

Health Education Intervention Programs in Early Childhood Education: A Systematic Review

 ,
,
Abstract
:1. Introduction
1.1. Health Education in Early Childhood
1.2. Aims
- In which areas of health education has intervention been conducted among 3–6-year-old children?
- How holistic is the approach to health education and health promotion in the applied intervention program?
- In what institutional environment are the intervention programs implemented?
- What kind of methods are used during the intervention programs?
- What are the achieved outcomes of applied interventions related to the health education of 3–6-year-old children? To what extent can these programs be considered effective?
- What are the issues that require further exploration?
2. Materials and Methods
2.1. Eligibility Criteria
- peer-reviewed empirical studies written in English language;
- studies focused on health education or health promotion aimed at 3–6-year-old children in an institutional environment (kindergarten, preschool or other ECEC institution);
- studies based on intervention with outcomes related to children.
- Studies were excluded from the analysis if the following conditions were present:
- the full text was not available;
- types of papers were any of the following: systematic or other reviews, study protocols, pilot studies, secondary analysis, content or document analysis, policy papers, validation of measuring tools without any results;
- studies aimed at parents or professionals working with children (educators, health care professionals, etc.)
- public health programs and measures or programs implemented in the framework of a long-term international project;
- infrastructural development without pedagogical intervention
- studies related to children with acute or chronic diseases or with special educational needs;
- programs supporting healthy development (e.g., development of cognitive or motor skills).
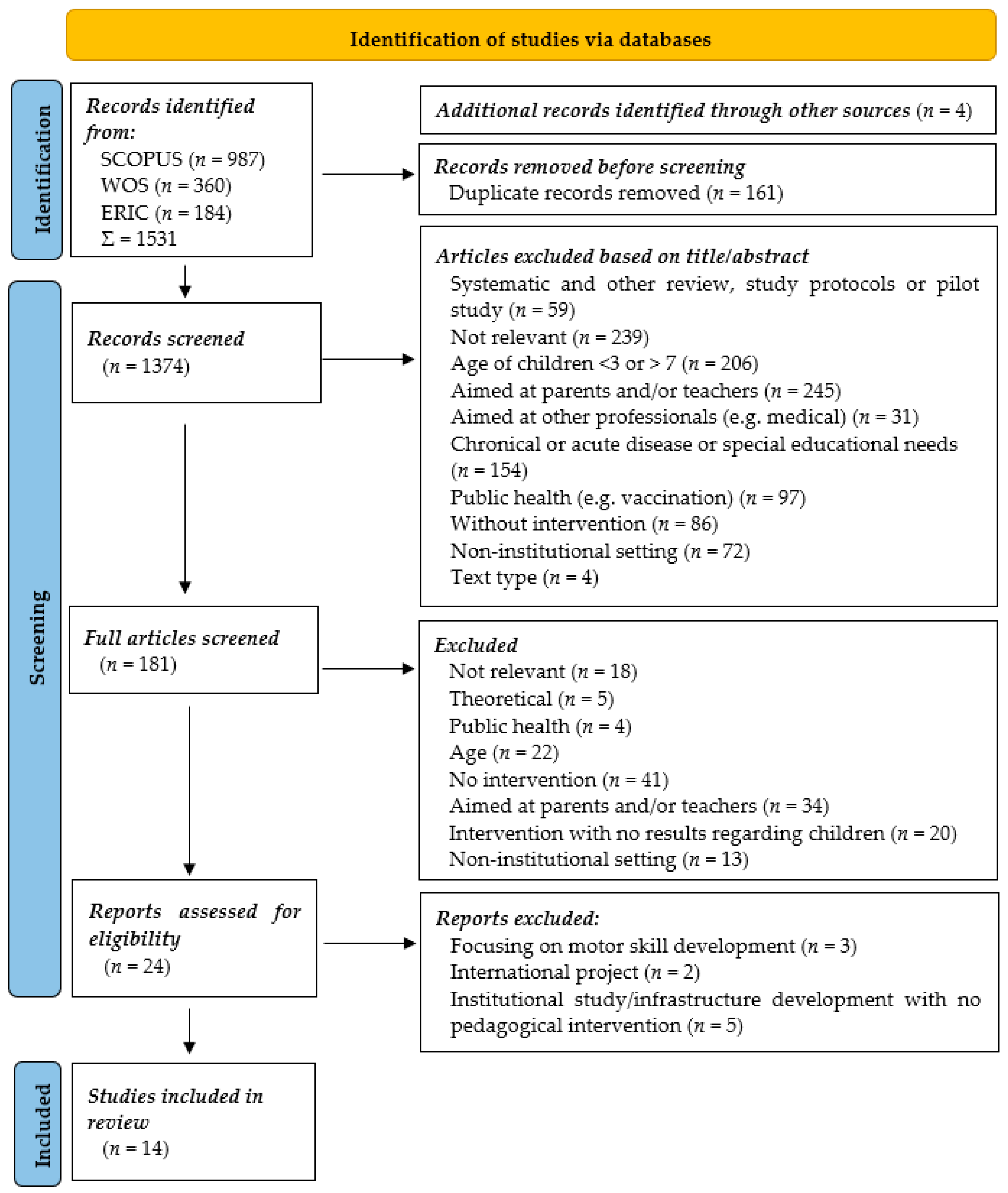
2.2. Information Sources
2.3. Selection Process
3. Results
3.1. Characteristics of Included Studies
3.2. Health Education Fields Examined in the Interventions
3.2.1. Physical Activity
3.2.2. Nutrition
3.2.3. Physical Activity and Nutrition
3.2.4. Nasal Hygiene
3.2.5. Smoking Prevention
3.2.6. Oral Health
3.3. Methods and Tools of the Interventions Studied
3.4. Quality Assessment
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD. Health at a Glance 2021: OECD Indicators; OECD Publishing: Paris, France, 2022. [Google Scholar] [CrossRef]
- WHO. World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Paris, France, 2022; Available online: https://cdn.who.int/media/docs/default-source/gho-documents/world-health-statistic-reports/worldhealthstatistics_2022.pdf (accessed on 25 June 2023).
