
Effect of Home-Based Tele-Pilates Intervention on Pregnant Women: A Pilot Study



Abstract
:1. Introduction
2. Materials
2.1. Subject
2.2. HTPE Program
2.3. Body Composition
2.4. Pelvic Tilt
2.5. Muscles of the Hip Joint
2.6. ODI Test
2.7. PSQI Test
2.8. Statistical Analyses
3. Results
3.1. Effect of HTPE on the Body Composition
3.2. Effect of HTPE on Muscles of the Hip Joint
3.3. Effect of HTPE on the Pelvic Tilt
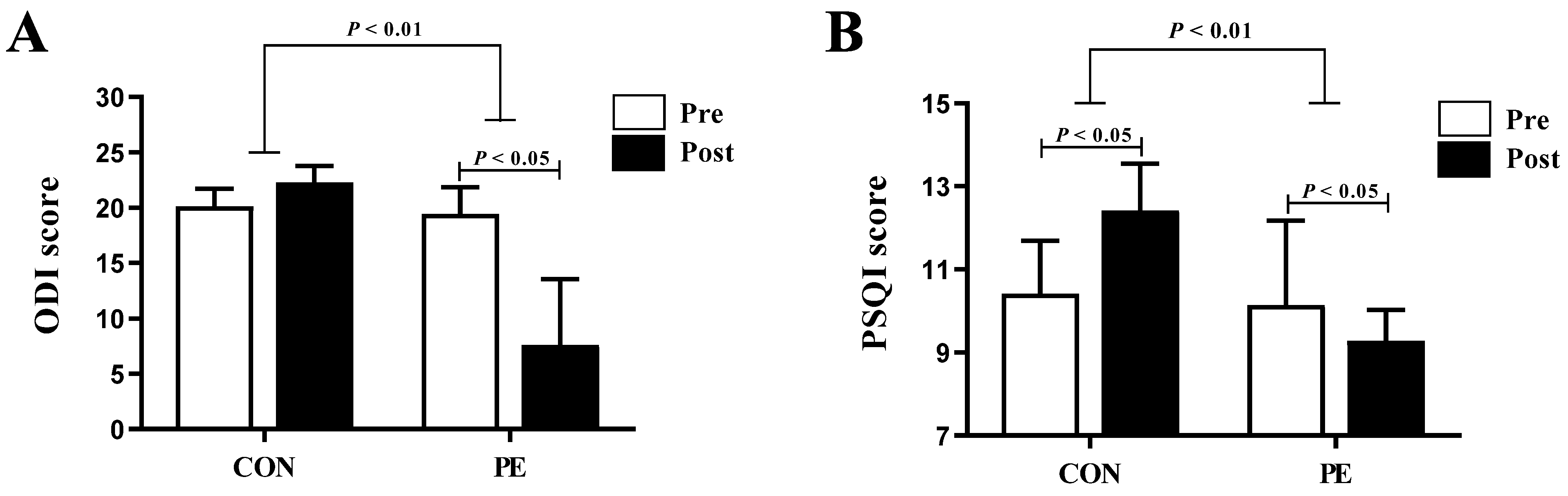
3.4. Effect of HTPE on the ODI and PSQI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mappa, I.; Distefano, F.A.; Rizzo, G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: A prospectic observational study. J. Perinat. Med. 2020, 48, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, R.; Hocaoğlu, M.; Günay, T.; Yardımcı, O.D.; Turgut, A.; Karateke, A. Anxiety and depression symptoms in the same pregnant women before and during the COVID-19 pandemic. J. Perinat. Med. 2020, 48, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Silva-Jose, C.; Sánchez-Polán, M.; Diaz-Blanco, Á.; Coterón, J.; Barakat, R.; Refoyo, I. Effectiveness of a Virtual Exercise Program During COVID-19 Confinement on Blood Pressure Control in Healthy Pregnant Women. Front. Physiol. 2021, 12, 279. [Google Scholar] [CrossRef]
- Marbán-Castro, E.; Pons-Duran, C.; García-Otero, L.; Chen, H.; Herrera, L.B.; Gil, M.d.M.; Goncé, A.; Ferriols-Pérez, E.; Rodríguez, M.Á.; Toro, P.; et al. Acceptability of Clinical Trials on COVID-19 during Pregnancy among Pregnant Women and Healthcare Providers: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 10717. [Google Scholar] [CrossRef]
- Long, G.; Haoning, M.; Ping, Y.; Mingsheng, T. Asymmetry in Paraspinal Muscles as a Predictor of the Development of Pregnancy-Related Low Back and Pelvic Pain: A Prospective Study. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Morino, S.; Ishihara, M.; Umezaki, F.; Hatanaka, H.; Yamashita, M.; Kawabe, R.; Aoyama, T. The effects of pelvic belt use on pelvic alignment during and after pregnancy: A prospective longitudinal cohort study. BMC Pregnancy Childbirth 2019, 19, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signe, N.; Nina, K.; Siv, M.; Kjell, Å.; Hilde, S. Impact of job adjustment, pain location and exercise on sick leave due to lumbopelvic pain in pregnancy: A longitudinal study. Scand. J. Prim. Health Care 2019, 37, 218–226. [Google Scholar]
- Chen, H.; D’Onofrio, G.; Hameed, F. Role of Exercise Treatment of Low Back Pain in Pregnancy. Curr. Phys. Med. Rehabil. Rep. 2020, 8, 322–328. [Google Scholar] [CrossRef]
- Pascual-Morena, C.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Lucerón-Lucas-Torres, M.; Sanabria-Martínez, G.; Poyatos-León, R.; Rodríguez-Martín, B.; Martínez-Vizcaíno, V. Exercise versus Metformin to Improve Pregnancy Outcomes among Overweight Pregnant Women: A Systematic Review and Network Meta-Analysis. J. Clin. Med. 2021, 10, 3490. [Google Scholar] [CrossRef]
