
Role-Play versus Standardised Patient Simulation for Teaching Interprofessional Communication in Care of the Elderly for Nursing Students

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
Background
2. Materials and Methods
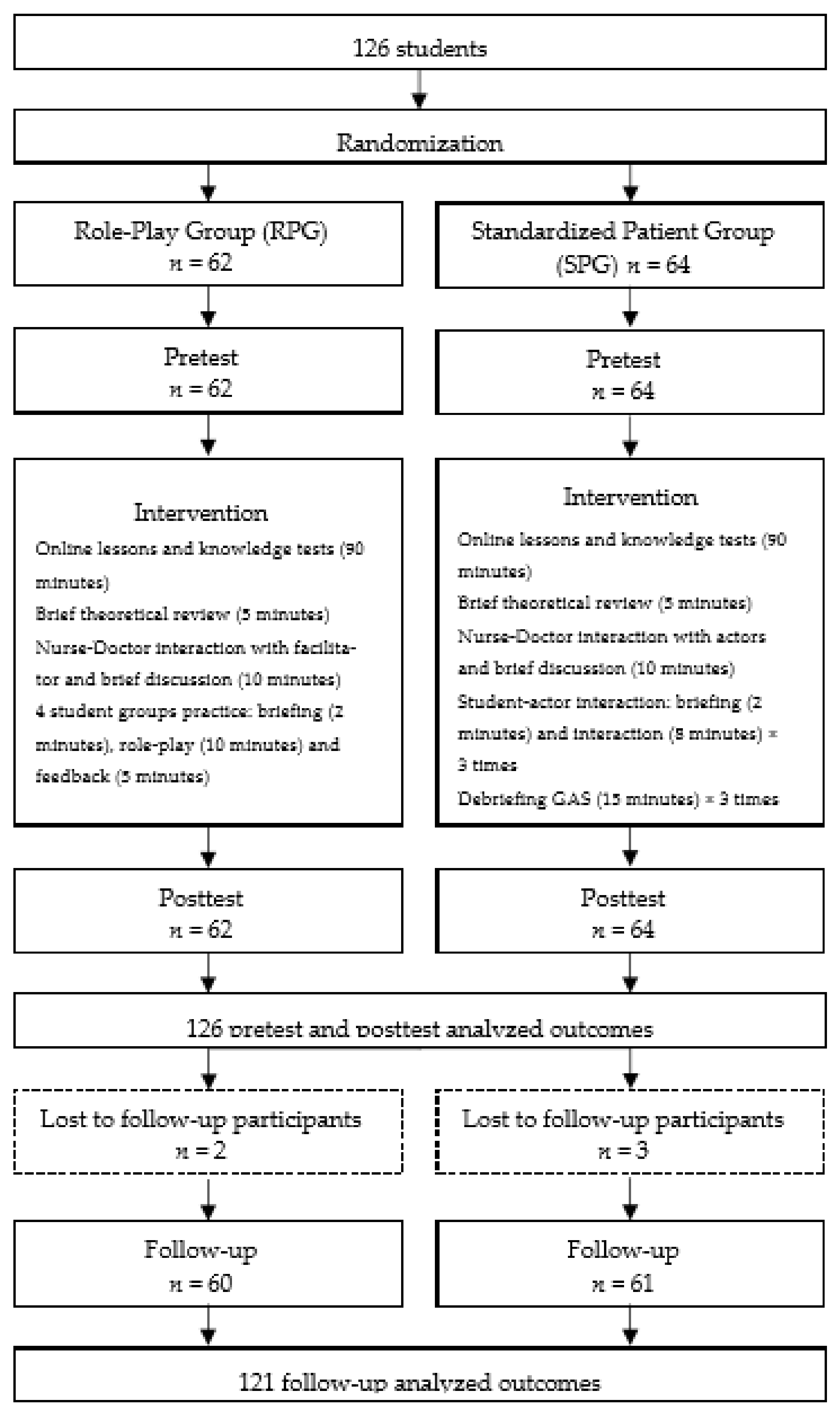
2.1. Design
2.2. Sample/Participants
2.3. Data Collection
2.4. Instruments
- The level of knowledge on interprofessional communication skills was assessed according to the interprofessional communication subscale of a multiple-choice questionnaire (IC-MCQ) [43]. The IC-MCQ comprised four questions about the situation-background-assessment-recommendation (SBAR) technique with five options and only one correct answer, including an ‘I don’t know’ answer.
