3.2. Discussion
The aim of the study, to identify differences regarding the method of estimation of pain within palliative care in north-eastern Sweden, was achieved. The results of the study showed an increased use of evidence-based assessment tools: a systematic pain management routine had been developed and implemented in the health care district. A systemized documentation system helped staff improve palliative care, as did visualization and awareness of pain management. Furthermore, the number of pain estimations increased when staff documented variation of pain, from “painlessness” to “worst possible pain”, in numbers instead of words; especially when number zero (“no pain”) was used. The documentation in numbers was easy to find and read in the medical records, and provided a clear, systematic way for documenting pain ratings. By rating patients’ experienced pain with evidence-based assessment tools on a scale from 0–10 (“no pain” to “worst possible pain”) instead of using words, a clear and systematic documentation system was developed. Furthermore, pain management routines also facilitated for uniform documentation in patients’ medical records; which is in line with earlier pain research [
4,
5,
6,
7,
8]. The conclusions of this paper could be described as learning outcomes through quality improvement in daily work (
Table 6).
Table 6.
.Key factorsfrom the currentstudy.
Table 6.
.Key factorsfrom the currentstudy.
Individual’s/team’s awareness and understanding of clinical practice Regular feedback—including verbal feedback—and follow-up on work methods and results throughout surveys Increased understanding of the significance of items, policies, evidence-based guidelines through double-loop learning facilitate for employee participation [ 5, 11, 12, 13] Dialogue and reflection about collaborative learning Do not blame: see every result as a possibility for improvement Reflect and share experiences with teams Positive working environment Understanding the value of evidence-based practices Using a sense of coherence (SOC) including comprehensibility, manageability, and meaningfulness [ 48]
|
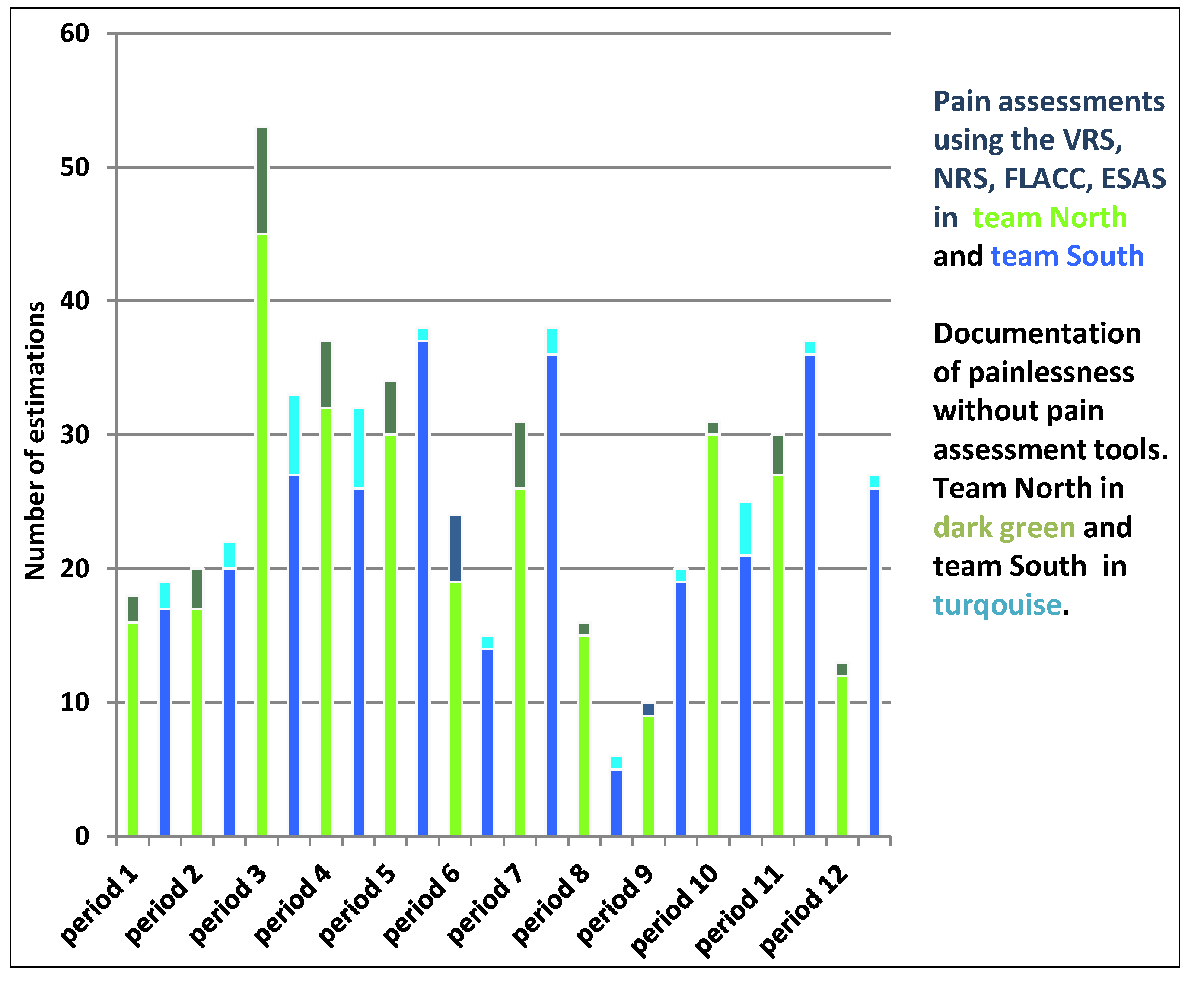
The results displayed some variability in the documentation of pain management, which could depend on difficulties to understand the value of documenting. However, the study showed an increased frequency of pain estimations including patients experiencing painlessness. The increase in pain management actions was also due to follow-up pain assessments for lower pain intensity estimations. In previous research, palliative care staff argued that the use of numbers clearly indicated patients’ need for pain management compared to documentation by words [
49]. Pain management research stresses that chronic pain is a problematic area since pain is a personal experience. Hence, staff has to work with person-centered care to achieve high-quality care [
50,
51].
Moreover, patients’ experiences and knowledge about pain assessment tools are changing, which is a key point in person-centered care [
52]. Therefore, it is significant to involve the teams around the patients in the decision-making process by using evidence-based assessment tools to help all actors develop high-quality pain management within palliative care. This is in line with research by Politi
et al. [
