
Modelling the Upper Airways of Mandibular Advancement Surgery: A Systematic Review
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Review Outcome Introduction
2.1. Airways Imaging Technique
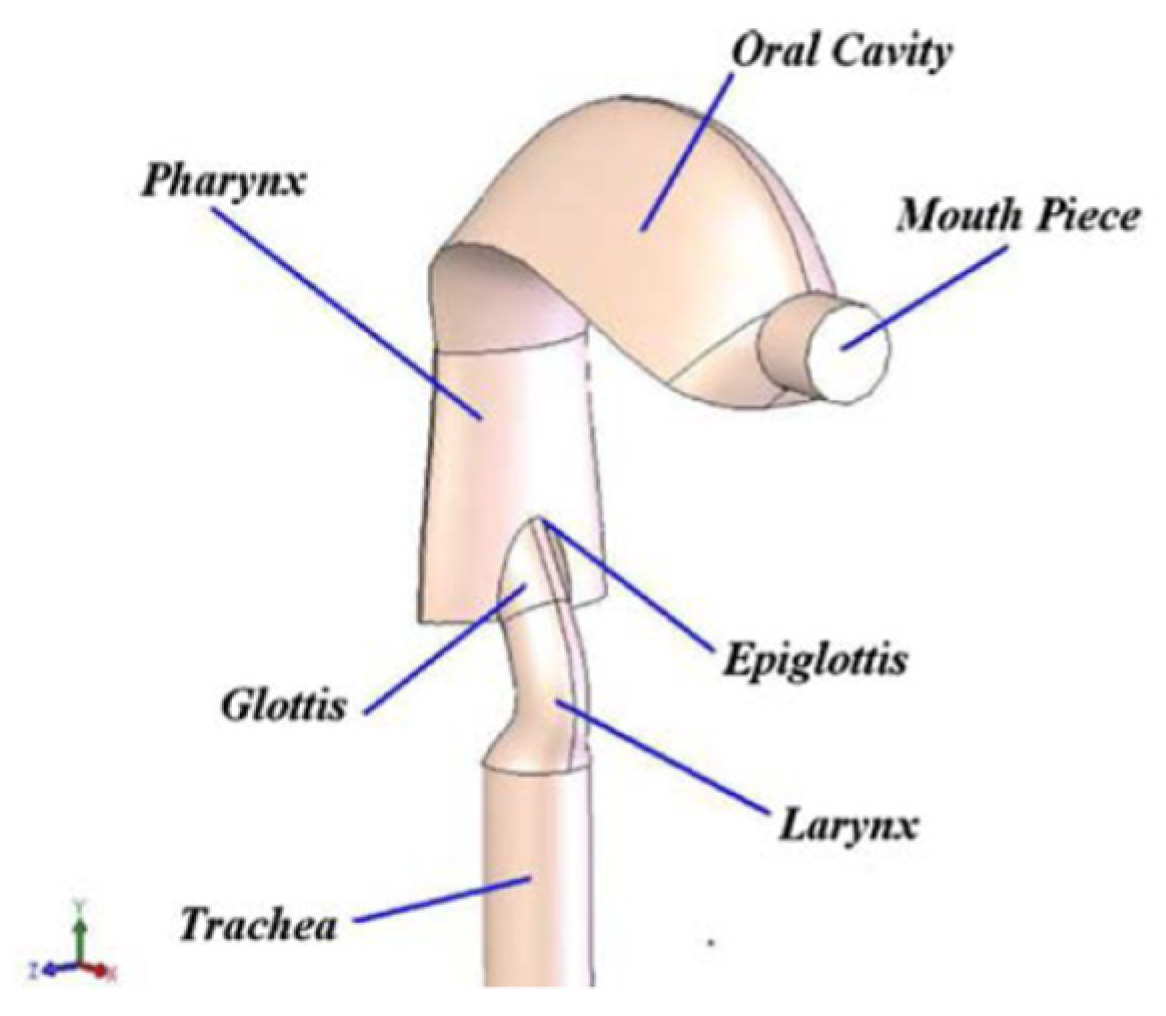
2.2. Modelling of Human UA
2.3. Exclusion of the Nasal Cavity
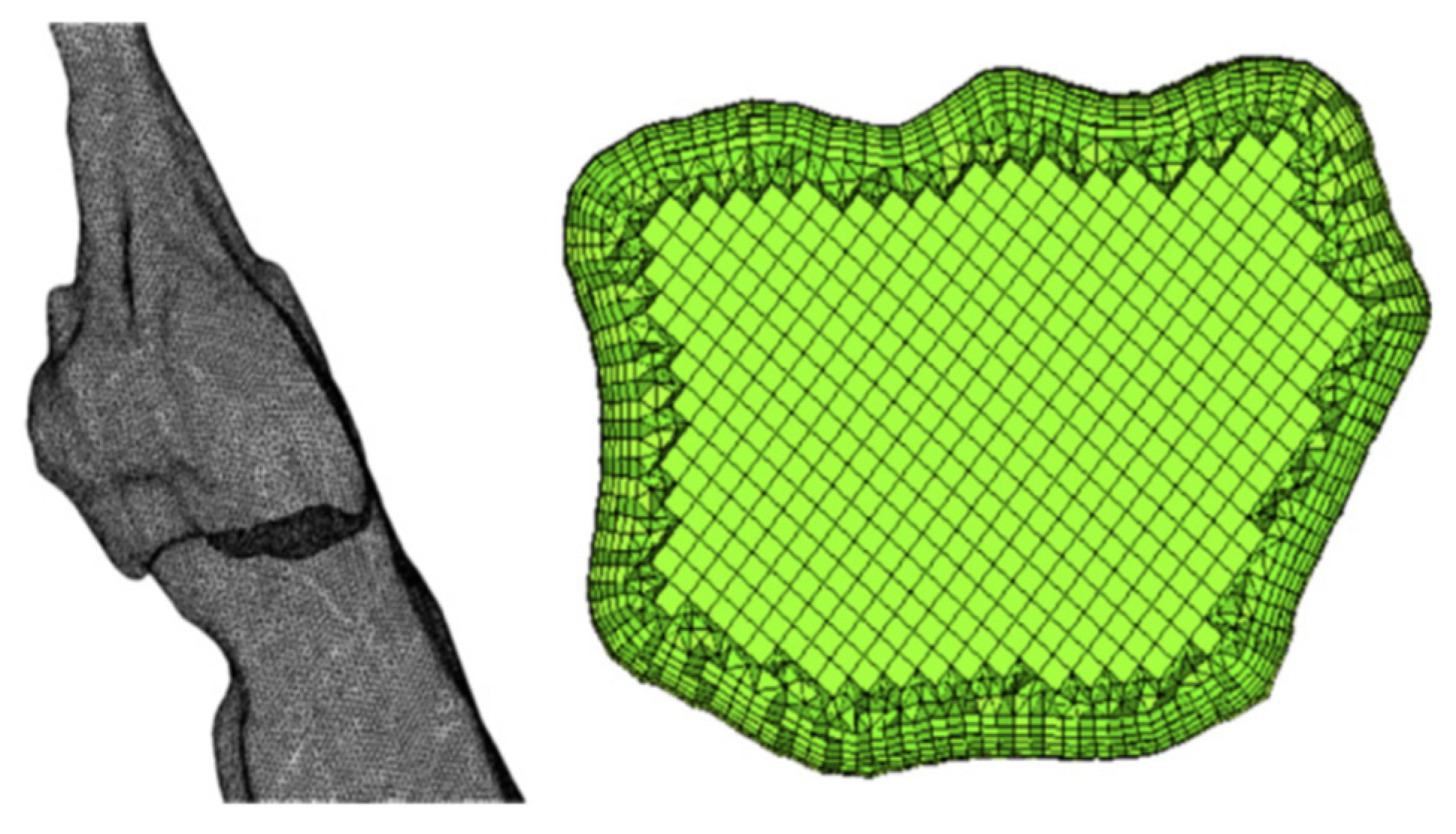
2.4. The Meshing of UA Geometry Accurate Model
2.5. Boundary Conditions
2.6. Turbulence Modelling of UA Flow
2.7. Location of the Inlet
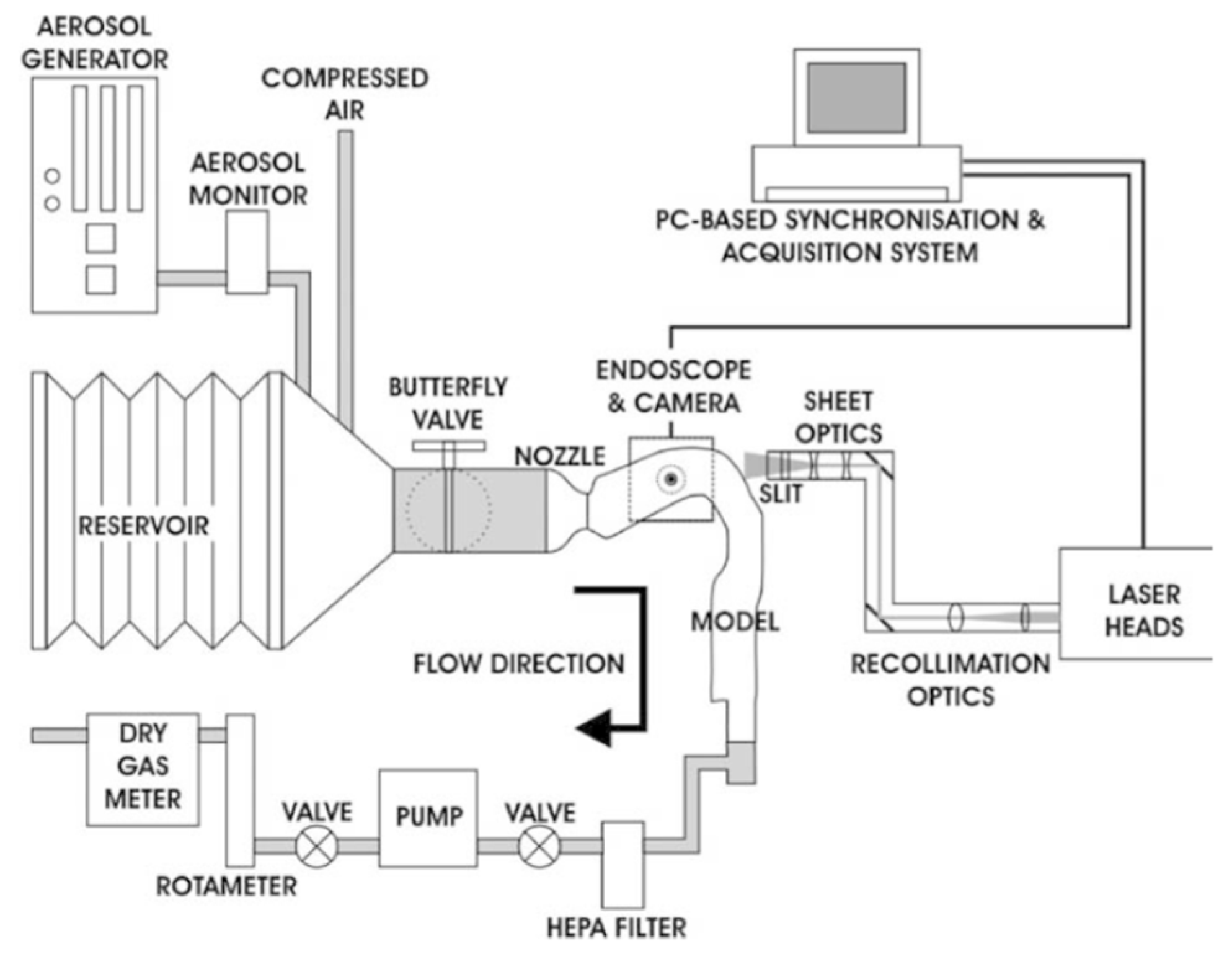
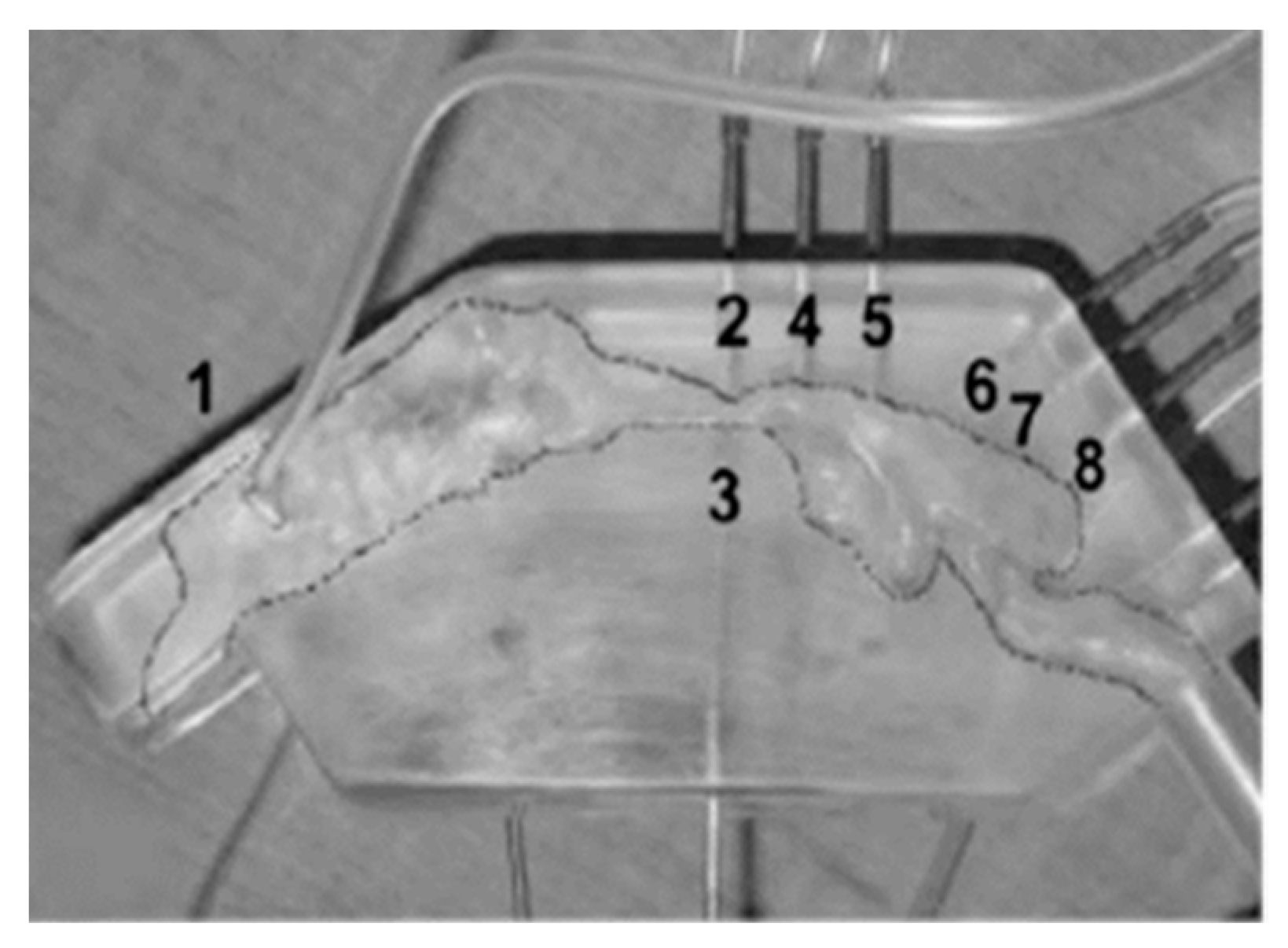
2.8. Experimental Validation
2.9. Numerical Modelling Issues of UA
3. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, C.-H.; Chin, W.-C.; Huang, Y.-S.; Wang, P.-F.; Li, K.K.; Pirelli, P.; Chen, Y.-H.; Guilleminault, C. Objective and subjective long term outcome of maxillomandibular advancement in obstructive sleep apnea. Sleep Med. 2020, 74, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Boyd, S.B.; Walters, A.S.; Waite, P.; Harding, S.M.; Song, Y. Long-term effectiveness and safety of maxillomandibular advancement for treatment of obstructive sleep apnea. J. Clin. Sleep Med. 2015, 11, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Richard, W.; Kox, D.; den Herder, C.; van Tinteren, H.; de Vries, N. One stage multilevel surgery (uvulopalatopharyngoplasty, hyoid suspension, radiofrequent ablation of the tongue base with/without genioglossus advancement), in obstructive sleep apnea syndrome. Eur. Arch. Oto-Rhino-Laryngol. 2007, 264, 439–444. [Google Scholar] [CrossRef]
- Uniken Venema, J.A.; Doff, M.H.; Joffe-Sokolova, D.; Wijkstra, P.J.; van der Hoeven, J.H.; Stegenga, B.; Hoekema, A. Long-term obstructive sleep apnea therapy: A 10-year follow-up of mandibular advancement device and continuous positive airway pressure. J. Clin. Sleep Med. 2020, 16, 353–359. [Google Scholar] [CrossRef]
- Tsui, W.; Yang, Y.; McGrath, C.; Leung, Y. Improvement in quality of life after skeletal advancement surgery in patients with moderate-to-severe obstructive sleep apnoea: A longitudinal study. Int. J. Oral Maxillofac. Surg. 2020, 49, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; White, D.P.; Malhotra, A. The impact of anatomic manipulations on pharyngeal collapse: Results from a computational model of the normal human upper airway. Chest 2005, 128, 1324–1330. [Google Scholar] [CrossRef] [Green Version]
- Aarts, M.C.; Rovers, M.M.; van der Heijden, G.J.; Grolman, W. The value of a mandibular repositioning appliance for the treatment of nonapneic snoring. Otolaryngol. -Head Neck Surg. 2011, 144, 170–173. [Google Scholar] [CrossRef]
- Vicini, C.; Dallan, I.; Campanini, A.; De Vito, A.; Barbanti, F.; Giorgiomarrano, G.; Bosi, M.; Plazzi, G.; Provini, F.; Lugaresi, E. Surgery vs ventilation in adult severe obstructive sleep apnea syndrome. Am. J. Otolaryngol. 2010, 31, 14–20. [Google Scholar] [CrossRef]
- Doff, M.H.; Hoekema, A.; Wijkstra, P.J.; van der Hoeven, J.H.; Huddleston Slater, J.J.; de Bont, L.G.; Stegenga, B. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: A 2-year follow-up. Sleep 2013, 36, 1289–1296. [Google Scholar] [CrossRef] [Green Version]
- Ito, S.; Otake, H.; Tsuiki, S.; Miyao, E.; Noda, A. Obstructive sleep apnea syndrome in a pubescent boy of short stature was improved with an orthodontic mandibular advancement oral appliance: A case report. J. Clin. Sleep Med. 2015, 11, 75–76. [Google Scholar] [CrossRef]
