1. Introduction
The enormous demand for medical implants has led to advances in the areas of biomaterials, engineering methods, and digital technologies [
1]. Biomaterials are characteristic or engineered materials utilized to strengthen or substitute tissue, organ, or organic structure with a view to improving the well-being of patients [
2]. Titanium and its combinations are among the few biomaterials that coordinate the human body’s prerequisite of supplanting bone tissue. Titanium alloys such as Ti6Al4V are considered to be the most favored metallic biomaterial for medical and healthcare applications [
3]. They provide a remarkable blend of elevated resistance to weight ratio, acceptable density, and superior corrosion resistance, as well as they are biocompatible and have nonmagnetic properties. Moreover, an appreciable ascent in the manufacturing of tailor-fabricated titanium implants with finer structure and biomechanical assistance has been acknowledged in medical applications. To improve the quality of the patient’s life, facilitating and applying customized implants is essential. Additionally, the study of the implant regarding its design fitting accuracy, biomechanical properties, and manufacturing process is of paramount importance.
The maxillofacial reconstruction is regarded as a strenuous and important procedure by surgeons. This can be related to the patient’s strict anatomical specifications, the mandible curvature, and the effective recovery of chewing and oral functioning [
4,
5]. The issue of mandibular reconstruction is even further exacerbated by a dramatic rise in mandibular abnormalities due to the complexity of the human body and evolving chewing behavior [
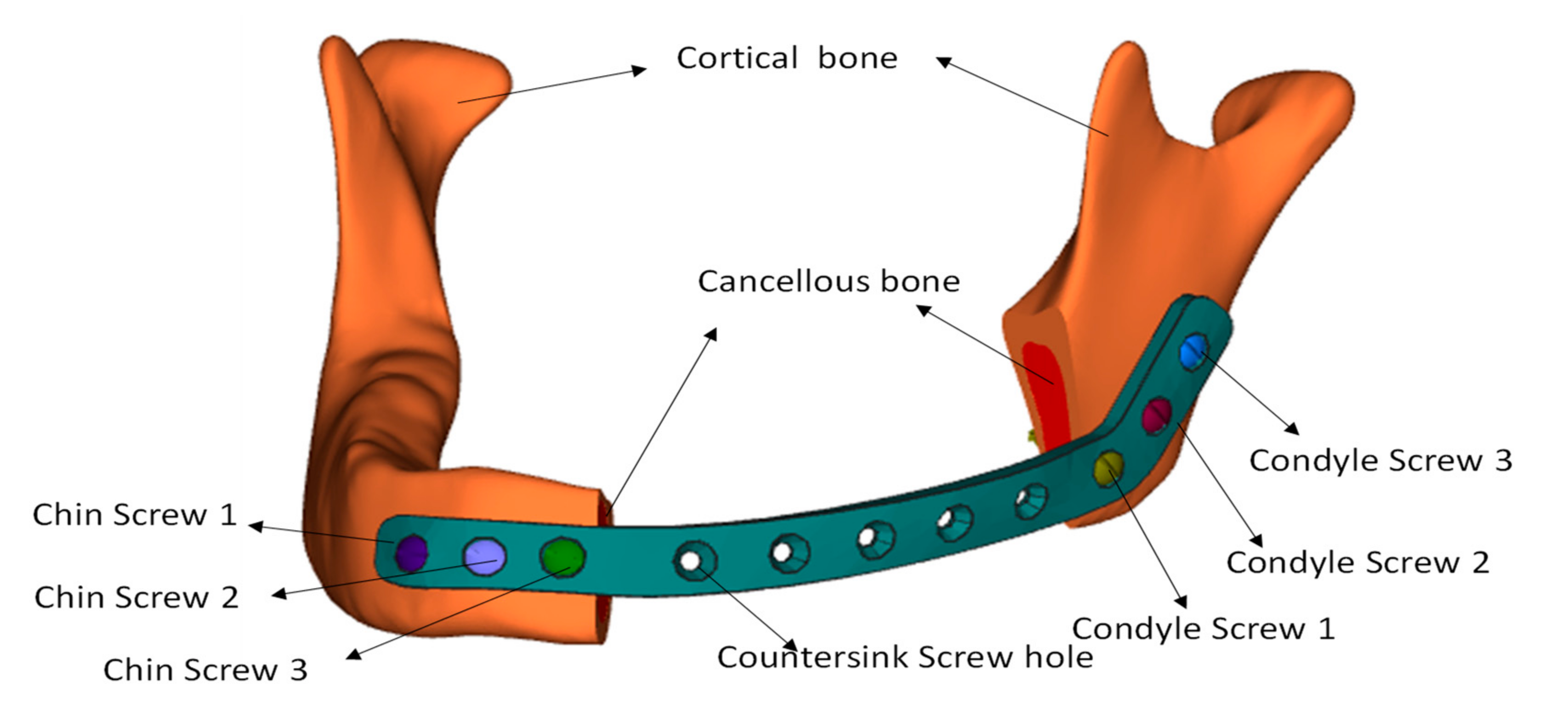
6]. The abnormality of mandibular continuity generally involves bone loss in density caused due to trauma related oral lesions, tumors, etc. Prompt and effective recovery of mandibular defects is important in order to avoid deterioration of masticatory operation, voice loss, cosmetic imperfection, and to effectively accomplish the patient’s welfare. It is therefore important to use specially made implants that not only minimize disparity and incompatibility, but also improve the appearance and actualization. The specific implant configuration not only promotes the reliability of the fitting but also mitigates the processing time as compared to generic plates.
