
Alzheimer’s Disease Prediction Using Deep Feature Extraction and Optimization

Abstract
:1. Introduction
- Transfer learning is employed on VGG19 with fine-tuned hyperparameters for deep feature extraction from the fc7 and fc8 layers.
- The process of feature concatenation is performed to create a unified feature space by considering the highest value.
- Redundancy in the features is eliminated using an updated version of the WoA with optimal settings.
2. Related Work
3. Materials and Methods
3.1. Dataset
3.2. Deep Feature Extraction
3.3. Feature Concatenation
| Algorithm 1: Pseudo code of feature concatenation |
| Normalize () Normalize () if length () < length (): Extend to match the length of else: Extend to match the length of = empty_vector of length () used_features = empty_set for i from 0 to length () − 1: weighted__value = * [i] weighted__value = * [i] if weighted__value > weighted__value and [i] no longer in used_features: [i] = [i] else if weighted_Y_2_value >= weighted__value and [i] no longer in used_features: [i] = [i] else: [i] = some_fallback_logic () used_features.Upload ([i]) |
3.4. Feature Optimization
Whale Optimization Algorithm
| Algorithm 2: Pseudo code of the whale optimization algorithm |
| Pseudocode of whale optimization algorithm Step 1: Initialization (Whale population) where Step 2: The computation of fitness for every solution. best search agent Step 3: While For every solution Updated and If1 If2 Revise the present location of the search agent by Equation (1). Else if2 The process of selecting a random search agent. The location of the search agent is subject to modification based on Equation (7). End if2 Else if1 The location of the search agent is subject to modification by Equation (5). End if1 End for Examine the trajectory of a search agent if it deviates from its designated search location and alters its course. Change if the better solution is presented End While Step 4: Return |
4. Results
4.1. AD Prediction Results of Features Extracted from fc7
4.2. AD Prediction Results of Features Extracted from fc8
4.3. AD Prediction Results of Feature Fusion Extracted from fc7 and fc8
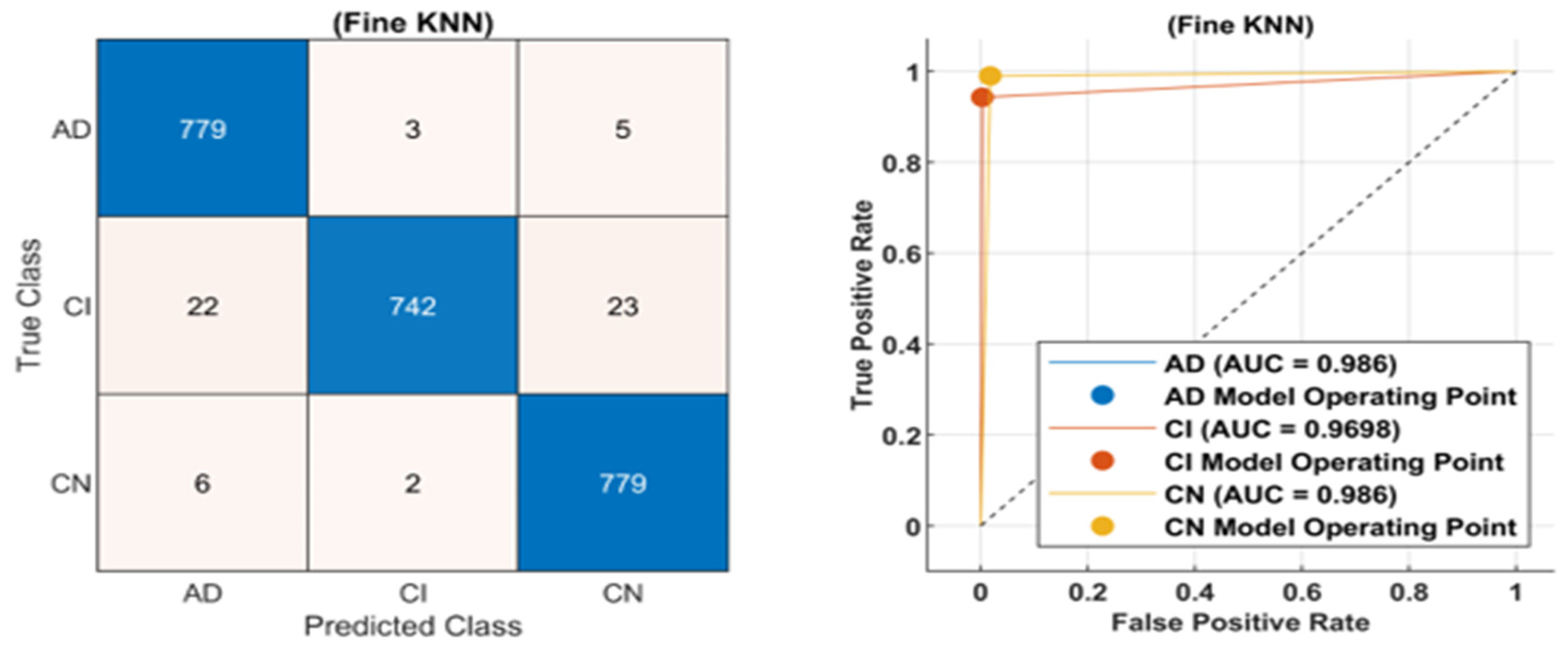
4.4. AD Prediction Results of Feature Optimization
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Marwa, E.-G.; Moustafa, H.E.-D.; Khalifa, F.; Khater, H.; AbdElhalim, E. An MRI-based deep learning approach for accurate detection of Alzheimer’s disease. Alex. Eng. J. 2023, 63, 211–221. [Google Scholar]
- DeTure, M.A.; Dickson, D.W. The neuropathological diagnosis of Alzheimer’s disease. Mol. Neurodegener. 2019, 14, 1–18. [Google Scholar]
- Chen, H.; Qiao, H.; Zhu, F.; Chen, L. Alzheimer’s Disease Clinical Scores Prediction based on the Label Distribution Learning using Brain Structural MRI. In Proceedings of the 2022 International Joint Conference on Neural Networks (IJCNN), Padua, Italy, 18–23 July 2022; pp. 1–8. [Google Scholar]
