
Deepening Undergraduate Students’ Thinking about Central Dogma through Problem-Based Learning

Abstract
:1. Introduction
2. Background
2.1. Overview of Problem-Based and Case-Based Learning
2.2. Overall Trends in General Biochemistry Undergraduate Education Case-Based Learning
3. Theoretical Framework: Situated Learning
4. Methods
4.1. Course Context and Participants
4.2. Intervention
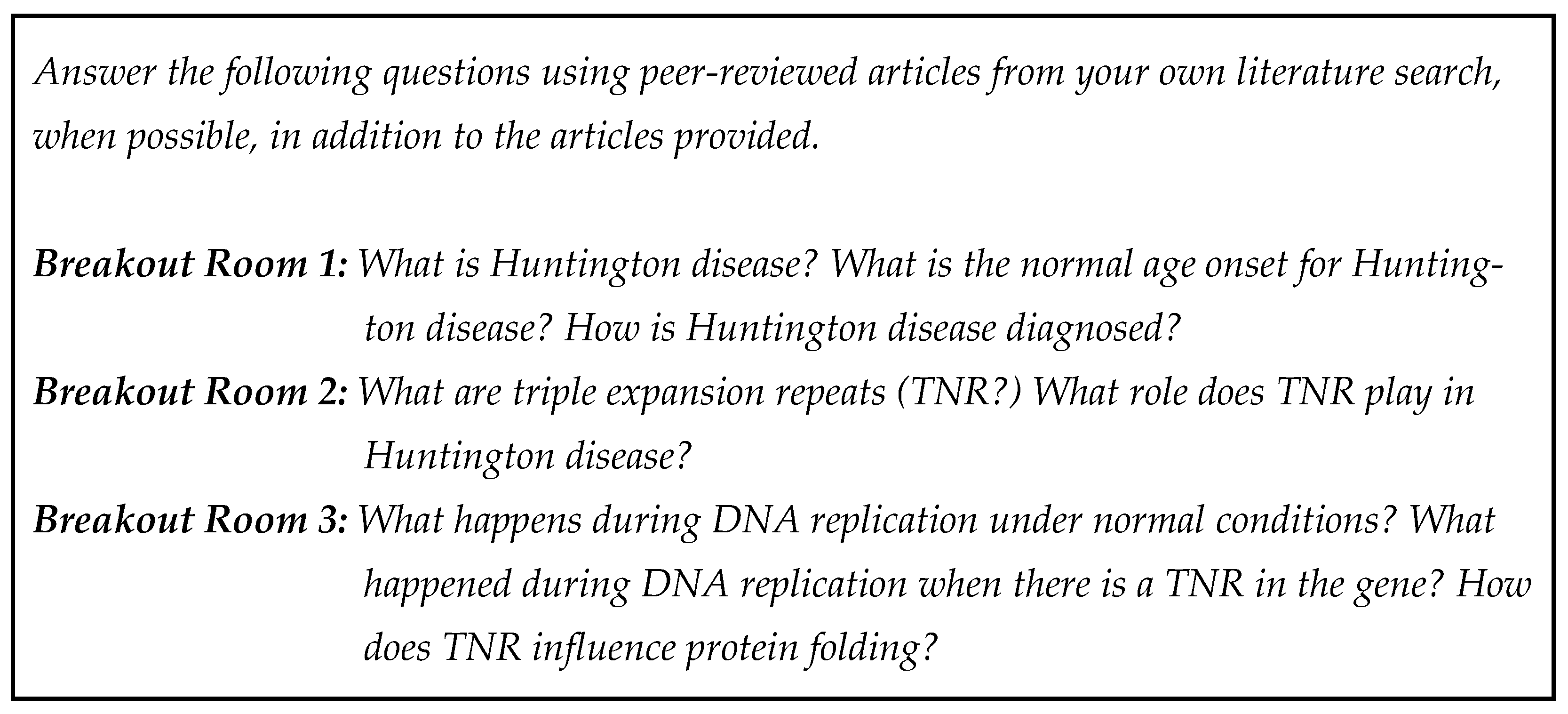
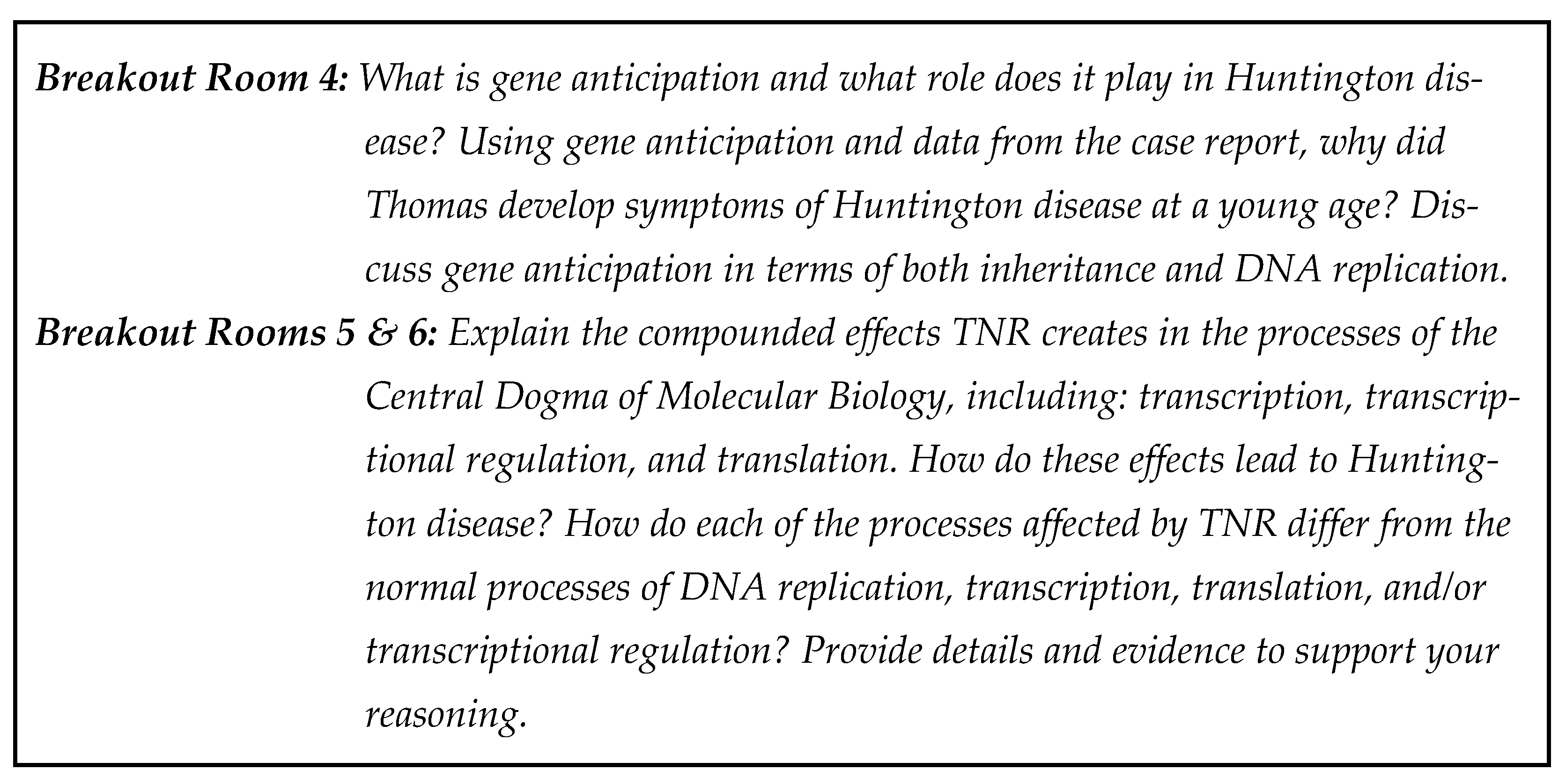
4.2.1. The Case Study
4.2.2. Implementation
4.3. Data Collection
- 1.
- How would you describe the relationship between gene, genotype, gene mutations, phenotype, and disease?
- 2.
- Think about the Central Dogma and Huntington’s disease. Which processes within the Central Dogma are involved in Huntington’s disease? How are they involved in Huntington’s disease?
4.4. Analysis
5. Findings
5.1. Trends within Foundational Knowledge about the Central Dogma
5.1.1. Pre-Survey Responses
Central Dogma Terms and Relationships: CBL− Group Pre-Survey Responses
“A gene codes for a genotype which is presented in physical appearance as a phenotype. A gene mutation can result in a switched up genotype or a new phenotype, and a disease can result in a larger issue depending on what it affects.”
“…If a particular gene carries a disease, it can be found in the genotype after mitosis and meiosis in the offspring. This genotype can display the phenotype of the gene in some cases. Gene mutations can be the cause of disease.”
“Gene is a region coded that will determine the genotype (sequence) and determine the physiological expression of the sequence (phenotype).”
“Gene mutations affect the gene itself, which can result in altered genotypes. Phenotypes are the physical trait observed from a genotype; if a mutant genotype is present and represents through a phenotype, this can result in disease.”