- Nishanth, R.; Sinha, R.; Paul, D.; Uppada, U.K.; Rama Krishna, B.; Tiwari, P. Evaluation of changes in the pharyngeal airway space as a sequele to mandibular advancement surgery: A cephalometric study. J. Maxillofac. Oral Surg. 2020, 19, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Prinsell, J.R. Maxillomandibular advancement surgery for obstructive sleep apnea syndrome. J. Am. Dent. Assoc. 2002, 133, 1489–1497. [Google Scholar] [CrossRef] [PubMed]
- Doff, M.H.; Jansma, J.; Schepers, R.H.; Hoekema, A. Maxillomandibular advancement surgery as alternative to continuous positive airway pressure in morbidly severe obstructive sleep apnea: A case report. CRANIO® 2013, 31, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Gokce, S.M.; Gorgulu, S.; Gokce, H.S.; Bengi, A.O.; Karacayli, U.; Ors, F. Evaluation of pharyngeal airway space changes after bimaxillary orthognathic surgery with a 3-dimensional simulation and modeling program. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 477–492. [Google Scholar] [CrossRef]
- Liu, S.-R.; Yi, H.-L.; Guan, J.; Chen, B.; Wu, H.-M.; Yin, S.-K. Changes in facial appearance after maxillomandibular advancement for severe obstructive sleep apnoea hypopnoea syndrome in Chinese patients: A subjective and objective evaluation. Int. J. Oral Maxillofac. Surg. 2012, 41, 1112–1119. [Google Scholar] [CrossRef]
- Torres, H.M.; Valladares-Neto, J.; Torres, É.M.; Freitas, R.Z.; Silva, M.A.G. Effect of genioplasty on the pharyngeal airway space following maxillomandibular advancement surgery. J. Oral Maxillofac. Surg. 2017, 75, 189.e1–189.e12. [Google Scholar] [CrossRef]
- Rashmikant, U.; Chand, P.; Singh, S.; Singh, R.; Arya, D.; Kant, S.; Agarwal, S. Cephalometric evaluation of mandibular advancement at different horizontal jaw positions in obstructive sleep apnoea patients: A pilot study. Aust. Dent. J. 2013, 58, 293–300. [Google Scholar] [CrossRef]
- Mhlaba, J.M.; Chen, M.L.; Bandla, H.P.; Baroody, F.M.; Reid, R.R. Predictive soft tissue airway volume analysis in mandibular distraction: Pushing the envelope in surgical planning for obstructive sleep apnea. J. Craniofacial Surg. 2016, 27, 181–184. [Google Scholar] [CrossRef]
- Denolf, P.L.; Vanderveken, O.M.; Marklund, M.E.; Braem, M.J. The status of cephalometry in the prediction of non-CPAP treatment outcome in obstructive sleep apnea patients. Sleep Med. Rev. 2016, 27, 56–73. [Google Scholar] [CrossRef]
- Aasgrav, E.; Johnsen, S.G.; Simonsen, A.J.; Müller, B. CFD simulations of turbulent flow in the human upper airways. Arxiv Med. Phys. 2017, 1706, 02565. [Google Scholar]
- Yu, C.-C.; Hsiao, H.-D.; Lee, L.-C.; Yao, C.-M.; Chen, N.-H.; Wang, C.-J.; Chen, Y.-R. Computational fluid dynamic study on obstructive sleep apnea syndrome treated with maxillomandibular advancement. J. Craniofacial Surg. 2009, 20, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Sittitavornwong, S.; Waite, P.D.; Shih, A.M.; Cheng, G.C.; Koomullil, R.; Ito, Y.; Cure, J.K.; Harding, S.M.; Litaker, M. Computational fluid dynamic analysis of the posterior airway space after maxillomandibular advancement for obstructive sleep apnea syndrome. J. Oral Maxillofac. Surg. 2013, 71, 1397–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martonen, T.B.; Quan, L.; Zhang, Z.; Musante, C. Flow simulation in the human upper respiratory tract. Cell Biochem. Biophys. 2002, 37, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Koenig, L.J.; Pruszynski, J.E.; Bradley, T.G.; Bosio, J.A.; Liu, D. Dimensional changes of upper airway after rapid maxillary expansion: A prospective cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 462–470. [Google Scholar] [CrossRef] [Green Version]