- Sultan, A.; Burcu, A.; Ayseren, C.; Ebru, G.; Sule, G. The Effects of COVID-19 Pandemic on Pregnant Women: Perceived Stress, Social Support and Sleep Quality. Yonago Acta Med. 2020, 63, 360–367. [Google Scholar]
- ACOG. Practice Advisory: Novel Coronavirus 2019 (COVID-19). 2020. American College of Obstetricians and Gynecologists. 2019. Available online: https://www.acog.org/Clinical-Guidance-and-Publications/Practice-Advisories/Practice-Advisory-Novel-Coronavirus (accessed on 12 December 2021).
- Mazzarino, M.; Kerr, D.; Morris, M. pilates program design and health benefits for pregnant women: A practitioners’ survey. J Bodyw. Mov. Ther. 2018, 22, 411–417. [Google Scholar] [CrossRef]
- Rodrigo, S.; Leonardo, A.; Deivison, S. Effects of the practice of Pilates in pregnancy: A literature review. Rev. Saúde Física Ment. 2019, 7, 30–44. [Google Scholar]
- Nadholta, P.; Bali, P.; Singh, A.; Anand, A. Potential benefits of Yoga in pregnancy-related complications during the COVID-19 pandemic and implications for working women. Work 2020, 67, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Rahul, T.; Pravin, K. The effects of selected Pilates exercise on the body composition of obese people. J. Crit. Rev. 2020, 7, 3374–3381. [Google Scholar]
- Rodríguez-Díaz, L.; Ruiz-Frutos, C.; Vázquez-Lara, J.M.; Ramírez-Rodrigo, J.; Villaverde-Gutiérrez, C.; Torres-Luque, G. Effectiveness of a physical activity programme based on the Pilates method in pregnancy and labour. Enferm. Clín. 2017, 27, 271–277. [Google Scholar] [CrossRef] [Green Version]
- Fairbank, J.; Couper, J.C.; Davies, J.B.; O’Brien, J.P. The Oswestry Low Back Pain Disability Questionnaire. Physiotherapy 1980, 66, 271–273. [Google Scholar]
- DiPietro, L.; Al-Ansari, S.S.; Biddle, S.J.; Borodulin, K.; Bull, F.C.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; et al. Advancing the global physical activity agenda: Recommendations for future research by the 2020 WHO physical activity and sedentary behavior guidelines development group. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–11. [Google Scholar] [CrossRef]
- Alessandro, G.; Gian, P.; Fabio, V.; Mara, P.; Palmira, B.; Laura, C.; Amerigo, G. Feasibility and cost-effectiveness of a multidisciplinary home-telehealth intervention programme to reduce falls among elderly discharged from hospital: Study protocol for a randomized controlled trial. BMC Geriatr. 2016, 16, 209. [Google Scholar]
- Hong, J.; Kim, J.; Kim, S.; Kong, H. Effects of home-based tele-exercise on sarcopenia among community-dwelling elderly adults: Body composition and functional fitness. Exp. Gerontol. 2017, 87 Pt A, 33–39. [Google Scholar] [CrossRef]