“Gene is a region coded that will determine the genotype (sequence) and determine the physiological expression of the sequence (phenotype). A disease has symptoms that are the phenotype of the mutated gene.”
“Genotypes are comprised of all the genes in an organism. Genes code for proteins that create the phenotype of an organism. Gene mutations can change the phenotype of an organism. Mutations can create certain phenotypic conditions that lead to a disease state.”
“A gene is a sequence of DNA that codes for a protein that can be expressed phenotypically. Genotype is the DNA sequence of an organism. Gene mutations are mutations in the genotype that may or may not be expressed phenotypically. Disease is the result of many possible errors in the central dogma and more, including, but not limited to, mutations occurring in replication, transcription, translation, RNA processing, and mitotic or meiotic mutations.”
Central Dogma Terms and Relationships: CBL+ Group Pre-Survey Responses
“A disease is when that changed phenotype is deleterious and affects some normal function/structure.”
5.1.2. Post-Survey Responses
Persistent Trends in Students’ Conceptions and Depth of Understanding: CBL− Post-Survey Responses
Pre-survey Response: “A gene codes for a genotype which is presented in physical appearance as a phenotype. A gene mutation can result in a switched up genotype or a new phenotype, and a disease can result in a larger issue depending on what it affects.”
Post-survey Response: “A gene is made up of genotypes which physically appear as a phenotype. A gene mutation could alter the genotype to change the phenotype, and if the mutation is bad enough can cause a disease.”