- Psychomotor skills were assessed using the IC-Checklist [43]. The IC-Checklist comprised five items pertaining to the skills needed to exchange information with other healthcare professionals. Using a rubric, the items were rated on a scale of 0–5, from ‘not competent’ to ‘fully competent’.
- The level of self-efficacy was assessed with the ‘Patient clinical Information Exchange and interprofessional communication Self-Efficacy Scale’ (PIE-SES) from the ‘Clinical Communication Self-Efficacy Toolkit’ [44]. The PIE-SES comprised six items rated on a scale of 0–100, from ‘I’m sure I can’t do it’ to ‘I’m sure I can do it’.
2.5. Outcome Measures
2.6. Ethical Considerations
2.7. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Intervention Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Abd Hamid, N.Z.; Abdul Rasid, S.Z.; Maon, S.; Mohd Hassan, N.; Suddin, L.S. Interprofessional Communication and Interprofessional Collaboration (IPC) among Health Care Professionals. Eur. Proc. Soc. Behav. Sci. 2016. [Google Scholar] [CrossRef]
- Piers, R.D.; Versluys, K.; Devoghel, J.; Vyt, A.; Van Den Noortgate, N. Interprofessional Teamwork, Quality of Care and Turnover Intention in Geriatric Care: A Cross-Sectional Study in 55 Acute Geriatric Units. Int. J. Nurs. Stud. 2019, 91, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.B.; Drulia, T.; Lynch, L. Enhancing SLP Students’ Perceptions of Older Persons and Collaborative Practice through Geriatric Interprofessional Teamwork. Perspect. ASHA Spec. Interest Groups 2021, 6, 941–954. [Google Scholar] [CrossRef]
- Claramita, M.; Tuah, R.; Riskione, P.; Prabandari, Y.S.; Effendy, C. Comparison of Communication Skills between Trained and Untrained Students Using a Culturally Sensitive Nurse–Client Communication Guideline in Indonesia. Nurse Educ. Today 2016, 36, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Gleddie, M.; Stahlke, S.; Paul, P. Nurses’ Perceptions of the Dynamics and Impacts of Teamwork with Physicians in Labour and Delivery. J. Interprof. Care 2018, 1–11. [Google Scholar] [CrossRef]
- Song, H.-S.; Choi, J.; Son, Y.-J. The Relationship between Professional Communication Competences and Nursing Performance of Critical Care Nurses in South Korea. Int. J. Nurs. Pract. 2017, 23, e12576. [Google Scholar] [CrossRef]
- Turkelson, C.; Aebersold, M.; Redman, R.; Tschannen, D. Improving Nursing Communication Skills in an Intensive Care Unit Using Simulation and Nursing Crew Resource Management Strategies: An Implementation Project. J. Nurs. Care Qual. 2017, 32, 331–339. [Google Scholar] [CrossRef]
- The Joint Commission Most Commonly Reviewed Sentinel Event Types. Available online: https://www.jointcommission.org/assets/1/6/Event_type_4Q_2018.pdf (accessed on 21 March 2021).
