
Prevalence of Frailty in the Middle East: Systematic Review and Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Search Strategy
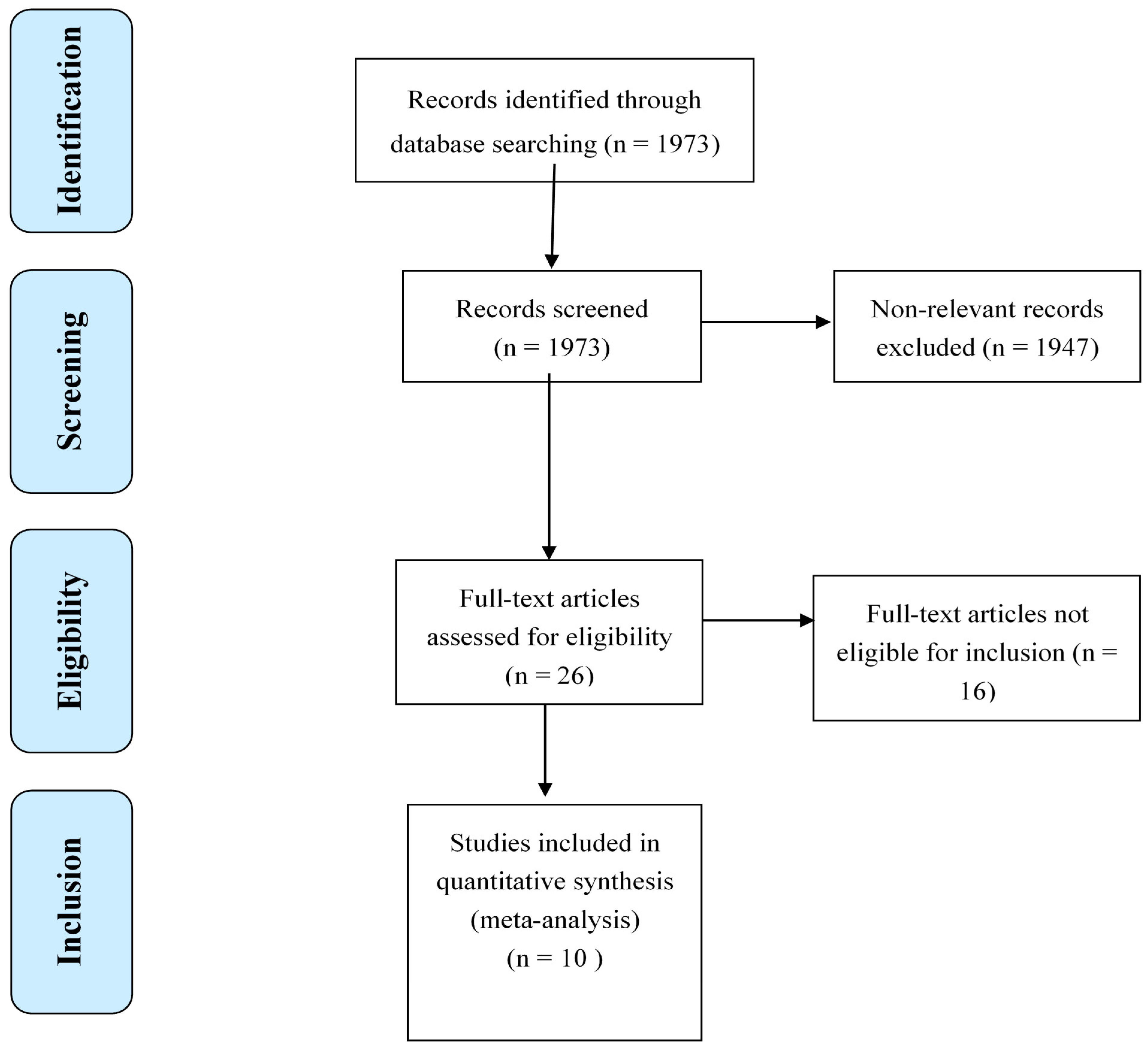
2.4. Study Selection
2.5. Data Extraction and Quality Assessment
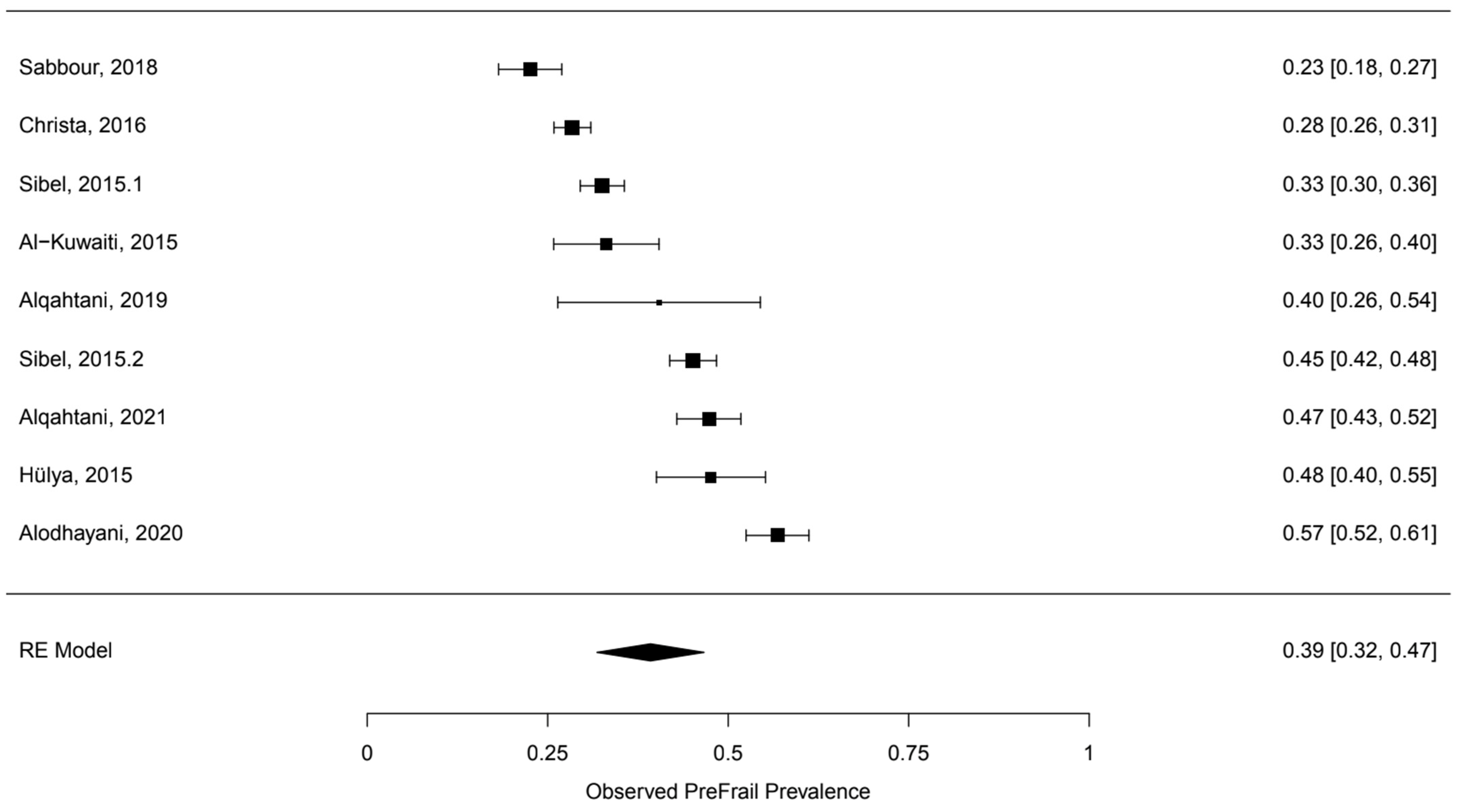
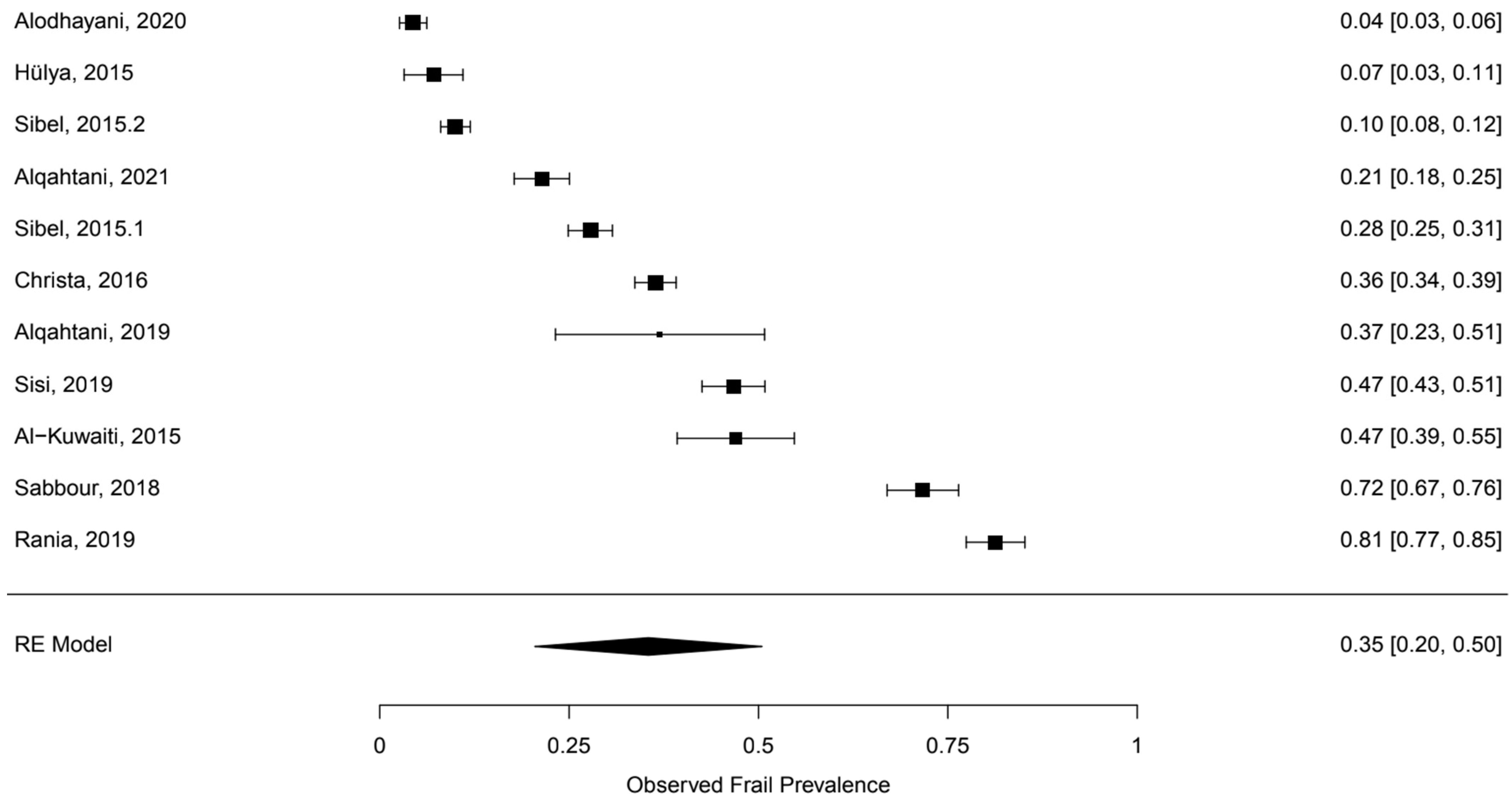
2.6. Data Synthesis and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Mañas, L.; Féart, C.; Mann, G.; Viña, J.; Chatterji, S.; Chodzko-Zajko, W.; Gonzalez-Colaço Harmand, M.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an operational definition of frailty: A Delphi method based consensus statement. The frailty operative definition-consensus conference project. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2013, 68, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Abate, M.; Di Iorio, A.; Di Renzo, D.; Paganelli, R.; Saggini, R.; Abate, G. Frailty in the elderly: The physical dimension. Eur. Med. Phys. 2006, 43, 407–415. [Google Scholar]
- Morley, J.E.; Vellas, B.; Van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of ageing. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Andrew, M.; Mitnitski, A. A comparison of two approaches to measuring frailty in elderly people. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 738–743. [Google Scholar] [CrossRef] [PubMed]
