Screening Tools Used by Clinical Pharmacists to Identify Elderly Patients at Risk of Drug-Related Problems on Hospital Admission: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Resources
2.2. Data Extraction
2.3. Search Terms and Search Strategy
2.4. Inclusion and Exclusion Criteria
2.4.1. Paper Inclusion Criteria
2.4.2. Paper Exclusion Criteria
2.4.3. Critical Appraisal and Data Extraction for Included Studies
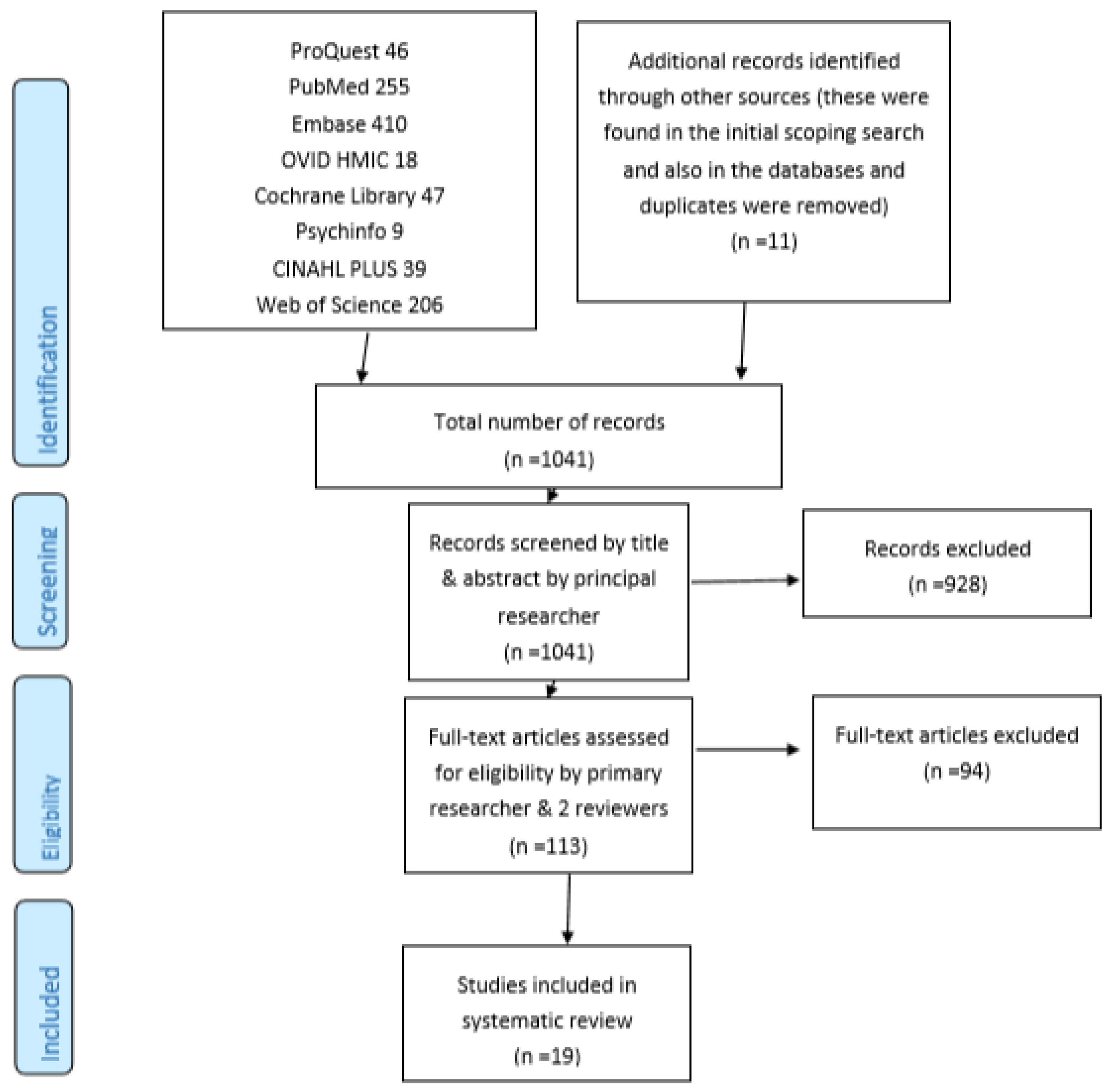
3. Results
3.1. Included Papers
3.2. Population Characteristics: Age
3.3. Population Characteristics: Gender
3.4. Population Characteristics: Ethnicity
3.5. Population Characteristics: Number of Study Participants
3.6. Development/Modelling, Utilisation or Validation of Assessment Tools
3.7. Study Setting (Country/Countries)
3.8. Primary Outcomes of the Studies
3.9. Number of Risk Factors Included in Risk Scores/Tools
3.10. Identification of Risk Factors
3.11. Statistical Analysis
3.12. Methodologies for Development of Point Scores
3.13. Performance of Risk Score/Tool/Model: Sensitivity, Specificity and/or Discriminatory Ability
3.14. Sample Size and Power of Study
3.15. Quality of Included Studies
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pharmaceutical Care Network Europe. The PCNE Classification V 9.0. Available online: https://www.pcne.org/upload/files/334_PCNE_classification_V9-0.pdf (accessed on 20 February 2019).
- NHS. East & South East England Specialist Pharmacy Services. Medicines Related Problems on Admission to Hospital—The Evidence 2014. Available online: https://www.sps.nhs.uk/wp-content/uploads/2014/04/Medicines_related_problems_on_admission_the_evidence_Apr14_Vs2_JW.pdf (accessed on 14 April 2013).
- Urbina, O.; Ferrández, O.; Grau, S.; Luque, S.; Mojal, S. Marin-Casino Mea. Design of a score to identify hospitalized patients at risk of drug-related problems. Pharmacoepidemiol. Drug Saf. 2014, 23, 923–932. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Proposed Working Definition of an Older Person in Africa for the MDS Project 2002. Available online: https://www.who.int/healthinfo/survey/ageingdefnolder/en/ (accessed on 1 January 2001).