- Alsufyani, N.A.; Noga, M.L.; Witmans, M.; Cheng, I.; El-Hakim, H.; Major, P.W. Using cone beam CT to assess the upper airway after surgery in children with sleep disordered breathing symptoms and maxillary-mandibular disproportions: A clinical pilot. J. Otolaryngol. -Head Neck Surg. 2017, 46, 31. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-S.; Wallace, C.G.; Hsiao, Y.-C.; Hsieh, Y.-J.; Wang, Y.-C.; Chen, N.-H.; Liao, Y.-F.; Liou, E.J.-W.; Chen, P.K.-T.; Chen, J.-P. Airway changes after cleft orthognathic surgery evaluated by three-dimensional computed tomography and overnight polysomnographic study. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Susarla, S.M.; Abramson, Z.R.; Dodson, T.B.; Kaban, L.B. Upper airway length decreases after maxillomandibular advancement in patients with obstructive sleep apnea. J. Oral Maxillofac. Surg. 2011, 69, 2872–2878. [Google Scholar] [CrossRef]
- Butterfield, K.J.; Marks, P.L.; McLean, L.; Newton, J. Linear and volumetric airway changes after maxillomandibular advancement for obstructive sleep apnea. J. Oral Maxillofac. Surg. 2015, 73, 1133–1142. [Google Scholar] [CrossRef]
- Ip, M.; Tan, K.; Peh, W.; Lam, K. Effect of Sandostatin® LAR® on sleep apnoea in acromegaly: Correlation with computerized tomographic cephalometry and hormonal activity. Clin. Endocrinol. 2001, 55, 477–483. [Google Scholar] [CrossRef]
- Ito, Y.; Cheng, G.C.; Shih, A.M.; Koomullil, R.P.; Soni, B.K.; Sittitavornwong, S.; Waite, P.D. Patient-specific geometry modeling and mesh generation for simulating obstructive sleep apnea syndrome cases by maxillomandibular advancement. Math. Comput. Simul. 2011, 81, 1876–1891. [Google Scholar] [CrossRef] [Green Version]
- Premaraj, T.S.; Ju, S.; Premaraj, S.; Kim, S.K.; Gu, L. Computational fluid dynamics modeling of pharyngeal airway resistance based on cone-beam computed tomography. J. Mech. Med. Biol. 2019, 19, 1950045. [Google Scholar] [CrossRef]
- Hsieh, Y.-J.; Liao, Y.-F.; Chen, N.-H.; Chen, Y.-R. Changes in the calibre of the upper airway and the surrounding structures after maxillomandibular advancement for obstructive sleep apnoea. Br. J. Oral Maxillofac. Surg. 2014, 52, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.E.; Min, S.W.; Kim, C.S.; Kwon, Y.S.; Hwang, J.Y. Effects of the jaw-thrust manoeuvre in the semi-sitting position on securing a clear airway during fibreoptic intubation. Anaesthesia 2015, 70, 933–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butterfield, K.J.; Marks, P.L.; McLean, L.; Newton, J. Pharyngeal airway morphology in healthy individuals and in obstructive sleep apnea patients treated with maxillomandibular advancement: A comparative study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Souza, F.J.F.d.B.; Evangelista, A.R.; Silva, J.V.; Périco, G.V.; Madeira, K. Cervical computed tomography in patients with obstructive sleep apnea: Influence of head elevation on the assessment of upper airway volume. J. Bras. Pneumol. 2016, 42, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Li, K.K.; Guilleminault, C.; Riley, R.W.; Powell, N.B. Obstructive sleep apnea and maxillomandibular advancement: An assessment of airway changes using radiographic and nasopharyngoscopic examinations. J. Oral Maxillofac. Surg. 2002, 60, 526–530. [Google Scholar] [CrossRef]
- Lin, C.H.; Liao, Y.F.; Chen, N.H.; Lo, L.J.; Chen, Y.R. Three-dimensional computed tomography in obstructive sleep apneics treated by maxillomandibular advancement. Laryngoscope 2011, 121, 1336–1347. [Google Scholar] [CrossRef]