- Stow, D.; Matthews, F.E.; Barclay, S.; Iliffe, S.; Clegg, A.; De Biase, S.; Robinson, L.; Hanratty, B. Evaluating frailty scores to predict mortality in older adults using data from population-based electronic health records: A case-control study. Age Ageing 2018, 47, 564–569. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Howlett, S.E.; MacKnight, C.; Beattie, B.L.; Bergman, H.; Hébert, R.; Hogan, D.B.; Wolfson, C.; McDowell, I. Prevalence, attributes, and outcomes of fitness and frailty in community-dwelling older adults: Report from the Canadian study of health and ageing. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 1310–1317. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Cawthon, P.M.; Fink, H.A.; Taylor, B.C.; Cauley, J.A.; Dam, T.-T.; Marshall, L.M.; Orwoll, E.S.; Cummings, S.R.; et al. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men. J. Am. Geriatr. Soc. 2009, 57, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Bandeen-Roche, K.; Xue, Q.L.; Ferrucci, L.; Walston, J.; Guralnik, J.M.; Chaves, P.; Zeger, S.L.; Fried, L.P. Phenotype of frailty: Characterization in the women’s health and ageing studies. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 262–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.P.; Morley, J.E.; Ong, P.; et al. Frailty: An emerging public health priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Siriwardhana, D.D.; Hardoon, S.; Rait, G.; Weerasinghe, M.C.; Walters, K.R. Prevalence of frailty and prefrailty among community-dwelling older adults in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Open 2018, 8, e018195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Al-Kuwaiti, S.J.; Aziz, F.; Blair, I. Frailty in community-dwelling older people in Abu Dhabi, United Arab Emirates: A cross-sectional study. Front. Public Health 2015, 3, 248. [Google Scholar] [CrossRef] [Green Version]