- World Health Organization. Men Ageing and Health—Achieving Health Across the Life Span 2001. Available online: https://apps.who.int/iris/bitstream/handle/10665/66941/WHO_NMH_NPH_01.2.pdf?sequence=1 (accessed on 1 January 2001).
- Petrovic, M.; Somers, A.; Onder, G. Geriatric Pharmacotherapy: Optimisation Through Integrated Approach in the Hospital Setting. In Developing Drug Products in an Aging Society; Stegemann, S., Ed.; Springer: Berlin, Germany, 2016; Volume 26. [Google Scholar]
- Stevenson, J.; Williams, J.; Burnham, T.; Prevost, A.; Schiff, R.; Erskine, D.; Davies, J.G. Predicting adverse drug reactions in older adults; A systematic review of the risk prediction models. Clin. Interv. Aging 2014, 9, 1581–1593. [Google Scholar]
- Alhawassi, T.; Krass, I.; Bajorek, B.; Pont, L. A systematic review of the prevalence and risk factors for adverse drug reactions in the elderly in the acute care setting. Clin. Interv. Aging. 2014, 9, 2079–2086. [Google Scholar] [PubMed] [Green Version]
- Yourman, L.; Lee, S.; Schonberg, M.; Widera, E.; Smith, A. Prognostic Indices for Older Adults A Systematic Review. JAMA J. Am. Med Assoc. 2012, 307, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; García, F.A.R.; Gillman, M.W.; Harper, D.M.; Kemper, A.R.; Krist, A.H.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 2564–2575. [Google Scholar] [CrossRef]
- Rodin, M.B. Breast cancer screening in older women: American Geriatrics Society Clinical Practice Committee. J. Am. Geriatr. Soc. 2000, 48, 842–844. [Google Scholar]
- Wolf, A.; Wender, R.; Etzioni, R.; Thompson, I.; D’Amico, A.; Volk, R.J.; DeSantis, C. American Cancer Society Guideline for the Early Detection of Prostate Cancer: Update 2010. CA A Cancer J. Clin. 2010, 60, 70–98. [Google Scholar] [CrossRef] [Green Version]
- Reference.MD. Inappropriate Prescribing. Available online: http://www.reference.md/files/D057/mD057970.html (accessed on 9 April 2020).
