
Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis


 ,
,  ,
, 

Abstract
:1. Introduction
2. Subjects and Methods
2.1. Research Design
2.2. Study Participants
2.3. Measurement Tools
2.4. Copenhagen Burnout Inventory
- (I)
- Personal exhaustion, which assesses the degree of physical and psychological exhaustion the person experiences. It refers to both the physical and psychological exhaustion that accumulates in a person during the day, (e.g.,“How often do you feel physically exhausted?”).
- (II)
- Work-related exhaustion, which assesses the degree of physical and psychological exhaustion the individual perceives about work. It describes work-related exhaustion (e.g.,“Is your job emotionally exhausting?”).
- (III)
- Patient-related exhaustion, which assesses the degree of physical and psychological exhaustion that is considered by the individual to be related to interaction with patients. It depicts exhaustion as a consequence of interpersonal relationships with patients (e.g.,“Does working with patients absorb your energy?”) [30].
2.5. Beck’s Depression Inventory
2.6. Sense of Coherence Questionnaire-13
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef]
- Tselebis, A.; Lekka, D.; Sikaras, C.; Tsomaka, E.; Tassopoulos, A.; Ilias, I.; Bratis, D.; Pachi, A. Insomnia, Perceived Stress, and Family Support among Nursing Staff during the Pandemic Crisis. Healthcare 2020, 8, 434. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Huang, E.; Zuo, Q.K. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: A meta-analysis. Ann. N. Y. Acad. Sci. 2021, 1486, 90–111. [Google Scholar] [CrossRef]
- Sikaras, C.; Ilias, I.; Tselebis, A.; Pachi, A.; Zyga, S.; Tsironi, M.; Gil, A.P.R.; Panagiotou, A. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health 2022, 9, 94–105. [Google Scholar] [CrossRef]
- Ibrahim, F.; Samsudin, E.Z.; Chen, X.W.; Toha, H.R. The Prevalence and Work-Related Factors of Burnout Among Public Health Workforce During the COVID-19 Pandemic. J. Occup. Environ. Med. 2022, 64, e20–e27. [Google Scholar] [CrossRef]
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Arnsten, A.F.T.; Shanafelt, T. Physician distress and burnout: The neurobiological perspective. Mayo Clin. Proc. 2021, 96, 763–769. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Greenglass, E.R. Introduction to special issue on burnout and health. Psychol. Health 2001, 16, 501–510. [Google Scholar] [CrossRef]