- Lee, W.H.; Hong, S.-N.; Kim, H.J.; Rhee, C.-S.; Lee, C.H.; Yoon, I.-Y.; Kim, J.-W. A comparison of different success definitions in non-continuous positive airway pressure treatment for obstructive sleep apnea using cardiopulmonary coupling. J. Clin. Sleep Med. 2016, 12, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Ristow, O.; Rückschloß, T.; Berger, M.; Grötz, T.; Kargus, S.; Krisam, J.; Seeberger, R.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Short-and long-term changes of the pharyngeal airway after surgical mandibular advancement in class II patients—A three-dimensional retrospective study. J. Cranio-Maxillofac. Surg. 2018, 46, 56–62. [Google Scholar] [CrossRef]
- Gottsauner-Wolf, S.; Laimer, J.; Bruckmoser, E. Posterior airway changes following orthognathic surgery in obstructive sleep apnea. J. Oral Maxillofac. Surg. 2018, 76, 1093.e1–1093.e21. [Google Scholar] [CrossRef]
- Slaats, M.A.; Van Hoorenbeeck, K.; Van Eyck, A.; Vos, W.G.; De Backer, J.W.; Boudewyns, A.; De Backer, W.; Verhulst, S.L. Upper airway imaging in pediatric obstructive sleep apnea syndrome. Sleep Med. Rev. 2015, 21, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Mylavarapu, G.; Mihaescu, M.; Fuchs, L.; Papatziamos, G.; Gutmark, E. Planning human upper airway surgery using computational fluid dynamics. J. Biomech. 2013, 46, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Barber, T.; Cistulli, P.; Sutherland, K.; Rosengarten, G. Computational fluid dynamics for the assessment of upper airway response to oral appliance treatment in obstructive sleep apnea. J. Biomech. 2013, 46, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Achilles, N.; Pasch, N.; Lintermann, A.; Schröder, W.; Mösges, R. Computational fluid dynamics: A suitable assessment tool for demonstrating the antiobstructive effect of drugs in the therapy of allergic rhinitis. Acta Otorhinolaryngol. Ital. 2013, 33, 36–42. [Google Scholar]
- Heenan, A.M.; Pollard, E.; Finlay, A.W. Experimental measurements and computational modeling of the flow field in a idealized human oropharynx. Exp. Fluids 2003, 35, 70–84. [Google Scholar] [CrossRef]
- Collins, T.; Tabor, G.; Young, P. A computational fluid dynamics study of inspiratory flow in orotracheal geometries. Med. Biol. Eng. Comput. 2007, 45, 829–836. [Google Scholar] [CrossRef]
- Barrera, J.E. Virtual surgical planning improves surgical outcome measures in obstructive sleep apnea surgery. Laryngoscope 2014, 124, 1259–1266. [Google Scholar] [CrossRef]
- Sutherland, K.; Chan, A.S.; Cistulli, P.A. Three-dimensional assessment of anatomical balance and oral appliance treatment outcome in obstructive sleep apnoea. Sleep Breath. 2016, 20, 903–910. [Google Scholar] [CrossRef]
- Schneider, D.; Kämmerer, P.W.; Schön, G.; Bschorer, R. A three-dimensional comparison of the pharyngeal airway after mandibular distraction osteogenesis and bilateral sagittal split osteotomy. J. Cranio-Maxillofac. Surg. 2015, 43, 1632–1637. [Google Scholar] [CrossRef]
- Spinelli, G.; Agostini, T.; Arcuri, F.; Conti, M.; Raffaini, M. Three-dimensional airways reconstruction in syndromic pedriatric patients following mandibular distraction osteogenesis. J. Craniofacial Surg. 2015, 26, 650–654. [Google Scholar] [CrossRef]
- Xu, C.; Sin, S.; McDonough, J.M.; Udupa, J.K.; Guez, A.; Arens, R.; Wootton, D.M. Computational fluid dynamics modeling of the upper airway of children with obstructive sleep apnea syndrome in steady flow. J. Biomech. 2006, 39, 2043–2054. [Google Scholar] [CrossRef] [PubMed]
