
A Feasible Method to Control Left Ventricular Assist Devices for Heart Failure Patients: A Numerical Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
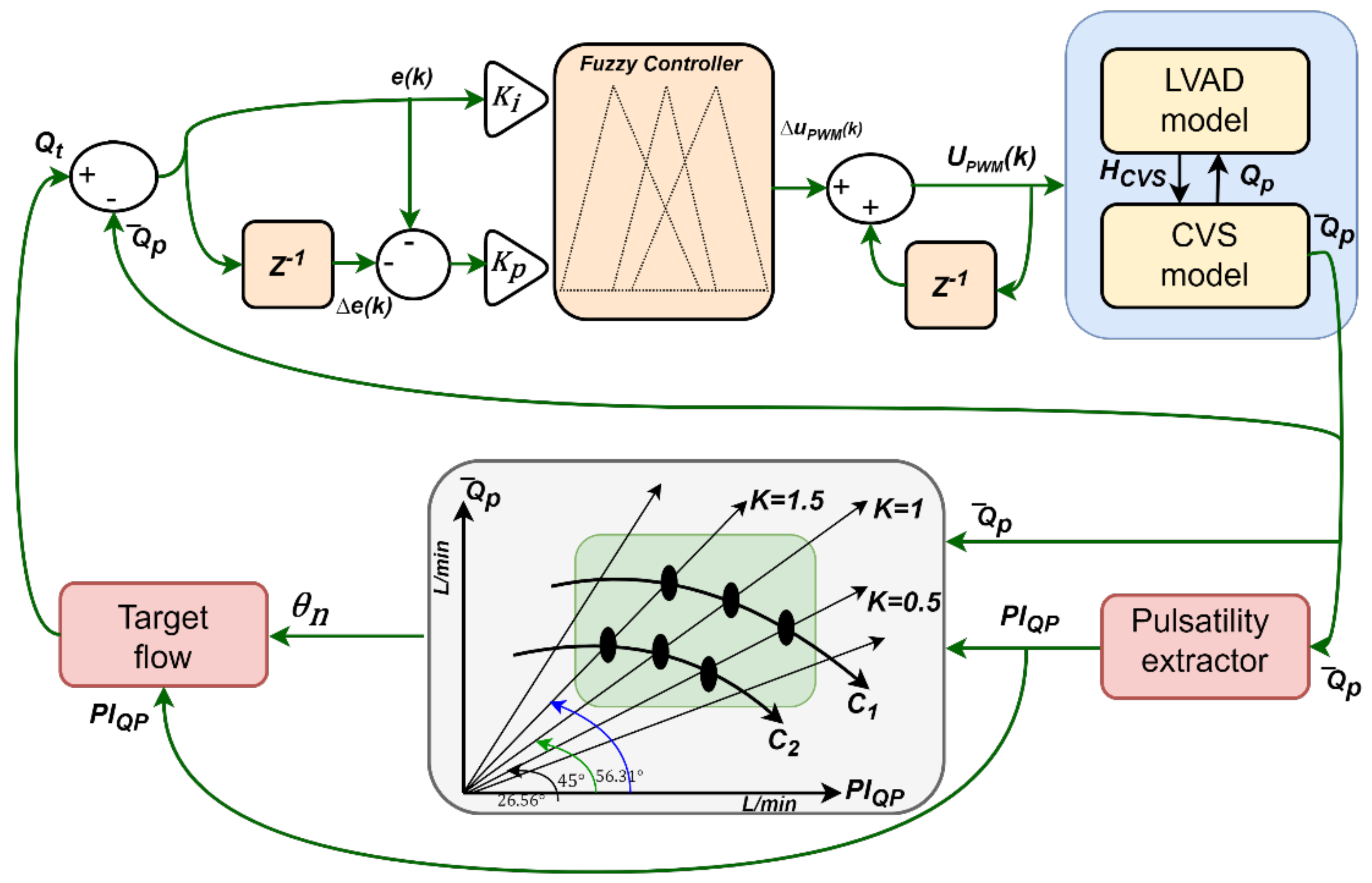
2.1. Control Strategy
2.2. Controller Design
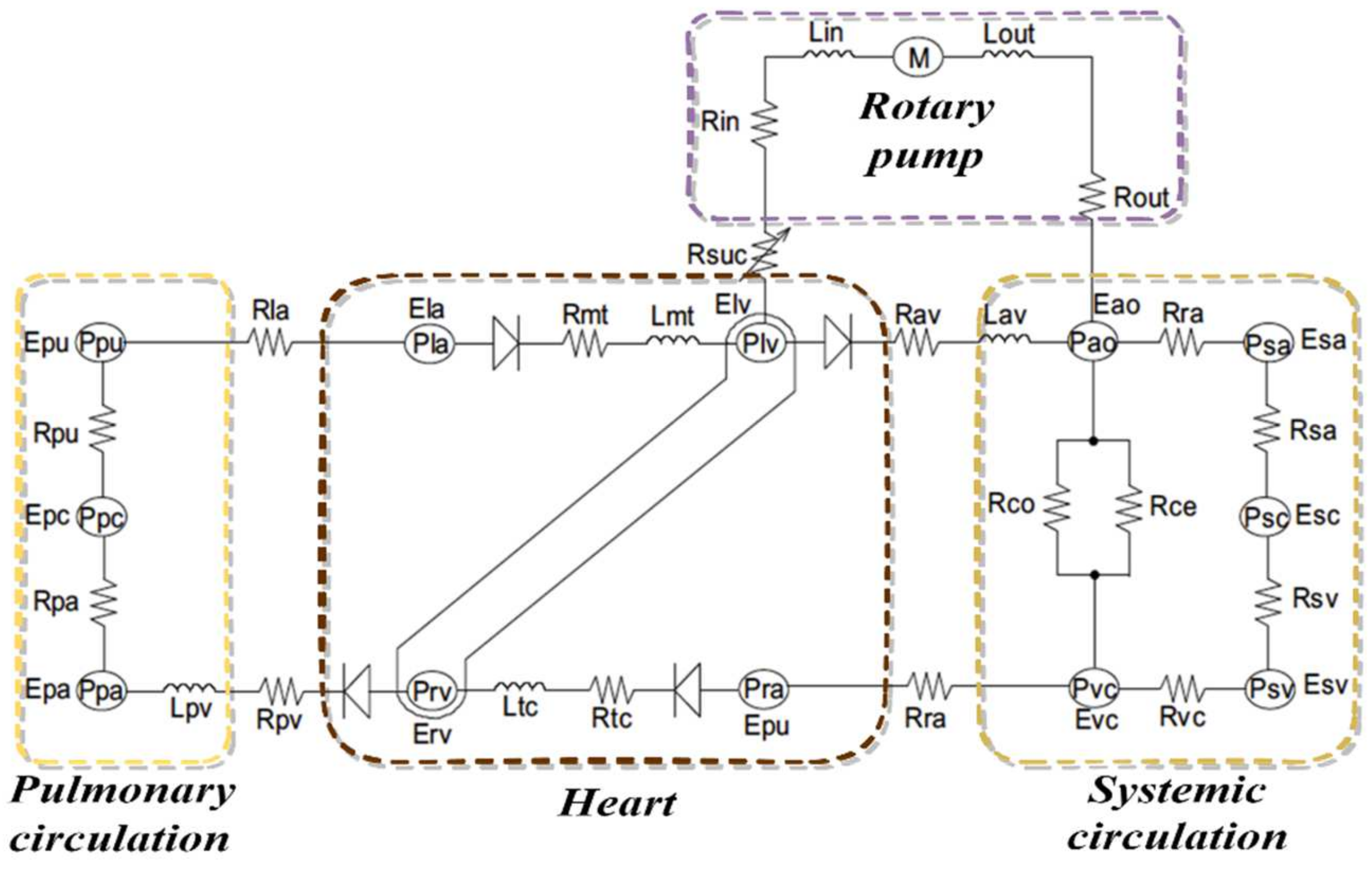
2.3. Software Model
2.4. Simulation Protocols
3. Results
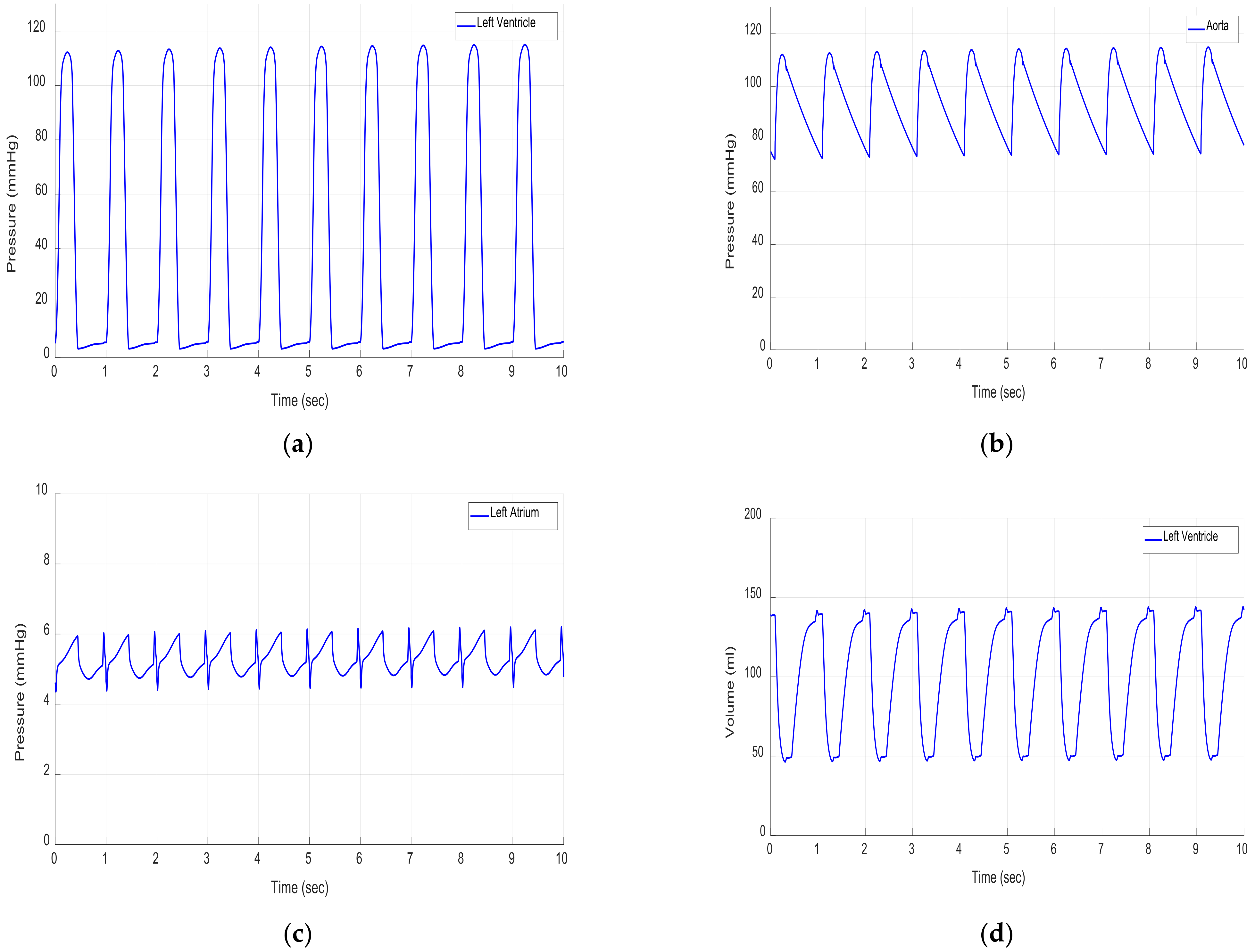
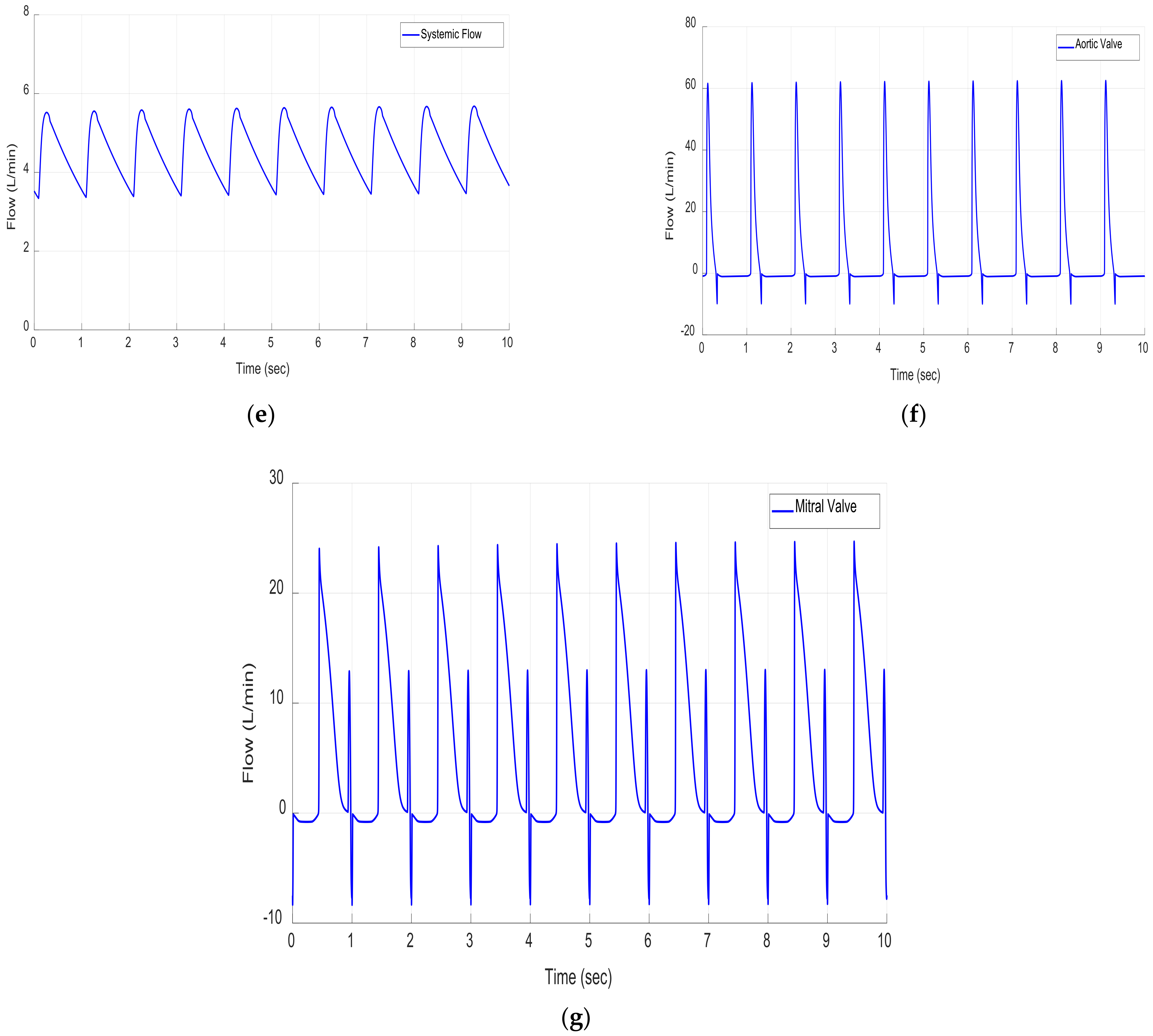
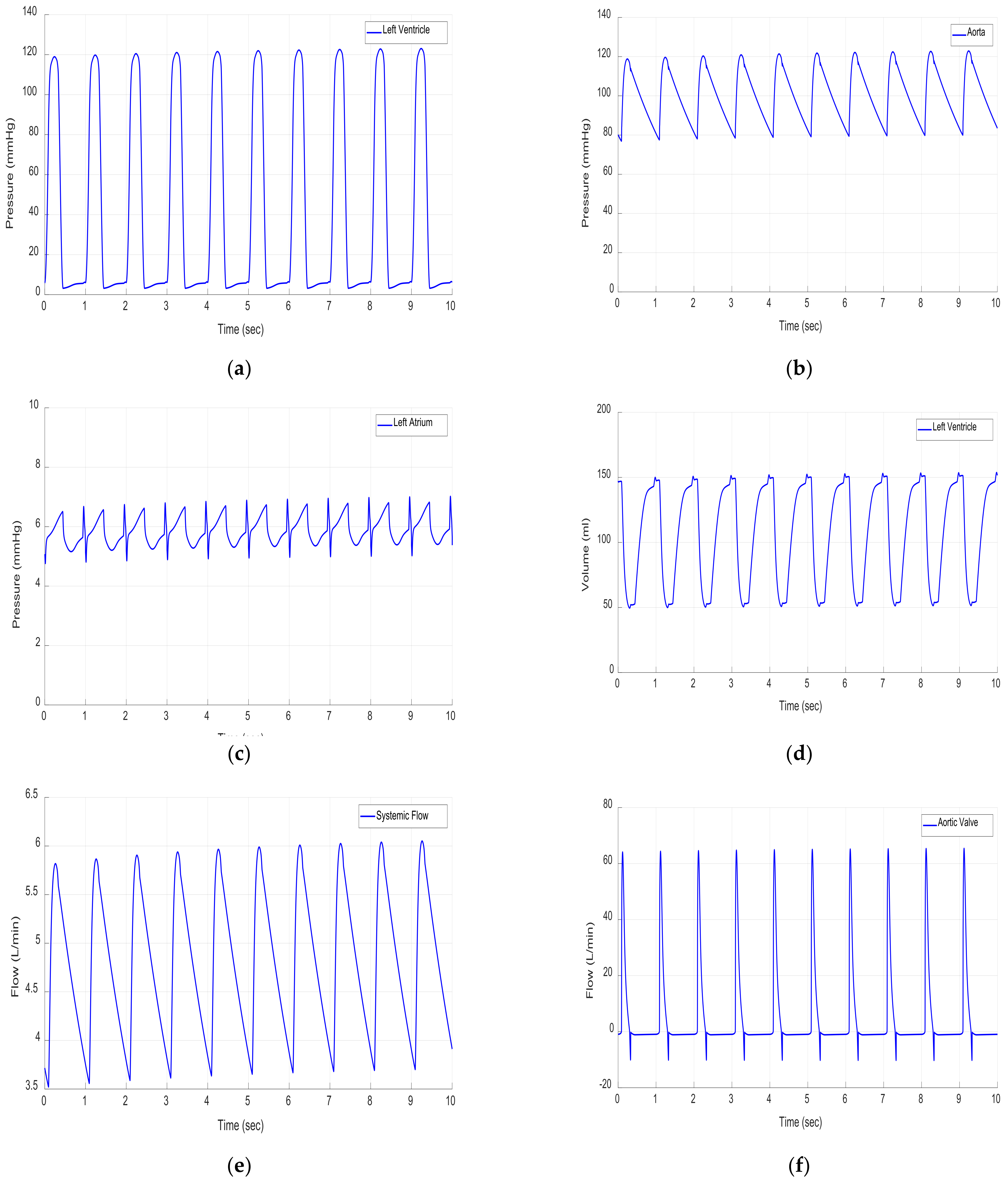
3.1. Results in Rest Scenario
3.2. Results in Moderate Scenario
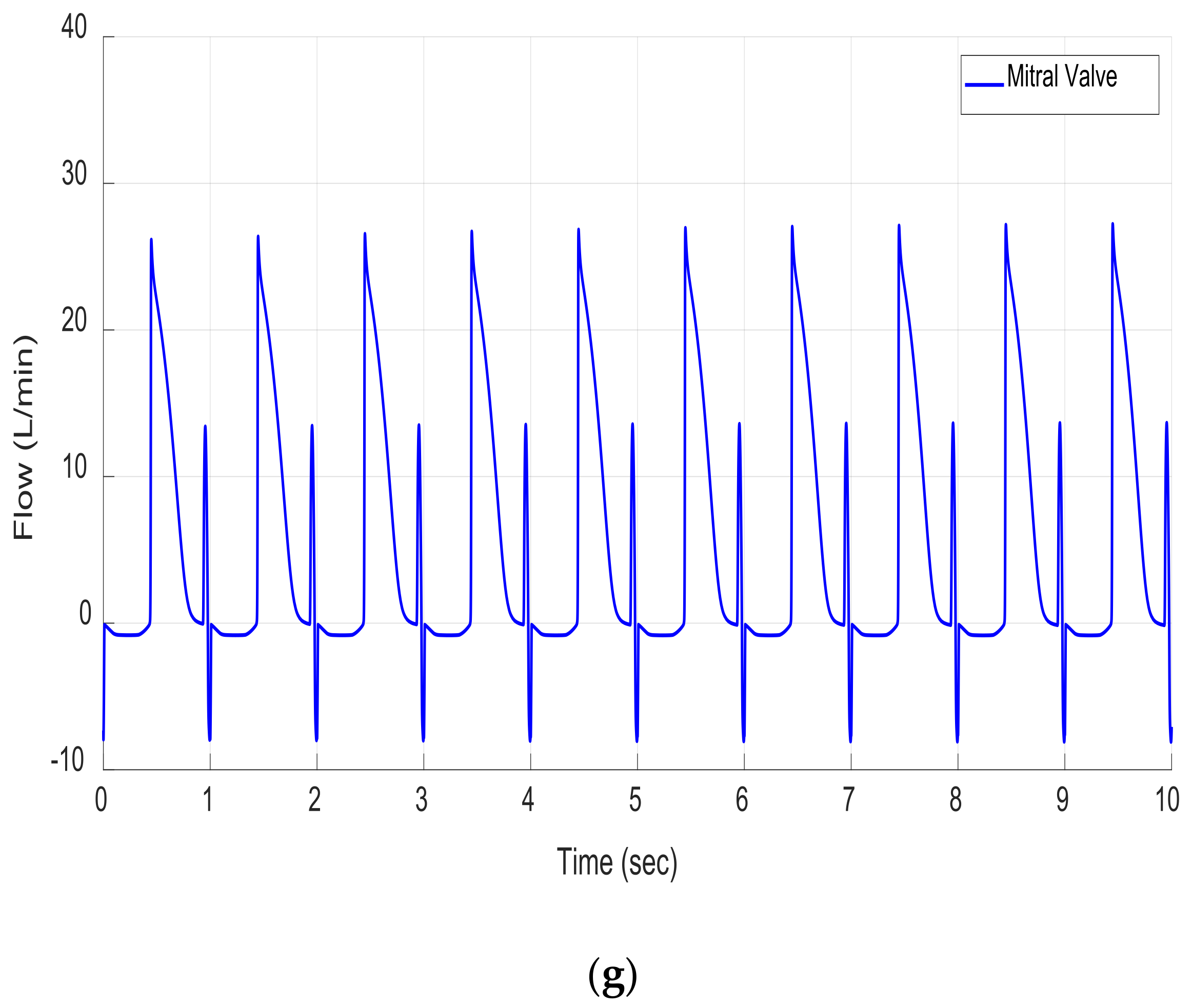
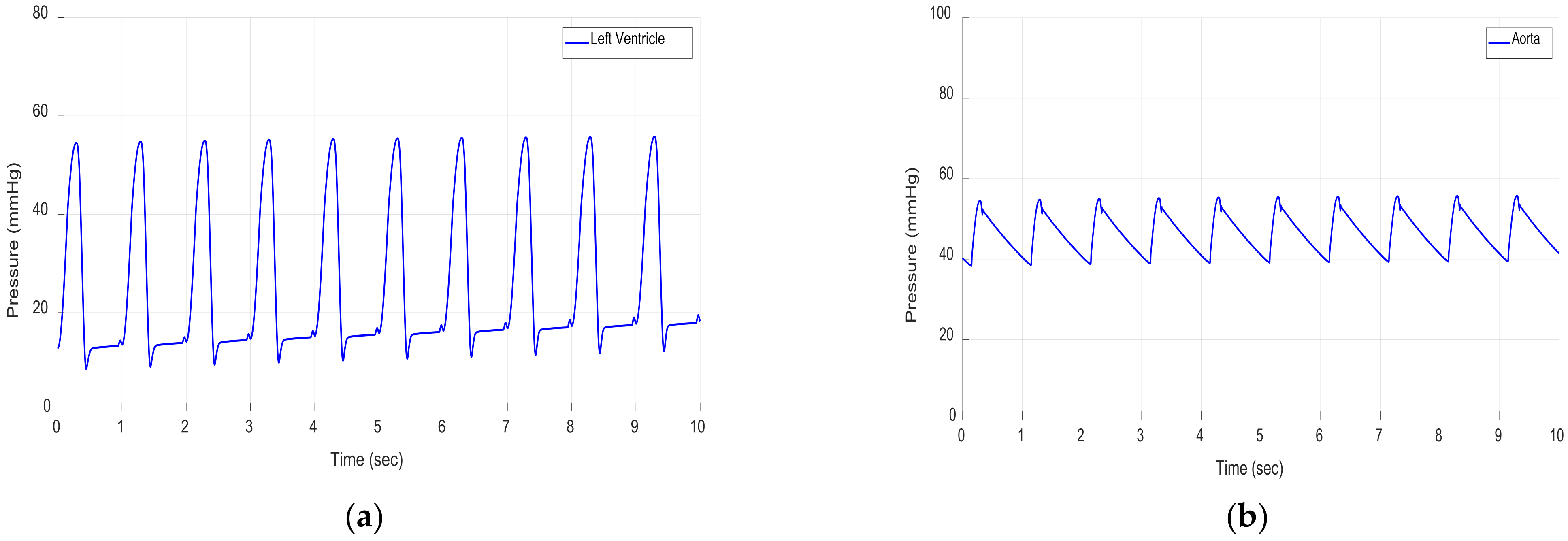
3.3. Results in Exercise Scenario
3.4. Constant Speed Controllers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gwak, K.W.; Ricci, M.; Snyder, S.; Paden, B.E.; Boston, J.R.; Simaan, M.A.; Antaki, J.F. In vitro evaluation of multiobjective hemodynamic control of a heart-assist pump. ASAIO J. 2005, 51, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Ketelhut, M.; Schrödel, F.; Stemmler, S.; Roseveare, J.; Hein, M.; Gesenhues, J.; Albin, T.; Abel, D. Iterative Learning Control of a Left Ventricular Assist Device. IFAC-PapersOnLine 2017, 50, 6684–6690. [Google Scholar] [CrossRef]
- Wu, Y.; Allaire, P.E.; Tao, G.; Adams, M.; Liu, Y.; Wood, H.; Olsen, D.B. A bridge from short-term to long-term left ventricular assist device—Experimental verification of a physiological controller. Artif. Organs 2004, 28, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Amacher, R.; Asprion, J.; Ochsner, G.; Tevaearai, H.; Wilhelm, M.J.; Plass, A.; Amstutz, A.; Vandenberghe, S.; Schmid Daners, M. Numerical optimal control of turbo dynamic ventricular assist devices. Bioengineering 2014, 1, 22–46. [Google Scholar] [CrossRef] [Green Version]