- O’Connor, M.N.; Gallagher, P.; O’Mahony, D. Inappropriate prescribing: Criteria, detection and prevention. Drugs Aging 2012, 29, 437–452. [Google Scholar] [CrossRef]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2014, 44, 213–238. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, P.; Barry, P.; O’Mahony, D. Inappropriate prescribing in the elderly. J. Clin. Pharm. Ther. 2007, 32, 113–121. [Google Scholar] [CrossRef]
- Lavan, A.H.; Gallagher, P.F.; O’Mahony, D. Methods to reduce prescribing errors in elderly patients with multimorbidity. Clin. Interv. Aging 2016, 11, 857–866. [Google Scholar] [PubMed] [Green Version]
- Hickson, R.P.; Steinke, D.T.; Skitterall, C.; Williams, S.D. Evaluation of a pharmaceutical assessment screening tool to measure patient acuity and prioritise pharmaceutical care in a UK hospital. Eur. J. Hosp. Pharm. Sci. Pract. 2017, 24, 74–79. [Google Scholar] [CrossRef] [PubMed]
- National Health Service. Greater Glasgow and Clyde. Pharmacy Prioritisation and Referral. PostScript Acute 2014, 17, 1–2. [Google Scholar]
- Hohl, C.M.; Yu, E.; Hunte, G.S.; Brubacher, J.R.; Hosseini, F.; Argent, C.P.; Singer, J. Clinical decision rules to improve the detection of adverse drug events in emergency department patients. Acad. Emerg. Med. Off. J. Soc. for Acad. Emerg. Med. 2012, 19, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Bruchet, N.; Loewen, P.; Lemos, J. Improving the Quality of Clinical Pharmacy Services: A Process to Identify and Capture High-Value? Quality Actions? Can. J. Hosp. Pharm. 2011, 64, 42–47. [Google Scholar] [PubMed] [Green Version]
- El Hajji, F.W.; Scullin, C.; Scott, M.G.; McElnay, J.C. Enhanced clinical pharmacy service targeting tools: Risk-predictive algorithms. J. Eval. Clin. Pract. 2015, 21, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Suggett, E.; Marriott, J. Risk Factors Associated with the Requirement for Pharmaceutical Intervention in the Hospital Setting: A Systematic Review of the Literature. Drugs Real World Outcomes 2016, 3, 241–263. [Google Scholar] [CrossRef] [Green Version]
- Tangiisuran, B. Predicting Adverse Drug Reactions in the Hospitalised Elderly. Ph.D. Thesis, University of Sussex, Brighton, UK, 2009. [Google Scholar]
- Tangiisuran, B.; Scutt, G.; Stevenson, J.; Wright, J.; Onder, O.; Petrovic, M. Development and Validation of a Risk Model for Predicting Adverse Drug Reactions in Older People during Hospital Stay: Brighton Adverse Drug Reactions Risk (BADRI) Model. PLoS ONE 2014, 9, e111254. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Petrovic, M. Adverse drug reactions in older people and their prevention: The need for a new approach. In Proceedings of the International Congress of The European Union Geriatric Medicine Society (EuGMS), Nice, France, 20–22 September 2017. [Google Scholar]
- Falconer, N.; Barras, M.; Cottrell, N. Systematic review of predictive risk models for adverse drug events in hospitalized patients. Br. J. Clin. Pharmacol. 2018, 84, 846–864. [Google Scholar] [CrossRef]
- Brady, A.; Curtis, C.; Jalal, Z. Prediction Tools, Models and Risk Score Systems Used by Clinical Pharmacists in the Acute Hospital Setting to Identify Elderly Patients Most Likely to Experience Drug Related Problems and/or Benefit From Hospital Pharmacist Intervention: A Systematic Review of the Literature. CRD42019115673. PROSPERO. 2019. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42019115673 (accessed on 22 March 2019).