- Huynh, J.; Kim, K.B.; McQuilling, M. Pharyngeal airflow analysis in obstructive sleep apnea patients pre-and post-maxillomandibular advancement surgery. J. Fluids Eng. 2009, 131, 091101. [Google Scholar] [CrossRef]
- Kita, S.; Oshima, M.; Shimazaki, K.; Iwai, T.; Omura, S.; Ono, T. Computational Fluid Dynamic Study of Nasal Respiratory Function Before and After Bimaxillary Orthognathic Surgery With Bone Trimming at the Inferior Edge of the Pyriform Aperture. J. Oral. Maxil. Surg. 2016, 74, 2241–2251. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Cheung, L.; Chong, M.; Chow, K.; Liu, C. Computational study on obstructive sleep apnea syndrome using patient–specific Models. In Proceedings of the World Congress on Engineering, London, UK, 6–8 July 2011. [Google Scholar]
- Zhao, M.; Barber, T.; Cistulli, P.A.; Sutherland, K.; Rosengarten, G. Simulation of upper airway occlusion without and with mandibular advancement in obstructive sleep apnea using fluid-structure interaction. J. Biomech. 2013, 46, 2586–2592. [Google Scholar] [CrossRef]
- Persak, S.C.; Sin, S.; McDonough, J.M.; Arens, R.; Wootton, D.M. Noninvasive estimation of pharyngeal airway resistance and compliance in children based on volume-gated dynamic MRI and computational fluid dynamics. J. Appl. Physiol. 2011, 111, 1819–1827. [Google Scholar] [CrossRef] [Green Version]
- Shah, D.H.; Kim, K.B.; McQuilling, M.W.; Movahed, R.; Shah, A.H.; Kim, Y.I. Computational fluid dynamics for the assessment of upper airway changes in skeletal Class III patients treated with mandibular setback surgery. Angle Orthod. 2016, 86, 976–982. [Google Scholar] [CrossRef] [Green Version]
- Calmet, H.; Gambaruto, A.M.; Bates, A.J.; Vázquez, M.; Houzeaux, G.; Doorly, D.J. Large-scale CFD simulations of the transitional and turbulent regime for the large human airways during rapid inhalation. Comput. Biol. Med. 2016, 69, 166–180. [Google Scholar] [CrossRef] [Green Version]
- Cheng, G.C.; Koomullil, R.P.; Ito, Y.; Shih, A.M.; Sittitavornwong, S.; Waite, P.D. Assessment of surgical effects on patients with obstructive sleep apnea syndrome using computational fluid dynamics simulations. Math. Comput. Simul. 2014, 106, 44–59. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Yan, W.; Liu, Y.; Choy, Y.S.; Wei, Y. Numerical investigation of flow characteristics in the obstructed realistic human upper airway. Comput. Math. Methods Med. 2016, 2016, 3181654. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Kim, H.-H.; ok Hong, S.; Baek, S.-H.; Kim, K.-W.; Suh, S.-H.; Choi, J.-Y. Change in the upper airway of patients with obstructive sleep apnea syndrome using computational fluid dynamics analysis: Conventional maxillomandibular advancement versus modified maxillomandibular advancement with anterior segmental setback osteotomy. J. Craniofacial Surg. 2015, 26, e765–e770. [Google Scholar] [CrossRef]
- Liu, S.Y.-C.; Huon, L.-K.; Iwasaki, T.; Yoon, A.; Riley, R.; Powell, N.; Torre, C.; Capasso, R. Efficacy of maxillomandibular advancement examined with drug-induced sleep endoscopy and computational fluid dynamics airflow modeling. Otolaryngol. -Head Neck Surg. 2016, 154, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, V.K.; Paul, A.R.; Jain, A. Capturing the wall turbulence in CFD simulation of human respiratory tract. Math. Comput. Simul. 2019, 160, 23–38. [Google Scholar] [CrossRef]