- Son, J.; Du, D.; Du, Y. Modelling and control of a failing heart managed by a left ventricular assist device. Biocybern. Biomed. Eng. 2020, 40, 559–573. [Google Scholar] [CrossRef]
- Ng, B.C.; Smith, P.A.; Nestler, F.; Timms, D.; Cohn, W.E.; Lim, E. Application of Adaptive Starling-Like Controller to Total Artificial Heart Using Dual Rotary Blood Pumps. Ann. Biomed. Eng. 2017, 45, 567–579. [Google Scholar] [CrossRef]
- Wu, Y. Adaptive physiological speed/flow control of rotary blood pumps in permanent implantation using intrinsic pump parameters. ASAIO J. 2009, 55, 335–339. [Google Scholar] [CrossRef]
- Chang, Y.; Gao, B.; Gu, K. A model-free adaptive control to a blood pump based on heart rate. ASAIO J. 2011, 57, 262–267. [Google Scholar] [CrossRef]
- Gaddum, N.R.; Stevens, M.; Lim, E.; Fraser, J.; Lovell, N.; Mason, D.; Timms, D.; Salamonsen, R. Starling-like flow control of a left ventricular assist device: In vitro validation. Artif. Organs 2014, 38, E46–E56. [Google Scholar] [CrossRef]
- Voigt, O.; Benkowski, R.J.; Morello, G.F. Suction detection for the MicroMed DeBakey left ventricular assist device. ASAIO J. 2005, 51, 321–328. [Google Scholar] [CrossRef]
- Wang, Y.; Faragallah, G.; Divo, E.; Simaan, M.A. Feedback control of a rotary left ventricular assist device supporting a failing cardiovascular system. In Proceedings of the American Control Conference (IEEE ACC), Montreal, QC, Canada, 27–29 June 2012; pp. 1137–1142. [Google Scholar]
- Tan, Y.; Nešić, D.; Mareels, I. On non-local stability properties of extremum seeking control. Automatica 2006, 42, 889–903. [Google Scholar] [CrossRef] [Green Version]