“Genotype is the sequence of DNA which has regions that code for specific genes, which specific regions of DNA sequence. These regions, after Central Dogma, are expressed and produce an observable phenotype. Gene mutations are any abnormal sequence of DNA within a gene encoding region and the product of such disease.”
“[T]hey are all related. genes code for traits and can rise to genotypes, these genes can mutate and lead to changes in phenotype and disease.”
“Genotypes are comprised of all of the genes present in an organism. Mutations can occur within these genes that may lead to a mutant phenotype. These mutant phenotypes may cause adverse reactions within the organism, leading to the disease condition.”
“A gene is what is encoded to make a protein, and a gene can be expressed phenotypically. The sequence of the gene is the genotype. The genotype can give a phenotype. When a mutation occurs, the sequence of the genotype is altered and could lead to a different phenotype like a disease.”
“They are all related. Genes code for traits and can rise to genotypes, these genes can mutate and lead to changes in phenotype and disease.”
“Genotypes are comprised of all the genes present in an organism. Mutations can occur within these genes that may lead to a mutant phenotype. The mutant phenotypes may cause adverse reactions within the organism, leading to the disease condition.
“A gene is made up of genotypes which physically appear as a phenotype…”
Gains in Deep-Level Learning: CBL+ Post-Survey Responses
Pre-survey Response: “…The genotype is a label for what kind of genes you have, while phenotype is the outward appearance of your genotype. Mutations in a gene can result in different genotypes that could lead to different phenotypes that are categorized as a disease.”
Post-survey Response: “An individuals has genes that correspond to their genotype. Genes can have mutations that result in a change in genotype that may or may not result in a new phenotype. Phenotypes are the the [sic] visual characteristics of a genotype. Genetic mutations can lead to phenotypes that are harmful and can be categorized as diseases.”
“Gene mutations can occur in a cell when the DNA for a gene has a mutation or in the process of expressing that gene. When a mutation is present in a person’s genotype that greatly impacts a person’s protein production or function, especially one that is necessary, it can result in a specific phenotype that is different than what is considered normal and can even present itself as a disease.”
“All the genes in an organism make up the organism’s genotype. The genes code for proteins which are expressed in the organism. This expression is the phenotype. When there is mutation in genes, proteins sometimes fold incorrectly and don’t function or function in an inappropriate way. This can cause disease.”
“Different genes are related to genotypes by different alleles on that gene. Gene mutations are a change in a specific allele on the gene such that a nucleotide or more than one nucleotide is changed…”
“Gene mutations can occur in a cell when the DNA for a gene has a mutation or in the process of expressing that gene. When a mutation is present in a person’s genotype that greatly impacts a person’s protein production or function, especially one that is necessary, it can result in a specific phenotype that is different then what is considered normal and can even present itself as a disease.”
“All the genes in an organism make up the organism’s genotype. The genes code for proteins which are expressed in the organism. This expression is the phenotype. When there is mutation in genes, proteins sometimes fold incorrectly and don’t function or function in an inappropriate way. This can cause disease.”
“Genotype refers to the genes of an organism. Phenotype is reflective of how the genes are expressed. Gene mutations can change the phenotype in a way that may or may not cause disease.”
“Our genes are what cause us to have a specific genotype which is simply just our genetic makeup. Gene mutation alter our genotype and can have effects on our phenotype due to the mutations, there are many diseases that are a results of gene mutations that also cause a phenotype.”
5.2. Trends in Students’ Application of Content Knowledge in the Context of Huntington Disease
5.2.1. Pre-Survey Responses
Limited Understanding of the Connection between the Central Dogma and HD: CBL− Pre-Survey Responses
“I do not have any knowledge of the pathogenetic nature of Huntington disease. I guess there is an allelic mutation, but I do not how that is incorporated into the onset of disease.”
“Huntington Disease is a disease caused by gene mutation resulting in a non-functional phenotype which relates perfectly to the central dogma.”
“I’m not sure which part of the central dogma is involved in Huntington’s disease. I know that occurs later in life, and it likely deals with the ineffective production of proteins in some capacity.”
Limited Understanding of the Connection between the Central Dogma and HD: CBL+ Pre-Survey Responses
“I am not sure but I would guess an error occurred during replication that leads to the transcription and translation that creates a protein that is wrong and that causes the disease.”
“The Central Dogma states that DNA makes RNA makes protein. Huntington’s disease is caused by errors in DNA replication when a specific repetitive region of the genome is incorrectly replicated. Extra repeats are added. Because the DNA is incorrect, the wrong RNA and protein will be synthesized because of a cascade effect.”
“Huntington disease is a genetic disease, and a mutation in the DNA causes the transcription and translation to be altered.”
“A certain genotype causes a protein to be formed incorrectly so that it doesn’t function properly. This causes Huntington’s disease.”
“There are specific mutations in the genome that lead to this disease.”
“Huntington’s disease is one gene mutation that is passed on from either parent. I’m not quite sure how they relate in scientific terms, I’d have to do more research.”
“Transcription and translation are processes within the Central Dogma that are involved in Huntington disease. Mistakes made during transcription and translation as well as other problems such as nondisjunction can result in Huntington disease.”
5.2.2. Post-Survey Responses
A Focus on Inheritance to Support Students’ Understanding: CBL− Post-Survey Responses
“…DNA replication produces multiple copies of TNRs that exacerbate the mutation and severity of the HD phenotype.”
