Medicine Prices, Availability, and Affordability in Private Health Facilities in Low-Income Settlements in Nairobi County, Kenya

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
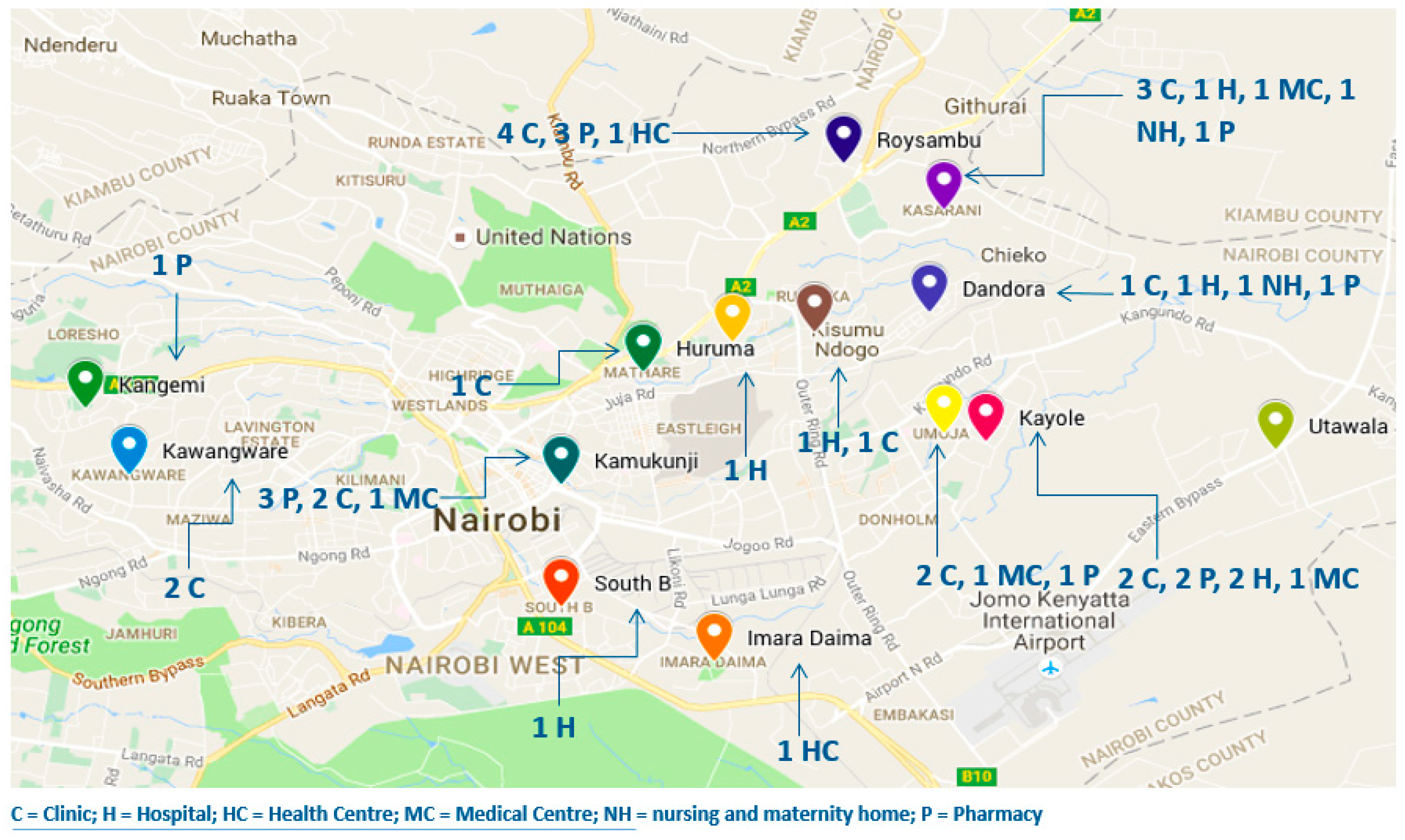
2.2. Study Area Description
2.3. Study Sites and Sampling
2.4. Data Collection and Data Management
2.5. Data Analysis
3. Results
3.1. Comparison of Innovator Brand, Lowest Price Generic Medicines, and International Reference Prices
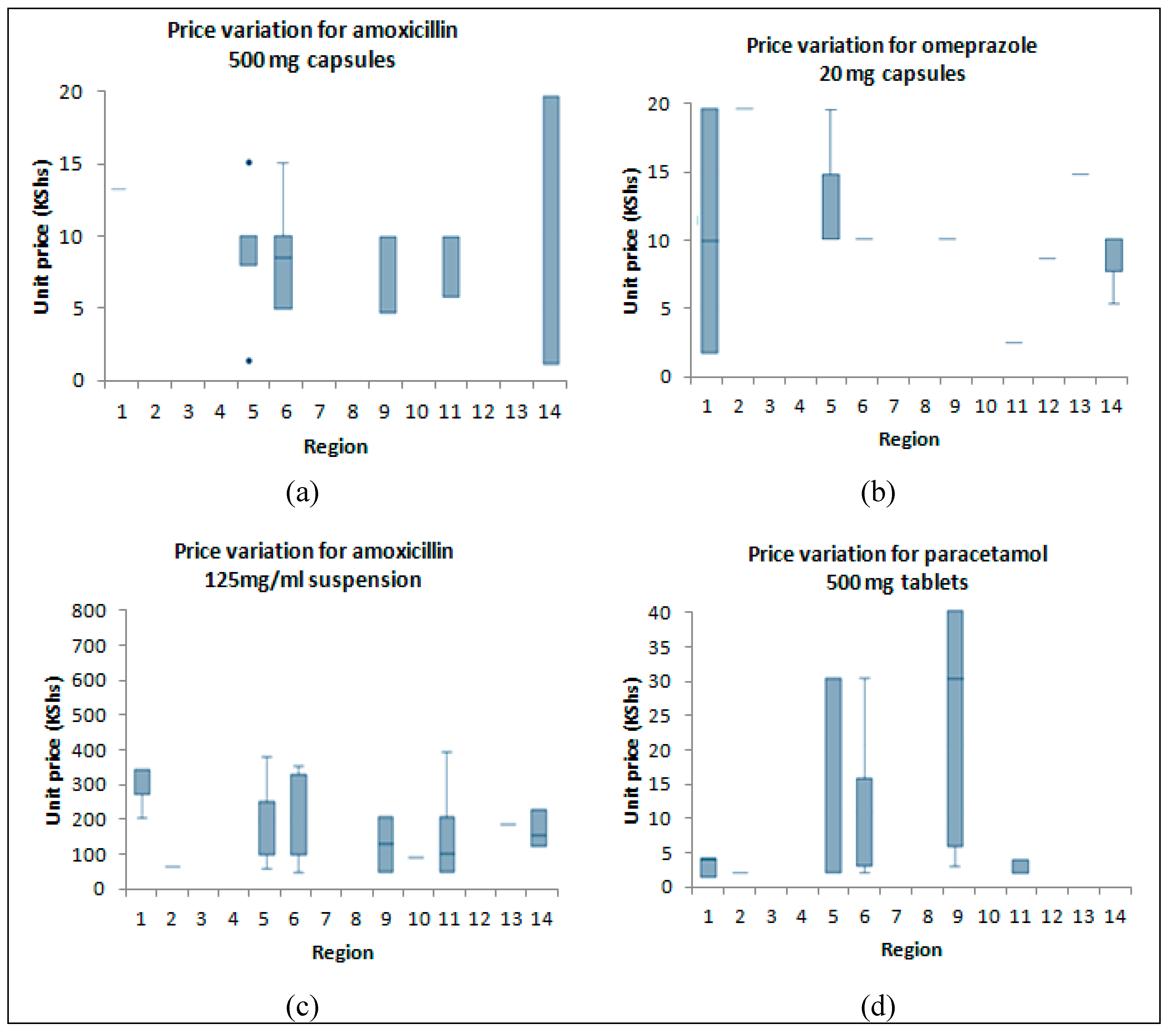
3.2. Price Variation across the Regions during the Study Period
3.3. Comparison of Prices within Therapeutic Classes
3.4. Affordability
3.5. Availability of Medicines in the 45 Facilities
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bright, T.; Felix, L.; Kuper, H.; Polack, S. A systematic review of strategies to increase access to health services among children in low and middle income countries. BMC Health Serv. Res. 2017, 17, 252. [Google Scholar] [CrossRef]
- Lu, Y.; Hernandez, P.; Abegunde, D.; Edejer, T. World Medicines Situation 2011; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Leisinger, K.M.; Garabedian, L.F.; Wagner, A.K. Improving access to medicines in low and middle income countries: Corporate responsibilities in context. South. Med. Rev. 2012, 5, 3–8. [Google Scholar]
- Cameron, A.; Ewen, M.; Ross-Degnan, D.; Ball, D.; Laing, R. Medicine prices, availability, and affordability in 36 developing and middle-income countries: A secondary analysis. Lancet 2009, 373, 240–249. [Google Scholar] [CrossRef]
- O’Donnell, O. Access to health care in developing countries: Breaking down demand side barriers. Cad. Saude Publica 2007, 23, 2820–2834. [Google Scholar] [CrossRef]