- Gwak, K.W. Application of extremum seeking control to turbodynamic blood pumps. ASAIO J. 2007, 53, 403–409. [Google Scholar] [CrossRef]
- Arndt, A.; Nüsser, P.; Lampe, B. Fully autonomous preload-sensitive control of implantable rotary blood pumps. Artif. Organs 2010, 34, 726–735. [Google Scholar] [CrossRef]
- Arndt, A.; Nüsser, P.; Graichen, K.; Müller, J.; Lampe, B. Physiological control of a rotary blood pump with selectable therapeutic options: Control of pulsatility gradient. Artif. Organs 2008, 32, 761–771. [Google Scholar] [CrossRef]
- Ferreira, A.; Boston, J.R.; Antaki, J.F. A control system for rotary blood pumps based on suction detection. IEEE Trans. Biomed. Eng. 2009, 56, 656–665. [Google Scholar] [CrossRef]
- Casas, F.; Ahmed, N.; Reeves, A. Minimal sensor count approach to fuzzy logic rotary blood pump flow control. ASAIO J. 2007, 53, 140–146. [Google Scholar] [CrossRef]
- Choi, S.; Antaki, J.F.; Boston, R.; Thomas, D. A sensorless approach to control of a turbodynamic left ventricular assist system. IEEE Trans. Control Syst. Technol. 2001, 9, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Huang, F.; Ruan, X.; Fu, X. Pulse-pressure-enhancing controller for better physiologic perfusion of rotary blood pumps based on speed modulation. ASAIO J. 2014, 60, 269–279. [Google Scholar] [CrossRef]
- Casas, F.; Orozco, A.; Smith, W.A.; De Abreu-García, J.A.; Durkin, J. A fuzzy system cardio pulmonary bypass rotary blood pump controller. Expert Syst. Appl. 2004, 26, 357–361. [Google Scholar] [CrossRef]
- Bakouri, M.; Salamonsen, R.F.; Savkin, A.V.; Alomari, A.H.H.; Lim, E.; Lovell, N.H. A Sliding Mode-Based Starling-Like Controller for Implantable Rotary Blood Pumps. Artif. Organs 2014, 38, 587–593. [Google Scholar] [CrossRef]