- James, H.; Mohanraj, T.; Hui, Y.; Dori, P.; Tracy, T.; Emily, R.; Tapan, M. Rationale and design of the tele-exercise and multiple sclerosis (TEAMS) study: A comparative effectiveness trial between a clinic- and home-based telerehabilitation intervention for adults with multiple sclerosis (MS) living in the deep south. Contemp. Clin. Trials 2018, 71, 186–193. [Google Scholar]
- Mohanraj, T.; James, H.; George, J.; Jereme, W.; Tapan, M.; Byron, L. TEAMS (Tele-Exercise and Multiple Sclerosis), a Tailored Telerehabilitation mHealth App: Participant-Centered Development and Usability Study. JMIR Mhealth Uhealth 2018, 6, e1018. [Google Scholar]
- Jen, J.; Dan, M.; Fadia, H.; Anna, S.; Eliezer, N.; Shlomit, R. Tele-Exercise as a Promising Tool to Promote Exercise in Children With Cystic Fibrosis. Front Public Health 2018, 6, 269. [Google Scholar]
- Jorge, C.; Jorge, P.; Serafín, D.; José Carlos, C.; Manuel, G.; Jorge, R.; Laura, M.; Sabina, B.; María, M.; Angelina, P.; et al. Cost-Effectiveness of “Tele-Square Step Exercise” for Falls Prevention in Fibromyalgia Patients: A Study Protocol. Int. J. Environ. Res. Public Health 2020, 17, 695. [Google Scholar]
- Park, D.S.; Jung, S.H. Effects of hamstring self-stretches on pelvic mobility in persons with low back pain. Phys. Ther. Rehabil. Sci. 2020, 9, 140–148. [Google Scholar] [CrossRef]
- Back, C.; Joo, J.; Kim, Y. Association between muscular strengths and gait characteristics of elderly people aged 65 to 74 and 75 and above. J. Korea Acad. -Ind. Coop. Soc. 2020, 2, 415–422. [Google Scholar]
- Lee, S.; Nam, S. Effects of Active Release Technique on Pain, Oswestry Disability Index and Pelvic Asymmetry in Chronic Low Back Pain Patients. Korean Soc. Phys. Med. 2020, 15, 133–141. [Google Scholar] [CrossRef]
- Kim, K.; Cho, Y.; Bae, J. Quality of sleep and quality of life measured monthly in pregnant women in South Korea. Sleep Breathin. 2020, 24, 1219–1222. [Google Scholar] [CrossRef]
- Suran, G.; Wenmei, S.; Chang, L.; Siwei, W. Structural Validity of the Pittsburgh Sleep Quality Index in Chinese Undergraduate Students. Front. Psychol. 2016, 3. [Google Scholar] [CrossRef] [Green Version]
- Birsner, M.; Bannerman, C. Physical activity and exercise during pregnancy and the postpartum period: ACOG committee opinion, number 804. Obs. Gynecol. 2020, 135, 178–188. [Google Scholar]
- Evangelou, C.; Sakkas, G.K.; Hadjicharalambous, M.; Aphamis, G.; Petrou, P.; Giannaki, C.D. The effect of a three month, low-load- high-repetitions group-based exercise program versus pilates on physical fitness and body composition in inactive women. J. Bodyw. Mov. Ther. 2021, 26, 18–23. [Google Scholar] [CrossRef]
- Sonmezer, E.; Özköslü, M.; Yosmaoğlu, H. The effects of clinical pilates exercises on functional disability, pain, quality of life and lumbopelvic stabilization in pregnant women with low back pain: A randomized controlled study. J. Back Musculoskelet. Rehabil. 2021, 34, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Kharitonova, L.; Papysheva, O.; Kotaish, G. The role of dyslipidemia in pregnant women with diabetes mellitus in the genesis of comorbid conditions in children. Exp. Clin. Gastroenterol. 2020, 1, 66–75. [Google Scholar] [CrossRef]