- Janeway, D. The Role of Psychiatry in Treating Burnout Among Nurses During the Covid-19 Pandemic. J. Radiol. Nurs. 2020, 39, 176–178. [Google Scholar] [CrossRef]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout-depression overlap: A review. Clin. Psychol. Rev. 2015, 36, 28–41. [Google Scholar] [CrossRef] [Green Version]
- Tavella, G.; Parker, G. Distinguishing burnout from depression: An exploratory qualitative study. Psychiatry Res. 2020, 291, 113212. [Google Scholar] [CrossRef]
- Bianchi, R.; Verkuilen, J.; Brisson, R.; Schonfeld, I.S.; Laurent, E. Burnout and depression: Label-related stigma, help-seeking, and syndrome overlap. Psychiatry Res. 2016, 245, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Kaschka, W.P.; Korczak, D.; Broich, K. Burnout: A fashionable diagnosis. Dtsch. Arztebl. Int. 2011, 108, 781. [Google Scholar] [CrossRef]
- Bakusic, J.; Schaufeli, W.; Claes, S.; Godderis, L. Stress, burnout and depression: A systematic review on DNA methylation mechanisms. J. Psychosom. Res. 2017, 92, 34–44. [Google Scholar] [CrossRef]
- Bakker, A.B.; Schaufeli, W.B.; Demerouti, E.; Janssen, P.P.; Van Der Hulst, R.; Brouwer, J. Using equity theory to examine the difference between burnout and depression. Anxiety Stress Coping 2000, 13, 247–268. [Google Scholar] [CrossRef]
- Iacovides, A.; Fountoulakis, K.; Kaprinis, S.; Kaprinis, G. The relationship between job stress, burnout and clinical depression. J. Affect. Disord. 2003, 75, 209–221. [Google Scholar] [CrossRef]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 13, 284. [Google Scholar] [CrossRef] [Green Version]
- Antonovsky, A. Health, Stress and Coping; Jossey Bass Inc.: San Francisco, CA, USA, 1979. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well; Jossey Bass Inc.: San Francisco, CA, USA, 1987. [Google Scholar]
- Eriksson, M.; Mittelmark, M.B. The Sense of Coherence and Its Measurement. In The Handbook of Salutogenesis; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Carstens, J.A.; Spangenberg, J.J. Major depression: A breakdown in sense of coherence? Psychol. Rep. 1997, 80, 1211–1220. [Google Scholar] [CrossRef]
- Généreux, M.; Schluter, P.J.; Landaverde, E.; Hung, K.K.; Wong, C.S.; Mok, C.P.Y.; Blouin-Genest, G.; O’Sullivan, T.; David, M.D.; Carignan, M.E.; et al. The Evolution in Anxiety and Depression with the Progression of the Pandemic in Adult Populations from Eight Countries and Four Continents. Int. J. Environ. Res. Public Health 2021, 18, 4845. [Google Scholar] [CrossRef]