- Fox, S. The Political Economy of Slums: Theory and Evidence from Sub-Saharan Africa. World Dev. 2014, 54, 191–203. [Google Scholar] [CrossRef]
- Awiti, J.O. Poverty and health care demand in Kenya. BMC Health Serv. Res. 2014, 14, 560. [Google Scholar] [CrossRef]
- Gulis, G.; Mulumba, J.A.A.; Juma, O.; Kakosova, B. Health status of people of slums in Nairobi, Kenya. Environ. Res. 2004, 96, 219–227. [Google Scholar] [CrossRef]
- Unger, A.; Riley, L.W. Slum health: From understanding to action. PLoS Med. 2007, 4, e295. [Google Scholar] [CrossRef]
- Vlahov, D.; Freudenberg, N.; Proietti, F.; Ompad, D.; Quinn, A.; Nandi, V.; Galea, S. Urban as a determinant of health. J. Urban Health 2007, 84, 16–26. [Google Scholar] [CrossRef]
- Sheuya, S.A. Improving the health and lives of people living in slums. Ann. N. Y. Acad. Sci. 2008, 1136, 298–306. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Schofield, L.; Wekesah, F.; Mohamed, S.; Mberu, B.; Ettarh, R.; Egondi, T.; Kyobutungi, C.; Ezeh, A. Vulnerability to Food Insecurity in Urban Slums: Experiences from Nairobi, Kenya. J. Urban Health 2014, 91, 1098–1113. [Google Scholar] [CrossRef]
- Sajjad, H. Living Standards and Health Problems of Lesser Fortunate Slum Dwellers: Evidence from an Indian City. Int. J. Environ. Prot. Policy 2014, 2, 54. [Google Scholar] [CrossRef]
- Kimani, J.K.; Ettarh, R.; Kyobutungi, C.; Mberu, B.; Muindi, K. Determinants for participation in a public health insurance program among residents of urban slums in Nairobi, Kenya: Results from a cross-sectional survey. BMC Health Serv. Res. 2012, 12, 66. [Google Scholar] [CrossRef]
- Amuyunzu-Nyamongo, M.; Nyamongo, I.K. Health seeking behaviour of mothers of under-five-year-old children in the slum communities of Nairobi, Kenya. Anthropol. Med. 2006, 13, 25–40. [Google Scholar] [CrossRef]