- Bakouri, M.A.; Savkin, A.V.; Alomari, A.H. Nonlinear modelling and control of left ventricular assist device. Electron. Lett. 2015, 51, 613–615. [Google Scholar] [CrossRef]
- Bakouri, M. Evaluation of an advanced model reference sliding mode control method for cardiac assist device using a numerical model. IET Syst. Biol. 2018, 12, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.; Gao, B. A global sliding mode controller design for an intra-aorta pump. ASAIO J. 2010, 56, 510–516. [Google Scholar] [CrossRef]
- Koh, V.C.; Pauls, J.P.; Wu, E.L.; Stevens, M.C.; Ho, Y.K.; Lovell, N.H.; Lim, E. A centralized multi-objective model predictive control for a biventricular assist device: An in vitro evaluation. Biomed. Signal Process. Control 2020, 59, 137–148. [Google Scholar] [CrossRef]
- Koh, V.C.; Ho, Y.K.; Stevens, M.C.; Salamonsen, R.F.; Lovell, N.H.; Lim, E. Synergy of first principles modelling with predictive control for a biventricular assist device: In silico evaluation study. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 1291–1294. [Google Scholar]
- Ng, B.C.; Salamonsen, R.F.; Gregory, S.D.; Stevens, M.C.; Wu, Y.; Mansouri, M.; Lovell, N.H.; Lim, E. Application of multiobjective neural predictive control to biventricular assistance using dual rotary blood pumps. Biomed. Signal Process. Control 2018, 39, 81–93. [Google Scholar] [CrossRef]
- Alomari, A.H.; Javed, F.; Savkin, A.V.; Lim, E.; Salamonsen, R.F.; Mason, D.G.; Lovell, N.H. Non-invasive measurements based model predictive control of pulsatile flow in an implantable rotary blood pump for heart failure patients. In Proceedings of the 2011 19th Mediterranean Conference on Control & Automation (MED), Corfu, Greece, 20–23 June 2011; pp. 491–496. [Google Scholar]