- Foronda, C.; MacWilliams, B.; McArthur, E. Interprofessional Communication in Healthcare: An Integrative Review. Nurse Educ. Pract. 2016, 19, 36–40. [Google Scholar] [CrossRef]
- Jakobsen, R.B.; Gran, S.F.; Grimsmo, B.; Arntzen, K.; Fosse, E.; Frich, J.C.; Hjortdahl, P. Examining Participant Perceptions of an Interprofessional Simulation-Based Trauma Team Training for Medical and Nursing Students. J. Interprof. Care 2018, 32, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Younis, J.R.; Mabrouk, S.M.; Kamal, F.F. Effect of the Planned Therapeutic Communication Program on Therapeutic Communication Skills of Pediatric Nurses. J. Nurs. Educ. Pract. 2015, 5, 109. [Google Scholar] [CrossRef] [Green Version]
- Manias, E.; Geddes, F.; Watson, B.; Jones, D.; Della, P. Communication Failures during Clinical Handovers Lead to a Poor Patient Outcome: Lessons from a Case Report. SAGE Open. Med. Case Rep. 2015, 3, 2050313X15584859. [Google Scholar] [CrossRef]
- Granheim, B.M.; Shaw, J.M.; Mansah, M. The use of interprofessional learning and simulation in undergraduate nursing programs to address interprofessional communication and collaboration: An integrative review of the literature. Nurse Educ. Today 2018, 62, 118–127. [Google Scholar] [CrossRef] [Green Version]
- Wilhelmsson, M.; Svensson, A.; Timpka, T.; Faresjö, T. Nurses’ Views of Interprofessional Education and Collaboration: A Comparative Study of Recent Graduates from Three Universities. J. Interprof. Care 2013, 27, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Yeh, V.J.-H.; Sherwood, G.; Durham, C.F.; Kardong-Edgren, S.; Schwartz, T.A.; Beeber, L.S. Designing and Implementing Asynchronous Online Deliberate Practice to Develop Interprofessional Communication Competency. Nurse Educ. Pract. 2019, 35, 21–26. [Google Scholar] [CrossRef]
- Doherty, C.; Landry, H.; Pate, B.; Reid, H. Impact of Communication Competency Training on Nursing Students’ Self-Advocacy Skills. Nurse Educ. 2016, 41, 252–255. [Google Scholar] [CrossRef]
- Omura, M.; Stone, T.E.; Maguire, J.; Levett-Jones, T. Exploring Japanese Nurses’ Perceptions of the Relevance and Use of Assertive Communication in Healthcare: A Qualitative Study Informed by the Theory of Planned Behaviour. Nurse Educ. Today 2018, 67, 100–107. [Google Scholar] [CrossRef]
- Yu, M.; Kang, K. Effectiveness of a Role-Play Simulation Program Involving the Sbar Technique: A Quasi-Experimental Study. Nurse Educ. Today 2017, 53, 41–47. [Google Scholar] [CrossRef]
- Anderson, L.W.; Krathwohl, D.R. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives; Pearson Education Limited: London, UK, 2013. [Google Scholar]
- Eun, K.; Hye Young, K. Effects of Simulation-Based Education Combined Team-Based Learning on Self-Directed Learning, Communication Skills, Nursing Performance Confidence and Team Efficacy in Nursing Students. J. Korean Acad. Fundam. Nurs. 2017, 24, 39–50. [Google Scholar] [CrossRef]
- Recommendation of the European Parliament and Council of 23 April 2008 on the establishment of the European Qualifications Framework for lifelong learning (2008/C 111/01). Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:C:2008:111:0001:0007:EN:PDF (accessed on 23 December 2021).
- Bandura, A. Guide for constructing self-efficacy scales. In Self-Efficacy Beliefs of Adolescents; Pajares, F., Urdan, T., Eds.; Information Age Publishing: Charlotte, NC, USA, 2006. [Google Scholar]
- Orden CIN/2134/2008, de 3 de julio. Boletín Oficial del Estado, 19 de julio de 2008, núm. 174, p.31681. Available online: https://www.boe.es/boe/dias/2008/07/19/pdfs/A31680-31683.pdf (accessed on 23 December 2021).