“Replication and translation are both deeply involved in Huntington disease. Replication is where the disease starts with the TNR expansion, then translation into a malformed protein that results in the disease.”
“Huntington’s disease is the result of the production of an abnormal protein from a genetic mutation that was inherited from either parent. DNA replication produces multiple copies of TNRs that exacerbate the mutation and severity of the HD phenotype.”
“…This trinucleotide expansion then becomes heritable as a dominant gene. This mutant gene causes the creation of mutant Huntingtin, a protein that can cause severe damage in the cells of the body, especially nerve cells…”
“…This mutant gene causes the creation of mutant Huntingtin, a protein that can cause severe damage in the cells of the body, especially nerve cells. In addition to this mutant protein, Huntington disease can have adverse effects on protein folding in chaperonins, and other effects on normal protein function within the cell.”
“Several aspects of the Central Dogma are involved in Huntington disease. Huntington disease can be caused by errors in DNA replication of the germline cell, causing a trinucleotide repeat expansion to occur. This trinucleotide expansion then becomes heritable as a dominant gene. This mutant gene causes the creation of mutant Huntingtin, a protein that can cause severe damage in the cells of the body, especially nerve cells. In addition to this mutant protein, Huntington disease can have adverse effects on protein folding in chaperonins, and other effects on normal protein function within the cell.”
“Huntington’s disease is the result of the production of an abnormal protein from a genetic mutation that was inherited from either parent. DNA replication produces multiple copies of TNRs that exacerbate the mutation and severity of the HD phenotype.”
“During DNA replication, the DNA polymerase adds on extra repeated nucleotides which will cause an expansion in the DNA. When this expanded DNA gets transcribed, the reading frame of the mRNA changes. Therefore, there is a phenotypic change in terms of proteins expressed and how many.”
“Replication and translation are both deeply involved in Huntington disease. Replication is where the disease starts with the TNR expansion, then translation into a malformed protein that results in the disease.”
Downstream Effects of the Central Dogma and Huntington Disease: CBL+ Post-Survey Responses
A gene is mutated by an expansion of a trinucleotide repeat. This causes the protein to not work and to form aggregates that are toxic.
“Huntington’s disease is caused by TNR mutations in a specific region of the genome. They cause repeats of the CAG sequence and with more TNR, the worse HD is for the patient.”
“All of the processes are involved because as the gene is replicated, there is a slippage in the DNA polymerase that creates TNRs, or trinucleotide repeats, of CAG in a hairpin loop. This hairpin loop when transcribed is incorporated into the mRNA as large amounts of repeats (from the 40s to 70s or even higher when ‘normal’ is considered under 34 repeats). This mRNA is then translated into a protein that has extra amino acids in the protein which leads to misfolding of the protein as extra beta sheets that change the structure enough to form aggregates which in bulk are toxic in the brain and destroy neuron function in the brain.”
“The process that are involved in Huntington disease are translation, DNA replication, and possible transcriptional regulation. During DNA replication, DNA polymerase slips off of the DNA template strand causing a hairpin loop that is incorporated into the DNA causing triple nucleotide repeats. These regions are unstable and in the IR-15 gene are the cause of Huntington Disease. It is speculated that these regions are worsened by DNA mismatch repair inaccurately correcting the error. This causes the repeat area to get even longer leading to earlier onset of worse symptoms of Huntington Disease. When this area is translated as it is found in the exons, it produces proteins that have a different Beta-sheet that causes them to fragment and then come back together in huge groups. These groups are toxic to neural cells and could be the result of cognitive impairment in individuals with Huntington’s disease.”
“Transcription and translation are definitely involved in Huntington’s disease. Huntington’s results from trinucleotide expansions, which can cause slippage and hairpin loops during transcription. These repeats can accumulate over time as more slippage occurs and the repeats are continuously transcribed/translated. When a certain threshold of repeats is reached, an individual is said to have Huntington disease. The more repeats present, the earlier the onset of Huntington’s.”
“The central dogma is involved in HD because as the person’s DNA is replicated, and as people with the disease reproduce, the more repeats there are in the DNA. These repeats are what is causing the problem in people with HD, so increasing the number of repeats just increases the severity of the disease.”
6. Discussion
“Genes codes for proteins which affect the phenotype of an organism. Gene mutations can change the protein produced by the gene and, therefore, change the phenotype of the organism. This phenotypic changes can be disease cause for the organism. The genotype is the specific alleles an organism has for a particular gene.”
“Genotypes are comprised of all the genes in an organism. Genes code for proteins that create the phenotype of an organism. Gene mutations can change the phenotype of an organism. Mutations can create certain phenotypic conditions that lead to a disease state.”
“Genotype is the sequence of DNA which has regions that code for specific genes, which specific regions of DNA sequence. These regions, after central dogma, are expressed and produce an observable phenotype. Gene mutations are any abnormal sequence of DNA within a gene encoding region and the product of such can be diseases.”
“Gene mutations can occur in a cell when the DNA for a gene has a mutation or in the process of expressing that gene. When a mutation is present in a person’s genotype that greatly impacts a person’s protein production or function, especially one that is necessary, it can result in a specific phenotype that is different then [sic] what is considered normal and can even present itself as a disease.”