- Fináncz, J.; Podráczky, J.; Nyitrai, Á.; Csima, M. Az egészségműveltség vizsgálatának megalapozása a koragyermekkori nevelésben dolgozók körében [Establishing the foundations for health literacy assessment among early childhood educators.]. Új Pedagógiai Szle. 2021, 71, 19–38. Available online: http://upszonline.hu/index.php?article=711112007 (accessed on 20 April 2023).
- United Nations. Declaration of the United Nations Conference on the Human Environment. 1972. Available online: https://documents-dds-ny.un.org/doc/UNDOC/GEN/NL7/300/05/PDF/NL730005.pdf?OpenElement (accessed on 28 June 2023).
- United Nations. Report of the World Commission on Environment and Development. “Our Common Future” (Brundtland Report). 1987. Available online: https://digitallibrary.un.org/record/139811#record-files-collapse-header (accessed on 18 June 2023).
- Sustainable Development Solutions Network. Health in the Framework of Sustainable Development. Technical Report for the POST-2015 Agenda. 2014. Available online: https://irp-cdn.multiscreensite.com/be6d1d56/files/uploaded/Health-For-All-Report.pdf (accessed on 12 June 2023).
- World Health Organization. Mental Health Atlas 2020; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240036703 (accessed on 16 June 2023).
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 14 May 2022).
- OECD. Investing in High-Quality Early Childhood Education and Care (ECEC). 2012. Available online: https://www.oecd.org/education/school/48980282.pdf (accessed on 11 April 2023).
- Vandenbroeck, M.; Lenaerts, K.; Beblavý, M. Benefits of Early Childhood Education and Care and the Conditions for Obtaining Them; EENEE Analytical Report No. 32. Prepared for the European Commission; Publications Office of the European Union: Luxembourg, 2018; Available online: https://data.europa.eu/doi/10.2766/20810 (accessed on 22 May 2023).
- Ansari, A.; Pianta, R.C.; Whittaker, J.V.; Vitiello, V.E.; Ruzek, E.A. Starting Early: The Benefits of Attending Early Childhood Education Programs at Age 3. Am. Educ. Res. J. 2019, 56, 1495–1523. [Google Scholar] [CrossRef]
- Hochbaum, G. M: Health Behavior; Wadsworth Publishing Company: Belmont, CA, USA, 1970. [Google Scholar]
- Petosa, R.; Oldfield, D. A Pilot Study of the Impact of Stress Management Techniques on the Classroom Behavior of Elementary School Students. J. Sch. Health 1985, 55, 69–71. [Google Scholar] [CrossRef]
- Sofianopoulo, K.; Bacopoulou, F.; Vlachakis, D.; Kokka, I.; Alexopoulos, E.; Varvogli, L.; Chrousos, G.P.; Darviri, C. Stress Management in Elementary School Students: A Pilot Randomised Controlled Trial. EMBnet J. 2021, 26, e976. [Google Scholar] [CrossRef]
- Royer, N.; Moreau, C. A Survey of Canadian Early Childhood Educators’ Psychological Wellbeing at Work. Early Child. Educ. J. 2016, 44, 135–146. [Google Scholar] [CrossRef]
- Manning, M.; Garvis, S.; Fleming, C.; Wong, G.T. The relationship between teacher qualification and the quality of the early childhood education and care environment. Campbell Syst. Rev. 2017, 13, 1–82. [Google Scholar] [CrossRef]
- World Health Organization. Standards for Healthy Eating, Physical Activity, Sedentary Behaviour and Sleep in Early Childhood Education and Care Settings: A Toolkit; World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/rest/bitstreams/1376768/retrieve (accessed on 10 June 2023).