- Anstey, S.; Powell, T.; Coles, B.; Hale, R.; Gould, D. Education and training to enhance end-of-life care for nursing home staff: A systematic literature review. BMJ Support. Palliat. Care 2016, 6, 353–361. [Google Scholar] [CrossRef]
- Lord, L.; Clark-Carter, D.; Grove, A. The Effectiveness of Communication-Skills Training Interventions in End-of-Life Noncancer Care in Acute Hospital-Based Services: A Systematic Review. Pall. Supp. Care 2016, 14, 433–444. [Google Scholar] [CrossRef]
- Moore, P.M.; Rivera, S.; Bravo-Soto, G.A.; Olivares, C.; Lawrie, T.A. Communication Skills Training for Healthcare Professionals Working with People Who Have Cancer. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Ross, A.J.; Anderson, J.E.; Kodate, N.; Thomas, L.; Thompson, K.; Thomas, B.; Key, S.; Jensen, H.; Schiff, R.; Jaye, P. Simulation Training for Improving the Quality of Care for Older People: An Independent Evaluation of an Innovative Programme for Inter-Professional Education. BMJ Qual. Saf. 2013, 22, 495–505. [Google Scholar] [CrossRef] [Green Version]
- Pazar, B.; Demiralp, M.; Erer, İ. The Communication Skills and the Empathic Tendency Levels of Nursing Students: A Cross-Sectional Study. Contemp. Nurse 2017, 53, 368–377. [Google Scholar] [CrossRef]
- Houghton, C.E.; Casey, D.; Shaw, D.; Murphy, K. Staff and Students’ Perceptions and Experiences of Teaching and Assessment in Clinical Skills Laboratories: Interview Findings from a Multiple Case Study. Nurse Educ. Today 2012, 32, e29–e34. [Google Scholar] [CrossRef]
- Shorey, S.; Kowitlawakul, Y.; Devi, M.K.; Chen, H.-C.; Soong, S.K.A.; Ang, E. Blended Learning Pedagogy Designed for Communication Module among Undergraduate Nursing Students: A Quasi-Experimental Study. Nurse Educ. Today 2018, 61, 120–126. [Google Scholar] [CrossRef]
- Schrant, B.L.; Archer, L.L.; Long, R. Human Patient Simulation as a Teaching Tool. Mo. Med. 2018, 115, 71–74. [Google Scholar]
- Bosse, H.M.; Nickel, M.; Huwendiek, S.; Schultz, J.H.; Nikendei, C. Cost-Effectiveness of Peer Role Play and Standardized Patients in Undergraduate Communication Training. BMC Med. Educ. 2015, 15, 183. [Google Scholar] [CrossRef] [Green Version]
- Gillette, C.; Stanton, R.B.; Rockich-Winston, N.; Rudolph, M.; Anderson, H.G. Cost-Effectiveness of Using Standardized Patients to Assess Student-Pharmacist Communication Skills. Am. J. Pharm. Educ. 2017, 81, 6120. [Google Scholar] [CrossRef] [Green Version]
- MacLean, S.; Kelly, M.; Geddes, F.; Della, P. Use of Simulated Patients to Develop Communication Skills in Nursing Education: An Integrative Review. Nurse. Educ. Today 2017, 48, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Judd, M. Broken Communication in Nursing Can Kill: Teaching Communication Is Vital. Creat. Nurs. 2013, 19, 101–104. [Google Scholar] [CrossRef]