Apparently, implementing tailor-mandibular architecture requires developers to fully recognize the advantages and inconveniences of the various designs. Hence, due to the differential output and increased cost of various designs, it is necessary to choose the most viable design for a particular task. As reported by Baker et al. [
7], it is only through a methodically formalized and well-defined philosophy that a worthwhile judgment (or selection) can be made. Certainly, multicriteria decision-making (MCDM) is one of those techniques and may be used to strengthen decision-making [
8,
9]. It is among the leading branches of operations research divisions comprising a set of deterministic possibilities estimated by a series of decision attributes [
10]. During the last few decades, MCDM has noticed a plausible use [
11]. It has evolved to meet various applications in the modern world such as supply chain management, finance, healthcare, factory location, environmental impact study, production, engineering, etc. [
12]. This paper, therefore, applies the MCDM approach and analyzes its applicability in choosing the optimal design to achieve mandibular reconstruction. The adequate implant design is required so that the desired strength, stability, and surface area can be attained for better osseointegration. The accuracy is higher so that it suits precisely on the mandible and provides the optimal aesthetic. The reduced cost and manufacturing time make the design of the implant available to all patients. The implant design can be readily accessible when the design and manufacturing complexities are lesser. The lower weight increases both the patient’s comfort and exhaustion. Hence, it is necessary to select the optimal implant design that displays all the desired characteristics listed. The MCDM strategy is used to decide on an optimal option in the context of diverse and contradictory criteria. The goal of this analysis is to furnish medical and engineering professionals with basic information on the relevance of the implant design criteria to be implemented, that will ultimately lead to better decision-making and improved implant performance.
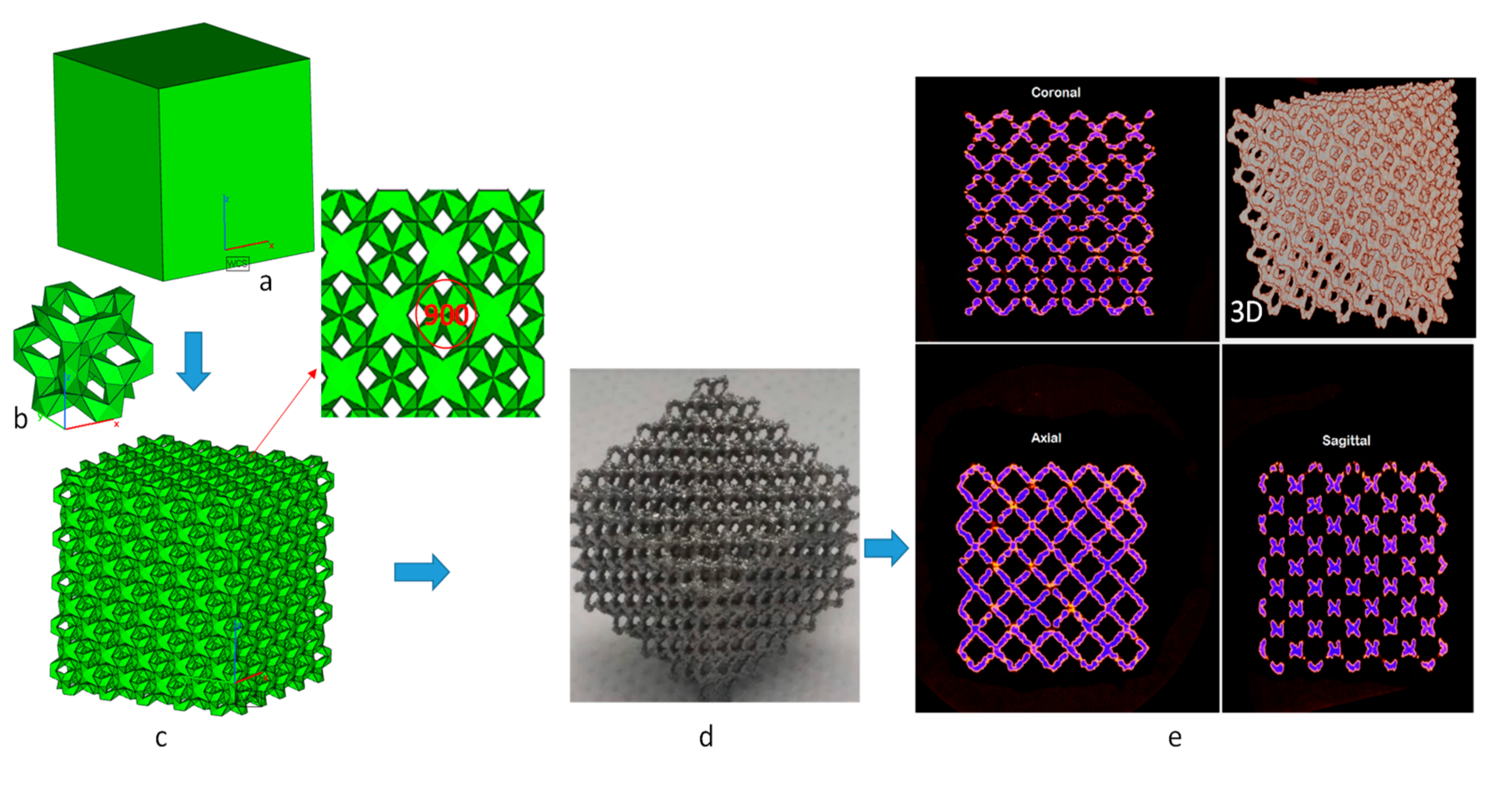
In the current implant industry, it is a standard practice that the design is chosen based on one or two criteria, overlooking the other variables. It is true that one design may be selected to satisfy specific requirements, but it may likely be possible that this design option does not perform well with other requirements. For example, among the four designs considered in this work, the analysis time, fabrication time, design, and manufacturing complexities for Design 1 are the lowest, but its stability is also the lowest. Similarly, if Design 3 is selected for some technological reasons, it provides very good stability, but the design complexity is very