- Alodhayani, A.A.; Alsaad, S.M.; Almofarej, N.; Alrasheed, N.; Alotaibi, B. Frailty, sarcopenia and health-related outcomes among elderly patients in Saudi Arabia. Saudi J. Biol. Sci. 2020, 28, 1213–1217. [Google Scholar] [CrossRef]
- Sabbour, S.M.; Abdul Rahamn, S.A.; Amin, G.E.; Mohamed, B.A. Frailty and malnutrition among Egyptian elderly: Prevalence and risk factors in the nursing home and community-dwelling elderly. Egypt. J. Geriatr. Gerontol. 2018, 5, 1–5. [Google Scholar] [CrossRef]
- Abdi, M.; Dabiran, S.; Hedayati, M.; Farmani, M.; Abdolmaleki, E.Y.; Rahidi, N. Prevalence of frailty and Prefrailty among Iraniancommunity-dwelling Older Adults. J. Res. Lepid. 2020, 51, 100–109. [Google Scholar] [CrossRef]
- Akın, S.; Mazıcıoglu, M.M.; Mucuk, S.; Gocer, S.; Şafak, E.D.; Arguvanlı, S.; Ozturk, A. The prevalence of frailty and related factors in community-dwelling Turkish elderly according to modified Fried Frailty Index and FRAIL scales. Ageing Clin. Exp. Res. 2015, 27, 703–709. [Google Scholar] [CrossRef]
- Khamis, R.; Sabbah, H.; Sabbah, S.; Peters, L.; Droubi, N.; Sabbah, I. Evaluating the psychometric properties of the Arabic version of the Groningen Frailty Indicator among Lebanese elderly people. J. Egypt. Public Health Assoc. 2019, 94, 28. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, B.A.; Alenazi, A.M.; Alshehri, M.M.; Osailan, A.M.; Alsubaie, S.F.; Alqahtani, M.A. Prevalence of frailty and associated factors among Saudi community-dwelling older adults: A cross-sectional study. BMC Geriatr. 2021, 21, 185. [Google Scholar] [CrossRef]