- De Backer, J.; Vos, W.; Gorlé, C.; Germonpré, P.; Partoens, B.; Wuyts, F.; Parizel, P.M.; De Backer, W. Flow analyses in the lower airways: Patient-specific model and boundary conditions. Med. Eng. Phys. 2008, 30, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Patel, T.R.; Li, C.; Krebs, J.; Zhao, K.; Malhotra, P. Modeling congenital nasal pyriform aperture stenosis using computational fluid dynamics. Int. J. Pediatr. Otorhinolaryngol 2018, 109, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Sul, B.; Wallqvist, A.; Morris, M.J.; Reifman, J.; Rakesh, V. A computational study of the respiratory airflow characteristics in normal and obstructed human airways. Comput. Biol. Med. 2014, 52, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.K.; Kim, K.B.; McQuilling, M.W.; Movahed, R. Fluid structure interaction simulations of the upper airway in obstructive sleep apnea patients before and after maxillomandibular advancement surgery. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 895–904. [Google Scholar] [CrossRef]
- Habbeche, A.; Saoudi, B.; Jaouadi, B.; Haberra, S.; Kerouaz, B.; Boudelaa, M.; Badis, A.; Ladjama, A. Purification and biochemical characterization of a detergent-stable keratinase from a newly thermophilic actinomycete Actinomadura keratinilytica strain Cpt29 isolated from poultry compost. J. Biosci. Bioeng. 2014, 117, 413–421. [Google Scholar] [CrossRef]
- Bates, A.J.; Schuh, A.; McConnell, K.; Williams, B.M.; Lanier, J.M.; Willmering, M.M.; Woods, J.C.; Fleck, R.J.; Dumoulin, C.L.; Amin, R.S. A novel method to generate dynamic boundary conditions for airway CFD by mapping upper airway movement with non-rigid registration of dynamic and static MRI. Int. J. Numer. Methods Biomed. Eng. 2018, 34, e3144. [Google Scholar] [CrossRef]
- Luo, H.; Sin, S.; McDonough, J.M.; Isasi, C.R.; Arens, R.; Wootton, D.M. Computational fluid dynamics endpoints for assessment of adenotonsillectomy outcome in obese children with obstructive sleep apnea syndrome. J. Biomech. 2014, 47, 2498–2503. [Google Scholar] [CrossRef] [Green Version]
- Zubair, M.; Riazuddin, V.N.; Abdullah, M.Z.; Ismail, R.; Shuaib, I.L.; Ahmad, K.A. Computational fluid dynamics study of the effect of posture on airflow characteristics inside the nasal cavity. Asian Biomed. 2013, 7, 835–840. [Google Scholar] [CrossRef]
- Iwasaki, T.; Sato, H.; Suga, H.; Minami, A.; Yamamoto, Y.; Takemoto, Y.; Inada, E.; Saitoh, I.; Kakuno, E.; Kanomi, R. Herbst appliance effects on pharyngeal airway ventilation evaluated using computational fluid dynamics. Angle Orthod. 2017, 87, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Rahimi-Gorji, M.; Gorji, T.B.; Gorji-Bandpy, M. Details of regional particle deposition and airflow structures in a realistic model of human tracheobronchial airways: Two-phase flow simulation. Comput. Biol. Med. 2016, 74, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Faizal, W.; Ghazali, N.N.N.; Khor, C.; Zainon, M.Z.; Badruddin, I.A.; Kamangar, S.; Ibrahim, N.B.; Razi, R.M. Computational analysis of airflow in upper airway under light and heavy breathing conditions for a realistic patient having obstructive sleep apnea. Comput. Model. Eng. Sci. 2021, 128, 583–604. [Google Scholar] [CrossRef]
- Zheng, Z.; Liu, H.; Xu, Q.; Wu, W.; Du, L.; Chen, H.; Zhang, Y.; Liu, D. Computational fluid dynamics simulation of the upper airway response to large incisor retraction in adult class I bimaxillary protrusion patients. Sci. Rep. 2017, 7, 45706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amatoury, J.; Cheng, S.; Kairaitis, K.; Wheatley, J.R.; Amis, T.C.; Bilston, L.E. Development and validation of a computational finite element model of the rabbit upper airway: Simulations of mandibular advancement and tracheal displacement. J. Appl. Physiol. 2016, 120, 743–757. [Google Scholar] [CrossRef] [Green Version]