- Midcentral Public Health Service. Health and Safety Guidelines for Early Childhood Education Services. June 2014. Available online: https://www.midcentraldhb.govt.nz/HealthServices/PublicHealth/healthprotection/Documents/MidCentral%20Public%20Health%20Service%20Health%20and%20Safety%20Guidelines%20for%20ECE%20Services.pdf (accessed on 11 June 2023).
- Australian Government, Department of Health. National Action Plan for the Health of Children and Young People 2020–2030; Australian Government: Canberra, Australia, 2019. Available online: https://www.health.gov.au/sites/default/files/documents/2021/04/national-action-plan-for-the-health-of-children-and-young-people-2020-2030-national-action-plan-for-the-health-of-children-and-young-people-2020-2030.pdf (accessed on 11 June 2023).
- National Council of Educational Research and Training. Guidelines for Preschool Education; National Council of Educational Research and Training: New Delhi, India, 2020; Available online: https://ncert.nic.in/dee/pdf/guidelines-for-preschool.pdf (accessed on 14 June 2023).
- Lamanauskas, V.; Malinauskiené, D.; Augiené, D. Health Education in Pre-school Institution: Integration, Effectiveness, Improvement. Eurasia J. Math. Sci. Technol. Educ. 2021, 17, em2046. [Google Scholar] [CrossRef]
- 363/2012. (XII. 17.) Korm. Rendelet az Óvodai Nevelés Országos Alapprogramjáról [Government Decree on the National Core Programme for Kindergarten Education]. Available online: https://net.jogtar.hu/jogszabaly?docid=a1200363.kor (accessed on 11 November 2022).
- Gelbmann, C.; Dieminger-Schnürch, B.; Seper, K.; Simetzberger, S.; Klausmann, L. Qualitätsstandard für die Verpflegung im Kindergarten; Bundesministerium für Soziales, Gesundheit, Pflege und Konsumentenschutz (BMSGPK): Wien, Austria, 2022; Available online: https://www.fitkid-aktion.de/fileadmin/user_upload/medien/DGE-QST/DGE_Qualitaetsstandard_Kita.pdf (accessed on 17 June 2023).
- IN FORM—Deutschlands Initiative für Gesunde Ernährung und mehr Bewegung. DGE-Qualitätsstandard für die Verpflegung in Kitas, 6th ed.; Deutsche Gesellschaft für Ernährung: Bonn, Germany, 2022; Available online: https://www.fitkid-aktion.de/fileadmin/user_upload/medien/DGE-QST/DGE_Qualitaetsstandard_Kita.pdf (accessed on 14 June 2023).
- National Consensus for School Health Education. National Health Education Standards. In Model Guidance for Curriculum and Instruction, 3rd ed.; National Consensus for School Health Education: Atlanta, GA, USA, 2022; Available online: https://www.schoolhealtheducation.org/wp-content/uploads/2022/10/National_Health_Education_Standards_Guide-10.02.2022.pdf (accessed on 12 June 2023).
- Ontario Public Service. The Kindergarten Program; Ontario Public Service: Ontario, Canada, 2016; Available online: https://files.ontario.ca/books/edu_the_kindergarten_program_english_aoda_web_july21.pdf (accessed on 14 June 2023).
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/337001/9789240014886-eng.pdf (accessed on 11 May 2023).
- Loewenstein, G.; Price, J.; Volpp, K. Habit formation in children: Evidence from incentives for healthy eating. J. Health Econ. 2016, 45, 47–54. [Google Scholar] [CrossRef]
- Borges Rodrigues, S.; Parisod, H.; Barros, L.; Salanterä, S. Examining Empowerment Interventions with Families and Preschool Children: Systematic Review of Randomized Controlled Trials. Health Educ. Behav. 2022, 49, 358–377. [Google Scholar] [CrossRef]
- Chirico, F.; Capitanelli, I.; Bollo, M.; Ferrari, G.; Maran, D.A. Association between workplace violence and burnout syndrome among schoolteachers: A systematic review. J. Health Soc. Sci. 2021, 6, 187–208. [Google Scholar]
- Mytton, J.; Ingram, J.; Manns, S.; Thomas, J. Facilitators and barriers to engagement in parenting programs: A qualitative systematic review. Health Educ. Behav. 2014, 41, 127–137. [Google Scholar] [CrossRef]
- Szpunar, M.; Bruijns, B.; Tucker, P. Measuring Early Childhood Educators’ Physical Activity and Sedentary Behavior-Related Self-Efficacy: A Systematic Review of Tools. Health Educ. Behav. 2021, 48, 455–467. [Google Scholar] [CrossRef]
- Bramantoro, T.; Santoso, C.M.A.; Hariyani, N.; Setyowati, D.; Zulfiana, A.A.; Nor, N.A.M.; Nagy, A.; Pratamawari, D.N.P.; Irmalia, W.R. Effectiveness of the school-based oral health promotion programmes from preschool to high school: A systematic review. PLoS ONE 2021, 16, e0256007. [Google Scholar] [CrossRef]