- Kwena, Z.A.; Sharma, A.; Muga, C.; Wamae, N.; Bukusi, E.A. Management of simulated patients with sexually transmitted infections by staff of retail pharmacies in kibera slums of nairobi. East Afr. Med. J. 2008, 85, 419–424. [Google Scholar] [CrossRef]
- Khan, M.M.H.; Grbner, O.; Krämer, A. Frequently used healthcare services in urban slums of Dhaka and adjacent rural areas and their determinants. J. Public Health 2012, 34, 261–271. [Google Scholar] [CrossRef]
- Miller, R.; Goodman, C. Performance of retail pharmacies in low- and middle-income Asian settings: A systematic review. Health Policy Plan. 2016, 31, 940–953. [Google Scholar] [CrossRef]
- Cameron, A.; Roubos, I.; Ewen, M.; Mantel-Teeuwisse, A.K.; Leufkens, H.G.M.; Laing, R.O. Differences in the availability of medicines for chronic and acute conditions in the public and private sectors of developing countries. Bull. World Health Organ. 2011, 89, 412–421. [Google Scholar] [CrossRef]
- Njuguna, J. Impact of Health Workers’ Strike in August 2014 on Health Services in Mombasa County Referral Hospital, Kenya. J. Health Care Poor Underserved 2015, 26, 1200–1206. [Google Scholar] [CrossRef]
- Olack, B.; Feikin, D.R.; Cosmas, L.O.; Odero, K.O.; Okoth, G.O.; Montgomery, J.M.; Breiman, R.F. Mortality trends observed in population-based surveillance of an urban slum settlement, Kibera, Kenya, 2007–2010. PLoS ONE 2014, 9, e85913. [Google Scholar] [CrossRef]
- Kenya Health Care Federation. Kenyan Healthcare Sector: Market Study Report; Kenya Healthcare Federation: Nairobi, Kenya, 2016; Available online: http://khf.co.ke/wp-content/uploads/2018/03/2016-Kenyan-Healthcare-Sector-Report.pdf (accessed on 20 February 2019).