- Semra, Ç.; Cuma, E.; Murat, Ş.; Nedim, Ç.; Alaeddin, A. The Effects of Pilates and Aerobic Exercise on Blood Pressure, Heart Rates, and Blood Serum Lipids in Sedentary Females. J. Educ. Train. Stud. 2019, 7, 2324–8068. [Google Scholar]
- Hyun, H.; Jeon, J. Effect of Mat Pilates on Body Fluid Composition, Pelvic Stabilization, and Muscle Damage during Pregnancy. Appl. Sci. 2020, 10, 9111. [Google Scholar] [CrossRef]
- Baek, S. The Effect of 12weeks Pilates Mat Exercise on Body Composition and Lipid Metabolism in Obese Middle-aged Women. DAEHAN Soc. Ind. Manag. 2020, 18, 108–117. [Google Scholar]
- Hu, X.; Ma, M.; Zhao, X.; Sun, W.; Liu, Y.; Zheng, Z.; Xu, L. Effects of exercise therapy for pregnancy-related low back pain and pelvic pain: A protocol for systematic review and meta-analysis. Medicine 2020, 99, 17318. [Google Scholar] [CrossRef] [PubMed]
- Lene, C.; Nina, K. Trunk, pelvic and hip kinematics during the Stork test in pregnant women with pelvic girdle pain, asymptomatic pregnant and non-pregnant women. Clin. Biomech. 2020, 80, 105168. [Google Scholar]
- Saori, M.; Mika, I.; Fumiko, U.; Hiroko, H.; Mamoru, Y.; Tomoki, A. Pelvic alignment changes during the perinatal period. PLoS ONE 2019, 10, e0223776. [Google Scholar] [CrossRef]
- Kulkarni, M.; Saini, S.; Palekar, T.; Hamdulay, N. Effects of pilates on core muscle strength and endurance in post 6 months delivered women. Proteus J. 2020, 11, 0889–6348. [Google Scholar]
- Sakamoto, A.; Nakagawa, H.; Nakagawa, H.; Gamada, K. Effects of exercises with a pelvic realignment device on low-back and pelvic girdle pain after childbirth: A randomized control study. J. Rehabil. Med. 2018, 50, 914–919. [Google Scholar] [CrossRef] [Green Version]
- Bogaert, J.; Stack, M.; Partington, S.; Marceca, J.; Tremback-Ball, A. The effects of stabilization exercise on low back pain and pelvic girdle pain in pregnant women. Ann. Phys. Rehabil. Med. 2018, 61, 157–158. [Google Scholar] [CrossRef]
- Pascoal, G.; Stuge Mota, P.; Hilde, G.; Bø, K. Therapeutic Exercise Regarding Musculoskeletal Health of the Pregnant Exerciser and Athlete. In Exercise and Sporting Activity During Pregnancy; Springer Science and Business Media LLC: Berlin, Germany, 2019; pp. 309–326. [Google Scholar]
- Buysse, D.; Reynolds, C.; Monk, T.; Berman, S.; Kupfer, D. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Picerno, P.; Pecori, R.; Raviolo, P.; Ducange, P. Smartphones and Exergame Controllers as BYOD Solutions for the e-tivities of an Online Sport and Exercise Sciences University Program. In Higher Education Learning Methodologies and Technologies Online; Burgos, D., Ed.; HELMeTO 2019. Communications in Computer and Information Science; Springer: Cham, Switzerland, 2019; Volume 1091. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Modes | Contents | Time (min) | Reps, Set, and Rest | RPE |