- dos Santos, A.P.; Nadanovsky, P.; de Oliveira, B.H. A systematic review and meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the primary dentition of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 1–12. [Google Scholar] [CrossRef]
- Matvienko-Sikar, K.; Toomey, E.; Delaney, L.; Flannery, C.; McHugh, S.; McSharry, J.; Byrne, M.; Queally, M.; Heary, C.; Kearney, P.M. Behaviour change techniques and theory use in healthcare professional-delivered infant feeding interventions to prevent childhood obesity: A systematic review. Health Psychol. Rev. 2019, 13, 277–294. [Google Scholar] [CrossRef]
- Nekitsing, C.; Blundell-Birtill, P.; Cockroft, J.E.; Hetherington, M.M. Systematic review and meta-analysis of strategies to increase vegetable consumption in preschool children aged 2–5 years. Appetite 2018, 127, 138–154. [Google Scholar] [CrossRef]
- Sanchez-Flack, J.C.; Herman, A.; Buscemi, J.; Kong, A.; Bains, A.; Fitzgibbon, M.L. A systematic review of the implementation of obesity prevention interventions in early childcare and education settings using the RE-AIM framework. Transl. Behav. Med. 2020, 10, 1168–1176. [Google Scholar] [CrossRef]
- Vanderloo, L.M.; Martyniuk, O.J.; Tucker, P. Physical and Sedentary Activity Levels Among Preschoolers in Home-Based Childcare: A Systematic Review. J. Phys. Act. Health 2015, 12, 879–889. [Google Scholar] [CrossRef]
- Alamneh, Y.M.; Adane, F. Magnitude and Predictors of Pneumonia among Under-Five Children in Ethiopia: A Systematic Review and Meta-Analysis. J. Environ. Public Health 2020, 2020, 1606783. [Google Scholar] [CrossRef]
- Szkwarko, D.; Hirsch-Moverman, Y.; Du Plessis, L.; Du Preez, K.; Carr, C.; Mandalakas, A.M. Child contact management in high tuberculosis burden countries: A mixed-methods systematic review. PLoS ONE 2017, 12, e0182185. [Google Scholar] [CrossRef]
- Systematic Review-Research Guide. Available online: https://libguides.murdoch.edu.au/systematic/PICO (accessed on 18 November 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 9, 2. [Google Scholar] [CrossRef]
- Braga-Pontes, C.; Simões-Dias, S.; Lages, M.; Guarino, M.P.; Graça, P. Nutrition education strategies to promote vegetable consumption in preschool children: The Veggies4myHeart project. Public Health Nutr. 2022, 25, 1061–1070. [Google Scholar] [CrossRef]
- Costa, P.; Ermini, T.; Sigaud, C.H.S. Effects of an educational playful intervention on nasal hygiene behaviors of preschoolers: A quasi-experimental study. Health Promot. Perspect. 2019, 9, 50–54. [Google Scholar] [CrossRef]
- de Droog, S.M.; Buijzen, M.; Valkenburg, P.M. Enhancing children’s vegetable consumption using vegetable-promoting picture books. The impact of interactive shared reading and character-product congruence. Appetite 2014, 73, 73–80. [Google Scholar] [CrossRef]
- Fastring, D.; Keel, K.; Colby, D.; Conner, J.M.; Hilbert, A. Head Start Centers Can Influence Healthy Behaviors: Evaluation of a Nutrition and Physical Activity Educational Intervention. J. Sch. Health 2019, 89, 698–704. [Google Scholar] [CrossRef]
- Kim, S.; Kim, H. Effectiveness of smoking prevention programs for preschool children in South Korea at post intervention. Child. Youth Serv. Rev. 2019, 101, 80–86. [Google Scholar] [CrossRef]
- Kobel, S.; Wirt, T.; Schreiber, A.; Kesztyüs, D.; Kettner, S.; Erkelenz, N.; Wartha, O.; Steinacker, J.M. Intervention Effects of a School-Based Health Promotion Programme on Obesity Related Behavioural Outcomes. J. Obes. 2014, 2014, 476230. [Google Scholar] [CrossRef]
- Kornilaki, E.N.; Skouteris, H.; Morris, H. Developing connections between healthy living and environmental sustainability concepts in Cretan preschool children: A randomized trial. Early Child Dev. Care 2021, 192, 1685–1698. [Google Scholar] [CrossRef]
- Min, J.; Kim, G.; Lim, H.; Carvajal, N.A.; Lloyd, C.W.; Wang, Y. A kindergarten-based child health promotion program: The Adapted National Aeronautics and Space Administration (NASA) Mission X for improving physical fitness in South Korea. Glob. Health Promot. 2019, 26, 52–61. [Google Scholar] [CrossRef]