- Tselebis, A.; Bratis, D.; Pachi, A.; Moussas, G.; Karkanias, A.; Harikiopoulou, M.; Theodorakopoulou, E.; Kosmas, E.; Ilias, I.; Siafakas, N.; et al. Chronic obstructive pulmonary disease: Sense of coherence and family support versus anxiety and depression. Psychiatrike 2013, 24, 109–116. [Google Scholar]
- Grothe, L.; Grothe, M.; Wingert, J.; Schomerus, G.; Speerforck, S. Stigma in Multiple Sclerosis: The Important Role of Sense of Coherence and Its Relation to Quality of Life. Int. J. Behav. Med. 2021, 1–7. [Google Scholar] [CrossRef]
- Kim, H.S.; Nho, J.H.; Nam, J.H. A serial multiple mediator model of sense of coherence, coping strategies, depression, and quality of life among gynecologic cancer patients undergoing chemotherapy. Eur.J. Oncol. Nurs. 2021, 54, 102014. [Google Scholar] [CrossRef]
- Malinauskiene, V.; Malinauskas, R. Predictors of Adolescent Depressive Symptoms. Int. J. Environ. Res. Public Health 2021, 18, 4508. [Google Scholar] [CrossRef]
- Stoyanova, K.; Stoyanov, D.S. Sense of Coherence and Burnout in Healthcare Professionals in the COVID-19 Era. Front. Psychiatry 2021, 12, 709587. [Google Scholar] [CrossRef]
- Tselebis, A.; Moulou, A.; Ilias, I. Burnout versus depression and sense of coherence: Study of Greek nursing staff. Nurs. Health Sci. 2001, 3, 69–71. [Google Scholar] [CrossRef]
- Samarati, P.; Sweeney, L. Protecting Privacy When Disclosing Information: K-Anonymity And Its Enforcement through Generalization and Suppression; Computer Science Laboratory—SRI International: Menlo Park, CA, USA, 1998. [Google Scholar]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Papaefstathiou, E.; Tsounis, A.; Malliarou, M.; Sarafis, P. Translation and validation of the Copenhagen Burnout Inventory amongst Greek doctors. Health Psychol. Res. 2019, 7, 7678. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, L.; Lukasse, M. Burnout among Norwegian midwives and the contribution of personal and work-related factors: A cross-sectional study. Sex. Reprod. Health 2016, 9, 42–47. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbauch, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Donias, S.; Demertzis, I. Validation of the Beck depression inventory. In Proceedings of the 10th Hellenic Congress of Neurology and Psychiatry, Thessaloniki, Greece, 1983; Varfis, G., Ed.; University Studio Press: Thessaloniki, Greece, 1983; pp. 486–492, (In Modern Greek). [Google Scholar]