|---|---|---|---|---|
| Warm-up | Low-impact stretching and Breathing | 10 | 10 | |
| Main exercise | Level 1: 1–3 week Arm circle, Cat cow, Bridge, Clam, Half-spine rotation, Leg circles, Half-squat Level 2: 4–6 week Donkey kick, Hip hinge, Leg side up, Half-saw, Half-lunges, Kneeing push-up Level 3: 7–8 week Half-lunge twist, Side lateral raise, Squat, Low-impact down dog, Deep breathing | 30 | 12–15 reps × 3 set 10 s rest between sets | 11–13 |
| Cool-down | Total body stretching | 10 | 10 |
| CON (n = 7) | PE (n = 7) | Diff (Post-Pre) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | p | Cohen’s d | |
| BW (kg) | 64.50 (8.70) | 69.90 (8.90) * | 69.10 (13.00) | 72.50 (16.20) * | 0.456 | 0.337 |
| SMM (kg) | 27.70 (9.00) | 28.20 (10.70) * | 23.40 (8.70) | 29.50 (8.10) * | 0.805 | 0.228 |
| BFM (kg) | 23.70 (12.10) | 24.90 (10.90) * | 25.10 (8.00) | 29.50 (8.10) | 0.259 | 0.706 |
| PBF (%)) | 39.30 (14.20) | 40.40 (9.80) * | 37.90 (11.10) | 37.70 (14.60) * | 0.209 | 0.768 |
| BMI (kg/m2) | 23.50 (1.60) | 25.50 (2.10) * | 25.30 (5.10) | 26.90 (4.80) * | 0.383 | 0.706 |
| FFM (kg) | 39.70 (10.40) | 39.90 (8.80) * | 40.60 (13.60) | 44.50 (18.20) * | 0.128 | 0.861 |
| CON (n = 7) | PE (n = 7) | Difference (Post-Pre) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | p | Cohen’s d | |
| RHF (lbs) ## | 3.80 (2.40) | 3.60 (2.30) | 4.30 (2.20) | 6.40 (3.80) * | 0.001 | 2.939 |
| RHA (lbs) ## | 3.50 (0.80) | 3.20 (0.70) | 5.00 (3.60) | 7.10 (1.70) * | 0.001 | 6.958 |
| LHF (lbs) ## | 3.60 (1.20) | 3.40 (1.00) | 4.80 (3.00) | 6.80 (2.90) * | 0.001 | 4.482 |
| LHA (lbs) ## | 3.30 (0.80) | 3.20 (1.40) | 4.30 (1.50) | 7.00 (1.80) * | 0.001 | 6.889 |
| CON (n = 7) | PE (n = 7) | Diff (Post-Pre) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | p | Cohen’s d | |
| 2.00 (0.00) | 3.00 (2.00) * | 2.00 (1.00) | 2.00 (2.00) | 0.259 | 0.681 | |
| 22.00 (8.00) | 28.00 (5.00) * | 24.00 (18.00) | 28.00 (12.00) * | 0.456 | 0.774 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyun, A.-H.; Cho, J.-Y.; Koo, J.-H. Effect of Home-Based Tele-Pilates Intervention on Pregnant Women: A Pilot Study. Healthcare 2022, 10, 125. https://doi.org/10.3390/healthcare10010125
Hyun A-H, Cho J-Y, Koo J-H. Effect of Home-Based Tele-Pilates Intervention on Pregnant Women: A Pilot Study. Healthcare. 2022; 10(1):125. https://doi.org/10.3390/healthcare10010125
Chicago/Turabian StyleHyun, Ah-Hyun, Joon-Yong Cho, and Jung-Hoon Koo. 2022. "Effect of Home-Based Tele-Pilates Intervention on Pregnant Women: A Pilot Study" Healthcare 10, no. 1: 125. https://doi.org/10.3390/healthcare10010125