- O’Dwyer, M.V.; Fairclough, S.J.; Ridgers, N.D.; Knowles, Z.R.; Foweather, L.; Stratton, G. Effect of a school-based active play intervention on sedentary time and physical activity in preschool children. Health Educ. Res. 2013, 28, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Palmer, K.K.; Webster, E.K.; Logan, S.W.; Chinn, K.M. The Effect of CHAMP on Physical Activity and Lesson Context in Preschoolers: A Feasibility Study. Res. Q. Exerc. Sport. 2018, 89, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.R.; Acharya, S.; Rao, J.C. School Interventions-based Prevention of Early-Childhood Caries among 3-5-year-old children from very low socioeconomic status: Two-year randomized trial. J. Public Health Dent. 2020, 80, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Schindler, J.M.; Corbett, D.; Forestell, C.A. Assessing the effect of food exposure on children’s identification and acceptance of fruit and vegetables. Eat. Behav. 2013, 14, 53–56. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Hennink-Kaminski, H.; Moore, R.; Burney, R.; Chittams, J.L.; Parker, P.; Luecking, C.T.; Hales, D.; Ward, D.S. Evaluating a child care-based social marketing approach for improving children’s diet and physical activity: Results from the Healthy Me, Healthy We cluster-randomized controlled trial. Transl. Behav. Med. 2021, 7, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, N.; Harris, N.; Lee, P. Lifestyle knowledge and preferences in preschool children: Evaluation of the Get up and Grow healthy lifestyle education programme. Health Educ. J. 2016, 75, 1012–1024. [Google Scholar] [CrossRef]
- A Guide to Evidence Synthesis: 9. Risk of Bias Assessment. Available online: https://guides.library.cornell.edu/evidencesynthesis/bias (accessed on 8 May 2023).
- RoB 2 for Cluster-Randomized Trials. Available online: https://www.riskofbias.info/welcome/rob-2-0-tool/rob-2-for-cluster-randomized-trials (accessed on 14 May 2023).
- ROBINS-I Tool (Risk of Bias in Non-randomized Studies—Of Interventions). Available online: https://www.riskofbias.info/welcome/home (accessed on 14 May 2023).
- Revised Cochrane Risk of Bias Tool for Randomized Trials (RoB 2.0). Available online: https://www.riskofbias.info/welcome/rob-2-0-tool/archive-rob-2-0-2016 (accessed on 14 May 2023).
- Gao, W.; Zhang, Y.; Wu, D.; Dong, Y.; Liu, N.; Wang, H. Compliance with Health-Related Behaviors Guidelines and Its Relationship with Multiple Factors in Preschool Children Aged 3–6 Years: A National Cross-Sectional Survey in China. Int. J. Environ. Res. Public Health 2022, 23, 1262. [Google Scholar] [CrossRef]
- De Craemer, M.; Verbestel, V.; Cardon, G.; Androutsos, O.; Manios, Y.; Chastin, S. Correlates of Meeting the Physical Activity, Sedentary Behavior, and Sleep Guidelines for the Early Years among Belgian Preschool Children: The ToyBox-Study. Int. J. Environ. Res. Public Health 2020, 24, 7006. [Google Scholar] [CrossRef]
- Sterdt, E.; Pape, N.; Kramer, S.; Liersch, S.; Urban, M.; Werning, R.; Walter, U. Do children’s health resources differ according to preschool physical activity programmes and parental behaviour? A mixed methods study. Int. J. Environ. Res. Public Health 2014, 26, 2407–2426. [Google Scholar] [CrossRef]
- Felix, E.; Silva, V.; Caetano, M.; Ribeiro, M.V.V.; Fidalgo, T.M.; Rosa Neto, F.; Sanchez, Z.M.; Surkan, P.J.; Martins, S.S.; Caetano, S.C. Excessive Screen Media Use in Preschoolers Is Associated with Poor Motor Skills. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 418–425. [Google Scholar] [CrossRef]
- Vanderloo, L.M.; Tucker, P. Physical activity and sedentary time among young children in full-day kindergarten: Comparing traditional and balanced day schedules. Health Educ. J. 2017, 76, 29–37. [Google Scholar] [CrossRef]
- Vanderloo, L.M.; Tucker, P.; Johnson, A.M.; van Zandvoort, M.M.; Burke, S.M.; Irwin, J.D. The influence of centre-based childcare on preschoolers’ physical activity levels: A cross-sectional study. Int. J. Environ. Res. Public Health 2014, 5, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Myers, G.; Wright, S.; Blane, S.; Pratt, I.S.; Pettigrew, S. A process and outcome evaluation of an in-class vegetable promotion program. Appetite 2018, 125, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Rasmus, K.; Toratti, A.; Karki, S.; Pesonen, P.; Laitala, M.L.; Anttonen, V. Acceptability of a Mobile Application in Children’s Oral Health Promotion-A Pilot Study. Int. J. Environ. Res. Public Health 2021, 22, 3256. [Google Scholar] [CrossRef]