- Tselebis, A.; Gournas, G.; Tzitzanidou, G.; Panagiotou, A.; Ilias, I. Anxiety and depression in Greek nursing and medical personnel. Psychol. Rep. 2006, 99, 93–96. [Google Scholar] [CrossRef]
- Antonovsky, A. The Structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef]
- Anagnostopoulou, T.; Kioseoglou, G. Sense of Coherence Scale. In Psychometric Tools in Greece; Stalikas, A., Triliva, S., Roussi, P., Eds.; EllinikaGrammata S.A.: Athens, Greece, 2002; pp. 291–292, (In Modern Greek). [Google Scholar]
- Nilsson, K.W.; Leppert, J.; Simonsson, B.; Starrin, B. Sense of coherence and psychological well-being: Improvement with age. J. Epidemiol. Community Health 2009, 64, 347–352. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Domínguez-Salas, S.; Rodríguez-Domínguez, C.; Allande-Cussó, R.; Romero-Martín, M.; Ruiz-Frutos, C. Gender perspective of psychological discomfort during COVID-19 confinement among Spanish adult population: A cross-sectional study. BMJ Open 2021, 11, e051572. [Google Scholar] [CrossRef]
- Carmel, S.; Anson, O.; Levenson, A.; Bonneh, D.Y.; Maoz, B. Life events, sense of coherence and health: Gender differences on the kibbutz. Soc. Sci. Med. 1991, 32, 1089–1096. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Sriharan, A.; West, K.J.; Almost, J.; Hamza, J.A.A.A. COVID-19-Related Occupational Burnout and Moral Distress among Nurses: A Rapid Scoping Review. Can. J. Nurs. Leadersh. 2021, 34, 7–19. [Google Scholar] [CrossRef]
- Elbarazi, I.; Loney, T.; Yousef, S.; Elias, A. Prevalence of and factors associated with burnout among health care professionals in Arab countries: A systematic review. BMC Health Serv. Res. 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tselebis, A.; Bratis, D.; Karkanias, A.; Apostolopoulou, E.; Moussas, G.; Gournas, G.; Ilias, I. Associations on dimensions of burnout and family support for a sample of Greek nurses. Psychol. Rep. 2008, 103, 63. [Google Scholar] [CrossRef]
- Abraham, C.M.; Zheng, K.; Norful, A.A.; Ghaffari, A.; Liu, J.; Poghosyan, L. Primary care nurse practitioner burnout and perceptions of quality of care. Nurs. Forum 2021, 56, 550–559. [Google Scholar] [CrossRef]