- Liebrecht, C.; Montenery, S. Use of Simulated Psychosocial Role-Playing to Enhance Nursing Students’ Development of Soft Skills. Creat. Nurs. 2016, 22, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Arentsen, A.; Welsh, D.; Jones, M.; Weber, D.; Taylor, S.; Kuperstein, J.; Rayens, M.K.; Salt, E. Student Perception of Improvement in Communication and Value in 2 Interprofessional Education Delivery Formats. Nurse Educ. 2016, 41, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Chaharsoughi, N.; Ahrari, S.; Alikhah, S. Comparison the Effect of Teaching of SBAR Technique with Role Play and Lecturing on Communication Skill of Nurses. J. Caring Sci. 2014, 3, 141. [Google Scholar] [CrossRef]
- Kesten, K.S. Role-Play Using SBAR Technique to Improve Observed Communication Skills in Senior Nursing Students. J. Nurs. Educ. 2011, 50, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Mast, M.; Humbert, J.; Bagnardi, M.; Richards, S. Teaching Handoff Communication to Nursing Students: A Teaching Intervention and Lessons Learned. Nurse Educ. 2016, 41, 189–193. [Google Scholar] [CrossRef]
- INACSL Standards Committee. INACSL standards of best practice: SimulationSM Debriefing. Clin. Simul. Nurs. 2016, 12, S21–S25. [Google Scholar] [CrossRef] [Green Version]
- Phrampus, P.E.; O’Donnell, J. Debriefing using a structured and supported approach. In The Comprehensive Textbook of Healthcare Simulation; Levine, A.I., DeMaria, S., Schwartz, A.D., Sim, A., Eds.; Springer: New York, NY, USA, 2014; pp. 73–84. [Google Scholar]
- Cortés-Rodríguez, A.E. Comparison of the effects of two educational strategies on the development of competence in basic professional communication amongst nursing students. Ph.D. Thesis, University of Almería, Almería, Spain, 18 May 2020. [Google Scholar]
- Hernández-Padilla, J.M.; Cortés-Rodríguez, A.E.; Granero-Molina, J.; Fernández-Sola, C.; Correa-Casado, M.; Fernández-Medina, I.M.; López-Rodríguez, M.M. Design and psychometric evaluation of the ‘Clinical communication self-efficacy toolkit. Int. J. Environ. Res. Public Health 2019, 16, 4534. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Padilla, J.M.; Suthers, F.; Granero-Molina, J.; Fernández-Sola, C. Effects of two retraining strategies on nursing students’ acquisition and retention of BLS/AED skills: A cluster randomised trial. Resuscitation 2015, 93, 27–34. [Google Scholar] [CrossRef]
- Domuracki, K.; Wong, A.; Olivieri, L.; Grierson, L.E. The impacts of observing flawed and flawless demonstrations on clinical skill learning. Med. Educ. 2015, 49, 186–192. [Google Scholar] [CrossRef]
- Hernández-Padilla, J.M.; Granero-Molina, J.; Márquez-Hernández, V.V.; Cortés-Rodríguez, A.E.; Fernández-Sola, C. Effects of a simulation-based workshop on nursing students’ competence in arterial puncture. Acta Paul. Enferm. 2016, 29, 678–85678. [Google Scholar] [CrossRef] [Green Version]
- Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95/46/EC (General Data Protection Regulation). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016R0679 (accessed on 23 December 2021).