- Lu, B.; Li, H.-X.; Chang, Z.-K.; Li, L.; Chen, N.-X.; Zhu, Z.-C.; Zhou, H.-X.; Li, X.-Y.; Wang, Y.-W.; Cui, S.-X. A practical Alzheimer’s disease classifier via brain imaging-based deep learning on 85,721 samples. J. Big Data 2022, 9, 1–22. [Google Scholar]
- Sudar, K.M.; Nagaraj, P.; Nithisaa, S.; Aishwarya, R.; Aakash, M.; Lakshmi, S.I. Alzheimer’s Disease Analysis using Explainable Artificial Intelligence (XAI). In Proceedings of the 2022 International Conference on Sustainable Computing and Data Communication Systems (ICSCDS), Erode, India, 7–9 April 2022; pp. 419–423. [Google Scholar]
- Liu, S.; Masurkar, A.V.; Rusinek, H.; Chen, J.; Zhang, B.; Zhu, W.; Fernandez-Granda, C.; Razavian, N. Generalizable deep learning model for early Alzheimer’s disease detection from structural MRIs. Sci. Rep. 2022, 12, 17106. [Google Scholar] [PubMed]
- Nguyen, D.; Nguyen, H.; Ong, H.; Le, H.; Ha, H.; Duc, N.T.; Ngo, H.T. Ensemble learning using traditional machine learning and deep neural network for diagnosis of Alzheimer’s disease. IBRO Neurosci. Rep. 2022, 13, 255–263. [Google Scholar] [PubMed]
- Payton, E.; Khubchandani, J.; Thompson, A.; Price, J.H. Parents’ expectations of high schools in firearm violence prevention. J. Community Health 2017, 42, 1118–1126. [Google Scholar]
- Ullah, Z.; Jamjoom, M. A Deep Learning for Alzheimer’s Stages Detection Using Brain Images. Comput. Mater. Contin. 2023, 74, 1457–1473. [Google Scholar] [CrossRef]
- Thangavel, P.; Natarajan, Y.; Preethaa, K.S. EAD-DNN: Early Alzheimer’s disease prediction using deep neural networks. Biomed. Signal Process. Control 2023, 86, 105215. [Google Scholar] [CrossRef]
- Khatri, U.; Kwon, G.-R. Alzheimer’s disease diagnosis and biomarker analysis using resting-state functional MRI functional brain network with multi-measures features and hippocampal subfield and amygdala volume of structural MRI. Front. Aging Neurosci. 2022, 14, 818871. [Google Scholar]
- Aaraji, Z.S.; Abbas, H.H. Automatic Classification of Alzheimer’s disease using brain MRI data and deep Convolutional Neural Networks. arXiv 2022, arXiv:2204.00068. [Google Scholar]
- Faisal, F.U.R.; Kwon, G.-R. Automated detection of Alzheimer’s disease and mild cognitive impairment using whole brain MRI. IEEE Access 2022, 10, 65055–65066. [Google Scholar] [CrossRef]
- Minne, P.; Fernandez-Quilez, A.; Aarsland, D.; Ferreira, D.; Westman, E.; Lemstra, A.W.; Ten Kate, M.; Padovani, A.; Rektorova, I.; Bonanni, L. A study on 3D classical versus GAN-based augmentation for MRI brain image to predict the diagnosis of dementia with Lewy bodies and Alzheimer’s disease in a European multi-center study. In Medical Imaging 2022: Computer-Aided Diagnosis; SPIE: Bellingham, WA, USA, 2022; pp. 624–632. [Google Scholar]