high. This study is carried out in such a way that most of the requirements are met by the one chosen implant design. For this purpose, all the criteria that are relevant to implant performance are identified. The possible criteria for implant design are established from the literature as well as by consultation with experts who provide opinions based on their expertise and experience. Based on the expert’s rating, the importance of each criterion in terms of weights is estimated. The collective decision-making (group of experts) approach is followed in this work to remove any bias in the decision model. The optimized implant design can then be selected from the available set of designs that can meet all the requirements or criteria. This research study takes into account four commonly used designs. Solid plate, sinewave, porous (top and bottom), and porous (inner) are the four designs. The list of criteria included Strength, Stability, Accuracy, Surface Area, Weight, Cost, Fabrication time, Design complexity, Manufacturing Complexity, Finite Element Modeling (FEM) analysis time, etc.
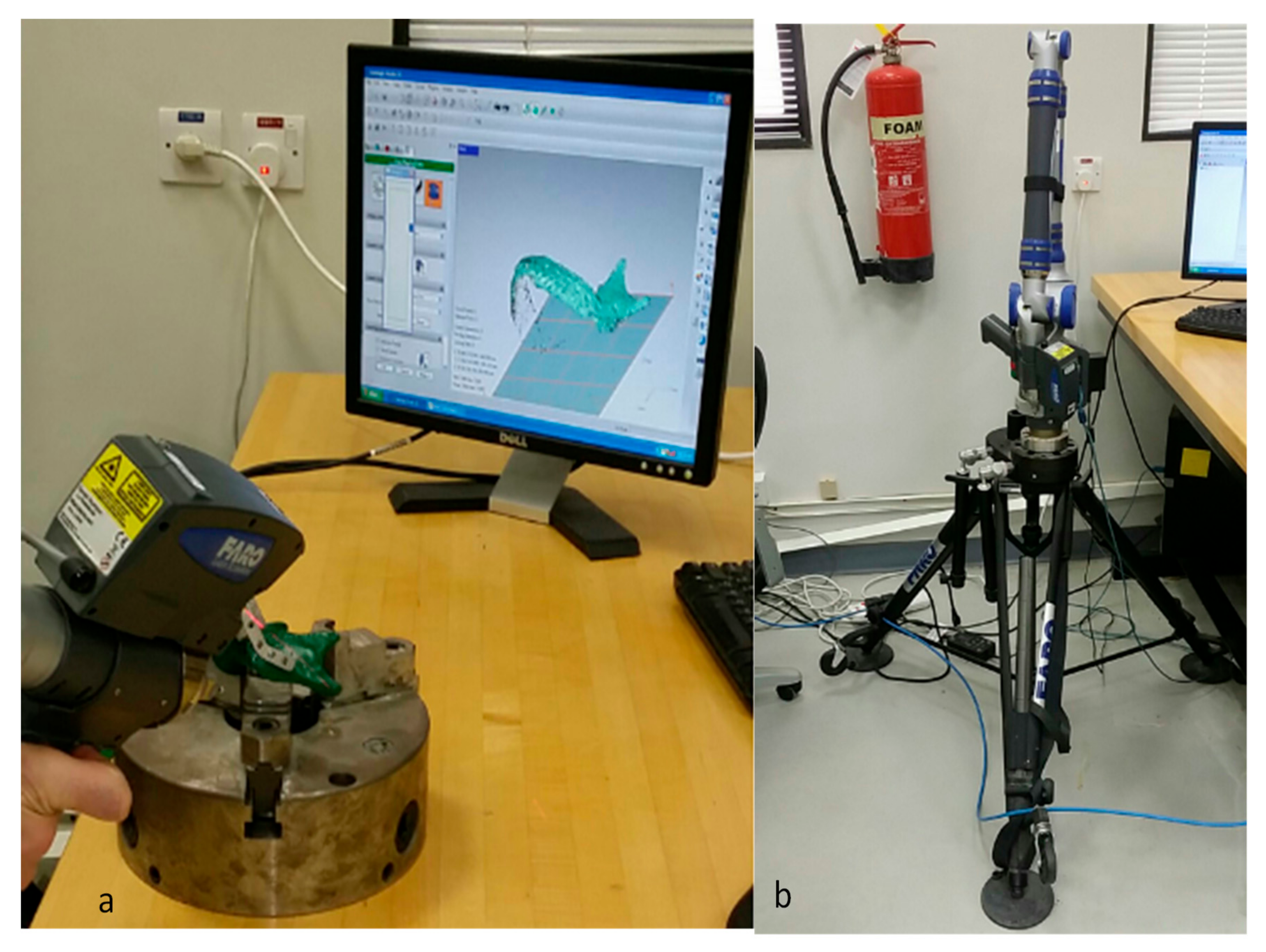
There are multiple criteria to evaluate the implant designs, so it can be described as an MCDM problem. It has many inputs, including qualitative and quantitative criteria, their values, opinions of experts, etc. The higher the precision of the different MCDM inputs, the better and more reliable the solution would be. There is, of course, a subjective element in the acquisition of opinions, and there is often a degree of ambiguity in data acquisition. For example, one of the criteria, stability, is evaluated by implementing a nondestructive scan-based micro-computed tomography (CT) technique. There are, however, many known and unknown variables that exist during micro-CT scans, and all of them cannot be considered during scanning. So, in the final result, there is always some degree of uncertainty. Hence, uncertainty and doubt in opinions and criteria assessment would have an impact on the quality of the results acquired. As a consequence, the method of Fuzzy Analytic Hierarchy Process (FAHP) has been adopted in this study to deal with incomplete, imprecise, and uncertain details ([
13,
14,
15]). FAHP’s advantages are its ease of use and its willingness to recognize subjectivity, uncertainty, and inconsistency in individual decisions or weight estimation [
16]. The two MCDM methods are used for grading various designs in order to ascertain the results derived from each other. The different fabricated designs are therefore evaluated using both FAHP-Techniques for Order of Preference by Similarity to Ideal Solution (TOPSIS) and FAHP-VlseKriterijumska Optimizacija I Kompromisno Resenje (VIKOR) to attain the optimum design.
The remainder of this paper is structured as below. The literature review is addressed in the accompanying