- Lastovkova, A.; Carder, M.; Rasmussen, H.M.; Sjoberg, L.; De Groene, G.J.; Sauni, R.; Vévoda, J.; Vevodova, S.; Lasfargues, G.; Svartengren, M.; et al. Burnout syndrome as an occupational disease in the European Union: An exploratory study. Ind. Health 2018, 56, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Généreux, M.; Schluter, P.J.; Hung, K.K.; Wong, C.S.; Pui Yin Mok, C.; O’Sullivan, T.; David, M.D.; Carignan, M.E.; Blouin-Genest, G.; Champagne-Poirier, O.; et al. One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults. Int. J. Environ. Res. Public Health 2020, 17, 8390. [Google Scholar] [CrossRef] [PubMed]
- Barni, D.; Danioni, F.; Canzi, E.; Ferrari, L.; Ranieri, S.; Lanz, M.; Iafrate, R.; Regalia, C.; Rosnati, R. Facing the COVID-19 Pandemic: The Role of Sense of Coherence. Front. Psychol. 2020, 11, 578440. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, S.K.; Sopp, M.R.; Schanz, C.G.; Staginnus, M.; Göritz, A.S.; Michael, T. Impact of COVID-19 on Public Mental Health and the Buffering Effect of a Sense of Coherence. Psychother. Psychosom. 2020, 89, 386–392. [Google Scholar] [CrossRef]
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to support resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst. Rev. 2020, 11, CD013779. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| P | D. S. | Age | W. E. (in Years) | BDI | Sense of Coherence Questionnaire (SOC) | Copenhagen Burnout Inventory (CBI) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | A | B | C | Total | Personal Burnout | Work Related Burnout | Patient Related Burnout | |||||
| Men N = 101 | Mean | 44.59 * | 19.07 | 6.93 ** | 65.13 ** | 24.64 ** | 18.50 ** | 21.98 * | 38.74 ** | 38.65 ** | 42.99 ** | 33.87 * |
| SD | 9.42 | 9.98 | 5.45 | 14.01 | 6.08 | 5.05 | 4.76 | 18.72 | 18.89 | 21.77 | 22.13 | |
| Women N= 559 | Mean | 42.13 * | 17.50 | 11.29 ** | 59.45 ** | 21.86 ** | 16.58 ** | 20.95 * | 49.03 ** | 52.22 ** | 54.67 ** | 39.27 * |
| SD | 9.89 | 10.75 | 8.16 | 12.94 | 5.88 | 4.85 | 4.39 | 18.36 | 19.05 | 21.67 | 22.98 | |
| Total N = 660 | Mean | 42.51 | 17.74 | 10.62 | 60.33 | 22.29 | 16.88 | 21.11 | 47.46 | 50.14 | 52.88 | 38.49 |
| SD | 9.85 | 10.64 | 7.95 | 7.95 | 5.99 | 4.93 | 4.44 | 18.77 | 19.63 | 22.07 | 22.92 | |
| Pearson Correlation N = 660 | AGE | Work Experience (in Years) | Sense of Coherence (SOC) | Beck Depression Inventory (BDI) | |
|---|---|---|---|---|---|
| Work Experience (in Years) | r | 0.922 ** | |||