- NHIF. Kenya National Health Insurance Fund (NHIF). 2014. Available online: http://www.nhif.or.ke/healthinsurance/ (accessed on 20 February 2019).
- Ministry of Health. Kenya National Health Accounts, 2015/16; Ministry of Health: Nairobi, Kenya, 2017. Available online: https://www.researchgate.net/publication/321864804_Kenya_National_Health_Accounts_FY_201516 (accessed on 20 February 2019).
- World Health Organization and Health Action International Africa. Measuring Medicine Prices, Availability, Affordability and Price Components; World Health Organization: Geneva, Switzerland, 2008; Available online: https://www.who.int/medicines/areas/access/OMS_Medicine_prices.pdf (accessed on 20 February 2019).
- African Population and Health Research Center (APHRC). Population and Health Dynamics in Nairobi’s Informal Settlements: Report of the Nairobi Cross-Sectional Slums Survey (NCSS) 2012; APHRC: Nairobi, Kenya, 2014; Available online: https://aphrc.org/wp-content/uploads/2014/08/NCSS2-FINAL-Report.pdf (accessed on 20 February 2019).
- StataCorp Stata Statistical Software; StataCorp LP: College Station, TX, USA, 2013.
- Management Science for Health. The International Medical Products Price Guide; MSH: Medford, OR, USA, 2015; Available online: http://mshpriceguide.org/en/drug-search-page-2/ (accessed on 12 September 2018 ).
- Government of Kenya. Legal Notice on the Regulation of Wages; Government of Kenya Press: Nairobi, Kenya, 2015. Available online: http://kenyalaw.org/kl/fileadmin/pdfdownloads/LegalNotices/2015/LN117_2015.pdf (accessed on 20 February 2019).
- Mhlanga, B.S.; Suleman, F. Price, availability and affordability of medicines. Afr. J. Prim. Health Care Fam. Med. 2014, 6, 1–6. [Google Scholar] [CrossRef]
- Ministry of Health. Clinical Management and Referral Guidelines Vol. III; World Health Organization: Geneva, Switzerland, 2009. Available online: http://apps.who.int/medicinedocs/documents/s21000en/s21000en.pdf (accessed on 20 February 2019).
- Mokaya, J.; Dotchin, C.L.; Gray, W.K.; Hooker, J.; Walker, R.W. The Accessibility of Parkinson’s Disease Medication in Kenya: Results of a National Survey. Mov. Disord. Clin. Pract. 2016, 3, 376–381. [Google Scholar] [CrossRef]
- Xu, K.; Evans, D.B.; Kawabata, K.; Zeramdini, R.; Klavus, J.; Murray, C.J.L. Household catastrophic health expenditure: A multicountry analysis. Lancet 2003, 362, 111–117. [Google Scholar] [CrossRef]
- World Health Organization and Health Action International Africa. Medicine Prices in Kenya; WHO: Geneva, Switzerland, 2006; Available online: https://www.who.int/medicines/areas/technical_cooperation/MedicinepricesKenya.pdf (accessed on 20 February 2019).