Section 2.
Section 3 and
Section 4 describe the MCDM approaches and illustrate experimentation respectively.
Section 5 define diverse criteria and analyze them by applying FAHP. The
Section 6 describes the usage of TOPSIS and VIKOR in optimum design selection and
Section 7 illustrates the conclusion part and future research work.
2. Literature Survey
Typically, regular commercial reconstruction plates (implants) are utilized in maxillofacial surgeries. Such plates are produced utilizing conventional techniques, like casting and metallurgical methods, that are often time-intensive procedures [
17]. The standard plates are particularly straight and have to be bent to fit them around the contoured jaw bone. It not only increases the time of operation (or treatment) but also includes the painstaking process of constantly evolving and tweaking the plate depending on the patient’s physiology. As it is a random and rigorous practice, the likelihood of inconsistencies between the bone and plate interface accentuates, leading to implant malfunction and patient distress. It is therefore important to use personalized implants that not only mitigate the discrepancy and incompatibility, but also improve the look and the precision of the implants. The individualized implant design not only facilitates the accuracy of the fitting but also lessens the operative time as opposed to regular plates.
With innovations in technology, such as biomedical simulation software and three-dimensional (3D) printing or additive manufacturing, custom implants can now be more precisely designed and produced in a shorter time frame. The integration of data capture, imaging, design, and additive production has enabled the development of tailor-made implants depending on the patient’s current needs. The enactment of embedded technologies will undeniably save significant amounts of money for medical professionals and completely overhaul the living conditions of a significant number of people [
18]. The satisfying impact of mandible reconstruction is heavily dependent on several implant dimensions including design manufacturing technology, biomechanical effects, precision, surface quality, and weight. There is no escaping the fact that 3D printing techniques offer exciting possibilities for bone reconstruction, regeneration, and surgery [
19]. Electron beam melting (EBM) technology is a well-known process in the production of medical implants and devices and has received the European market approval (CE/Conformité Européene) and as well as food and drug administration approval (FDA) from United States [
20]. EBM system, popularized in 1997 by ARCAM AB, produces parts in a layer by layer mode by fusing metal powder [
21]. It can be satisfactorily used to build 3D titanium alloy scaffolds with sophisticated architecture for medical applications [
22].