- Roberts-Gray, C.; Sweitzer, S.J.; Ranjit, N.; Potratz, C.; Rood, M.; Romo-Palafox, M.J.; Byrd-Williams, C.E.; Briley, M.E.; Hoelscher, D.M. Structuring Process Evaluation to Forecast Use and Sustainability of an Intervention: Theory and Data From the Efficacy Trial for Lunch Is in the Bag. Health Educ. Behav. 2017, 44, 559–569. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, Z.; Yang, M.; Wang, F.; Xiao, S. Reducing environmental tobacco smoke exposure of preschool children: A randomized controlled trial of class-based health education and smoking cessation counseling for caregivers. Int. J. Environ. Res. Public Health 2015, 12, 692–709. [Google Scholar] [CrossRef]
- Leidner, A.J.; Maughan, E.D.; Bjork, A.; Black, C.; Mazyck, D.; Underwood, J.M. Vaccination-Related Activities at Schools With Kindergartners: Evidence From a School Nurse Survey. J. Sch. Nurs. 2020, 36, 464–471. [Google Scholar] [CrossRef]
- Lee, B.; Kim, Y.E. Factor Structure and Validation of the 12-Item Korean Version of the General Health Questionnaire in a Sample of Early Childhood Teachers. Educ. Sci. 2021, 11, 243. [Google Scholar] [CrossRef]
- Bundy, A.; Engelen, L.; Wyver, S.; Tranter, P.; Ragen, J.; Bauman, A.; Baur, L.; Schiller, W.; Simpson, J.M.; Niehues, A.N.; et al. Sydney Playground Project: A Cluster-Randomized Trial to Increase Physical Activity, Play, and Social Skills. J. Sch. Health 2017, 87, 751–759. [Google Scholar] [CrossRef]
- Sando, O.J.; Mehus, N. Supportive indoor environments for functional play in ECEC institutions: A strategy for promoting well-being and physical activity? Early Child Dev. Care 2021, 191, 921–932. [Google Scholar] [CrossRef]
- Appel, J.M.; Fullerton, K.; Hennessy, E.; Korn, A.R.; Tovar, A.; Allender, S.; Hovmand, P.S.; Kasman, M.; Swinburn, B.A.; Hammond, R.A.; et al. Design and methods of Shape Up Under 5: Integration of systems science and community-engaged research to prevent early childhood obesity. PLoS ONE 2019, 1, e0220169. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.Y.; Leung, K.M.; Tam, W.W.; Lee, A. Varicella vaccine uptake and associated factors in children in Hong Kong. Epidemiol. Infect. 2014, 142, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Calle-Bustos, A.M.; Juan, M.C.; García-García, I.; Abad, F. An augmented reality game to support therapeutic education for children with diabetes. PLoS ONE 2017, 28, e0184645. [Google Scholar] [CrossRef] [PubMed]
- Noordam, A.C.; Carvajal-Velez, L.; Sharkey, A.B.; Young, M.; Cals, J.W. Care seeking behaviour for children with suspected pneumonia in countries in sub-Saharan Africa with high pneumonia mortality. PLoS ONE 2015, 23, e0117919. [Google Scholar] [CrossRef]
- Milgramm, A.; Corona, L.L.; Janicki-Menzie, C.; Christodulu, K.V. Community-based Parent Education for Caregivers of Children Newly Diagnosed with Autism Spectrum Disorder. J. Autism Dev. Disord. 2022, 52, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Sigmundsson, H.; Haga, M. Motor competence is associated with physical fitness in four- to six-year-old preschool children. Eur. Early Child. Educ. Res. J. 2016, 24, 477–488. [Google Scholar] [CrossRef]
- Ruiz-Esteban, C.; Terry Andrés, J.; Méndez, I.; Morales, Á. Analysis of Motor Intervention Program on the Development of Gross Motor Skills in Preschoolers. Int. J. Environ. Res. Public Health 2020, 7, 4891. [Google Scholar] [CrossRef]
- Ngololo Kamara, E.; Kasanda, C.; Van Rooy, G. Provision of Integrated Early Childhood Development in Namibia: Are We on the Right Track? Educ. Sci. 2018, 8, 117. [Google Scholar] [CrossRef]
- Delaney, T.; Jackson, J.K.; Jones, J.; Hall, A.; Dives, A.; Wedesweiler, T.; Campbell, L.; Nathan, N.; Romiti, M.; Trost, S.G.; et al. A Cluster Randomised Controlled Trial of an Intervention to Increase Physical Activity of Preschool-Aged Children Attending Early Childhood Education and Care: Study Protocol for the ‘Everybody Energise’ Trial. Int. J. Environ. Res. Public Health 2019, 4, 4275. [Google Scholar] [CrossRef]
- Mooses, K.; Mäestu, J.; Riso, E.M.; Hannus, A.; Mooses, M.; Kaasik, P.; Kull, M. Different Methods Yielded Two-Fold Difference in Compliance with Physical Activity Guidelines on School Days. PLoS ONE 2016, 25, e0152323. [Google Scholar] [CrossRef]