- Aebersold, M.; Tschannen, D.; Sculli, G. Improving Nursing Students’ Communication Skills Using Crew Resource Management Strategies. J. Nurs. Educ. 2013, 52, 125–130. [Google Scholar] [CrossRef]
- Hagemeier, N.E.; Hess, R.; Hagen, K.S.; Sorah, E.L. Impact of an Interprofessional Communication Course on Nursing, Medical, and Pharmacy Students’ Communication Skill Self-Efficacy Beliefs. Am. J. Pharm. Educ. 2014, 78, 186. [Google Scholar] [CrossRef] [Green Version]
- Liaw, S.Y.; Zhou, W.T.; Lau, T.C.; Siau, C.; Chan, S.W. An Interprofessional Communication Training Using Simulation to Enhance Safe Care for a Deteriorating Patient. Nurse Educ. Today 2014, 34, 259–264. [Google Scholar] [CrossRef]
- Smithburger, P.L.; Kane-Gill, S.L.; Kloet, M.A.; Lohr, B.; Seybert, A.L. Advancing Interprofessional Education through the Use of High Fidelity Human Patient Simulators. Pharm. Pract. 2013, 11, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Becker, K.L.; Rose, L.E.; Berg, J.B.; Park, H.; Shatzer, J.H. The Teaching Effectiveness of Standardized Patients. J. Nurs. Educ. 2006, 45, 10. [Google Scholar] [CrossRef]
- Quail, M.; Brundage, S.B.; Spitalnick, J.; Allen, P.J.; Beilby, J. Student Self-Reported Communication Skills, Knowledge and Confidence across Standardised Patient, Virtual and Traditional Clinical Learning Environments. BMC Med. Educ. 2016, 16, 73. [Google Scholar] [CrossRef] [Green Version]
- Khan, B.A.; Ali, F.; Vazir, N.; Barolia, R.; Rehan, S. Students’ perceptions of clinical teaching and learning strategies: A Pakistani perspective. Nurse Educ. Today 2012, 32, 85–90. [Google Scholar] [CrossRef]
- Gellis, Z.D.; Kim, E.; Hadley, D.; Packel, L.; Poon, C.; Forciea, M.A.; Bradway, C.; Streim, J.; Seman, J.; Hayden, T.; et al. Evaluation of Interprofessional Health Care Team Communication Simulation in Geriatric Palliative Care. Gerontol. Geriatr. Educ. 2019, 40, 30–42. [Google Scholar] [CrossRef]
- Brydges, R.; Nair, P.; Ma, I.; Shanks, D.; Hatala, R. Directed self-regulated learning versus instructor-regulated learning in simulation training. Med. Educ. 2012, 46, 648–656. [Google Scholar] [CrossRef]
- Cadorin, L.; Suter, N.; Dante, A.; Williamson, S.N.; Devetti, A.; Palese, A. Self-Directed Learning Competence Assessment within Different Healthcare Professionals and amongst Students in Italy. Nurse Educ. Pract. 2012, 12, 153–158. [Google Scholar] [CrossRef]
- Chen, M.C. Relationships among Self-Directed Learning, Learning Styles, Learning Strategies and Learning Achievement for Students of Technology University in Taiwan by Using Structural Equation Models. In Recent Researches in Educational Technologies; Gavriluta, N., Raducanu, R., Iliescu, M., Costin, H., Mastorakis, N., Olej, V., Strouhal, J., Eds.; WSEAS Press: Attica, Greece, 2010; pp. 67–72. [Google Scholar]
- Knowles, M. Self-Directed Learning: A Guide for Learners and Teachers; Cambridge Book Company: New York, NY, USA, 1975. [Google Scholar]
