114, 2210–2213. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswamy Chetty, Y.V.; Pankaja, S.S.; Kulkarni, S.V.; Sridhar, M.; Ranganatha, M. Benign paravertebral ancient neurilemmoma in a young adult: A rare occurrence. J. Clin. Diagn. Res. 2015, 9, PD11. [Google Scholar]
- Synková, B.; Holý, R.; Kovář, D.; Astl, J. Cystic Schwannoma of the Recurrent Laryngeal Nerve, a Rare Cause of Vocal Cord Paresis. Otorinolaryngol. Foniatr. 2017, 66, 81–83. [Google Scholar]
- Zhang, L.; Gao, M.; Zhang, T.; Chong, T.; Wang, Z.; Liu, W.; Li, H. Surgical management of retroperitoneal schwannoma complicated with severe hydronephrosis: A case report. Medicine 2018, 97, e12528. [Google Scholar] [CrossRef] [PubMed]
- Tulli, M.; Bondi, S.; Bussi, M. Voluminous laryngeal schwannoma excision with a mini-invasive external approach: A case report. Acta Otorhinolaryngol. Ital. 2017, 37, 242. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, W.P.; Brody, R.M.; LiVolsi, V.A.; Wang, A.R.; Mirza, N.A. Trauma-induced schwannoma of the recurrent laryngeal nerve after thyroidectomy. Laryngoscope 2016, 126, 1408–1410. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Wang, W.-C.; Chen, C.-H.; Chen, Y.-K.; Lin, L.-M. Ancient schwannoma of the mouth floor–A case report and review. Oral Oncol. Extra 2006, 42, 281–285. [Google Scholar] [CrossRef] [Green Version]
- Dsouza, R.; Kota, A.A.; Agarwal, S.; Issac, R. Cervical sympathetic schwannoma: A forgotten differential for Horner’s syndrome. ANZ J. Surg. 2020, 90, 638–640. [Google Scholar] [CrossRef]
- Ash, L.; Srinivasan, A.; Mukherj, S.K. Radiological Reasoning: Submucosal laryngeal mass. Am. J. Roentgenol. 2008, 191, S18–S21. [Google Scholar] [CrossRef] [PubMed]
- Saita, V.; Azzolina, A.; Galia, A.; Fraggetta, F. Schwannoma of the epiglottis: Case report focusing on clinico-pathological aspects. Acta Otorhinolaryngol. Ital. 2005, 25, 378. [Google Scholar]
- Al-Otieschan, A.T.; Mahasin, Z.Z.; Gangopadhyay, K.; Al-Dayel, F.; Jamshed, A. Schwannoma of the larynx: Two case reports and review of the literature. J. Otolaryngol. 1996, 25, 412–415. [Google Scholar] [PubMed]
- Fader, F.; Yunus, M.R.M.; Baki, M.M. Recurrent laryngeal nerve schwannoma: Same setting of resection and injection laryngoplasty. BMJ Case Rep. 2021, 14, e245193. [Google Scholar] [CrossRef]
- Tulli, M.; Bondi, S.; Smart, C.E.; Giordano, L.; Trimarchi, M.; Galli, A.; Di Santo, D.; Biafora, M.; Bussi, M. Diagnosis and treatment of laryngeal schwannoma: A systematic review. Otolaryngol. Neck Surg. 2018, 158, 222–231. [Google Scholar] [CrossRef]
- Behuria, S.; Rout, T.K.; Pattanayak, S. Diagnosis and management of schwannomas originating from the cervical vagus nerve. Ann. R. Coll. Surg. Engl. 2015, 97, 92–97. [Google Scholar] [CrossRef]
- Knulst, R.; Bosman, W.-M.; Ritchie, E.D.; da Costa, A. Cystic schwannoma of the recurrent laryngeal nerve: A rare finding posing diagnostic difficulties. Case Rep. 2014, 2014, bcr2014203873. [Google Scholar] [CrossRef]
- Berton, A.; Longo, U.G.; Candela, V.; Fioravanti, S.; Giannone, L.; Arcangeli, V.; Alciati, V.; Berton, C.; Facchinetti, G.; Marchetti, A. Virtual reality, augmented reality, gamification, and telerehabilitation: Psychological impact on orthopedic patients’ rehabilitation. J. Clin. Med. 2020, 9, 2567. [Google Scholar] [CrossRef]
- Longo, U.G.; De Salvatore, S.; Candela, V.; Zollo, G.; Calabrese, G.; Fioravanti, S.; Giannone, L.; Marchetti, A.; De Marinis, M.G.; Denaro, V. Augmented Reality, Virtual Reality and Artificial Intelligence in Orthopedic Surgery: A Systematic Review. Appl. Sci. 2021, 11, 3253. [Google Scholar] [CrossRef]
- Kim, H.J.; Jo, Y.J.; Choi, J.S.; Kim, H.J.; Park, I.S.; You, J.S.; Oh, J.S.; Moon, S.Y. Virtual reality simulation and augmented reality-guided surgery for total maxillectomy: A case report. Appl. Sci. 2020, 10, 6288. [Google Scholar] [CrossRef]