- Zhao, Z.; Chuah, J.H.; Lai, K.W.; Chow, C.-O.; Gochoo, M.; Dhanalakshmi, S.; Wang, N.; Bao, W.; Wu, X. Conventional machine learning and deep learning in Alzheimer’s disease diagnosis using neuroimaging: A review. Front. Comput. Neurosci. 2023, 17, 1038636. [Google Scholar] [CrossRef] [PubMed]
- Orouskhani, M.; Zhu, C.; Rostamian, S.; Zadeh, F.S.; Shafiei, M.; Orouskhani, Y. Alzheimer’s disease detection from structural MRI using conditional deep triplet network. Neurosci. Inform. 2022, 2, 100066. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, Z.; Jin, Y.; Hou, W. VGG-TSwinformer: Transformer-based deep learning model for early Alzheimer’s disease prediction. Comput. Methods Programs Biomed. 2023, 229, 107291. [Google Scholar] [CrossRef] [PubMed]
- Sudharsan, M.; Thailambal, G. An Recognition of Alzheimer Disease using Brain MRI Images with DPNMM through Adaptive Model. In Proceedings of the 2022 International Conference on Edge Computing and Applications (ICECAA), Tamilnadu, India, 13–15 October 2022; pp. 952–959. [Google Scholar]
- Dhinagar, N.J.; Thomopoulos, S.I.; Rajagopalan, P.; Stripelis, D.; Ambite, J.L.; Ver Steeg, G.; Thompson, P.M. Evaluation of transfer learning methods for detecting Alzheimer’s disease with brain MRI. In Proceedings of the 18th International Symposium on Medical Information Processing and Analysis, Valparaiso, Chile, 9–11 November 2022; pp. 504–513. [Google Scholar]
- Kolides, A.; Nawaz, A.; Rathor, A.; Beeman, D.; Hashmi, M.; Fatima, S.; Berdik, D.; Al-Ayyoub, M.; Jararweh, Y. Artificial intelligence foundation and pre-trained models: Fundamentals, applications, opportunities, and social impacts. Simul. Model. Pract. Theory 2023, 126, 102754. [Google Scholar] [CrossRef]
- Rao, K.N.; Gandhi, B.R.; Rao, M.V.; Javvadi, S.; Vellela, S.S.; Basha, S.K. Prediction and Classification of Alzheimer’s Disease using Machine Learning Techniques in 3D MR Images. In Proceedings of the 2023 International Conference on Sustainable Computing and Smart Systems (ICSCSS), Coimbatore, India, 14–16 June 2023; pp. 85–90. [Google Scholar]
- Marcus, D.S.; Fotenos, A.F.; Csernansky, J.G.; Morris, J.C.; Buckner, R.L. Open access series of imaging studies: Longitudinal MRI data in nondemented and demented older adults. J. Cogn. Neurosci. 2010, 22, 2677–2684. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 10–15 June 2019; pp. 6105–6114. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Chang, A.J.; Roth, R.; Bougioukli, E.; Ruber, T.; Keller, S.S.; Drane, D.L.; Gross, R.E.; Welsh, J.; Abrol, A.; Calhoun, V. MRI-based deep learning can discriminate between temporal lobe epilepsy, Alzheimer’s disease, and healthy controls. Commun. Med. 2023, 3, 33. [Google Scholar] [CrossRef]
