Sport and Its Relationship with Oncology in Future Primary Education Teachers



Abstract
:1. Introduction
- -
- Employment of specific mind and body techniques and vice versa;
- -
- Integration of systematic exercises for the development of the healing process of mind and body;
- -
- Aiding the healing process of a patient to encourage individual recuperation [25].
- -
- Working sensitivity;
- -
- Shortening division between mind and body;
- -
- Increasing creativity;
- -
- Improving creativity;
- -
- Increasing working efficiency;
- -
- Developing bodily assertion to increase self-confidence;
- -
- Encouraging the improvement of learning (assimilation and flexibility for changing behaviors);
- -
- Improving and developing a broad, thoughtful, positive attitude and considering modifying it for the benefit of oneself and others;
- -
- Modify and be modified, analyze and be analyzed, criticize and be criticized;
- -
- Work on different technical aspects, which form this task.
- -
- Spatial orientation: the ability to continuously support the movement of the body, in relation to location;
- -
- Spatial structuring: the ability to learn how the distribution of space through the hierarchy of interaction between spaces, leading to the appreciation of independence, following elements, etc.;
- -
- Spatial organization: the ability to distribute the space based on the location and structure of the space;
- -
- Temporality: the concept derived from Arteaga, Viciana & Conde [33] as the way of reflecting on current affairs, as a result of the transformations or actions carried out, allowing division into:
- -
- Temporary spatial: concept of time and control of remarkable concepts in order to orient themselves in time.
- -
- Structuring and spatial organization: awareness of places of origin: order and time.
- -
- Corporal consciousness: Castañer [34] explains it as a mixture or addition, of body image and image of itself, it collects some concepts, as well;
- -
- Corporal image: Castañer [34] marks this concept of corporal image as limited for the physical character of a person, this need has one “Subjective Conception of typical body, parallel to the conception other people have of our body”.
- -
- Personal knowledge: this attempts to encourage the subject to understand him or herself, in relation to their opportunities, which are manifested through the whole body, creating a feeling of self-knowledge and a sense of self-realization of what he/she desires to achieve;
- -
- Interpersonal communication: obtaining relevant correspondence from a minimum of two people; This is divided into oral and non-oral communication;
- -
- Introspective communication: concerns the data provided by the individual on their internal self, of the various environments to which the data belongs. This could be established by either the internal world of the subject, the objectivity of each person (real) or the internal world of the subject, which they wish to determine; (invented).
2. Materials and Methods
- -
- The questionnaire was prepared with an operationalization table, taking into account dependent, independent and general objective variables and specific objectives. Six measures were established with a total of thirty-eight items;
- -
- First, we carried out a validation of content, with expert judgement and a pilot test. Second, an exploratory factor analysis was carried out to validate the construction of the questionnaire.
- -
- The dependent variables are perception, knowledge;
- -
- The independent variables are tumors, information, mass media.