- Xi, J.; April Si, X.; Dong, H.; Zhong, H. Effects of glottis motion on airflow and energy expenditure in a human upper airway model. Eur. J. Mech. B/Fluids 2018, 72, 23–37. [Google Scholar] [CrossRef]
- Suga, H.; Iwasaki, T.; Mishima, K.; Nakano, H.; Ueyama, Y.; Yamasaki, Y. Evaluation of the effect of oral appliance treatment on upper-airway ventilation conditions in obstructive sleep apnea using computational fluid dynamics. Cranio 2019, 39, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Gutmark, E.J.; Wootton, D.M.; Sin, S.; Wagshul, M.E.; Subramaniam, D.R.; Arens, R. Biomechanics of the soft-palate in sleep apnea patients with polycystic ovarian syndrome. J. Biomech. 2018, 76, 8–15. [Google Scholar] [CrossRef]
- Fletcher, A.; Choi, J.; Awadalla, M.; Potash, A.E.; Wallen, T.J.; Fletcher, S.; Chang, E.H. The effect of geniglossal advancement on airway flow using a computational flow dynamics model. Laryngoscope 2013, 123, 3227–3232. [Google Scholar] [CrossRef] [Green Version]
- Powell, N.B.; Mihaescu, M.; Mylavarapu, G.; Weaver, E.M.; Guilleminault, C.; Gutmark, E. Patterns in pharyngeal airflow associated with sleep-disordered breathing. Sleep Med. 2011, 12, 966–974. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.Y.; Barber, T.; Cistulli, P.; Sutherland, K.; Rosengarten, G. Predicting the treatment response of oral appliances for obstructive sleep apnea using computational fluid dynamics and fluid-structure interaction simulations. In Proceedings of the Asme International Mechanical Engineering Congress and Exposition, San Diego, CA, USA, 15–21 November 2013. [Google Scholar]
- Mihaescu, M.; Mylavarapu, G.; Gutmark, E.J.; Powell, N.B. Large eddy simulation of the pharyngeal airflow associated with obstructive sleep apnea syndrome at pre and post-surgical treatment. J. Biomech. 2011, 44, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Barber, T.; Cistulli, P.; Sutherland, K.; Rosengarten, G. Computational fluid dynamic study of upper airway flow to predict the success of oral appliances in treating sleep apnea. In Proceedings of the 17th Australasian Fluid Mechanics Conference, Auckland, New Zealand, 5–9 December 2010; pp. 579–582. [Google Scholar]
- Paxman, T.; Noga, M.; Finlay, W.H.; Martin, A.R. Experimental evaluation of pressure drop for flows of air and heliox through upper and central conducting airway replicas of 4-to 8-year-old children. J. Biomech. 2019, 82, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, K.W.; Guentsch, E.; Hoskinson, M.K.; Finlay, W.H. On the suitability of k-ε turbulence modeling for aerosol deposition in the mouth and throat: A comparison with experiment. J. Aerosol Sci. 2000, 31, 739–749. [Google Scholar] [CrossRef]
- Xu, C.; Brennick, M.J.; Dougherty, L.; Wootton, D.M. Modeling upper airway collapse by a finite element model with regional tissue properties. Med. Eng. Phys. 2009, 31, 1343–1348. [Google Scholar] [CrossRef] [Green Version]
- De Backer, J.W.; Vanderveken, O.M.; Vos, W.G.; Devolder, A.; Verhulst, S.L.; Verbraecken, J.A.; Parizel, P.M.; Braem, M.J.; de Heyning, P.H.V.; De Backer, W.A. Functional imaging using computational fluid dynamics to predict treatment success of mandibular advancement devices in sleep-disordered breathing. J. Biomech. 2007, 40, 3708–3714. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Keywords |
|---|---|