Maxillofacial bone is more of a twisted structure than a normal and uniform one. Correspondingly, few studies have tried to tailor the prosthesis configuration for mandibular reconstruction [
23] and so little literature is available on maxillofacial scaffold analysis. Furthermore, there is no conclusive evidence and review concerning the choice of the correct mandibular prosthetic design. Numerous designs for mandibular reconstruction may be possible, such as a solid plate [
24], Sinewave design plate [
25], porous design [
26,
27], etc. The Solid plate is a common mandibular reconstruction plate matching the patient bone contours whereas the Sinewave plate is a new design plate that also matching the bone contours but in a sinewave design form. The porous design plates are scaffolds holding bone grafts. Preferably the scaffolds should be highly permeable, free of cracks, and biocompatible with tissue growth [
28]. The titanium scaffolds can accomplish lifelong bone stabilization and support entire bone-in-growth in contrast to solid (bulk) bone growth, as illustrated in numerous research studies [
29,
30]. Furthermore, solid titanium implants can give rise to bone resorption owing to variations in mechanical properties, which causes the stress shielding implications on the adjacent bone and inevitably contribute to implant failure [
31]. The exemplary porosity affects cell activity and the interconnected pores channels promote cell growth and rapid vascularization [
32]. Promoting quick osseointegration is extremely important for successful implantation, otherwise longer cure time will result in implant malfunction [
33]. Due to the uniqueness of different designs, it is important to choose the most appropriate design, and that is only possible through proper selection techniques, such as MCDM. MCDM provides an important decision-making mechanism that can be used in a variety of fields, in which finding the best option is incredibly complicated [
34]. The literature seldom mentions research relating to the choice of custom mandible designs using MCDM. However, considerable work can be found in other domains where MCDM can be listed on the basis of either a single technique or its hybrid. Sadeghzadeh and Salehi, for example, applied the MCDM method in the automobile industry [
35]. They researched multiple regulations for strategic fuel cell technologies and implemented TOPSIS to classify primary approaches for fuel cell technology advancement. Similarly, Ozcan et al. [
36] suggested the principle of Analytic Hierarchy Process (AHP), TOPSIS, ELECTRE, and Grey to choose the appropriate warehouse location, despite high unpredictability and a range of products. Li et al. [
37] conducted an assessment of coal mines to evaluate the non-risk working of mines. Weights for diverse criteria were estimated by exploiting the entropy technique, while TOPSIS was executed to assess coal mines depending on their safety situations. AHP is viewed as a widely used MCDM techniques [
38]. The AHP, for instance, was implemented to achieve optimal maintenance solutions for the interactive learning and fabric industries by H. Fazlollahtabar and Yousefpoor [
39] and Ilangkumaran and Kumanan [
40], respectively. Bentes et al. [
41] deployed a confluence of Balanced Scorecard (BSC) and AHP to improve the efficiency of the Brazilian telecom company. The BSC had been used to analyze varied performance measures and AHP was used to list the capabilities of the different operational divisions. With their inherent strengths and skills, there have been many approaches to MCDM. Consequently, they must be selected or implemented as required by the application. Pourjavad and Shirouyehzad [
42] undertook detailed research on the three MCDM approaches TOPSIS, ELECTRE, and VIKOR for use in assembly channels. They studied the efficiency of simultaneous production facilities in the mining industry and examined the efficacy of MCDM methods.
Various fuzzy and conventional decision-making approaches are also helping health care and medical decisions. Sobolev et al. [
43] proposed a computer-based simulation study in the analysis of surgical care delivery. Brailsford et al. [
44] applied an integrated patient behavior simulation for the evaluation of breast cancer. Bahraminasab and Jahan [
45] proposed a detailed VIKOR approach for the material choice in the femoral part of the entire knee replacements. Lee et al. [
46] presented a fuzzy cognitive map of an MCDM approach in the acceptance of dental implant abutments. Cosma et al. [
47] presented a computational intelligence approach, which included metaheuristic optimization algorithms for the prediction of prostate cancer and addressed its challenges. Baccour [
48] proposed a novel integrated TOPSIS and VIKOR method for the categorization of heart diseases. Aenishaenslin et al. [
49] presented a Preference Ranking Organization Method for Enrichment of Evaluations (PROMETHEE) MCDM approach to study Lyme diseases. Venhorst et al. [
50] introduced a tool established on the nominal group technique and Delphi method for breast cancer interventions. Martinez et al. [
51] employed the symmetrical triangular fuzzy approach to identify the titanium implant surface areas which influenced the implant performance. An expert-based questionnaire survey was performed to identify various implant properties on the biological, physicochemical, and mechanical performance. Nazari et al. [
52] accomplished a clinical decision support advisor depending on a fuzzy interference system and FAHP to evaluate the patient’s condition and its diagnosis for heart diseases. Obanijesu and emuyibofarhe justice [
53] designed a neuro-fuzzy system with eight inputs and one output for the detection of heart attacks. Banerjee et al. [
54] recommended a unique combinatorial technique using fuzzy logic-based neural network models for the prediction of mechanical properties in orthopedic implants. It is interesting to know that most of the studies did not address group decision-making, the imprecision of expert views, and the uncertainty of the acquired criteria data. It is very complicated to weigh and also preserve the continuity of judgment using existing approaches, particularly with added criteria. These techniques needed a great deal of information and were unable to cope with incomplete information or knowledge. They required consistent preferences of the experts as well as precise details for high-quality results. These techniques did not deal with an incomplete amount of data and presumed that all measurements of output and input were defined.