3. Results
3.1. Construction Validity. (Exploratory Factor Analysis.)
3.2. Correlation Analysis
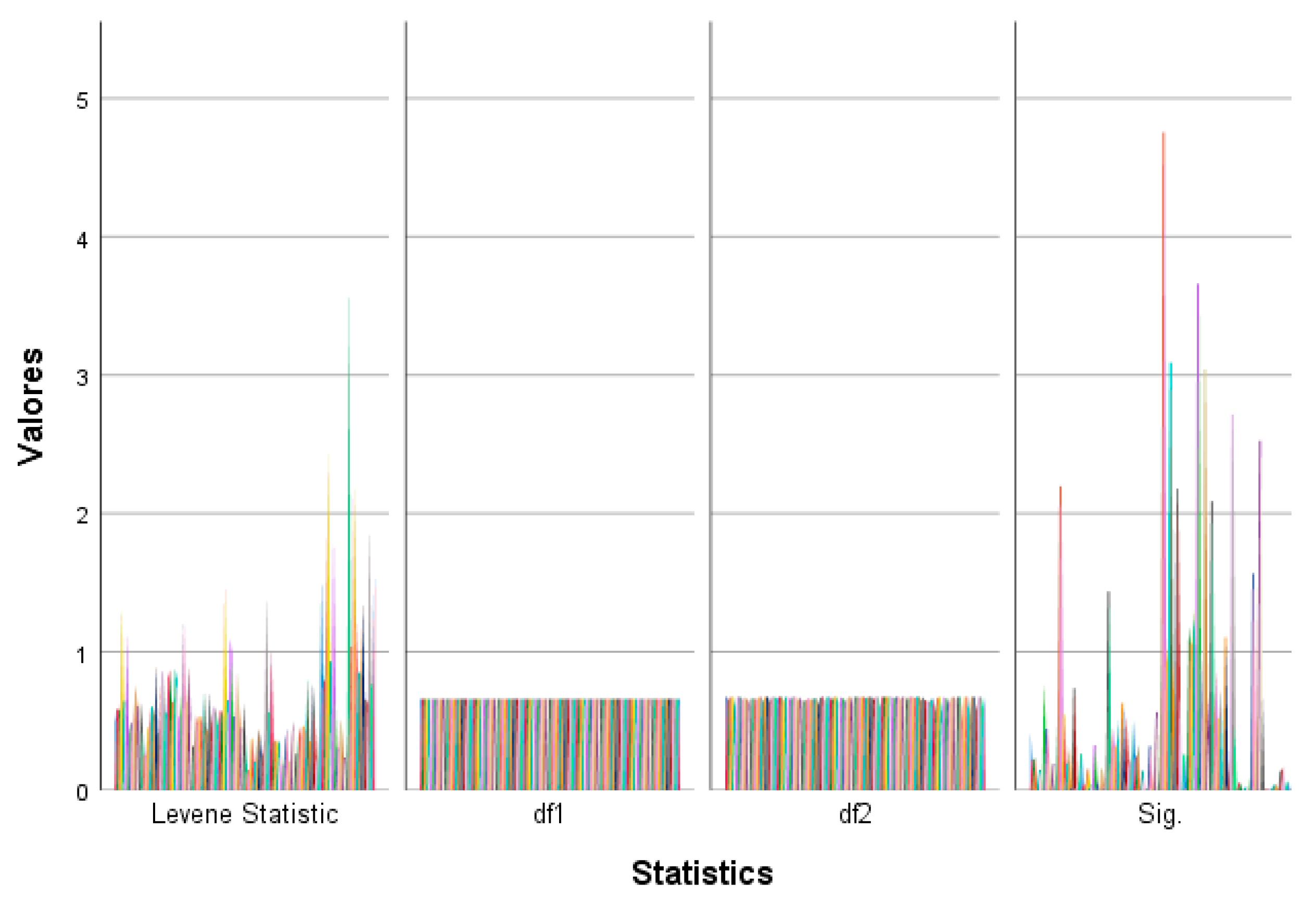
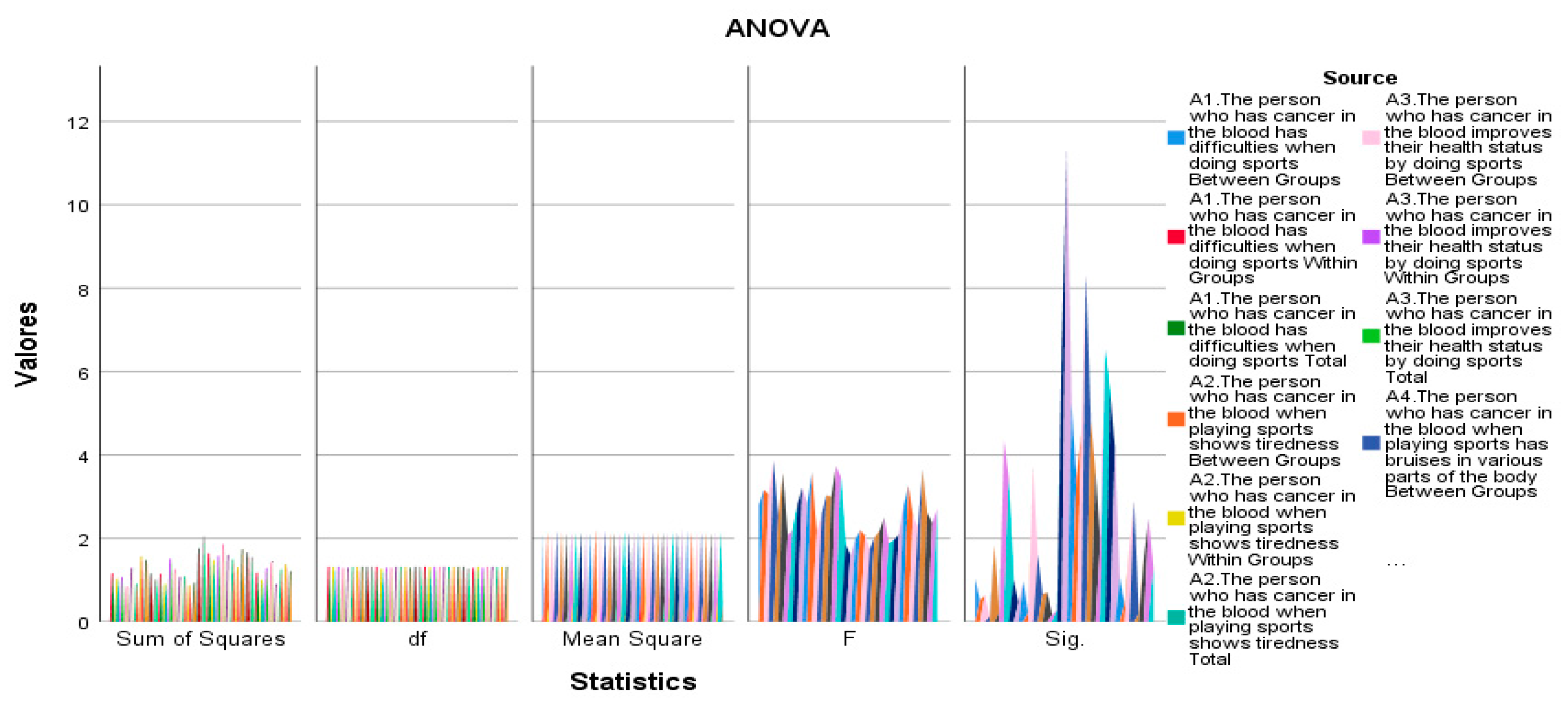
3.3. Hypothesis Contrast (ANOVA)
3.4. Descriptive Analysis.
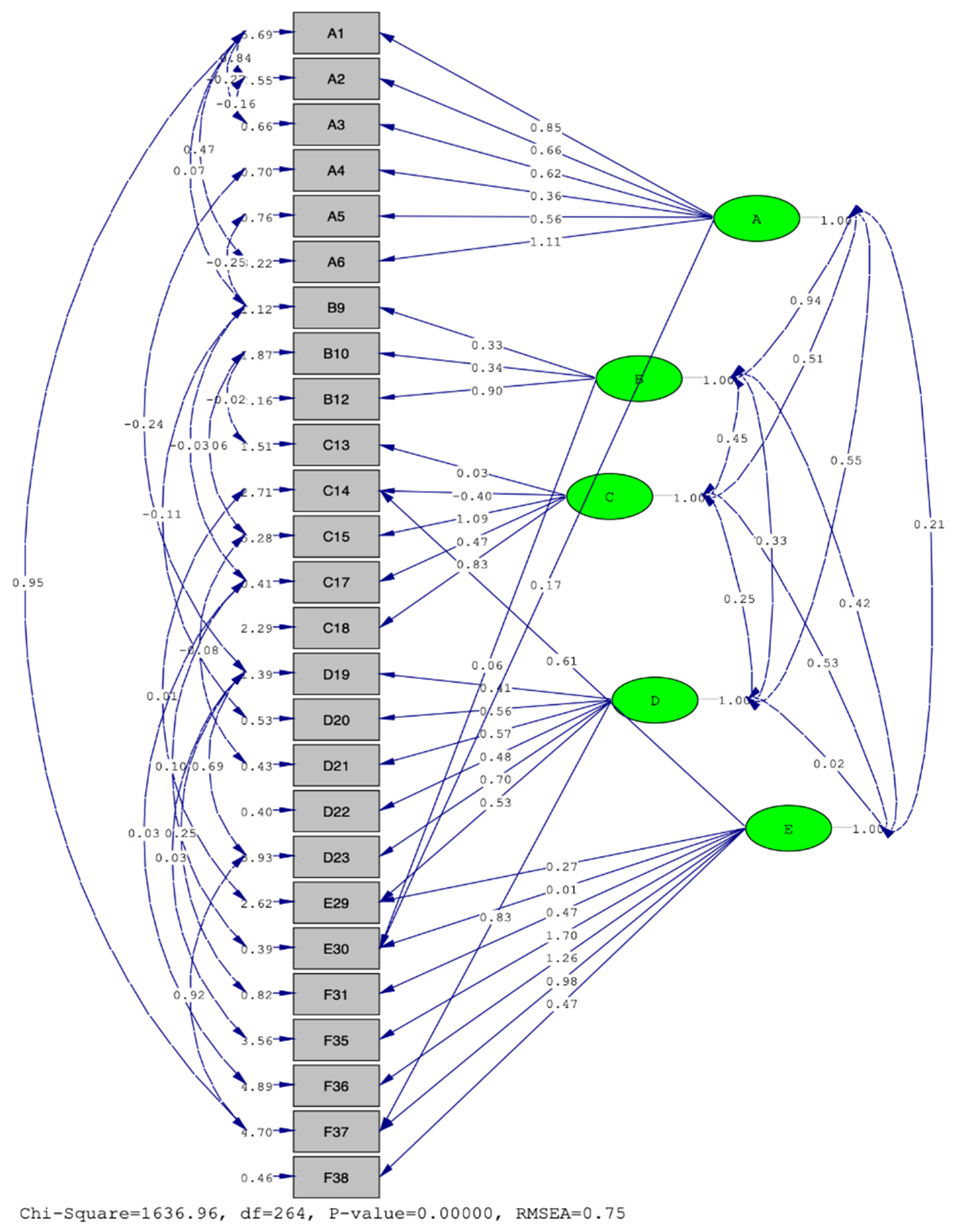
3.5. Confirmatory Factorial Analysis
- -
- Major influence of the latent variable on A6—The person with blood cancer has breathing difficulty.
- -
- Less influence of the latent variable on A4—The person with blood cancer has bruises in various parts of the body when playing sport.
- -
- Major influence of the latent variable on B12—The person with a bone tumor shows changes in behavior when playing sport.
- -
- Less influence of the latent variable on B9—The person with a bone tumor shows exhaustion when playing sport.
- -
- Major influence of the latent variable on C15—The person with a brain tumor is tired when playing sport.
- -
- Less influence of the latent variable on C14—The person with a brain tumor can play sport.
- -
- Major influence of the latent variable on D23—I would like to know more about oncology
- -
- Less influence of the latent variable on D19—I am interested in sports-related oncology topics.
- -
- Major influence of the latent variable on F35—Sport is good for your life.
- -
- Less influence of the latent variable on E30—I do not gather information from any particular medium.