- Shamrat, F.J.M.; Akter, S.; Azam, S.; Karim, A.; Ghosh, P.; Tasnim, Z.; Hasib, K.M.; De Boer, F.; Ahmed, K. AlzheimerNet: An effective deep learning based proposition for alzheimer’s disease stages classification from functional brain changes in magnetic resonance images. IEEE Access 2023, 11, 16376–16395. [Google Scholar] [CrossRef]
- Mao, C.; Xu, J.; Rasmussen, L.; Li, Y.; Adekkanattu, P.; Pacheco, J.; Bonakdarpour, B.; Vassar, R.; Shen, L.; Jiang, G. AD-BERT: Using Pre-trained Language Model to Predict the Progression from Mild Cognitive Impairment to Alzheimer’s Disease. J. Biomed. Inform. 2023, 144, 104442. [Google Scholar] [CrossRef]
- Rehman, A.; Saba, T.; Mujahid, M.; Alamri, F.S.; ElHakim, N. Parkinson’s Disease Detection Using Hybrid LSTM-GRU Deep Learning Model. Electronics 2023, 12, 2856. [Google Scholar] [CrossRef]
- Cheung, E.Y.; Shea, Y.; Chiu, P.K.; Kwan, J.S.; Mak, H.K. Diagnostic efficacy of voxel-mirrored homotopic connectivity in vascular dementia as compared to alzheimer’s related neurodegenerative diseases—A resting state fMRI study. Life 2021, 11, 1108. [Google Scholar] [CrossRef] [PubMed]
- Loddo, A.; Buttau, S.; Di Ruberto, C. Deep learning based pipelines for Alzheimer’s disease diagnosis: A comparative study and a novel deep-ensemble method. Comput. Biol. Med. 2022, 141, 105032. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Goel, T.; Tanveer, M.; Lin, C.; Murugan, R. Deep learning based diagnosis and prognosis of Alzheimer’s disease: A comprehensive review. IEEE Trans. Cogn. Dev. Syst. 2023. [Google Scholar] [CrossRef]
- ADNI|Alzheimer’s Disease Neuroimaging Initiative. 2022. Available online: https://adni.loni.usc.edu/ (accessed on 14 May 2023).
- ADNI Extracted Axial. Available online: https://www.kaggle.com/datasets/katalniraj/adni-extracted-axial (accessed on 14 May 2023).
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data 2021, 8, 1–74. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hussain, N.; Majid, A.; Alhaisoni, M.; Chan Bukhari, S.A.; Kadry, S.; Nam, Y.; Zhang, Y.-D. Classification of Positive COVID-19 CT Scans Using Deep Learning. Comput. Mater. Contin. 2021, 66, 2923–2938. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Fei-Fei, L. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Schmidt-Hieber, J. Nonparametric Regression Using Deep Neural Networks with ReLU Activation Function. arXiv 2020, arXiv:1708.06633. [Google Scholar]
- Mirjalili, S.; Lewis, A. The whale optimization algorithm. Adv. Eng. Softw. 2016, 95, 51–67. [Google Scholar] [CrossRef]
- Fix, E.; Hodges, J.L. Discriminatory analysis. Nonparametric discrimination: Consistency properties. Int. Stat. Rev./Rev. Int. De Stat. 1989, 57, 238–247. [Google Scholar] [CrossRef]
- Joachims, T. Making Large-Scale SVM Learning Practical; Technical Report; 1998. Available online: https://www.econstor.eu/handle/10419/77178 (accessed on 14 May 2023).