- Annonio, D.; Hoffman, L.A.; Zedreck, J.; Robertson, L.B.; Tuite, P.K.; Ready, S.E.T. Go Improving Patient-Nurse Communication. Nurs. Manag. 2016, 47, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H. Effects of a Support Program on Nurses’ Communication with Hospitalized Children’s Families. Compr. Child. Adolesc. Nurs. 2017, 40, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Rask, M.T.; Jensen, M.L.; Andersen, J.; Zachariae, R. Effects of an Intervention Aimed at Improving Nurse-Patient Communication in an Oncology Outpatient Clinic. Cancer Nurs. 2009, 32, E1–E11. [Google Scholar] [CrossRef] [PubMed]
- Raurell-Torredà, M.; Rascón-Hernán, C.; Malagón-Aguilera, C.; Bonmatí-Tomás, A.; Bosch-Farré, C.; Gelabert-Vilella, S.; Romero-Collado, A. Effectiveness of a training intervention to improve communication between/awareness of team roles: A randomized clinical trial. J. Prof. Nurs. 2020. [Google Scholar] [CrossRef]
- Medina Valadares, A.F.; Da Silva Magro, M.C. Opinion of nursing students on realistic simulation and the curriculum internship in hospital setting. ACTA Paul. Enferm. 2014, 27, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Hsu, L.-L.; Chang, W.-H.; Hsieh, S.-I. The Effects of Scenario-Based Simulation Course Training on Nurses’ Communication Competence and Self-Efficacy: A Randomized Controlled Trial. J. Prof. Nurs. 2015, 31, 37–49. [Google Scholar] [CrossRef]
- Doyle, D.; Copeland, H.L.; Bush, D.; Stein, L.; Thompson, S. A Course for Nurses to Handle Difficult Communication Situations.A Randomized Controlled Trial of Impact on Self-Efficacy and Performance. Patient Educ. Couns. 2011, 82, 100–109. [Google Scholar] [CrossRef]
- Brown, C.E.; Back, A.L.; Ford, D.W.; Kross, E.K.; Downey, L.; Shannon, S.E.; Curtis, J.R.; Engelberg, R.A. Self-Assessment Scores Improve After Simulation-Based Palliative Care Communication Skill Workshops. Am. J. Hosp. Palliat. Care 2018, 35, 45–51. [Google Scholar] [CrossRef]
- Roh, Y.S.; Ahn, J.W.; Kim, E.; Kim, J. Effects of prebriefing on psychological safety and learning outcomes. Clin. Simul. Nurs. 2018, 25, 12–19. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | SPG (n = 64) | RPG (n = 62) | Total Sample (n = 126) | t-Test | p-Value |
|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | |||
| Age (years) | 22.77 ± 6.70 | 22.29 ± 6.03 | 22.53 ± 6.36 | −0.44 | 0.66 |
| n (%) | n (%) | n (%) | Χ2 | p-value | |
| Gender Female Male | 51 (79.7) 13 (20.3) | 46 (74.2) 16 (25.8) | 97 (77.0) 29 (23.0) | 0.54 | 0.46 |
| Education level (completed) Upper secondary education Others | 62 (96.9) 2 (3.1) | 61 (98.4) 1 (1.6) | 123 (97.6) 3 (2.4) | 2.48 | 0.48 |
| Basic interpersonal communication training | 36 (56.2) | 45 (72.6) | 81 (64.3) | 0.06 | 0.80 |
| SPG | RPG | Time vs. Int. | |||||
|---|---|---|---|---|---|---|---|
| Pre-Test (n = 64) | Post-Test (n = 63) | Follow-Up (n = 63) | Pre-Test (n = 62) | Post-Test (n = 61) | Follow-Up (n = 61) | p 1 | |
| Knowledge | |||||||
| ≥70% of IC-MCQ answered correctly | 4(6%) | 46(72%) | 40(62%) | 7(11%) | 41(66%) | 46(74%) | 0.54 |
| Self-efficacy | |||||||
| ≥70% achieved in PIE-SES | 29(45%) | 47(76%) | 48(77%) | 30(48%) | 52(85%) | 50(82%) | 0.56 |
| Communication Skills | |||||||
| ≥3 points achieved in IC-Checklist | 27(42%) | 62(98%) | 60(97%) | 31(50%) | 59(97%) | 57(93%) | 0.99 |
| Interprofessional Communication Competence | |||||||
| Overall competence achieved 2 | 1(2%) | 36(56%) | 35(55%) | 2(3%) | 38(63%) | 42(68%) | 0.48 |