It is clear that earlier publications seldom discussed research on the selection of acceptable implant design in mandibular reconstruction. Most researchers have suggested their specific implant designs (based on one or two aspects) for mandibular reconstruction. They did not, however, compare different designs using a robust decision-making approach like MCDM. Moreover, the earlier researches concentrated on one or two aspects of the design. Some designs, for example, were good in terms of stability; some were good in terms of design complexity, etc. The numerous criteria that may be very critical in the overall performance of the implant were overlooked in these studies. In order to create a better solution, a decision problem that includes a large number of criteria is especially useful. This research is therefore inspired by the need to resolve the constraint of fewer criteria when evaluating various designs. It is also evident from the literature that analysis on the application of MCDM in the selection of an effective design for mandibular reconstruction is rarely discussed. Thus, the need to demonstrate the successful application of MCDM in the implant industry also motivates this study.
Developing a cost-effective and differentiating custom mandibular design can be defined as a problem of optimization. It is because the selection of an optimal design can be affected by many factors. The presence of a wide variety of alternative design concepts therefore renders the selection process a complicated and nuanced activity [
55]. A systematic approach is therefore required to assess a vast array of designs and recognize the most appropriate one. The combined use of multiple strategies is beneficial to prevent drawbacks and to take advantage of individual methods. The AHP is augmented with soft computing techniques such as fuzzy sets (FAHP) [
56,
57] and combined with TOPSIS/VIKOR approaches in this work to overcome the limitations of earlier initiatives. This approach is very beneficial since it can solve the problems of decision-making in an arbitrary and unpredictable setting and needs a minimal level of knowledge on criteria. The following sections demonstrate the application of MCDM methods when selecting an optimal design for mandibular reconstruction.
5. Criteria of Different Designs
The criteria can be classified either as benefits or as cost criteria. The benefit criteria can be defined as those requirements which demand higher values, i.e., they exhibit a positive impact on performance. For example, strength, stability, and surface area are criteria of benefit in this research. Likewise, cost criteria have a negative influence, which is that the performance deteriorates if its values rise. The FEM analysis time, average deviation (accuracy), weight, cost, fabrication time, design complexity, and manufacturing complexity can be classified as cost criteria. The cost of the implant (in dollars, including the cost of the materials, software setup, etc.) was estimated by the cost model. The stability, accuracy, and weight were determined through micro-CT scan, 3D comparison, and weight measurement as discussed in the previous section. The strength and analysis time were computed using FEA simulation, while the surface area was estimated through software calculation. The design complexity and manufacturing complexity depended on the literature surveys, user experience, number of parameters involved, etc. They define the ease of design of the implant. The different criteria and their respective values may be outlined in
Table 5.
The different levels of the intangible criteria, namely, stability, design complexity, and manufacturing complexity were assured depending on knowledge and experimentation. The intangible criteria are regarded as criteria that are not measurable on a well-defined scale. As shown in
Table 6, the levels were thus defined using the scale for intangibles.
Table 7 outlines the various criteria that were established using experiments, software calculation, and expert opinions. The values of intangible requirements are also displayed in this table.
There were 4 experts whose experience and expertise were applied to decide and weigh different criteria necessary to choose an optimal design. A decision matrix depending on expert opinions was accomplished utilizing Saaty’s intensity scale as illustrated in
Table 8. The group of diverse experts (4 experts) assessed the criteria in this work because a single expert provides limited expertise and experience. The weights from the individual experts were aggregated to get combined weight. The goal of this approach was to find an ideal expert with the highest degree of decision consistency, the most accurate assessment, and whose evaluation was aligned with those of the other experts in the group. This method of group criteria weights guaranteed that the relevance of the criteria and therefore the final chosen implant design met the specifications from the point of view of experts.
The decision matrices for 4 experts were obtained as the outcome of this phase. The data collected from various experts were validated to conform their consistency prior to further processing [
99]. In order to analyze the reliability of decisions, Saaty [
98] introduced a random consistency index (
RI) depicted in
Table 9. The consistency ratio,
CR that correlates the consistency index (
CI) with the
RI must be described as below.