- Lee, R.E.; Szeszulski, J.; Lorenzo, E.; Arriola, A.; Bruening, M.; Estabrooks, P.A.; Hill, J.L.; O’Connor, T.M.; Shaibi, G.Q.; Soltero, E.G.; et al. Sustainability via Active Garden Education: The Sustainability Action Plan Model and Process. Int. J. Environ. Res. Public Health 2022, 1, 5511. [Google Scholar] [CrossRef] [PubMed]
- Farewell, C.V.; Maiurro, E.; Powers, J.; Puma, J. The Healthy Environment Project: Promoting sustainable change in early childhood education settings. Health Educ. J. 2021, 80, 472–486. [Google Scholar] [CrossRef]
- Latomme, J.; Cardon, G.; De Bourdeaudhuij, I.; Iotova, V.; Koletzko, B.; Socha, P.; Moreno, L.; Androutsos, O.; Manios, Y.; De Craemer, M.; et al. Effect and process evaluation of a kindergarten-based, family-involved intervention with a randomized cluster design on sedentary behaviour in 4- to 6-year old European preschool children: The ToyBox-study. PLoS ONE 2017, 5, e0172730. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Huang, Y.; Zhang, Y.; Liu, F.; Feng, C.X.; Liu, T.; Li, C.; Ling, D.D.; Mu, Y.; Tarver, S.L.; et al. Evaluation of fast food behavior in pre-school children and parents following a one-year intervention with nutrition education. Int. J. Environ. Res. Public Health 2014, 30, 6780–6790. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, L.D.; Nadler, C.; Hepburn, S.; Rosenberg, S.; Reynolds, A.; Zubler, J. Toileting Resistance Among Preschool-Age Children with and Without Autism Spectrum Disorder. J. Dev. Behav. Pediatr. 2022, 1, 216–223. [Google Scholar] [CrossRef]
- Zhou, N.; Wong, H.M.; McGrath, C. Social story-based oral health promotion for preschool children with special healthcare needs: A 24-month randomized controlled trial. Community Dent. Oral Epidemiol. 2020, 48, 415–422. [Google Scholar] [CrossRef]
- Feng, D.; Song, H.; Esperat, M.C.; Black, I. A Multicomponent Intervention Helped Reduce Sugar-Sweetened Beverage Intake in Economically Disadvantaged Hispanic Children. Am. J. Health Promot. 2016, 30, 594–603. [Google Scholar] [CrossRef]
- Rathnayake, N.; De Silva Weliange, S.; Guruge, G.N.D. Effectiveness of a health promotion intervention to address determinants of child neglect in a disadvantaged community in Sri Lanka. J. Health Popul. Nutr. 2021, 8, 48. [Google Scholar] [CrossRef]
- López-Banet, L.; Miguélez Rosique, J.A.; Martínez-Carmona, M.; Ayuso Fernández, G.E. Development of Food Competence in Early Childhood Education. Educ. Sci. 2022, 12, 64. [Google Scholar] [CrossRef]
- Palmer, K.K.; Farquhar, J.M.; Chinn, K.M.; Robinson, L.E. Are Gross Motor Skill Interventions an Equitable Replacement for Outdoor Free Play Regarding Children’s Physical Activity? Am. J. Health Promot. 2022, 36, 643–650. [Google Scholar] [CrossRef]
- Chuang, R.J.; Sharma, S.V.; Perry, C.; Diamond, P. Does the CATCH Early Childhood Program Increase Physical Activity Among Low-Income Preschoolers?—Results From a Pilot Study. Am. J. Health Promot. 2018, 32, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, T.; Quissell, D.O.; Henderson, W.G.; Thomas, J.F.; Bryant, L.L.; Braun, P.A.; Albino, J.E. Factors Associated with Oral Health Status in American Indian Children. J. Racial Ethn. Health Disparities 2014, 1, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Sokal-Gutierrez, K.; Chung, K.; Lin, W.; Khanh, L.N.; Chung, R.; Hoang, H.T.; Ivey, S.L. Maternal and Child Nutrition and Oral Health in Urban Vietnam. Int. J. Environ. Res. Public Health 2019, 19, 2579. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Grace, R.; Elcombe, E.; Villarosa, A.R.; Mack, H.A.; Kemp, L.; Ajwani, S.; Wright, D.C.; Anderson, C.; Bucknall, N.; et al. The oral health behaviours and fluid consumption practices of young urban Aboriginal preschool children in south-western Sydney, New South Wales, Australia. Health Promot. J. Austr. 2018, 29, 23–30. [Google Scholar] [CrossRef]


{kind=link}
| Author (Year) | Country | Title | Journal Source | Health Education Dimension | Study Population |
|---|---|---|---|---|---|
| Braga- Pontes et al. (2022) [44] | Portuguese | Nutrition education strategies to promote vegetable consumption in preschool children: the Veggies4myHeart project | Public Health Nutrition | nutrition | 3–6 years old children (n = 162) |