- Bakouri, M.; Alassaf, A.; Alshareef, K.; Abdelsalam, S.; Ismail, H.F.; Ganoun, A.; Alomari, A.H. An Optimal H-Infinity Controller for Left Ventricular Assist Devices Based on a Starling-like Controller: A Simulation Study. Mathematics 2022, 10, 731. [Google Scholar] [CrossRef]
- Lim, E.; Dokos, S.; Salamonsen, R.F.; Rosenfeldt, F.L.; Ayre, P.J.; Lovell, N.H. Numerical Optimization Studies of Cardiovascular-Rotary Blood Pump Interaction. Artif. Organs 2012, 36, 110–124. [Google Scholar] [CrossRef]
- Stefanovska, A. Physics of the human cardiovascular system. Contemp. Phys. 1999, 40, 31–55. [Google Scholar] [CrossRef]
- Alomari, A.H.; Savkin, A.V.; Stevens, M.; Mason, D.G.; Timms, D.L.; Salamonsen, R.F.; Lovell, N.H. Developments in control systems for rotary left ventricular assist devices for heart failure patients: A review. Physiol. Meas. 2013, 34, R1. [Google Scholar] [CrossRef]
- Bozkurt, S. Physiologic outcome of varying speed rotary blood pump support algorithms: A review study. Australas. Phys. Eng. Sci. Med. 2016, 39, 13–28. [Google Scholar] [CrossRef]
- Cysyk, J.; Newswanger, R.; Popjes, E.; Pae, W.; Jhun, C.S.; Izer, J.; Weiss, W.; Rosenberg, G. Cannula tip with integrated volume sensor for rotary blood pump control: Early-stage development. ASAIO J. 2019, 65, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Horobin, J.T.; Simmonds, M.J.; Nandakumar, D.; Gregory, S.D.; Tansley, G.; Pauls, J.P.; Girnghuber, A.; Balletti, N.; Fraser, J.F. Speed Modulation of the HeartWare HVAD to Assess In Vitro Hemocompatibility of Pulsatile