- Onder, G.; Petrovic, M.; Tangiisuran, B.; Meinardi, M.C.; Markito-Notenboom, W.P. Development and Validation of a Score to Assess Risk of Adverse Drug Reactions Among In-Hospital Patients 65 Years or Older. The GerontoNet ADR Risk Score. Arch. Intern. Med. 2010, 70, 1142–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trivalle, C.; Burlaud, A.; Ducimetière, P. Risk factors for adverse drug events in hospitalized elderly patients: A geriatric score. Eur. Geriatr. Med. 2011, 2, 284–289. [Google Scholar] [CrossRef]
- O’Connor, M.N.; Gallagher, P.; Byrne, S.; O’Mahony, D. Adverse drug reactions in older patients during hospitalisation: Are they predictable? Age Ageing 2012, 41, 771–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alassaad, A.; Melhus, H.; Hammarlund-Udenaes, M.; Bertilsson, M.; Gillespie, U.; Sundstrom, J. A tool for prediction of risk of rehospitalisation and mortality in the hospitalised elderly: Secondary analysis of clinical trial data. BMJ Open 2015, 5, e007259. [Google Scholar] [CrossRef] [PubMed]
- Suggett, E.L. Risk Assessment of Patients in an Acute Trust as a Means of Directing a Clinical Pharmacy Service. Ph.D. Thesis, University of Birmingham, Birmingham, UK, 2017. [Google Scholar]
- Hohl, C.M.; Partovi, N.; Ghement, I.; Wickham, M.E.; McGrail, K.; Reddekopp, L.N.; Sobolev, B. Impact of early in-hospital medication review by clinical pharmacists on health services utilization. PLoS ONE 2017, 12, e0170495. [Google Scholar] [CrossRef]
- Bonnerup, D.K.; Lisby, M.; Saedder, E.A.; Sorensen, C.A.; Brock, B.; Andersen, L.; Nielsen, L.P. Risk of prescribing errors in acutely admitted patients: A pilot study. Int. J. Clin. Pharm. 2016, 38, 1157–1163. [Google Scholar] [CrossRef]
- Kaufmann, C.P.; Stampfli, D.; Mory, N.; Hersberger, K.E.; Lampert, M.L. Drug-Associated Risk Tool: Development and validation of a self-assessment questionnaire to screen for hospitalised patients at risk for drug-related problems. BMJ Open 2018, 8, e016610. [Google Scholar] [CrossRef] [Green Version]
- Falconer, N.; Nand, S.; Liow, D.; Jackson, A.; Seddon, M. Development of an electronic patient prioritization tool for clinical pharmacist interventions. Am. J. Health Syst. Pharm. AJHP Off. J. Am. Soc. Health Syst. Pharm. 2014, 71, 311–320. [Google Scholar] [CrossRef]
- Falconer, N.; Liow, D.; Zeng, I.; Parsotam, N.; Seddon, M.; Nand, S. Validation of the assessment of risk tool: Patient prioritisation technology for clinical pharmacist interventions. Eur. J. Hosp. Pharm. Sci. Pract. 2017, 24, 320–326. [Google Scholar] [CrossRef]
- McAuliffe, L.H.; Zullo, A.R.; Dapaah-Afriyie, R.; Berard-Collins, C. Development and validation of a transitions-of-care pharmacist tool to predict potentially avoidable 30-day readmissions. Am. J. Health Syst. Pharm. AJHP Off. J. Am. Soc. Health Syst. Pharm. 2018, 75, 111–119. [Google Scholar] [CrossRef]
- McElnay, J.C.; McCallion, C.R.; Al-Deagi, F.; Scott, M.G. Development of a Risk Model for Adverse Drug Events in the Elderly. Clin. Drug Investig. 1997, 13, 47–55. [Google Scholar] [CrossRef]