- Alqahtani, B.A.; Nasser, T.A. Assessment of frailty in Saudi community-dwelling older adults: Validation of measurements. Ann. Saudi Med. 2019, 39, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Boulos, C.; Salameh, P.; Barberger-Gateau, P. Malnutrition and frailty in community dwelling older adults living in a rural setting. Clin. Nutr. 2016, 35, 138–143. [Google Scholar] [CrossRef]
- Sisi, M.M.; Shamshirgaran, S.M.; Rezaeipandari, H.; Matlabi, H. Multidimensional approach to frailty among rural older people: Applying the Tilburg frailty indicator. Elder. Health J. 2019, 5, 92–101. [Google Scholar] [CrossRef]
- Çakmur, H. Frailty among elderly adults in a rural area of Turkey. Med. Sci. Monit. 2015, 21, 1232–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mata, F.A.F.D.; Pereira, P.P.D.S.; de Andrade, K.R.C.; Figueiredo, A.C.M.G.; Silva, M.T.; Pereira, M.G. Prevalence of frailty in Latin America and the Caribbean: A Systematic Review and Meta-analysis. PLoS ONE 2016, 11, e0160019. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Sezgin, D.; O’Donovan, M.R.; Molloy, D.W.; Clegg, A.; Rockwood, K.; Liew, A. Prevalence of frailty in 62 countries across the world: A systematic review and meta-analysis of population-level studies. Age Ageing 2021, 50, 96–104. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs. World Population Ageing 2017; United Nations: New York, NY, USA, 2017.