The λmax specifies the decision matrix’s maximum eigenvalue and n denotes the count of attributes. If CR is less than or equal to 10%, the discrepancy is permissible, otherwise expert must amend their decision matrix.
6. Selection of Design
The potential benefit of choosing the optimal design had to do specifically with patient satisfaction. The choice of the best design for the given application drives the patient’s level of satisfaction. Random design selection can lead to a higher cost-benefit ratio. A combination of various MCDM methods was applied to get the optimal design. The systematic procedure pursued to accomplish the desired implant design is outlined in
Figure 12.
To calculate the weights of different criteria, a group of four experts graded different criteria on a scale of 1 to 10, with 1 being the lowest priority and 10 being the utmost priority.
Table 10 presents the ranking results thus recorded.
The goal behind several experts was to combine more than one professional’s opinions to remove any prejudice. The decisions of the consultants were converted into decision matrices as shown in
Table 11 to examine anomalies in the judgments of experts and to calculate their weights.
For each expert, the
CR was determined to conform whether their decision was appropriate or not. The inconsistency was satisfactory because
CR in each case was less than 10%, as described in
Table 12.
Determination of Weights Using FAHP
The crisp values compiled in each decision matrix were translated into TrFNs. The TrFNs for various intensities of importance are depicted in
Table 13.
Chang’s extent analysis was used to measure the weights for individual experts after translation into TrFNs. The decision matrix by Expert 1 was utilized as an illustration in this computation. The primary stage was to generate a fuzzy pairwise matrix, as depicted in
Table 14.
Consequently, the synthetic fuzzy values were computed using Equations (1)–(4).
S1 = (20.50, 23.07, 28.30, 31) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S2 = (35, 39, 47, 51) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S3 = (5.89,6.97, 9.22, 10.40) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S4 = (35, 39, 47, 51) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S5 = (3.75, 4.01, 4.98, 6.08) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S6 = (20.50, 23.07, 28.30, 31) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S7 = (20.50, 23.07, 28.30, 31) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S8 = (5.89, 6.97, 9.22, 10.40) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S9 = (5.89, 6.97, 9.22, 10.40) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
S10 = (3.75, 4.01, 4.98, 6.08) ⊗ (1/238.365, 1/216.516, 1/176.162, 1/56.658)
These fuzzy values were then analyzed utilizing Equation (5).
The weights for various criteria can be calculated by employing Equation (6).
d′(C1) = min (0.9435, 1, 0.9435, 1, 1, 1, 1, 1, 1) = 0.9435
d′(C2) = min (1, 1, 1, 1, 1, 1, 1, 1) = 1
d′(C3) = min (0.6442, 0.4007, 0.4007, 1, 0.6442, 0.6442, 1, 1, 1) = 0.4007
d′(C4) = min (1, 1, 1, 1, 1, 1, 1, 1) = 1
d′(C5) = min (0.3726, 0.1820, 0.9375, 0.1820, 0.3726, 0.3726, 0.9375, 0.9375, 1) = 0.1820
d′(C6) = min (1, 0.9435, 1, 0.9435, 1, 1, 1, 1, 1) = 0.9435
d′(C7) = min (1, 0.9435, 1, 0.9435, 1, 1, 1, 1, 1) = 0.9435
d′(C8) = min (0.6442, 0.4007, 1, 0.4007, 1, 0.6442, 0.6442, 1, 1) = 0.4007
d′(C9) = min (0.6442, 0.4007, 1, 0.4007, 1, 0.6442, 0.6442, 1, 1) = 0.4007
d′(C10) = min (0.3726, 0.1820, 0.9375, 0.1820, 1, 0.3726, 0.3726, 0.9375, 0.9375) = 0.1820
The weight vector can now be denoted as below.
w′ = (0.9435, 1, 0.4007, 1, 0.1820, 0.9435, 0.9435, 0.4007, 0.4007, 0.1820)
Upon normalization, the weight vector can be interpreted as
w = (0.1475, 0.1563, 0.0626, 0.1563, 0.0285, 0.1475, 0.1475, 0.0626, 0.0626, 0.0285)
Correspondingly, the remainder weights for other judgment matrices were estimated. The individual weights, as shown in
Table 15, were also accumulated and normalized utilizing the geometric mean (GM) procedure.
The TOPSIS and VIKOR methods were practiced to find the optimal design when the weights were ascertained. The implementation of TOPSIS began with data normalization to obtain the weighted normalized decision matrix by exploiting Equations (9) and (10). The weighted normalized decision matrix for Expert 1 is presented in
Table 16.
Subsequently, the PIS as well as negative ideal solution NIS were estimated using Equation (11).
PIS = {0.1012, 0.1099, 0.0137, 0.0683, 0.0221, 0.0562, 0.0563, 0.0213, 0.0068, 0.0117}; NIS = {0.0474, 0.0366, 0.0426, 0.0898, 0.0053, 0.0987, 0.0987, 0.0429, 0.0478, 0.0164}
Finally, the relative closeness to the ideal solution (
Table 17) was estimated for different designs using Equations (12) and (13).