- Alauddin, M.S.; Baharuddin, A.S.; Mohd Ghazali, M.I. The Modern and Digital Transformation of Oral Health Care: A Mini Review. Healthcare 2021, 9, 118. [Google Scholar] [CrossRef]
- Huang, T.-K.; Yang, C.-H.; Hsieh, Y.-H.; Wang, J.-C.; Hung, C.-C. Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J. Med. Sci. 2018, 34, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinter, C.; Lasso, A.; Choueib, S.; Asselin, M.; Fillion-Robin, J.-C.; Vimort, J.-B.; Martin, K.; Jolley, M.A.; Fichtinger, G. Slicervr for medical intervention training and planning in immersive virtual reality. IEEE Trans. Med. Robot. Bionics 2020, 2, 108–117. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. NICE Guidelines; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- Mikoshi, A.; Edo, H.; Hase, T.; Sakima, T.; Uno, K.; Kumazawa, F.; Sato, K.; Shinmoto, H. Laryngeal schwannoma with extralaryngeal extension mimicking a thyroid tumour. Case Rep. 2021, 7, 20210089. [Google Scholar] [CrossRef]
- Lee, Y.S.; Kim, J.O.; Park, S.E. Ancient schwannoma of the thigh mimicking a malignant tumour: A report of two cases, with emphasis on MRI findings. Br. J. Radiol. 2010, 83, e154–e157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crist, J.; Hodge, J.R.; Frick, M.; Leung, F.P.; Hsu, E.; Gi, M.T.; Venkatesh, S.K. Magnetic resonance imaging appearance of schwannomas from head to toe: A pictorial review. J. Clin. Imaging Sci. 2017, 7, 38. [Google Scholar] [CrossRef]
- Domanski, H.A.; Åkerman, M.; Engellau, J.; Gustafson, P.; Mertens, F.; Rydholm, A. Fine-needle aspiration of neurilemoma (schwannoma). A clinicocytopathologic study of 116 patients. Diagn. Cytopathol. 2006, 34, 403–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartella, A.K.; Kamal, M.; Scholl, I.; Schiffer, S.; Steegmann, J.; Ketelsen, D.; Hölzle, F.; Lethaus, B. Virtual reality in preoperative imaging in maxillofacial surgery: Implementation of “the next level”? Br. J. Oral Maxillofac. Surg. 2019, 57, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Moreta-Martinez, R.; García-Mato, D.; García-Sevilla, M.; Pérez-Mañanes, R.; Calvo-Haro, J.A.; Pascau, J. Combining Augmented Reality and 3D Printing to Display Patient Models on a Smartphone. J. Vis. Exp. 2020, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romak, J.J.; Neel, H.B., III; Ekbom, D.C. Laryngeal schwannoma: A case presentation and review of the mayo clinic experience. J. Voice 2017, 31, 129.e15–129.e18. [Google Scholar] [CrossRef]
- Butler, R.T.; Patel, R.M.; McHugh, J.B. Head and neck schwannomas: 20-year experience of a single institution excluding cutaneous and acoustic sites. Head Neck Pathol. 2016, 10, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Ansari, I.; Ansari, A.; Graison, A.A.; Patil, A.J.; Joshi, H. Head and neck schwannomas: A surgical challenge—A series of 5 cases. Case Rep. Otolaryngol. 2018, 2018, 4074905. [Google Scholar] [CrossRef] [Green Version]
- Kshettry, V.R.; Hsieh, J.K.; Ostrom, Q.T.; Kruchko, C.; Barnholtz-Sloan, J.S. Incidence of vestibular schwannomas in the United States. J. Neurooncol. 2015, 124, 223–228. [Google Scholar] [CrossRef]
- House, S.A.; Fisher, E.L. Hoarseness in adults. Am. Fam. Physician 2017, 96, 720–728. [Google Scholar] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filipov, I.; Chirila, L.; Sandulescu, M.; Cristache, C.M. A Predictable Approach of a Rare and Frequently Misdiagnosed Entity: Laryngeal Nerve Schwannoma. Healthcare 2022, 10, 59. https://doi.org/10.3390/healthcare10010059
Filipov I, Chirila L, Sandulescu M, Cristache CM. A Predictable Approach of a Rare and Frequently Misdiagnosed Entity: Laryngeal Nerve Schwannoma. Healthcare. 2022; 10(1):59. https://doi.org/10.3390/healthcare10010059
Chicago/Turabian StyleFilipov, Iulian, Lucian Chirila, Mihai Sandulescu, and Corina Marilena Cristache. 2022. "A Predictable Approach of a Rare and Frequently Misdiagnosed Entity: Laryngeal Nerve Schwannoma" Healthcare 10, no. 1: 59. https://doi.org/10.3390/healthcare10010059