- Kamat, V.R.; Nichter, M. Pharmacies, self-medication and pharmaceutical marketing in Bombay, India. Soc. Sci. Med. 1998, 47, 779–794. [Google Scholar] [CrossRef]
- Shafie, A.A.; Hassali, M.A. Price comparison between innovator and generic medicines sold by community pharmacies in the state of Penang, Malaysia. J. Generic Med. 2008, 6, 35–42. [Google Scholar] [CrossRef]
- Gelders, S.; Ewen, M.; Noguchi, N.; Laing, R. Price, Availability and Affordability. An International Comparison of Chronic Disease Medicines. An International Comparison of Chronic Disease Medicines; World Health Organization Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2006. [Google Scholar]
- Rockers, P.C.; Laing, R.O.; Wirtz, V.J. Equity in access to non-communicable disease medicines: A cross-sectional study in Kenya. BMJ Glob. Health 2018, 3, e000828. [Google Scholar] [CrossRef]
- World Health Organization. Medicine Prices in Tanzania; WHO: Geneva, Switzerland, 2004; Available online: https://www.who.int/medicines/areas/technical_cooperation/MedicinepricesTanzania.pdf?ua=1 (accessed on 20 February 2019).
- World Health Organization and Health Action International Africa. Medicine Prices in Uganda; WHO: Geneva, Switzerland, 2005; Available online: https://www.who.int/medicines/areas/technical_cooperation/MedicinePricesUganda.pdf (accessed on 20 February 2019).
- Mong, S.; Masese, I.; Muia, D.M. Coping with Food Insecurity in Math are Valley Slum in Nairobi, Kenya. J. Sociol. Soc. Work 2016, 4, 98–108. [Google Scholar]
- World Bank Poverty and Equity Data; World Bank Group: Washington, DC, USA, 2019; Available online: http://povertydata.worldbank.org/poverty/country/KEN (accessed on 20 February 2019).
- Amendah, D.D.; Buigut, S.; Mohamed, S. Coping Strategies among Urban Poor: Evidence from. PLoS ONE 2014, 9, e83428. [Google Scholar] [CrossRef]
- Niens, L.M.; Brouwer, W.B.F. Measuring the affordability of medicines: Importance and challenges. Health Policy 2013, 112, 45–52. [Google Scholar] [CrossRef]
- Rumboldt, Z.; Marinkovic, M.; Drinovec, J. Enalapril versus captopril: A double-blind multicentre comparison in essential hypertension. Int. J. Clin. Pharmacol. Res. 1988, 8, 181–188. [Google Scholar]
- Ndugwa, R.P.; Zulu, E.M. Child morbidity and care-seeking in Nairobi slum settlements: The role of environmental and socio-economic factors. J. Child Health Care 2008, 12, 314–328. [Google Scholar] [CrossRef] [PubMed]
- Perez-Casas, C.; Herranz, E.; Ford, N. Pricing of drugs and donations: Options for sustainable equity pricing. Trop. Med. Int. Health 2001, 6, 960–964. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.A.; Knight, R.; Roughead, E.E.; Brooks, G.; Mant, A. Policy options for pharmaceutical pricing and purchasing: Issues for low- and middle-income countries. Health Policy Plan. 2015, 30, 267–280. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Product | Unit Price (KShs) * | Price Ratios | ||||||