“Huntington’s disease is the result of the production of an abnormal protein from a genetic mutation that was inherited from either parent. DNA replication produces multiple copies of TNRs that exacerbate the mutation and severity of the HD phenotype.”
“Replication is involved in HD because of errors during replication by slippage of DNA polymerase. Transcription is involved because the extra CAG repeats will be included in the RNA product forming a hairpin loop. The translation is involved because the extra CAG repeats will code for extra glutamines which will, in turn, cause different abnormal/toxic protein folding in a gain of function mutation.”
“During DNA replication, the DNA polymerase adds on extra repeated nucleotides which will cause an expansion in the DNA. When this expanded DNA gets transcribed, the reading frame of the mRNA changes. Therefore, there is a phenotypic change in terms of proteins expressed and how many.”
“All of the processes are involved because as the gene is replicated, there is a slippage in the DNA polymerase that creates TNRs, or trinucleotide repeats, of CAG in a hairpin loop. This hairpin loop when transcribed is incorporated into the mRNA as large amounts of repeats (from the 40s to 70s or even higher when “normal” is considered under 34 repeats). This mRNA is then translated into a protein that has extra amino acids in the protein which leads to misfolding of the protein as extra beta sheets that change the structure enough to form aggregates which in bulk are toxic in the brain and destroy neuron function in the brain.”
7. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savery, J.R. Overview of problem-based learning: Definitions and distinctions. In Essential Readings in Problem-Based Learning; Walking, A.E., Hmelo-Silver, C.E., Leary, H., Ertmer, P.A., Eds.; Purdue University Press: West Lafayette, IN, USA, 2015; pp. 5–15. [Google Scholar]
- Barrows, H.S. A taxonomy of problem-based learning methods. Med. Educ. 1986, 20, 481–486. [Google Scholar] [CrossRef]
- Harden, R.M.; Davis, M.H. The continuum of problem-based learning. Med. Teach. 1998, 20, 317–322. [Google Scholar]
- Kulak, V.; Newton, G. An Investigation of the Pedagogical Impact of Using Case-Based Learning in a Undergraduate Biochemistry Course. Int. J. High. Educ. 2015, 4, 13–24. [Google Scholar] [CrossRef]
- Herreid, C.F. The case study method in the STEM classroom. Metrop. Univ. 2006, 17, 30–40. [Google Scholar]
- Allchin, D. Problem- and case-based learning in science: An introduction to distinctions, values, and outcomes. CBE Life Sci. Educ. 2013, 12, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Cornely, K. The use of case studies in an undergraduate biochemistry course. J. Chem. Educ. 1998, 75, 475. [Google Scholar] [CrossRef]
- Hartfield, P.J. Reinforcing constructivist teaching in advanced level biochemistry through the introduction of case-based learning activities. J. Learn. Des. 2010, 3, 20–31. [Google Scholar] [CrossRef]
- Knight, J.D.; Fulop, R.M.; Márquez-Magana, L.; Tanner, K.D. Investigative cases and student outcomes in an upper-division cell and molecular biology laboratory course at a minority-serving institution. CBE Life Sci. Educ. 2008, 7, 382–393. [Google Scholar] [CrossRef]
- Kulak, V.; Newton, G.; Sharma, R. Does the Use of Case-Based Learning Impact the Retention of Key Concepts in Undergraduate Biochemistry? Int. J. High. Educ. 2017, 6, 110–120. [Google Scholar]
- Porzecanski, A.L.; Bravo, A.; Groom, M.J.; Dávalos, L.M.; Bynum, N.; Abraham, B.J.; Cigliano, J.A.; Griffiths, C.; Stokes, D.L.; Cawthorn, M.; et al. Using case studies to improve the critical thinking skills of undergraduate conservation biology students. Case Stud. Environ. 2021, 5, 1536396. [Google Scholar] [CrossRef]
- Rybarczyk, B.J.; Baines, A.T.; McVey, M.; Thompson, J.T.; Wilkins, H. A case-based approach increases student learning outcomes and comprehension of cellular respiration concepts. Biochem. Mol. Biol. Educ. 2007, 35, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Vedi, N.; Dulloo, P. Students’ perception and learning on case based teaching in anatomy and physiology: An e-learning approach. J. Adv. Med. Educ. Prof. 2021, 9, 8–17. [Google Scholar] [PubMed]
- Chhabra, N.; Kaur, A.; Kukreja, S.; Gill, M. Introduction of Case-based Learning as a Teaching/Learning Tool to enhance Students’ Knowledge in Biochemistry. AMEI’s Curr. Trends Diagn. Treat. 2019, 1, 96–99. [Google Scholar] [CrossRef]
- Birk, T.; Lee, V.; Corbit, A. The Effects of Sex, Ethnicity, and Socioeconomic Status on Student Perceptions of Case-Based Learning in Anatomy and Physiology Classes. HAPS Educ. 2019, 23, 385–395. [Google Scholar] [CrossRef]