- A–B (0.94), B–C (0.45), C–D (0.25), D–E (0.02)
- A–C (0.51), A–D (0.55), A–E (0.21), B–D (0.33), B–E (0.42), C–E (0.53)
- A (blood cancer and sport)–B (Bone tumor and sport)
- A (blood cancer and sport)–D (information of cancer and sport)
- D (cancer and sports information)–E (oncology and sports information media.)
- A (blood cancer and sport)–E (oncology and sports information media.)
- -
- -
- CFI compares the improvement in the fit of the model in comparison with an invalid model to evaluate the degree of loss, which occurs in the adjustment when changing from the proposed model to the invalid model [50]. To accept the proposed model, its value should be ≥0.95 and the resulting value is 0.058
- -
- RMSEA, among the indices based on the co-variances, the mean square error of approximation (RMSEA) was chosen. In this case the model would present an acceptable fit if the value was <0.07 [51]. The value we calculated in our model was 0.75.
- -
- NNFI reflects the proportion of total information explained by a model; because this index is not normalized, its values may adopt values outside the range of 0 and 1, a value of 0.97 seems to be more reasonable as an indication of good f model fit. The value we obtained is −0.16 [52].
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- García, I.F. Los programas de ayuda para la mejora de la convivencia en instituciones. Revista de pedagogía 2008, 60, 137–150. [Google Scholar]
- Blacklock, R.E.; Rhodes, R.E.; Brown, S.G. Relationship between regular walking, physical activity, and health-related quality of life. J. Phys. Act. Health 2007, 4, 138–152. [Google Scholar] [CrossRef] [PubMed]
- Candel, N.; Olmedilla, A.; Blas, A. Relaciones entre la práctica de actividad física y el autoconcepto, la ansiedad y la depresión en chicas adolescentes. Cuad. De Psicol. Del Deporte 2008, 8, 61–77. [Google Scholar]
- Martínez López, E.J.; Lozano, L.M.; Zagalaz, M.L.; Romero, S. Valoración y autoconcepto del alumnado con sobrepeso. Influencia de la escuela, actitudes sedentarias y de actividad física. Rev. Int. De Cienc. Del Deporte 2009, 17, 44–59. [Google Scholar]
- Almedom, A.; Glandon, D. Resilience is not the absence of PTSD anymore than health is the absence of disease. J. Loss Trauma 2007, 5, 127–143. [Google Scholar] [CrossRef]
- Fredrickson, B.L. Positivity: Discover the Ratio that Tips Your Life toward Flourishing; Three Rivers Press, New York: Crown, NY, USA, 2009; pp. 1–279. [Google Scholar]
- Lyubomirsky, S.; Dickerhoof, R. Handbook of Girls’ and Women’s Psychological Health; Worell, J., Goodheart, C.D., Eds.; Oxford University Press: New York, NY, USA, 2005; pp. 1–494. [Google Scholar]
- Steel, P.; Schmidt, J.; Shultz, J. Refining the relationship between personality and subjective well-being. Psychol. Bull. 2008, 134, 138–161. [Google Scholar] [CrossRef]
- Oliva, A.; Ríos, M.; Antolín, L.; Parra, A.; Hernando, A.; Pertegal, A. Más allá del déficit: Construyendo un modelo de desarrollo positivo adolescente. Infanc. Aprendiz. 2010, 33, 223–234. [Google Scholar] [CrossRef]
- Reina, C.; Oliva, A.; Parra, A. Percepciones de autoevaluación: Autoestima, autoeficacia y satisfacción vital en la adolescencia. Psychol. Soc. Educ. 2010, 2, 47–59. [Google Scholar] [CrossRef] [Green Version]
- García, P.L.R. Educación Física y Salud en Primaria: Hacia Una Educación Corporal Significativa y Autónoma; INDE. Publicaciones: Barcelona, Spain, 2006; pp. 1–266. [Google Scholar]
- Delgado, M.; Fernández, M.D.; Tercedor, P.; Sánchez, P.T. Estrategias de Intervención en Educación Para la Salud Desde la Educación Física; INDE. Publicaciones: Barcelona, Spain, 2002; pp. 1–211. [Google Scholar]