|---|---|---|---|---|---|---|---|---|
| n | IB | LPG | IRP | IB/LPG | LPG MPR | IB MPR | ||
| 1 | Omeprazole 20 mg | 16 | 200 | 10 | 1.41 | 20.0 | 7.1 | 141.8 |
| 2 | Ranitidine 300 mg | 12 | 58 | 11.5 | 3.75 | 5.0 | 3.1 | 15.5 |
| 3 | Furosemide 40 mg | 7 | 40 | 3 | 0.62 | 13.3 | 4.8 | 64.5 |
| 4 | Enalapril 10 mg | 8 | - | 10 | 4.42 | - | 2.3 | - |
| 5 | Nifedipine 20 mg | 8 | 82 | 5 | 2.33 | 16.4 | 2.1 | 35.2 |
| 6 | Hydrochlorothiazide 25 mg | 2 | - | 5 | 0.43 | - | 11.6 | - |
| 7 | Atenolol 50 mg | 8 | - | 10 | 1.07 | - | 9.3 | - |
| 8 | Paracetamol 500 mg | 16 | 3.2 | 1 | 0.44 | 3.2 | 2.3 | 7.3 |
| 9 | Paracetamol 125 mg/5mL syrup (100 mL) | 24 | 320 | 50 | 52.0 | 6.4 | 1.0 | 6.2 |
| 10 | Ibuprofen 400 mg | 13 | - | 1 | 1.18 | - | 0.8 | - |
| 11 | Diclofenac 50 mg | 13 | 53 | 2.8 | 0.45 | 18.9 | 6.2 | 117.8 |
| 12 | Amoxicillin 500 mg | 13 | 25 | 1 | 3.00 | 25.0 | 0.3 | 8.3 |
| 13 | Amoxicillin 125 mg/5 mL (100 mL) | 13 | 320 | 50 | 46.0 | 6.4 | 1.1 | 7.0 |
| 14 | AmoxiClav 500 mg/125 mg | 17 | 125 | 50 | 16.4 | 2.5 | 3.0 | 7.6 |
| 15 | AmoxiClav 250/62.5 mg/5 mL (100 mL) | 18 | 800 | 150 | 521 | 5.3 | 0.3 | 1.5 |
| 16 | Sulfamethox./Trimethoprim 400 mg/80 mg | 6 | - | 5 | 1.20 | - | 4.2 | - |
| 17 | Sulfamethox./Trimethoprim 200/40 mg/5 mL (100 mL) | 11 | 400 | 50 | 42.0 | 8.0 | 1.2 | 9.5 |
| 18 | Ciprofloxacin 500 mg | 15 | 350 | 10 | 3.73 | 35.0 | 2.7 | 93.8 |
| 19 | Ceftriaxone 1 g | 18 | 2670 | 35 | 39.8 | 76.3 | 0.9 | 67.1 |
| 20 | Clotrimazole cream 20 g | 12 | 235 | 40 | 27.0 | 5.9 | 1.5 | 8.7 |
| 21 | Clotrimazole pessary 100 mg | 11 | 142 | 17 | 7.50 | 8.4 | 2.3 | 18.9 |
| 22 | Fluconazole 200 mg | 8 | 130 | 10 | 7.03 | 13.0 | 1.4 | 18.5 |
| 23 | Aciclovir 400 mg | 5 | - | 10 | 8.35 | - | 1.2 | - |
| 24 | Chlorpheniramine 4 mg | 11 | 30 | 1 | 0.20 | 30.0 | 5.0 | 150.0 |
| 25 | Cetirizine 10 mg | 11 | 50 | 10 | 1.20 | 5.0 | 8.3 | 41.7 |
| 26 | Salbutamol inhaler (200 dose) | 3 | 350 | 400 | 184 | 0.9 | 2.2 | 1.9 |
| 27 | Amitriptyline 25 mg | 1 | - | 2 | 0.84 | - | 2.4 | - |
| 28 | Artemether/lumefantrine 20 mg/120 mg | 13 | 17 | 3 | 16.2 | 5.7 | 0.2 | 1.0 |
| 29 | Metformin 500 mg | 8 | 14 | 1 | 1.50 | 14.0 | 0.7 | 9.3 |
| 30 | Glibenclamide 5 mg | 2 | 15 | 3 | 0.57 | 5.0 | 5.3 | 26.3 |
| 31 | Metronidazole 400 mg | 8 | 9 | 1 | 1.18 | 9.0 | 0.8 | 7.6 |
| 32 | Metronidazole 200 mg/5 mL (100 mL) | 13 | 600 | 20 | 54 | 30.0 | 0.4 | 11.1 |
| 33 | Albendazole 400 mg | 16 | 200 | 15 | 7.88 | 13.3 | 1.9 | 25.4 |
| 34 | Albendazole 200 mg/5 mL (10 mL) | 11 | 200 | 50 | 32.0 | 4.0 | 1.6 | 6.3 |
| 35 | Levonorgestrel 0.75 mg | 7 | 75 | 50 | 22.5 | 1.5 | 2.2 | 3.3 |
| Medicine | LPG Price Per Course | Days Worked for the LPGW to Buy a Treatment Course Assuming Disposable Income | ||
|---|---|---|---|---|
| 100% * | 40% | 7% | ||
| ANTI-ULCERS | ||||
| Omeprazole 20 mg (1 × 2 tablets daily, 30 days) | 300 | 0.57 | 1.42 | 8.13 |