and Continuous Flow Regimes in a Rotary Blood Pump. Artif. Organs 2018, 42, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Meki, M.; Wang, Y.; Sethu, P.; Ghazal, M.; El-Baz, A.; Giridharan, G. A Sensorless Rotational Speed-Based Control System for Continuous Flow Left Ventricular Assist Devices. IEEE Trans. Biomed. Eng. 2020, 67, 1050–1060. [Google Scholar] [CrossRef] [PubMed]
- Fetanat, M.; Stevens, M.; Hayward, C.; Lovell, N.H. A Physiological Control System for an Implantable Heart Pump That Accommodates for Interpatient and Intrapatient Variations. IEEE Trans. Biomed. Eng. 2020, 67, 1167–1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misgeld, B.J.; Werner, J.; Hexamer, M. Robust and self-tuning blood flow control during extracorporeal circulation in the presence of system parameter uncertainties. Med. Biol. Eng. Comput. 2005, 43, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Boston, R.; Antaki, J.F. Hemodynamic controller for left ventricular assist device based on pulsatility ratio. Artif. Organs 2007, 31, 114–125. [Google Scholar] [CrossRef]
- Arndt, A.; Nüsser, P.; Lampe, B.P.; Müller, J. Physiological control of a rotary left ventricular assist device: Robust control of pressure pulsatility with suction prevention and suppression. IFMBE Proc. 2009, 25, 775–778. [Google Scholar]
- Wang, Y.; Koenig, S.C.; Slaughter, M.S.; Giridharan, G.A. Rotary blood pump control strategy for preventing left ventricular suction. ASAIO J. 2015, 61, 21–30. [Google Scholar] [CrossRef]
- Giridharan, G.A.; Skliar, M. Nonlinear controller for ventricular assist devices. Artif. Organs 2002, 26, 980–984. [Google Scholar] [CrossRef]