- Saedder, E.A.; Lisby, M.; Nielsen, L.P.; Rungby, J.; Andersen, L.V.; Bonnerup, D.K.; Brock, B. Detection of Patients at High Risk of Medication Errors: Development and Validation of an Algorithm. Basic Clin. Pharmacol. Toxicol. 2016, 118, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrovic, M.; Tangiisuran, B.; Rajkumar, C.; van der Cammen, T.; Onder, G. Predicting the Risk of Adverse Drug Reactions in Older Inpatients: External Validation of the GerontoNet ADR Risk Score Using the CRIME Cohort. Drugs Aging 2017, 34, 135–142. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Connor, M.; Eustace, J.; Byrne, S.; Petrovic, M.; Gallagher, P. The adverse drug reaction risk in older persons (ADRROP) prediction scale: Derivation and prospective validation of an ADR risk assessment tool in older multi-morbid patients. Eur. Geriatr. Med. 2018, 9, 191–199. [Google Scholar] [CrossRef]
- Ayorinde, A.A.; Williams, I.; Mannion, R.; Song, F.; Skrybant, M.; Lilford, R.J.; Chen, Y.F. Assessment of publication bias in systematic reviews of health services and delivery research (Poster). J. Epidemiol. Community Health 2018, 72, A79. Available online: https://jech.bmj.com/content/72/Suppl_1/A79.2.info (accessed on 5 September 2018).


{kind=link}
| Author | Tool |
|---|---|
| Tangiisuran B. et al. [25] (note: this research was also reported in PhD thesis [24] but only counted as one piece of research in this SR) | BADRI model |
| Onder G. et al. [30] | GerontoNet ADR Risk Score |
| Trivalle C. et al. [31] | A geriatric score |
| O’Connor M.N. et al. [32] | GerontoNet ADR Risk Score |
| Alassaad A. et al. [33] | The 80+ score |
| Suggett E. [34] | Risk scores to identify patients who were at high risk of (hospital) pharmacist intervention (no specific name for score stated by authors) |
| Hohl C.M. et al. (2017) [35] | Clinical decision rules |
| Hohl C.M. et al. (2012) [20] | Clinical decision rules |
| Bonnerup D.K. et al. [36] | MERIS score |
| Kaufmann C.P. et al. (2018) [37] | Drug-Associated Risk Tool (DART) |
| Falconer N. et al. (2014) [38] | Assessment of Risk Tool (ART) |
| Falconer N. et al. (2017) [39] | Assessment of Risk Tool (ART), |
| McAuliffe L. et al. [40] | MEDCOINS score |
| McElnay J.C. et al. [41] | A predictive model for adverse drug events (ADEs) in elderly patients (no specific name for model stated by authors) |
| Urbina O. et al. [3] | A score that quantifies the risk of a DRP during hospital admission (no specific name for score stated by authors) |
| Hickson R.P. et al. [18] | Pharmaceutical assessment screening tool (PAST) |
| Saedder E.A. et al. [42] | MERIS score |
| Petrovic M. et al. [43] | GerontoNet ADR Risk Score |
| O’Mahony D. et al. [44] | The adverse drug reaction risk in older persons (ADRROP) prediction scale |
| Author | Sensitivity | Specificity | Other | |||
|---|---|---|---|---|---|---|
| Discriminatory Ability: AUROC/AUCROC | Discriminatory Ability: C-statistic | Overall Accuracy | Other | |||