- Ferrer, M. Atención Educativa a Niños Oncológicos; Universidad de Zaragoza: Zaragoza, Spain, 2018; pp. 1–36. [Google Scholar]
- Cintra, O.; Balboa, Y. La actividad física: Un aporte para la salud. Lecturaas: Educación Física y Deportes 2011, 16, 159. [Google Scholar]
- Leiva, A.P.; Márquez, P.G.O.; Rodríguez, C.G.; Navas, J.M.M.; Bozal, R.G. Ejercicio físico y calidad de vida en estudiantes universitarios. Int. J. Dev. Educ. Psychol. 2017, 2, 437–446. [Google Scholar]
- Meneses Echávez, J.F.; González Jiménez, E.; Correa Bautista, J.E.; Valle, J.S.R.; Ramírez Vélez, R. Efectividad del ejercicio físico en la fatiga de pacientes con cáncer durante el tratamiento activo: Revisión sistemática y metaanálisis. Cad. De Saúde Pública 2015, 31, 667–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, P.W.N.; Braun, K.L. The effectiveness of dance interventions to improve older adults’ health: A systematic literature review. Altern. Ther. Health Med. 2015, 21, 1–64. [Google Scholar]
- Bohórquez Gómez-Millán, M.R.; Lorenzo Fernández, M.; García González, A.J. Actividad física como promotor del autoconcepto y la independencia personal en personas mayores. Rev. Iberoam. De Psicol. Del Ejerc. Y El Deporte Riped 2014, 9, 533–546. [Google Scholar]
- Zampieri, S.; Mosole, S.; Löfler, S.; Fruhmann, H.; Burggraf, S.; Cvečka, J.; Mayr, W. Ejercicio físico en el envejecimiento: Nueve semanas de press de piernas o entrenamiento de estimulación eléctrica en ancianos sedentarios de 70 años. Rev. Eur. De Miología Traslacional 2015, 25, 1–237. [Google Scholar]
- Savela, S.; Komulainen, P.; Sipilä, S.; Strandberg, T. Ikääntyneiden liikunta-minkälaista ja mihin tarkoitukseen? Duodecim 2015, 131, 1719–1725. [Google Scholar] [PubMed]
- Duclow, D. Williams James, Mind-Cure, and the Religion of Healthy-Mindedness. J. Relig. Health 2002, 41, 45–56. [Google Scholar] [CrossRef]
- Benson, H. The Science of Meditation. Psychol. Today 2001, 3, 56–60. [Google Scholar]
- Daleo, R. Are Relaxation tapes helpful for Young? Child Health Alert 1997, 15, 1–2. [Google Scholar]
- Jacobs, G. The Physiology of MindBody Interactions: The Stress Response and the Relaxation Response. J. Altern. Complementary Med. 2001, 7, 83–92. [Google Scholar] [CrossRef]
- Slanger, S.; Kushner, R. Mind/Body Medicine: An introduction for the Generalist Physician and Nutritionist. Nutr. Clin. Care 2001, 4, 256–264. [Google Scholar]
- Shang, C. Emerging Paradigms in Mind- Body Medicine. J. Altern. Complementary Med. 2001, 7, 83–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolsko, P.; Einsenberg, D.; Davis, R.; Phillips, R. Use of Mind-Body Medical Therapies. Result of a National Survey. J. Gene Intern. Med. 2004, 19, 43–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brehm, M.; Kampfe, C.H. Creative Dance Improvisation: Fostering Creative Expression, Group Cooperation, and Multiple Intelligences. In Proceedings of the Conference on Education, Beijing, China, 9–13 July 1997. [Google Scholar]
- Stokoe, P. La Expresión Corporal y el Niño; Ricordi Americana S.A.E.C: Buenos Aires, Argentina, 1967; pp. 1–112. [Google Scholar]
- Mays, D. Creative Dance. Prim. Educ. 2000, 6, 15–19. [Google Scholar]
- Stokoe, P.; Harf, R. La Expresión Corporal en el Jardín de Infantes; Paidos Ibérica: Barcelona, Spain, 1992; pp. 1–140. [Google Scholar]
- Sheet Johnstone, M. Thinking in Movement. J. Aesthet. Art Crit. 1891, 39, 399–407. [Google Scholar] [CrossRef]