- Giridharan, G.A.; Skliar, M. Physiological control of blood pumps using intrinsic pump parameters: A computer simulation study. Artif. Organs 2006, 30, 301–307. [Google Scholar] [CrossRef]
- Faragallah, G.; Wang, Y.; Divo, E.; Simaan, M. A new control system for left ventricular assist devices based on patient-specific physiological demand. Inverse Probl. Sci. Eng. 2012, 20, 721–734. [Google Scholar] [CrossRef] [Green Version]
- Endo, G.; Araki, K.; Kojima, K.; Nakamura, K.; Matsuzaki, Y.; Onitsuka, T. The index of motor current amplitude has feasibility in control for continuous flow pumps and evaluation of left ventricular function. Artif. Organs 2001, 25, 697–702. [Google Scholar] [CrossRef]
- Rigatos, G.; Siano, P.; Raffo, G. A nonlinear H-infinity control method for multi-DOF robotic manipulators. Nonlinear Dyn. 2017, 88, 329–348. [Google Scholar] [CrossRef]
- Creager, M.A. Baroreceptor reflex function in congestive heart failure. Am. J. Cardiol. 1992, 69, 10–16. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
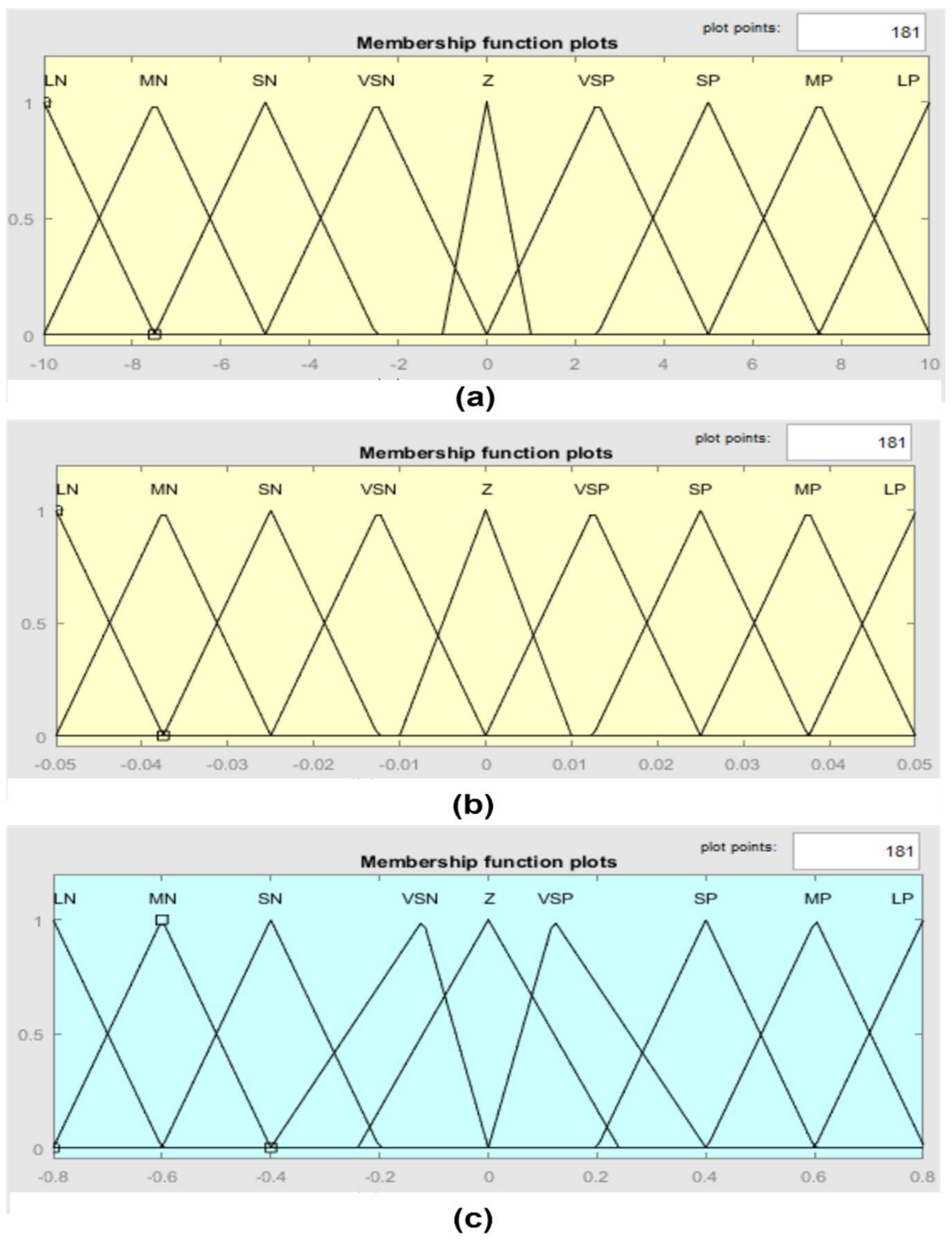
| Label | LN | MN | SN | VSN | Z | VSP | SP | MP | LP |
|---|---|---|---|---|---|---|---|---|---|
| Definition | Large negative | Medium negative | Small negative | Very small negative | Zero | Very small positive | Small Positive | Medium positive | Large positive |
| Δe | LN | MN | SN | Z | SP | MP | LP | |
|---|---|---|---|---|---|---|---|---|
| e | ||||||||
| LN | LN | LN | LN | MN | SN | VSN | Z | |
| MN | LN | LN | MN | SN | VSN | Z | VSP | |
| SN | LN | MN | SN | VSN | Z | VSP | SP | |
| Z | MN | SN | VSN | Z | VSP | SP | MP | |
| SP | SN | VSN | Z | VSP | SP | MP | LP | |
| MP | VSN | Z | VSP | SP | MP | LP | LP | |