| WoS | ALL = ((maxillomandibular OR mandibular OR mandible* OR jaw* OR maxilla) AND (advance$ OR improvement OR gain OR elevation) AND (“obstructive sleep apnea” OR snoring OR “sleep* disorder breath$” OR “pharyngeal airway resist$” OR “sleep apnea”)) |
| Author | Geometry | Turbulence Model | Flowrate Lmin | Remarks |
|---|---|---|---|---|
| Rahimi-Gorji, Gorji and Gorji-Bandpy [73] | CT-scan | k-ω | 10, 15, 30, 60 | Particle deposition study |
| Xi, April Si, Dong and Zhong [77] | CT-scan | LES | 15 | Effects of glottis motion on airflow |
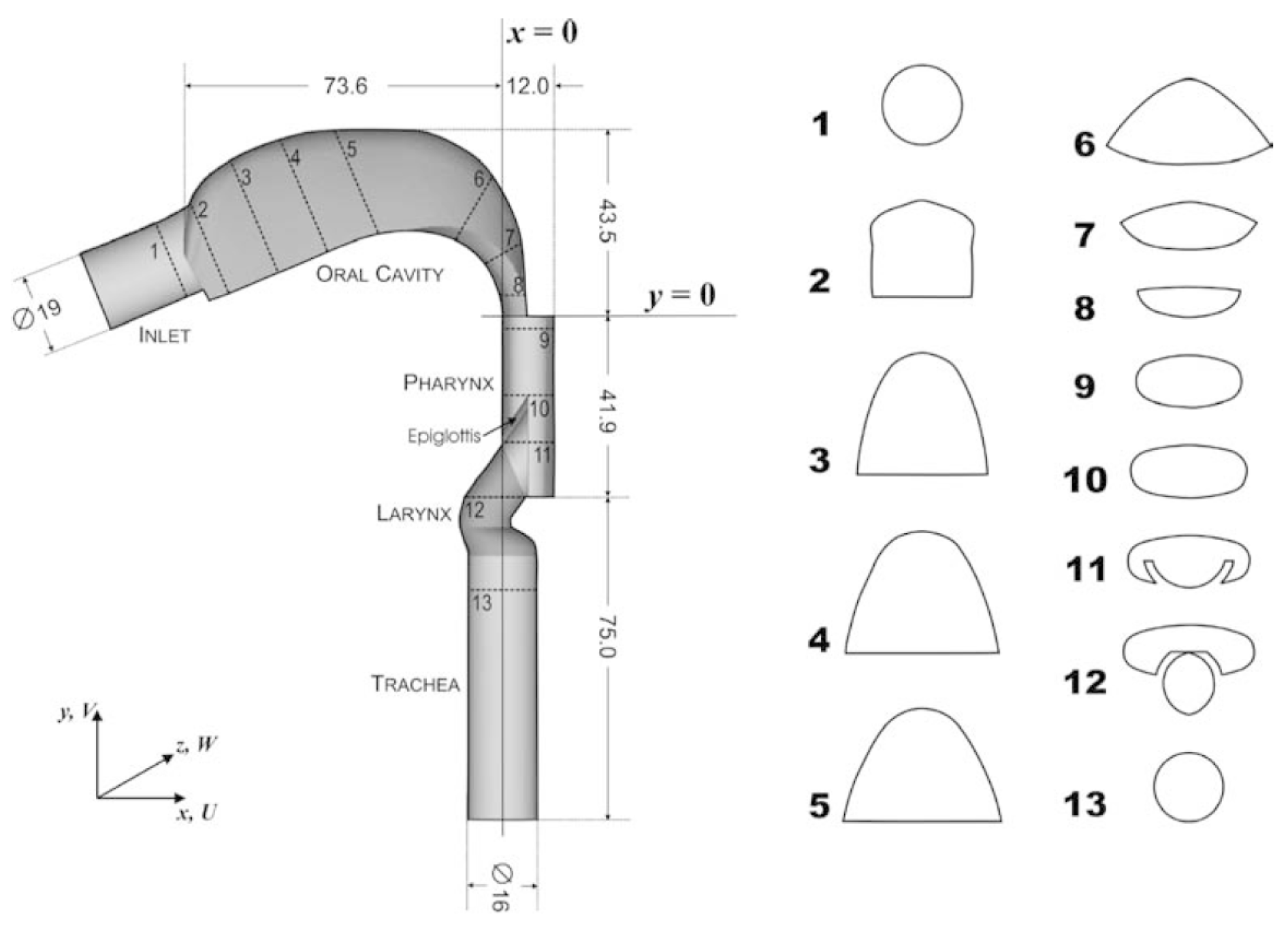
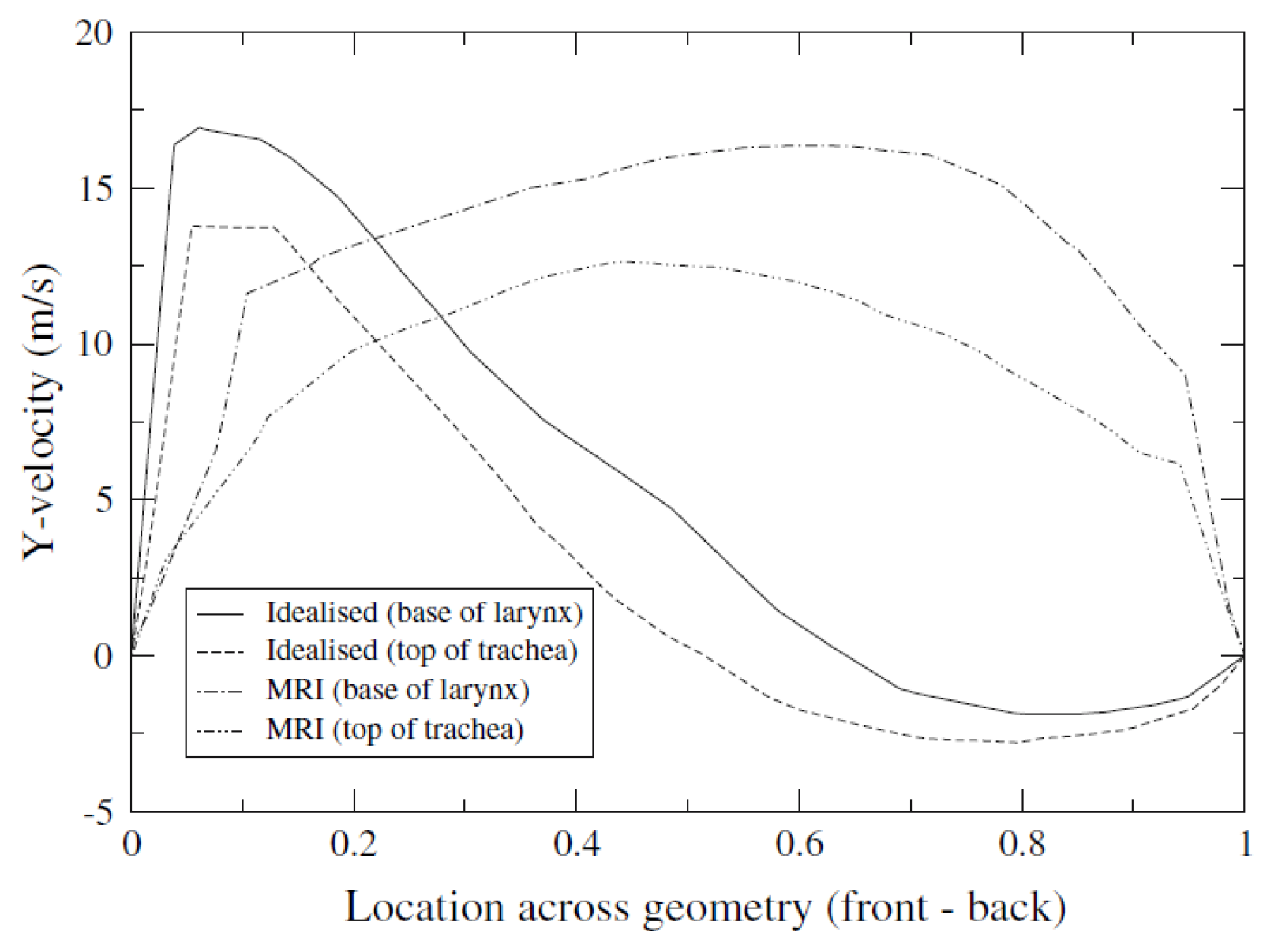
| Collins, Tabor and Young [46] | MRI | k-ω | 72 | Comparison of the idealized vs. accurate geometry model |
| Zubair, Riazuddin, Abdullah, Ismail, Shuaib and Ahmad [71] | CT-scan | laminar | 15 | Study of the effect of posture |
| Zhao, Barber, Cistulli, Sutherland and Rosengarten [43] | MRI | SST k-ω | 10 | Study of upper airway response to oral appliance treatment |
| Cheng, Koomullil, Ito, Shih, Sittitavornwong and Waite [59] | CT-scan | K-ϵ | 42 | Surgical assessment |
| Heenan, Pollard and Finlay [45] | reconstruct model | k–ϵ | 15, 30, and 90 | Study of the idealized airways |
| Suga, et al. [78] | CT-scan | k-ϵ | 30 | Study of the effect of oral appliance treatment |
| Gutmark, et al. [79] | MRI | SST k-ω | 10 | Biomechanics of the soft palate |
| Srivastav, Paul and Jain [63] | CT-scan | k-ϵ, k-ω | 60 | Capturing the wall turbulence |
| Bates, Schuh, McConnell, Williams, Lanier, Willmering, Woods, Fleck, Dumoulin and Amin [69] | MRI | LES | time-dependent 0–3 Ls | New method to generate dynamic boundary conditions for airway |
| Fletcher et al. [80] | CT-scan | LES | 9.06 and 20.52 | Genioglossal advancement (GGA) |
| De Backer, Vos, Gorlé, Germonpré, Partoens, Wuyts and Parizel [64] | CT-scan | Laminar and k-ϵ | 23 | Analyses in the lower airways |
| Srivastav, Paul and Jain [63] | CT-scan | K-ω and k-ϵ | 60 | Simulation of the human respiratory tract |
| Patel, Li, Krebs, Zhao and Malhotra [65] | CT-scan | laminar | 4.67 | Congenital nasal pyriform aperture stenosis (CNPAS) |
| MRI | k-ϵ | |||
| Zhao, Barber, Cistulli, Sutherland and Rosengarten [55] | MRI | K-ω | 10 | MAS |
| Premaraj, Ju, Premaraj, Kim and Gu [31] | CT-scan | K-ω | 18 | Maxillary anterior guided orthotics (MAGO) |
| Cheng, Koomullil, Ito, Shih, Sittitavornwong and Waite [59] | CT-scan | k-ϵ | 42 | Full airways with the nasal cavity |
| Liu, Yan, Liu, Choy and Wei [60] | CT-scan | LES | 16.8, 30, 60 | Including the nasal cavity with an extension funnel |
| Powell et al. [81] | CT-scan | LES, K-ω SST | 30 | Patterns in pharyngeal airflow study |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdul Latif, M.F.; Ghazali, N.N.N.; Abdullah, M.F.; Ibrahim, N.B.; Razi, R.M.; Badruddin, I.A.; Kamangar, S.; Hussien, M.; Ahammad, N.A.; Khan, A. Modelling the Upper Airways of Mandibular Advancement Surgery: A Systematic Review. Mathematics 2023, 11, 219. https://doi.org/10.3390/math11010219
Abdul Latif MF, Ghazali NNN, Abdullah MF, Ibrahim NB, Razi RM, Badruddin IA, Kamangar S, Hussien M, Ahammad NA, Khan A. Modelling the Upper Airways of Mandibular Advancement Surgery: A Systematic Review. Mathematics. 2023; 11(1):219. https://doi.org/10.3390/math11010219
Chicago/Turabian StyleAbdul Latif, Mohd Faruq, Nik Nazri Nik Ghazali, M. F. Abdullah, Norliza Binti Ibrahim, Roziana M. Razi, Irfan Anjum Badruddin, Sarfaraz Kamangar, Mohamed Hussien, N. Ameer Ahammad, and Azeem Khan. 2023. "Modelling the Upper Airways of Mandibular Advancement Surgery: A Systematic Review" Mathematics 11, no. 1: 219. https://doi.org/10.3390/math11010219