| Costa et al. (2019) [45] | Sao Paulo, Brazil | Effects of an educational playful intervention on nasal hygiene behaviors of preschoolers: a quasi-experimental study | Health Promotion Perspectives | nasal hygiene | 3–4 years old children (n = 39) |
| De Droog et al. (2014) [46] | Netherland | Enhancing children’s vegetable consumption using vegetable-promoting picture books. The impact of interactive shared reading and character–product congruence | Appetite | nutrition | 4–6 years old children (n = 160) |
| Fastring et al. (2019) [47] | Jackson County, USA | Head Start Centers Can Influence Healthy Behaviors: Evaluation of a Nutrition and Physical Activity Educational Intervention | The Journal of school health | physical activity, nutrition | 3–5 years old children (n = 434) |
| Kim & Kim (2019) [48] | South Korea | Effectiveness of smoking prevention programs for preschool children in South Korea at post intervention | Children and Youth Services Review | smoking prevention | 5–6 years old children (n = 652) |
| Kobel et al. (2019) [49] | South-west Germany | Intervention effects of a kindergarten-based health promotion program on obesity-related behavioral outcomes and BMI percentiles | Preventive Medicine Reports | physical activity, nutrition, screen media consumption | 3–4 years old children (n = 558) |
| Kornilaki et al. (2021) [50] | Crete, Greece | Developing connections between healthy living and environmental sustainability concepts in Cretan preschool children: a randomized trial | Early Child Development and Care | physical activity, nutrition, sustainability | 4–5 years old children (n = 329) |
| Min et al. (2019) [51] | South Korea | A kindergarten-based child health promotion program: the Adapted National Aeronautics and Space Administration (NASA) Mission X for improving physical fitness in South Korea | Global Health Promotion | physical activity | 5 years old children (n = 212) |
| O’Dwyer et al. (2013) [52] | England | Effect of a school-based active play intervention on sedentary time and physical activity in preschool children | Health Education Research | physical activity | 4–5 years old children (n = 240) |
| Robinson et al. (2018) [53] | Midwestern city, USA | The Effect of CHAMP on Physical Activity and Lesson Context in Preschoolers: A Feasibility Study | Research Quarterly for Exercise and Sport | physical activity | 3–4 years old children (n = 72) |
| Samuel et al. (2020) [54] | Chennai, India | School Interventions-based Prevention of Early Childhood Caries among 3–5-year-old children from very low socioeconomic status: Two-year randomized trial | Journal of public health dentistry | oral health | 3–5 years old children (n = 420) |
| Schindler et al. (2013) [55] | USA | Assessing the effect of food exposure on children’s identification and acceptance of fruit and vegetables | Eating Behaviors | nutrition | 5–6 years old children (n = 58) |
| Vaughn et al. (2021) [56] | North Carolina, USA | Evaluating a child care-based social marketing approach for improving children’s diet and physical activity: Results from the Healthy Me, Healthy We cluster-randomized controlled trial | Translational Behavioral Medicine | physical activity, nutrition | 3–4 years old children (n = 853) |
| Wiseman et al. (2016) [57] | South Brisbane, Australia | Lifestyle Knowledge and Preferences in Preschool Children: Evaluation of the “Get up and Grow” Healthy Lifestyle Education Program | Health Education Journal | physical activity nutrition | 3–5 years old children (n = 82) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fináncz, J.; Podráczky, J.; Deutsch, K.; Soós, E.; Bánfai-Csonka, H.; Csima, M. Health Education Intervention Programs in Early Childhood Education: A Systematic Review. Educ. Sci. 2023, 13, 988. https://doi.org/10.3390/educsci13100988
Fináncz J, Podráczky J, Deutsch K, Soós E, Bánfai-Csonka H, Csima M. Health Education Intervention Programs in Early Childhood Education: A Systematic Review. Education Sciences. 2023; 13(10):988. https://doi.org/10.3390/educsci13100988
Chicago/Turabian StyleFináncz, Judit, Judit Podráczky, Krisztina Deutsch, Evelin Soós, Henrietta Bánfai-Csonka, and Melinda Csima. 2023. "Health Education Intervention Programs in Early Childhood Education: A Systematic Review" Education Sciences 13, no. 10: 988. https://doi.org/10.3390/educsci13100988