| LP | Z | VSP | SP | MP | LP | LP | LP | |
| Variable | Unit | Healthy | Heart Failure (HF) |
|---|---|---|---|
| Total blood volume ( | mL | 5300 | 5800 |
| Left ventricle contractility () | mm Hg/mL | 1.7235 | 0.5322 |
| Right ventricle contractility () | mm Hg/mL | 3.5443 | 0.7100 |
| Systematic vascular resistance () | mm Hg·s/mL | 0.7411 | 1.1100 |
| Hemodynamic Parameters | Unit | Healthy | HF Patient with an LVAD | ||
|---|---|---|---|---|---|
| Rest | Moderate | Exercise | |||
| Left ventricle pressure | mmHg | 120 | 112 | 118 | 55 |
| Aortic pressure | mmHg | 120 | 113 | 120 | 54.66 |
| Left atrial pressure | mmHg | 6 | 4.78 | 6 | 14.87 |
| Left ventricle volume | mL | 150 | 140 | 150 | 287 |
| Systematic flow | L/min | 6 | 5.5 | 6 | 1.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakouri, M.; Alassaf, A.; Alshareef, K.; Smida, A.; AlMohimeed, I.; Alqahtani, A.; Aboamer, M.A.; Alharbi, Y. A Feasible Method to Control Left Ventricular Assist Devices for Heart Failure Patients: A Numerical Study. Mathematics 2022, 10, 2251. https://doi.org/10.3390/math10132251
Bakouri M, Alassaf A, Alshareef K, Smida A, AlMohimeed I, Alqahtani A, Aboamer MA, Alharbi Y. A Feasible Method to Control Left Ventricular Assist Devices for Heart Failure Patients: A Numerical Study. Mathematics. 2022; 10(13):2251. https://doi.org/10.3390/math10132251
Chicago/Turabian StyleBakouri, Mohsen, Ahmad Alassaf, Khaled Alshareef, Amor Smida, Ibrahim AlMohimeed, Abdulrahman Alqahtani, Mohamed Abdelkader Aboamer, and Yousef Alharbi. 2022. "A Feasible Method to Control Left Ventricular Assist Devices for Heart Failure Patients: A Numerical Study" Mathematics 10, no. 13: 2251. https://doi.org/10.3390/math10132251