- García-Ponce, Á.L.; Martínez-Poveda, B.; Blanco-López, Á.; Quesada, A.R.; Suárez, F.; Alonso-Carrión, F.J.; Medina, M.Á. A problem-/case-based learning approach as a useful tool for studying glycogen metabolism and its regulation. Biochem. Mol. Biol. Educ. 2021, 49, 236–241. [Google Scholar] [CrossRef]
- NGSS Lead States. Next Generation Science Standards: For States, by States; The National Academies Press: Washington, DC, USA, 2013. [Google Scholar]
- National Research Council. A New Biology for the 21st Century; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Hays, E.; Levine, J.; Rethi, S.; Smith, E.K.; Upadhya, S.; Sobering, A.K.; Weiler, T. Reevaluating Biochemistry and Nutrition Education Through Opinions of Clinicians and Educators. Med. Sci. Educ. 2019, 29, 189–197. [Google Scholar] [CrossRef]
- Gadbury-Amyot, C.C.; Overman, P.R.; Crain, G. The development and implementation of an online applied biochemistry bridge course for a dental hygiene curriculum. J. Dent. Educ. 2009, 73, 83–94. [Google Scholar] [CrossRef]
- Ebomoyi, M.I.; Agoreyo, F.D. Preclinical Students’ Perceptions of Their Courses and Pre-Clinical Specialty Choice; College of Medical Sciences, University of Benin: Benin City, Nigeria, 2007. [Google Scholar]
- Watmough, S.; O’Sullivan, H.; Taylor, D. Graduates from a traditional medical curriculum evaluate the effectiveness of their medical curriculum through interviews. BMC Med. Educ. 2009, 9, 64. [Google Scholar] [CrossRef]
- Rhodes, A.; Wilson, A.; Rozell, T. Value of case-based learning within STEM courses: Is it the method or is it the student? CBE—Life Sci. Educ. 2020, 19, ar44. [Google Scholar] [CrossRef]
- Srinivasan, M.; Wilkes, M.; Stevenson, F.; Nguyen, T.; Slavin, S. Comparing problem-based learning with case-based learning: Effects of a major curricular shift at two institutions. Acad. Med. 2007, 82, 74–82. [Google Scholar] [CrossRef]
- Schmidt, H.G. A brief history of problem-based learning. In One-Day, One-Problem: An Approach to Problem-Based Learning; O’Grady, G., Yew, E., Goh, K.P., Schmidt, H.G., Eds.; Springer: Singapore, 2012; pp. 21–40. [Google Scholar]
- Simons, K.D.; Ertmer, P.A. Scaffolding disciplined inquiry in problem-based environments. Int. J. Learn. 2005, 12, 297–305. [Google Scholar]
- Alt, D.; Raichel, N. Reflective journaling and metacognitive awareness: Insights from a longitudinal study in higher education. Reflective Pract. 2020, 21, 145–158. [Google Scholar] [CrossRef]
- Yadav, A.; Lundeberg, M.; DeSchryver, M.; Dirkin, K.; Schiller, N.A.; Maier, K.; Her-reid, C.F. Teaching science with case studies: A national survey of faculty perceptions of the benefits and challenges of using cases. J. Coll. Sci. Teach. 2007, 37, 34. [Google Scholar]
- Hyland, D.; van Kampen, P.; Nolan, B. Student perceptions of a guided inquiry approach to a service-taught ordinary differential equations course. Int. J. Math. Educ. Sci. Technol. 2023, 54, 250–276. [Google Scholar] [CrossRef]
- Cresswell, S.L.; Loughlin, W.A. A case-based scenario with interdisciplinary guided-inquiry in chemistry and biology: Experiences of first year forensic science students. J. Chem. Educ. 2017, 94, 1074–1082. [Google Scholar] [CrossRef]
- Trigwell, K.; Prosser, M.; Waterhouse, F. Relations between teachers’ approaches to teaching and students’ approaches to learning. High. Educ. 1999, 37, 57–70. [Google Scholar] [CrossRef]
- Yan, Q.; Ma, L.; Zhu, L.; Zhang, W. Learning effectiveness and satisfaction of international medical students: Introducing a Hybrid–PBL curriculum in biochemistry. Biochem. Mol. Biol. Educ. 2017, 45, 336–342. [Google Scholar] [CrossRef]
- Lave, J.; Wenger, E. Situated Learning: Legitimate Peripheral Participation; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Goodwin, C. Professional vision. Am. Anthropol. 1994, 96, 606–633. [Google Scholar] [CrossRef]
- Hedegaard, M. Situated learning and cognition: Theoretical learning and cognition. Mind Cult. Act. 1998, 5, 114–126. [Google Scholar] [CrossRef]
- Lowyck, Y. Bridging learning theories and technology-enhanced environments: A critical appraisal of its history. In Handbook of Research on Educational Communications and Technology; Spector, J.M., Merrill, M.D., Elen, J., Bishop, M.J., Eds.; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Vygotsky, L.S. Ausgewahlte Schrifren [Selected Writings]; Pahl-Rugenstein: Koln, Germany, 1987. [Google Scholar]
- Brown, J.S.; Collins, A.; Duguid, P. Debating the situation: A rejoinder to Palincsar & Wineburg’s response. Educ. Res. 1989, 18, 10–12. [Google Scholar]
- Brown, J.S.; Collins, A.; Duguid, P. Situated cognition and the culture of learning. Educ. Res. 1989, 18, 32–42. [Google Scholar] [CrossRef]