Design 3, which was a porous top and bottom plate had the highest
θi among four different designs and was therefore identified as the optimal design. Thus, the three designs can be classified as follows.
The VIKOR-based MCDM approach also started with a definition of the normalized decision matrix, as seen in
Table 18.
Eventually, the best values (
vj+) were established for each criterion in the normalized decision matrix, which can be seen in
Table 19. The
Si,
Ri, and
Qi values computed for different variants can be seen in
Table 20.
According to the VIKOR ranking method also, the porous top and bottom plate “Design 3” was ranked the best, followed by Design 1, Design 2, and Design 4. A compromise solution was implemented in VIKOR so two conditions were verified as discussed in
Section 3.3 above.
As Q (Design 1) − Q (Design 3) = 0.5115 and DQ = 0.3333, the condition 1 (acceptable advantage) was met. Therefore, it was possible to differentiate the best one between Design 3 and Design 1. Moreover, the option best ranked according to Q values had also been best ranked by R and S. Thus, it satisfied both the acceptability criterion. It suggested that condition 2 was also satisfied. Finally, Design 3 was recommended as the best configuration, based on the VIKOR method.
Based on the analysis using FAHP and TOPSIS as well as FAHP and VIKOR, Design 3 was the most appropriate design. The integrated solution focused on FAHP and TOPSIS, as well as FAHP and VIKOR, has provided similar outcomes. Design 3 (porous top and bottom plate) was the optimal design because it satisfied the combined requirements of stability, accuracy, strength, and cost. In addition, porous implants provided less stress shielding effect compared to solid plates and certainly resulted in faster healing times. Moreover, the Design 3 (top and bottom) porous implant showed increased stability and excellent accuracy compared to the Design 4 (inner porous). It also had good mechanical strength, greater surface area, relatively lower cost, low weight, and manufacturing time. The manufacturing complexity of Design 3 was also not very high.
The sensitivity analysis (
Table 21) indicated that the ranking order produced through the applied integrated approach was stable and reliable. It can be justified by the argument that the value
W for each expert was near to 1. The ranking order accomplished for ten scenarios in each scheme and original ranking order were investigated for their similarities to estimate the values of
W. The higher
W values implied that the ranking order obtained in this study was accurate and insensitive to weight fluctuations.
7. Conclusions
This work provided an application method for analyzing the various implant designs and choosing the most suitable one. This approach was based on the assessment of four different designs, namely solid plate, sinewave, porous (top and bottom), and porous (inner) that are presently extensively used. The performance evaluation included the investigation of the various attributes of different designs. The specifications acquired from the experts were used in MCDM to select a viable and sustainable design. In this work, the decision-making process based on FAHP and TOPSIS as well as FAHP and VIKOR were used to methodologically choose the optimal implant design. Such methods are capable of understanding the complexity of human thought and of expertly addressing MCDM problems. These strategies have the strength and the ability to solve any incoherence and ambiguity with an increase in criteria. Obviously, the decisions made by the established selection techniques were effective and fulfilled all their requirements appropriately. This work is notable because of its different implant designs, the recognition of their advantages and disadvantages, the deployment of TrFNs in extent analysis technique (FAHP), the transformation of crisp values into TrFNs, and the use of TOPSIS and VIKOR to rank various variants. This approach is accessible and can produce reasonable, proficient, and feasible results due to its unique characteristics.
The results were estimated in view of the potential ambiguity in decision making and the uncertainty in criteria assessment. Moreover, sensitivity analysis ensured that the weights and rankings were consistent and efficient in this work. The use of FAHP weights in addition to TOPSIS and the VIKOR rankings makes the selection process more adaptable, accurate, and practical. This model is particularly valuable in implant design selection or other analogous situations, in which the level of indecision is supposed to differ owing to the vibrant and demanding market together with capricious consumer needs. Conversely, with a rise in the number of criteria and varying designs, this selection strategy might become repetitive, computationally demanding, and tedious. Moreover, because the effectiveness of this decision-making strategy relies on expert assessments, the ranking process may also appear to be overestimated. Indeed, a comprehensive investigation of the reliability of the fuzzy pairwise comparison matrix with TrFNs is needed in the years ahead. Since the fundamental issue of implant design selection has not been handled proactively due to its dynamic nature, this research aims to help designers or physicians choose the most suitable design. In addition to the example provided in this work, the applied techniques can also be used for other application domains, like strategy formulation, product development, project assessment, evaluation of suppliers, hospitality sector, infrastructure services, etc. Such work will eventually allow manufacturers and industrial firms to choose the most feasible implant design. Due to the ever-evolving implant sector and changing consumer preferences, the repository has to be revised regularly with new designs and requirements. For this purpose, more requirements and varying designs will be explored in future work to establish a more reliable design selection system.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}