| Ranitidine 300 mg (1 tablet daily, 30 days) | 345 | 0.65 | 1.64 | 9.35 |
| ANTIPROTOZOALS FOR ACUTE AMEBIASIS | ||||
| Metronidazole 400 mg (1 × 3 tablets daily, 5 days) | 15 | 0.03 | 0.07 | 0.43 |
| ANTIBACTERIALS (FOR UPPER RESPIRATORY TRACT INFECTIONS) AND INHALER | ||||
| Ciprofloxacin 500 mg (1 × 2 tablets daily, 7 days) | 140 | 0.27 | 0.66 | 3.79 |
| Amoxicillin 500 mg (1 × 3 capsules daily, 7 days) | 21 | 0.04 | 0.10 | 0. 57 |
| Amoxicillin/Clavulanic acid 625 mg (1 × 2 tablets daily, 7 days) | 700 | 1.33 | 3..32 | 18.97 |
| Ceftriaxone 1000 mg (1g daily, 7 days) | 245 | 0.46 | 1.16 | 6.64 |
| Sulfamethox./Trimethoprim 240 mg/5 mL (1 bottle) | 400 | 0.76 | 1.90 | 10.84 |
| Salbutamol inhaler 1 mcg/dose (1 inhaler) | 400 | 0.76 | 1.90 | 10.84 |
| ANTIHYPERTENSIVES | ||||
| Hydrochlorthiazide 25 mg (1 × 1 tablet daily, 30 days) | 150 | 0.28 | 0.71 | 4.07 |
| Furosemide 40 mg (1 × 1 tablet daily, 30 days) | 90 | 0.17 | 0.43 | 2.44 |
| Atenolol 50 mg (1 × 1 tablet daily, 30 days) | 300 | 0.57 | 1.42 | 8.13 |
| Enalapril 20 mg (1 × 1 tablet daily, 30 days) | 300 | 0.57 | 1.42 | 8.13 |
| Nifedipine 20 mg (1 × 3 tablet daily, 30 days) | 150 | 0.84 | 2.13 | 12.21 |
| HYPOGLYCEMICS | ||||
| Metformin 500 mg (1 × 3 tablets daily, 30 days) | 90 | 0.18 | 0.42 | 2.43 |
| Glibenclamide 5 mg (1 × 1 tablet daily, 30 days) | 90 | 0.17 | 0.43 | 2.44 |
| Product | Number of Facilities Stocking the Medicine (% of 45 Facilities) |
|---|---|
| Aciclovir tablets 400 mg | 13 (29) |
| Amitriptyline tablets | 8 (18) |
| Amoxicillin capsules | 30 (67) |
| Atenolol tablets | 17 (38) |
| Beclomethasone inhaler | 1 (2) |
| Ceftriaxone injection | 27 (60) |
| Ciprofloxacin tablets | 34 (76) |
| Enalapril tablets * | 20 (44) |
| Fluoxetine tablets | 2 (4) |
| Glibenclamide tablets | 18 (40) |
| Hydrochlorthiazide tablets | 27 (60) |
| Ranitidine tablets | 12 (27) |
| Omeprazole capsules | 30 (67) |
| Salbutamol inhaler | 19 (42) |
| Sulfamethoxazole/Trimethoprim suspension | 30 (67) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ongarora, D.; Karumbi, J.; Minnaard, W.; Abuga, K.; Okungu, V.; Kibwage, I. Medicine Prices, Availability, and Affordability in Private Health Facilities in Low-Income Settlements in Nairobi County, Kenya. Pharmacy 2019, 7, 40. https://doi.org/10.3390/pharmacy7020040
Ongarora D, Karumbi J, Minnaard W, Abuga K, Okungu V, Kibwage I. Medicine Prices, Availability, and Affordability in Private Health Facilities in Low-Income Settlements in Nairobi County, Kenya. Pharmacy. 2019; 7(2):40. https://doi.org/10.3390/pharmacy7020040
Chicago/Turabian StyleOngarora, Dennis, Jamlick Karumbi, Warnyta Minnaard, Kennedy Abuga, Vincent Okungu, and Isaac Kibwage. 2019. "Medicine Prices, Availability, and Affordability in Private Health Facilities in Low-Income Settlements in Nairobi County, Kenya" Pharmacy 7, no. 2: 40. https://doi.org/10.3390/pharmacy7020040