- Arteaga, M.; Viciana, V.; Conde, J. Desarrollo de la Expresividad Corporal; INDE publicaciones: Barcelona, Spain, 1997; pp. 1–166. [Google Scholar]
- Castañer, M. Expresión Corporal y Danza; INDE Publicaciones: Barcelona, Spain, 2000; pp. 1–104. [Google Scholar]
- Fernández, J.; Hortigüela, D.; Pérez Pueyo, Á. Revisando los modelos pedagógicos en educación física. Ideas clave para incorporarlos al aula. Rev. Española De Educ. Física Y Deportes 2018, 423, 7–80. [Google Scholar]
- López, M.D. Espacio Europeo de Educación Superior: Competencias profesionales y empleabilidad. Rev. Iberoam. De Educ. 2008, 46, 4. [Google Scholar]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S. Physical activity and mortality in cancer survivors: A systematic review and meta-analysis. JNCI Cancer Spectr. 2020, 4, 80. [Google Scholar] [CrossRef]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Denlinger, C. American College of Sports Medicine roundtable report on physical activity, sedentary behavior, and cancer prevention and control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Carriedo, A.; Méndez Giménez, A.; Fernández-Río, J.; Cecchini, J.A. Nuevas posibilidades y recursos para la enseñanza de la expresión corporal en educación física: Internet y los retos virales (New ways and resources for teaching body expression in physical education: Internet and viral challenges). Retos 2020, 37, 722–730. [Google Scholar]
- Castejón, F.J. Iniciación deportiva. Aprendizaje y enseñanza; Pilar Teleña: Madrid, Spain, 2001; pp. 1–140. [Google Scholar]
- Malla, F.; Zabala, I. La previsión del futuro en la empresa (III): El método Delphi. Estud. Empresariales 1978, 39, 13–24. [Google Scholar]
- García Ferrando, M. Postmodernidad y Deporte: Entre la Individualización y la Masificación. Encuesta Sobre Hábitos Deportivos de los Españoles; Centro de Investigaciones Sociológicas: Madrid, Spain, 2006; pp. 1–312. [Google Scholar]
- Díaz de Rada, V. Tipos de Encuestas y Diseños de Investigación; Universidad Pública de Navarra: Pamplona, Spain, 2002; pp. 1–243. [Google Scholar]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Fisher, R. Métodos Estadísticos Para Investigadores; Aguilar: Madrid, Spain, 1949; pp. 1–322. [Google Scholar]
- Kaplan, D. Structural Equation Modeling: Foundations and Extensions; Sage Publications: Thousand Oaks, CA, USA, 2008; pp. 1–215. [Google Scholar]
- Kline, R. Principles and Practices of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2005; pp. 1–445. [Google Scholar]
- Carmines, E.; Mclver, J. Analyzing Models with Unobserved Models: Analysis of Covariance Structures. Social Measurement: Current Issues; Bohrnstedt, G.W., Borgatta, E.F., Eds.; Saga Publications, Inc.: Beverly Hills, CA, USA, 1981; pp. 65–115. [Google Scholar]
- Jöreskog, K.G. Un método general para estimar un sistema de ecuaciones estructurales lineales. Ets Res. Bull. Ser. 1970, 2, 1–41. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling: A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Steiger, J.H. Comprender las limitaciones de la evaluación de ajuste global en el modelado de ecuaciones estructurales. Pers. Y Difer. Individ. 2007, 42, 893–898. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Name | Items Integrated in Every Factor of Questionnaire |
|---|---|---|
| I | A (blood cancer and sport) | A1. A2. A3. A4. A5. A6 |
| B (tumor of bones and sport) | B7. B8. B9. B10. B11. B12 | |
| C (cerebral tumor and sport) | C13. C14. C15. C16. C17. C18 | |
| D (information of cancer and sport) | D19. D21. D22. D23. D24 | |
| E (mass information oncology and sport) | E25. E27. E28. E29. E30 | |