| SPG | RPG | SPG vs. RPG Pre-Test | SPG vs. RPG Post-Test | |||||
|---|---|---|---|---|---|---|---|---|
| Pre-Test n = 64 | Post-Test n = 63 | p-Value 1 | Pre-Test n = 62 | Post-Test n = 61 | p-Value 1 | p-Value 2 | p-Value 2 | |
| Knowledge | ||||||||
| ≥70% of IC-MCQ * answered correctly | 4(6%) | 46(72%) | <0.001 | 7(11%) | 41(66%) | <0.001 | 0.48 | 0.49 |
| Self-efficacy | ||||||||
| ≥70% in PIE-SES ** achieved | 29(45%) | 47(76%) | <0.001 | 30(48%) | 52(85%) | <0.001 | 0.53 | 0.20 |
| Communication skills | ||||||||
| ≥ 3 points achieved in IC-Checklist | 27(42%) | 62(98%) | <0.001 | 31(50%) | 59(97%) | <0.001 | 0.42 | 0.54 |
| Interprofessional communication competence | ||||||||
| Overall competency achieved 3 | 1(2%) | 36(56%) | <0.001 | 2(3%) | 38(63%) | <0.001 | 0.29 | 0.45 |
| SPG | RPG | SPG vs. RPG Follow-Up Test | |||||
|---|---|---|---|---|---|---|---|
| Post-Test n = 63 | Follow-Up Test n = 63 | p-Value 1 | Post-Test n = 62 | Follow-Up Test n = 61 | p-Value 1 | p-Value 2 | |
| Knowledge | |||||||
| ≥70% of IC-MCQ * answered correctly | 46(72%) | 40(62%) | 0.24 | 41(66%) | 46(74%) | 0.30 | 0.16 |
| Self-efficacy | |||||||
| ≥70% in PIE-SES ** achieved | 47(76%) | 48(77%) | 1 | 52(85%) | 50(82%) | 1 | 0.56 |
| Communication skills | |||||||
| ≥ 3 points achieved in IC-Checklist | 62(98%) | 60(97%) | 1 | 59(97%) | 57(93%) | 0.69 | 0.38 |
| Interprofessional communication competence | |||||||
| Overall competency achieved 3 | 36(56%) | 35(55%) | 1 | 38(63%) | 42(68%) | 0.61 | 0.13 |
| SPG | RPG | |||||
|---|---|---|---|---|---|---|
| Pre-Test n = 63 | Follow-Up Test n = 63 | p-Value 1 | Pre-Test n = 62 | Follow-Up Test n = 61 | p-Value 1 | |
| Knowledge | ||||||
| ≥70% of IC-MCQ * answered correctly | 4(6%) | 40(62%) | <0.001 | 7(11%) | 46(74%) | <0.001 |
| Self-efficacy | ||||||
| ≥70% in PIE-SES ** achieved | 29(45%) | 48(77%) | 0.004 | 30(48%) | 50(82%) | <0.001 |
| Communication skills | ||||||
| ≥3 points achieved in IC-Checklist | 27(42%) | 60(97%) | <0.001 | 31(50%) | 57(93%) | <0.001 |
| Interprofessional communication competence | ||||||
| Overall competency achieved 2 | 1(2%) | 35(55%) | <0.001 | 2(3%) | 42(68%) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortés-Rodríguez, A.E.; Roman, P.; López-Rodríguez, M.M.; Fernández-Medina, I.M.; Fernández-Sola, C.; Hernández-Padilla, J.M. Role-Play versus Standardised Patient Simulation for Teaching Interprofessional Communication in Care of the Elderly for Nursing Students. Healthcare 2022, 10, 46. https://doi.org/10.3390/healthcare10010046
Cortés-Rodríguez AE, Roman P, López-Rodríguez MM, Fernández-Medina IM, Fernández-Sola C, Hernández-Padilla JM. Role-Play versus Standardised Patient Simulation for Teaching Interprofessional Communication in Care of the Elderly for Nursing Students. Healthcare. 2022; 10(1):46. https://doi.org/10.3390/healthcare10010046
Chicago/Turabian StyleCortés-Rodríguez, Alda Elena, Pablo Roman, María Mar López-Rodríguez, Isabel María Fernández-Medina, Cayetano Fernández-Sola, and José Manuel Hernández-Padilla. 2022. "Role-Play versus Standardised Patient Simulation for Teaching Interprofessional Communication in Care of the Elderly for Nursing Students" Healthcare 10, no. 1: 46. https://doi.org/10.3390/healthcare10010046