- Sukkriang, N.; Punsawad, C. Comparison of geriatric assessment tools for frailty among community elderly. Heliyon 2020, 6, e04797. [Google Scholar] [CrossRef]
- Singh, S.; Bajorek, B. Defining ‘elderly’ in clinical practice guidelines for pharmacotherapy. Pharm. Pract. 2014, 12, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caterino, J.M.; Valasek, T.; Werman, H.A. Identification of an age cutoff for increased mortality in patients with elderly trauma. Am. J. Emerg. Med. 2010, 28, 151–158. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Country | Sample Size (% Male) | Mean Age | Outcomes | Prevalence of Frailty % | Study Settings | Methods of Sampling | Was the Sample Size Justified? Powered |
|---|---|---|---|---|---|---|---|---|
| Al-Kuwaiti et al. (2015) [15] | UAE | 160 (53%) | 65.6 | Fried Frailty Criteria | 47 | Community-dwelling | Convenience sampling | yes |
| Alodhayani et al. (2020) [16] | Saudi Arabia | 498 (27%) | 69.9 | Edmonton frailty scale | 4.41 | Public tertiary hospital | Convenience sampling | yes |
| Sabbour et al. (2018) [17] | Egypt | 350 (50%) | 66.3 | SHARE Frailty Instrument | 71.7 | Community + nursing homes | Convenience sampling | no |
| Sibel et al. (2015) [19] | Turkey | 906 (94.4%) | 71.5 | Fried Frailty Criteria | 27.8 | Community-dwelling | Random sampling | no |
| Sibel et al. (2015) [19] | Turkey | 906 (94.4%) | 71.5 | FRAIL scale | 10 | Community-dwelling | Random sampling | no |
| Rania et al. (2019) [20] | Iran | 555 (52%) | 71.5 | Tilburg Frailty Indicator | 46.7 | Community-dwelling | Random sampling | yes |
| Alqahtani et al. (2021) [23] | Saudi Arabia | 486 (65%) | 71 | Fried Frailty Criteria | 21.4 | Community-dwelling | Convenience sampling | yes |
| Alqahtani et al. (2019) [24] | Saudi Arabia | 47 (16%) | 70 | Frail scale | 37 | Community-dwelling | Convenience sampling | no |
| Christa et al. (2016) [25] | Lebanon | 1200 (46%) | 75.7 | Study of Osteoporotic Fractures | 36.4 | Community-dwelling | Random sampling | no |
| Sisi et al. (2019) [26] | Iran | 555 (52%) | 71.5 | Tilburg Frailty Indicator | 46.7 | Community-dwelling | Random sampling | yes |
| Hulya et al. (2015) [27] | Turkey | 168 (46%) | 72.7 | Fried Frailty Criteria | 7.1 | Community-dwelling | Convenience sampling | yes |
| Study | Selection | Comparability | Outcome | Total |
|---|---|---|---|---|
| Al-Kuwaiti et al. (2015) [15] | *** | * | *** | 7 |
| Alodhayani et al. (2020) [16] | *** | ** | 5 | |
| Sabbour et al. (2018) [17] | * | ** | 3 | |
| Sibel et al. (2015) [19] | *** | * | *** | 7 |
| Sibel et al. (2015) [19] | *** | * | *** | 7 |
| Rania et al. (2019) [20] | **** | **** | 8 | |
| Alqahtani et al. (2021) [23] | *** | * | ** | 6 |
| Alqahtani et al. (2019) [24] | *** | *** | 6 | |
| Christa et al. (2016) [25] | **** | * | ** | 7 |
| Sisi et al. (2019) [26] | **** | *** | 7 | |
| Hulya et al. (2015) [27] | *** | ** | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, B.A.; Alshehri, M.M.; Elnaggar, R.K.; Alsaad, S.M.; Alsayer, A.A.; Almadani, N.; Alhowimel, A.; Alqahtani, M.; Alenazi, A.M. Prevalence of Frailty in the Middle East: Systematic Review and Meta-Analysis. Healthcare 2022, 10, 108. https://doi.org/10.3390/healthcare10010108
Alqahtani BA, Alshehri MM, Elnaggar RK, Alsaad SM, Alsayer AA, Almadani N, Alhowimel A, Alqahtani M, Alenazi AM. Prevalence of Frailty in the Middle East: Systematic Review and Meta-Analysis. Healthcare. 2022; 10(1):108. https://doi.org/10.3390/healthcare10010108
Chicago/Turabian StyleAlqahtani, Bader A., Mohammed M. Alshehri, Ragab K. Elnaggar, Saad M. Alsaad, Ahmed A. Alsayer, Noura Almadani, Ahmed Alhowimel, Mohammed Alqahtani, and Aqeel M. Alenazi. 2022. "Prevalence of Frailty in the Middle East: Systematic Review and Meta-Analysis" Healthcare 10, no. 1: 108. https://doi.org/10.3390/healthcare10010108