| p | 0.001 | ||||
| Sense of Coherence (SOC) | r | 0.114 ** | 0.075 | ||
| p | 0.001 | 0.054 | |||
| Beck Depression Inventory (BDI) | r | 0.025 | 0.038 | −0.628 ** | |
| p | 0.518 | 0.329 | 0.001 | ||
| Copenhagen Burnout Inventory (CBI) | r | 0.045 | 0.094 * | −0.602 ** | 0.663 ** |
| p | 0.244 | 0.016 | 0.001 | 0.001 | |
| Dependent Variable: Beck Depression Inventory (BDI) | R Square | R Square Change | Beta | t | p |
|---|---|---|---|---|---|
| Copenhagen Burnout Inventory (CBI) | 0.437 | 0.437 | 0.661 | 22.55 | 0.01 * |
| Sense of Coherence (SOC) | 0.721 | 0.083 | −0.361 | −10.66 | 0.01 * |
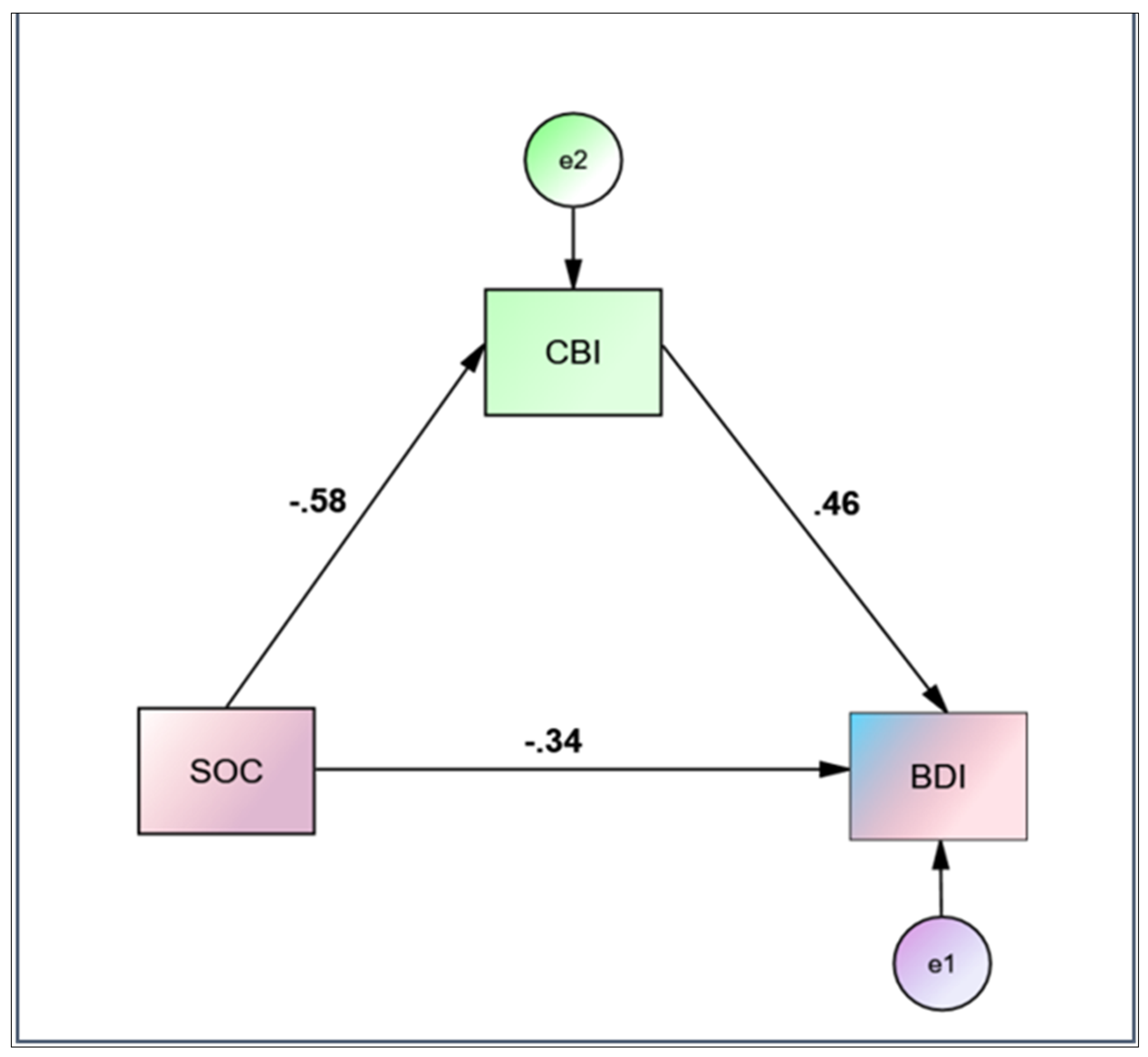
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
| SOC → CBI | −0.8515 | 0.0442 | −19.2810 | 0.001 | −0.9382 | −0.7648 |
| SOC → BDI | −0.3759 | 0.0182 | −20.6734 | 0.001 | −0.4115 | −0.3402 |
| SOC → CBI → BDI | 0.1875 | 0.0143 | 13.0854 | 0.001 | 0.1594 | 0.2157 |
| Effects | ||||||
| Direct | −0.2162 | 0.0203 | −10.6601 | 0.001 | −0.2560 | −0.1764 |
| Indirect * | −0.1597 | 0.0149 | −0.1899 | −0.1308 | ||
| Total | −0.3759 | 0.0182 | −20.6734 | 0.001 | −0.4115 | −0.3402 |
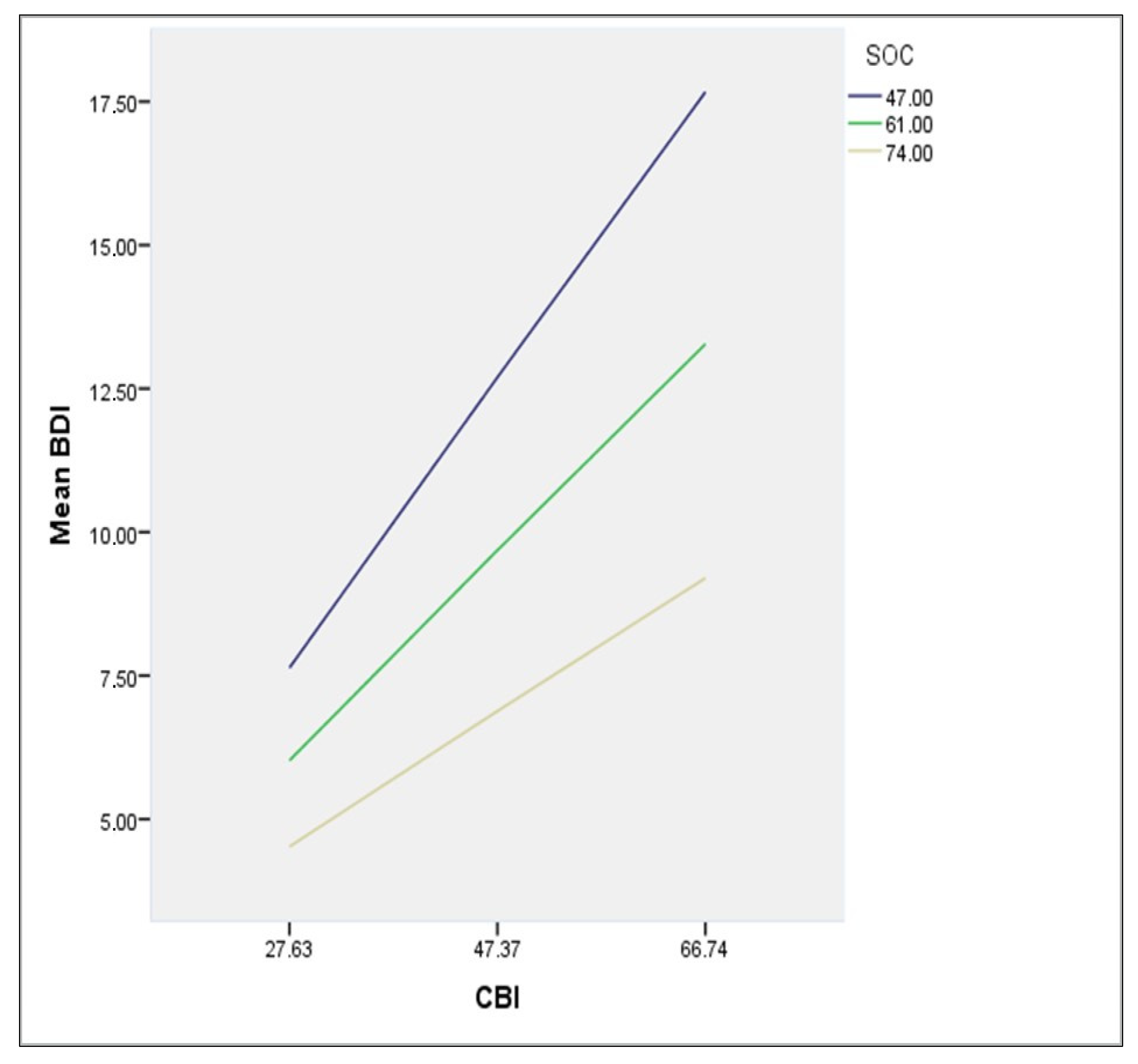
| Outcome Variable: Beck Depression Inventory (BDI) | b | SE | t | p |
|---|---|---|---|---|
| Constant | −0.6021 [−6.0401, 4.8359] | 2.7694 | −0.2174 | 0.8280 |
| Copenhagen Burnout Inventory (CBI) | 0.4945 [0.4037, 0.5853] | 0.0463 | 10.6909 | 0.001 |
| Sense of coherence (SOC) | 0.0246 [−0.0535, 0.1026] | 0.0398 | 0.617 | 0.5371 |
| Interaction (CBI × SOC) | −0.0051 [−0.0065, −0.0036] | 0.0007 | −6.9555 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pachi, A.; Sikaras, C.; Ilias, I.; Panagiotou, A.; Zyga, S.; Tsironi, M.; Baras, S.; Tsitrouli, L.A.; Tselebis, A. Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare 2022, 10, 134. https://doi.org/10.3390/healthcare10010134
Pachi A, Sikaras C, Ilias I, Panagiotou A, Zyga S, Tsironi M, Baras S, Tsitrouli LA, Tselebis A. Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare. 2022; 10(1):134. https://doi.org/10.3390/healthcare10010134
Chicago/Turabian StylePachi, Argyro, Christos Sikaras, Ioannis Ilias, Aspasia Panagiotou, Sofia Zyga, Maria Tsironi, Spyros Baras, Lydia Aliki Tsitrouli, and Athanasios Tselebis. 2022. "Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis" Healthcare 10, no. 1: 134. https://doi.org/10.3390/healthcare10010134