- Lu, D.; Popuri, K.; Ding, G.W.; Balachandar, R.; Beg, M.F. Multimodal and multiscale deep neural networks for the early diagnosis of Alzheimer’s disease using structural MR and FDG-PET images. Sci. Rep. 2018, 8, 5697. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Liu, Z.; Yan, W.Q.; Klette, R. Early diagnosis of Alzheimer’s disease using deep learning. In Proceedings of the 2nd International Conference on Control and Computer Vision, Marseille, France, 18–20 September 2019; pp. 87–91. [Google Scholar]
- Bringas, S.; Salomón, S.; Duque, R.; Lage, C.; Montaña, J.L. Alzheimer’s disease stage identification using deep learning models. J. Biomed. Inform. 2020, 109, 103514. [Google Scholar] [CrossRef]
- Kundaram, S.S.; Pathak, K.C. Deep learning-based Alzheimer disease detection. In Proceedings of the Fourth International Conference on Microelectronics, Computing and Communication Systems: MCCS 2019, Ranchi, India, 11–12 May 2021; pp. 587–597. [Google Scholar]
- Sisodia, P.S.; Ameta, G.K.; Kumar, Y.; Chaplot, N. A review of deep transfer learning approaches for class-wise prediction of Alzheimer’s disease using MRI images. Arch. Comput. Methods Eng. 2023, 30, 2409–2429. [Google Scholar] [CrossRef]
- Bangyal, W.H.; Rehman, N.U.; Nawaz, A.; Nisar, K.; Ibrahim, A.A.A.; Shakir, R.; Rawat, D.B. Constructing Domain Ontology for Alzheimer Disease Using Deep Learning Based Approach. Electronics 2022, 11, 1890. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Year | Dataset | Model | Accuracy |
|---|---|---|---|---|
| [6] | 2022 | MRI Brain Images | DL model | 96% |
| [7] | 2022 | MRI | Deep TL model | 93.52% |
| [10] | 2023 | MRI Images | DL-based radiomics | 93.50% |
| [18] | 2022 | MRI, PET | AD dataset | 94.61% |
| [19] | 2023 | MRI | Deep CNN | 89% |
| [20] | 2023 | Brain Dataset | AlexNet framework | 98.35% |
| [22] | 2023 | MRI | CNN | 98.67% |
| [23] | 2022 | MRI | ML | 94.64% |
| [24] | 2022 | MRI | DL and ML | 91.70% |
| [25] | 2022 | MRI | ML | 95.30% |
| [26] | 2022 | MRI | DL | 82.2% |
| Method | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) | FNR (%) | Time (s) |
|---|---|---|---|---|---|---|
| F-KNN | 97.3 | 95.4 | 96.8 | 96.1 | 2.7 | 900 |
| C-SVM | 96.4 | 93.1 | 95.6 | 94.3 | 3.6 | 712 |
| Q-SVM | 94.2 | 91.2 | 94.3 | 92.7 | 5.8 | 656 |
| MG-SVM | 91.8 | 92 | 91.6 | 91.6 | 8.2 | 989 |
| W-KNN | 92.3 | 92.3 | 92.6 | 92.3 | 7.7 | 1256 |
| ES-KNN | 97.1 | 97.3 | 96.3 | 96.3 | 2.9 | 1522 |
| ESD | 93.9 | 94 | 94 | 93.66 | 6.1 | 1823 |
| Classes | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) |
|---|---|---|---|---|
| AD | 98.31 | 98.31 | 98.31 | 98.31 |
| CI | 97.71 | 97.71 | 97.71 | 97.71 |
| CN | 98.56 | 98.56 | 98.56 | 98.56 |
| Method | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) | FNR (%) | Time (s) |