- González, N.; Moll, L.C.; Amanti, C. (Eds.) Funds of Knowledge: Theorizing Practices in Households, Communities, and Classrooms; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2005. [Google Scholar]
- Palincsar, A.S. Response to Brown, Collins and Duguid’s “Situated cognition and the culture of learning”: Less charted waters. Educ. Res. 1989, 18, 5–7. [Google Scholar]
- Vosniadou, S. The Framework Theory Approach to the Problem of Conceptual Change. In Handbook of Research on Conceptual Change; Vosniadou, S., Ed.; Routledge: Oxfordshire, UK, 2007. [Google Scholar]
- Vosniadou, S. Reframing the classical approach to conceptual change: Preconceptions, misconceptions and synthetic models. In Second International Handbook of Science Education; Springer: Dordrecht, The Netherlands, 2012; pp. 119–130. [Google Scholar] [CrossRef]
- Inagaki, K.; Hatano, G. Conceptual change in naïve biology. In Handbook of Research on Conceptual Change; Vosniadou, S., Ed.; Routledge: Oxfordshire, UK, 2007. [Google Scholar]
- Bandura, A. Social Learning Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1977. [Google Scholar]
- Hendricks, C.C. Teaching causal reasoning through cognitive apprenticeship: What are results from situated learning? J. Educ. Res. 2001, 94, 302–311. [Google Scholar] [CrossRef]
- Lunce, L.M. Simulations: Bringing the benefits of situated learning to the traditional classroom. J. Appl. Educ. Technol. 2006, 3, 37–45. [Google Scholar]
- Stake, R.E. The Art of Case Study Research; Sage Publications: London, UK, 1995. [Google Scholar]
- Creswell, J.W.; Hanson, W.E.; Clark Plano, V.L.; Morales, A. Qualitative research designs: Selection and implementation. Couns. Psychol. 2007, 35, 236–264. [Google Scholar] [CrossRef]
- Duesterhus, P.; Schimmelmann, B.G.; Wittkugel, O.; Schulte-Markwort, M. Huntington disease: A case study of early onset presenting as depression. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 1293–1297. [Google Scholar] [CrossRef]
- Nance, M.A.; Myers, R.H. Juvenile onset Huntington’s disease—Clinical and research perspectives. Ment. Retard. Dev. Disabil. Res. Rev. 2001, 7, 153–157. [Google Scholar] [CrossRef]
- Committee on Bioethics; Committee on Genetics; American College of Medical Genetics, Genomics Social, Ethical and Legal Issues Committee; Fallat, M.E.; Katz, A.L.; Mercurio, M.R.; Moon, M.R.; Okun, M.L.; Webb, S.A.; Weise, K.L.; et al. Ethical and policy issues in genetic testing and screening of children. Pediatrics 2013, 131, 620–622. [Google Scholar] [CrossRef]
- Stoker, T.B.; Mason, S.L.; Greenland, J.C.; Holden, S.T.; Santini, H.; Barker, R.A. Huntington’s disease: Diagnosis and management. Pract. Neurol. 2022, 22, 32–41. [Google Scholar] [CrossRef]
- Gubert, C.; Renoir, T.; Hannan, A.J. Why Woody got the blues: The neurobiology of depression in Huntington’s disease. Neurobiol. Dis. 2020, 142, 104958. [Google Scholar] [CrossRef]
- Hachinski, V.; Iadecola, C.; Petersen, R.C.; Breteler, M.M.; Nyenhuis, D.L.; Black, S.E.; Powers, W.J.; DeCarli, C.; Merino, J.G.; Kalaria, R.N.; et al. National Institute of Neurological Disorders and Stroke–Canadian stroke network vascular cognitive impairment harmonization standards. Stroke 2006, 37, 2220–2241. [Google Scholar] [CrossRef] [PubMed]
- Craufurd, D.; MacLeod, R.; Frontali, M.; Quarrell, O.; Bijlsma, E.K.; Davis, M.; Hjermind, L.E.; Lahiri, N.; Mandich, P.; Martinez, A.; et al. Diagnostic genetic testing for Huntington’s disease. Pract. Neurol. 2015, 15, 80–84. [Google Scholar] [CrossRef]
- Clayton, E.W. How much control do children and adolescents have over genomic testing, parental access to their results, and parental communication of those results to others? J. Law Med. Ethics 2015, 43, 538–544. [Google Scholar] [CrossRef]
- MacLeod, R.; Tibben, A.; Frontali, M.; Evers-Kiebooms, G.; Jones, A.; Martinez-Descales, A.; Roos, R.A.; Editorial Committee; Working Group ‘Genetic Testing Counselling’ of the European Huntington Disease Network. Recommendations for the predictive genetic test in Huntington’s disease. Clin. Genet. 2013, 83, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Botkin, J.R.; Belmont, J.W.; Berg, J.S.; Berkman, B.E.; Bombard, Y.; Holm, I.A.; Levy, H.P.; Ormond, K.E.; Saal, H.M.; Spinner, N.B.; et al. Points to consider: Ethical, legal, and psychosocial implications of genetic testing in children and adolescents. Am. J. Hum. Genet. 2015, 97, 6–21. [Google Scholar] [CrossRef] [PubMed]
- Uhlmann, W.R.; Roberts, J.S. Ethical issues in neurogenetics. In Handbook of Clinical Neurology; Geschwind, D.H., Paulson, H.L., Klein, C., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 147, pp. 23–36. [Google Scholar]