| Tangiisuran B. et al. | 80.0% for internal validation; 84% for external validation | 55.0% for internal validation; 43% for external validation | 0.74 (95%CI = 0.68–0.79) for internal validation; 0.73 (95%CI = 0.66–0.80) for external validation | |||
| Onder et al. | 68% (development) | 65% (development) | 0.71 (95% CI = 0.68–0.73) (development) 0.70 (95% CI = 0.63–0.78) (validation) | |||
| Trivalle et al. | n/r | n/r | 0.70 (95% CI = 0.635–0.74) | |||
| O’Connor et al. | n/r | n/r | 0.62 (95% CI = 0.57–0.68) on admission (lower on subsequent days, days 5 & 10 post-admission) | |||
| Alassaad A. (&et al) | n/r | n/r | 0.71 | |||
| Suggett E. | n/r | n/r | 0.607 for main data; 0.616 for validation data | |||
| Hohl et al (2017) | n/r | n/r | n/r | n/r | n/r | |
| Hohl et al (2012) | 1) More sensitive rule (ADE rule) 96.7% (95%CI = 91.8–98.6%) | 1) 40.3% | ||||
| 2) More specific rule (Adverse Drug Reaction Rule) 90.8% (95%CI = 81.4–95.7%) | 2) 59.1% | |||||
| Bonnerup et al. | n/r | n/r | n/r | n/r | n/r | |
| Kaufmann et al. | 67% average (range = 21–100) | 88% average (range = 27–100) | n/r | |||
| Falconer et al. (2014) | n/r | n/r | n/r | n/r | n/r | |
| Falconer et al. (2017) | n/r | n/r | 0.72 (95%CI = 0.66–0.78) to predict at least one unintended medication discrepancy; from score from 2 flags (>8 regular admission medicines and readmission within 30 days of discharge) | |||
| McAuliffe et al. | n/r | n/r | 0.65 (95%CI = 0.60–0.70) | Hosmer-Lemeshow goodness-of-fit = 0.99 | ||
| McElnay et al. | 41% (validation) | 69% (validation) | 63% | |||
| Urbina et al. | n/r | n/r | 0.778 (95% CI = 0.768–0.789) (training set); 0.776 (95%CI = 0.759–0.792) (validation set) | Hosmer-Lemeshow goodness-of-fit = non-significant (p = 0.13) (validation set) | ||
| Hickson et al. | n/r | n/r | n/r | n/r | n/r | n/r |
| Saedder et al. | 0.64 (for final version of MERIS) | 0.75 (for final version of MERIS) | 0.76, 0.87, 0.74, 0.66 for final MERIS score in different populations within study | |||
| Petrovic et al. | n/r | n/r | 0.64 (95%CI = 0.55–0.74) to predict ADRs probably or definitely related to drug use; 0.69 (95%CI = 0.60–0.77) for predicting Type A ADRs; subgroup analysis: AUC = 0.70–0.79 and 0.80–0.89 | |||
| O’Mahony et al. | n/r | n/r | 0.623 (95% CI = 0.598–0.665) (derivation cohort); 0.592 (95%CI = 0.532–0.652) (vallidation cohort) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brady, A.; Curtis, C.E.; Jalal, Z. Screening Tools Used by Clinical Pharmacists to Identify Elderly Patients at Risk of Drug-Related Problems on Hospital Admission: A Systematic Review. Pharmacy 2020, 8, 64. https://doi.org/10.3390/pharmacy8020064
Brady A, Curtis CE, Jalal Z. Screening Tools Used by Clinical Pharmacists to Identify Elderly Patients at Risk of Drug-Related Problems on Hospital Admission: A Systematic Review. Pharmacy. 2020; 8(2):64. https://doi.org/10.3390/pharmacy8020064
Chicago/Turabian StyleBrady, Amanda, Chris E. Curtis, and Zahraa Jalal. 2020. "Screening Tools Used by Clinical Pharmacists to Identify Elderly Patients at Risk of Drug-Related Problems on Hospital Admission: A Systematic Review" Pharmacy 8, no. 2: 64. https://doi.org/10.3390/pharmacy8020064