| F (information of sport) | F31. F32. F35. F36. F37. F38 | |
| II | D20, E26 | |
| IV | F33, F34 |
| Items | |
|---|---|
| A1 | The person that presents cancer in the blood has difficulties practicing sport. |
| A2 | The person that presents cancer in the blood when practicing sport suffers from exhaustion. |
| A3 | The person that presents cancer in the blood improves his or her health condition when practicing sport. |
| A4 | The person that presents with cancer in the blood when practicing sport has bruises in various parts of his/her body. |
| A5 | The person that presents with cancer in the blood when practicing sport has changes in behavior. |
| A6 | The person that presents cancer in the blood when practicing sport have breathing difficulty. |
| B7 | The person that presents tumor of the bones has an inability to practicing sport. |
| B8 | The person that presents tumor of the bones can do sport. |
| B9 | The person that has tumor of the bones have exhaustion when doing sport. |
| B10 | The person that has tumor of the bones when doing sport will have bruises in various parts of his/her body. |
| B11 | The person that presents tumor of the bones have fatigue when walking. |
| B12 | The person that presents tumor of the bones, if he/she practices sport will show a change of behavior. |
| C13 | The person that presents cerebral tumor cannot do sport. |
| C14 | The person that has a cerebral tumor can do sport. |
| C15 | The person that presents cerebral tumor has exhaustion. |
| C16 | The person when have cerebral tumor will display a loss of equilibrium when doing sport. |
| C17 | The person that presents cerebral tumor will have breathing difficulties when doing sport. |
| C18 | The person that presents cerebral tumor will have bruises doing sport. |
| D19 | I am interested in topics of oncology associated with sport. |
| D21 | I try to keep up to date about what is happening nowadays in sport in relation with oncology. |
| D22 | I try to keep up to date about of types of oncology and their relationship with sport. |
| D23 | I would like to learn more about of oncology. |
| D24 | To investigate about how we can improve the lives of people that have cancer through sport. |
| E25 | I inform myself through newspapers and books of sport in relation to health. |
| E27 | I inform myself through newspapers and magazines of a general purposes. |
| E28 | I inform myself through television and radio. |
| E29 | I inform myself through the Internet. |
| E30 | I do not inform myself through any particular medium. |
| F31 | It is always good to know how sport affect to people with cancer. |
| F32 | Everyone should know about sport. |
| F35 | Sport is good for your life. |
| F36 | Sport can heal. |
| F37 | One should always investigate different sports. |
| F38 | People should do sport from an early age |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melero García, L.; Hernández Fernández, A.; Pérez Navío, E. Sport and Its Relationship with Oncology in Future Primary Education Teachers. Educ. Sci. 2020, 10, 167. https://doi.org/10.3390/educsci10060167
Melero García L, Hernández Fernández A, Pérez Navío E. Sport and Its Relationship with Oncology in Future Primary Education Teachers. Education Sciences. 2020; 10(6):167. https://doi.org/10.3390/educsci10060167
Chicago/Turabian StyleMelero García, Lucía, Antonio Hernández Fernández, and Eufrasio Pérez Navío. 2020. "Sport and Its Relationship with Oncology in Future Primary Education Teachers" Education Sciences 10, no. 6: 167. https://doi.org/10.3390/educsci10060167