- Huntington, G. On chorea. In The Medical and Surgical Reporter of Philadelphia; S.W. Butler: Philadelphia, PA, USA, 1872; Volume 26, pp. 317–321. [Google Scholar]
- Huntington, G. On chorea. J. Neuropsychiatry Clin. Neurosci. 2003, 15, 109–112. [Google Scholar] [CrossRef]
- MacDonald, M.E.; Ambrose, C.M.; Duyao, M.P.; Myers, R.H.; Lin, C.; Srinidhi, L.; Barnes, G.; Taylor, S.A.; James, M.; Groot, N.; et al. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell 1993, 72, 971–983. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Grounded Theory Procedures and Techniques, 3rd ed.; Sage: Newcastle upon Tyne, UK, 2008. [Google Scholar]
- Miles, M.B.; Huberman, A.M. Qualitative Data Analysis: An Expanded Sourcebook; Sage Publications: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Gilbert, J.K.; Watts, D.M. Concepts, misconceptions and alternative conceptions: Changing perspectives in science education. Stud. Sci. Educ. 1983, 10, 61–98. [Google Scholar] [CrossRef]
- Saldaña, J. The Coding Manual for Qualitative Researchers; SAGE Publications Inc.: Newcastle upon Tyne, UK, 2016. [Google Scholar]
- O’Connor, C.; Joffe, H. Intercoder reliability in qualitative research: Debates and practical guidelines. Int. J. Qual. Methods 2020, 19, 1609406919899220. [Google Scholar] [CrossRef]
- Trundle, K.C.; Atwood, R.K.; Christopher, J.E. Preservice elementary teachers’ conceptions of moon phases before and after instruction. J. Res. Sci. Teach. Off. J. Natl. Assoc. Res. Sci. Teach. 2002, 39, 633–658. [Google Scholar] [CrossRef]
- Newman, D.L.; Snyder, C.W.; Fisk, J.N.; Wright, L.K. Development of the central dogma concept inventory (CDCI) assessment tool. CBE Life Sci. Educ. 2016, 15, ar9. [Google Scholar] [CrossRef] [PubMed]
- Murray-Nseula, M. Incorporating case studies into an undergraduate genetics course. J. Scholarsh. Teach. Learn. 2011, 11, 75–85. [Google Scholar]
- Shaw, K.R.M.; Van Horne, K.; Zhang, H.; Boughman, J. Essay contest reveals misconceptions of high school students in genetics content. Genetics 2008, 178, 1157–1168. [Google Scholar] [CrossRef] [PubMed]
- Persky, A.M.; Robinson, J.D. Moving from novice to expertise and its implications for instruction. Am. J. Pharm. Educ. 2017, 81, 6065. [Google Scholar] [CrossRef] [PubMed]
- Nicklen, P.; Keating, J.L.; Paynter, S.; Storr, M.; Maloney, S. Remote-online case-based learning: A comparison of remote-online and face-to-face, case-based learning-a randomized controlled trial. Educ. Health 2016, 29, 195. [Google Scholar]
- Raupach, T.; Muenscher, C.; Anders, S.; Steinbach, R.; Pukrop, T.; Hege, I.; Tullius, M. Web-based collaborative training of clinical reasoning: A randomized trial. Med. Teach. 2009, 31, e431–e437. [Google Scholar] [CrossRef]
- Dennis, J. Problem-based learning in online vs. face-to-face environments. Educ. Health Chang. Learn. Pract. 2003, 16, 198. [Google Scholar] [CrossRef]
- Taradi, S.K.; Taradi, M.; Radić, K.; Pokrajac, N. Blending problem-based learning with Web technology positively impacts student learning outcomes in acid-base physiology. Adv. Physiol. Educ. 2005, 29, 35–39. [Google Scholar] [CrossRef]
- Thompson, K.L.; Gendreau, J.L.; Strickling, J.E.; Young, H.E. Cadaveric dissection in relation to problem-based learning case sequencing: A report of medical student musculoskeletal examination performances and self-confidence. Anat. Sci. Educ. 2019, 12, 619–626. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gender | Number of Students (Out of n = 19) | Percentage of Students |
| Female | 11 | 57.9% |
| Male | 8 | 42.1% |
| Race | Number of Students (Out of n = 19) | Percentage of Students |
| White | 16 | 84.2% |
| Asian | 2 | 10.5% |
| Other or unknown | 1 | 5.2% |
| Year | Number of Students (Out of n = 19) | Percentage of Students |
|---|---|---|
| Second Year | 6 | 31.6% |
| Third Year | 5 | 26.3% |
| Fourth Year | 7 | 36.8% |
| Graduate Student | 1 | 5.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharp, K.A.; Krall, R.M.; Chalfant, J. Deepening Undergraduate Students’ Thinking about Central Dogma through Problem-Based Learning. Educ. Sci. 2023, 13, 854. https://doi.org/10.3390/educsci13090854
Sharp KA, Krall RM, Chalfant J. Deepening Undergraduate Students’ Thinking about Central Dogma through Problem-Based Learning. Education Sciences. 2023; 13(9):854. https://doi.org/10.3390/educsci13090854
Chicago/Turabian StyleSharp, Katherine Alberta, Rebecca McNall Krall, and Jeffrey Chalfant. 2023. "Deepening Undergraduate Students’ Thinking about Central Dogma through Problem-Based Learning" Education Sciences 13, no. 9: 854. https://doi.org/10.3390/educsci13090854