|---|---|---|---|---|---|---|
| F-KNN | 96.2 | 96 | 96 | 96.33 | 3.8 | 900 |
| C-SVM | 95.5 | 95.6 | 95.4 | 95.6 | 4.5 | 712 |
| Q-SVM | 91.7 | 91.6 | 92 | 92 | 8.3 | 809.35 |
| MG-SVM | 88.5 | 88.3 | 88.3 | 88.6 | 11.5 | 840.25 |
| W-KNN | 91.2 | 91.3 | 91.66 | 91 | 8.8 | 1182.7 |
| ES-KNN | 95.5 | 95.6 | 95.6 | 95.6 | 4.5 | 2167.9 |
| ESD | 88.4 | 88 | 88.6 | 88.33 | 11.6 | 18,446 |
| Classes | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) |
|---|---|---|---|---|
| AD | 98.09 | 98.09 | 98.09 | 98.09 |
| CI | 96.48 | 96.48 | 96.48 | 96.48 |
| CN | 97.88 | 97.88 | 97.88 | 97.88 |
| Method | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) | FNR (%) | Time (s) |
|---|---|---|---|---|---|---|
| F-KNN | 98 | 97 | 98.3 | 97.6 | 2 | 972 |
| C-SVM | 98 | 97.6 | 98.3 | 98 | 2 | 912.2 |
| Q-SVM | 96.4 | 96.3 | 96.3 | 96.3 | 3.6 | 879 |
| MG-SVM | 94.4 | 94.3 | 94.6 | 94.3 | 5.6 | 1420.5 |
| W-KNN | 92.4 | 92.3 | 92.6 | 92.3 | 7.6 | 1882.7 |
| ES-KNN | 97.5 | 97.3 | 97.3 | 97.6 | 2.5 | 2667.9 |
| ESD | 95.7 | 95.6 | 96 | 95.6 | 4.3 | 3752.2 |
| Classes | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) |
|---|---|---|---|---|
| AD | 98.64 | 98.64 | 98.64 | 98.64 |
| CI | 98.31 | 98.31 | 98.31 | 98.31 |
| CN | 98.98 | 98.98 | 98.98 | 98.98 |
| Method | Accuracy (%) | Precision (%) | Recall (%) | F1 Score (%) | FNR (%) | Time (s) |
|---|---|---|---|---|---|---|
| F-KNN | 99 | 99.6 | 99.6 | 99.6 | 1 | 12 |
| C-SVM | 97.5 | 98 | 98 | 98 | 2.5 | 39.15 |
| Q-SVM | 95.3 | 95.3 | 95.3 | 95 | 4.7 | 54.42 |
| MG-SVM | 94 | 94.3 | 94.3 | 94 | 6 | 61.52 |
| W-KNN | 92 | 92 | 92.3 | 91.66 | 8 | 65.35 |
| ES-KNN | 92.4 | 92.6 | 92.3 | 92.3 | 7.6 | 89.65 |
| ESD | 97.3 | 97.3 | 97.3 | 97 | 2.7 | 109.35 |
| Reference | Year | Method | Accuracy |
|---|---|---|---|
| [44] | 2018 | Deep CNN | 82.4% |
| [45] | 2019 | ConvNets | 97.65% |
| [46] | 2020 | Deep CNN | 91% |
| [47] | 2021 | Deep CNN | 98.57% |
| [7] | 2022 | Ensemble of ML and DL | 96% |
| [12] | 2022 | Segmentation and DL | 93.50% |
| [49] | 2022 | DL-based ontology | 94.61% |
| [48] | 2023 | Deep CNN | 93.52% |
| [28] | 2023 | DL-based Alzheimer Net | 98.67% |
| Proposed | DL and Feature Optimization | 99% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammad, F.; Al Ahmadi, S. Alzheimer’s Disease Prediction Using Deep Feature Extraction and Optimization. Mathematics 2023, 11, 3712. https://doi.org/10.3390/math11173712
Mohammad F, Al Ahmadi S. Alzheimer’s Disease Prediction Using Deep Feature Extraction and Optimization. Mathematics. 2023; 11(17):3712. https://doi.org/10.3390/math11173712
Chicago/Turabian StyleMohammad, Farah, and Saad Al Ahmadi. 2023. "Alzheimer’s Disease Prediction Using Deep Feature Extraction and Optimization" Mathematics 11, no. 17: 3712. https://doi.org/10.3390/math11173712