53] who stress the importance of interaction due to the impact that physicians’ communication of uncertainty has on both patients’ involvement in decisions and their satisfaction with health care decisions. Results showed that pain estimations performed by patients was the best way to handle pain management. Since evidence-based guidelines for pain management improve quality in palliative care, the staff has an obligation to improve the process of informed consent for patients.
Furthermore, the meaning of pain estimation for patients who experienced freedom of pain was a value in itself in this study. The change of method of estimate pain, using evidence-based tools for pain management benefited patient outcome due to increased pain assessments. However, there is a risk of misconception regarding documentation by numbers due to the nature of pain. As other researchers point out [
32,
33,
34], numbers are not enough; documentation needs to be complemented with pain localization, character of pain,
etc. to understand and provide optimal treatment.
The study showed an increased level of pain documentation (100%) even after the project ended. However, an increased awareness and understanding of patients’ pain experiences is not transferable to the estimation itself, which is why validated pain assessment instruments are crucial. The results displayed some variation in the teams concerning pain documentation, which could be explained by lack of equipment—such as a laptop—for documenting pain management when the staff visited patients in their homes [
49]. Palliative care research [
54] stresses the need for health information technology (HIT) and technical equipment such as adequate software, as well as for technical, analytical, and statistical support to facilitate for quality assessments and quality improvements. Furthermore, researchers highlight key factors such as engagement and involvement from stakeholders at all levels in the organization to draw attention to local needs. However, the lack of a laptop or other technical equipment for documentation affects work efficiency. In addition, the staff also needs to learn from others’ experiences to improve the quality of care [
55].
Another positive change was the awareness of the importance of objectively documenting all forms of patient estimations of pain during. The increased documentation of pain management using all patients’ pain assessments (from “painless” to “worst pain”) resulted in a majority of patient estimations being made visible for the staff. The contradictions that initially existed in the improvement work where that there were few notes in the medical records regarding patients’ experiences of intensity of pain. The staff’s experience of the pain was documented—not the patients’. Hence, the staff need feedback on work [
29,
30] and one way is by visualizing patients’ pain intensity. Improvement work can help reduce financial costs by using resources in a systematic way based on clinical guidelines that are grounded in research [
35,
36,
37,
38]. The quality of care could increase by examining key factors for palliative care processes, such as the pain management procedure. The staff’s pain management skills increased, which results in satisfaction and efficiency at work. Research shows that pain diagram patterns also help facilitate various diagnoses within rheumatology, but more research on pain patterns is needed [
56,
57]. In addition, research stresses the significance of self-reporting pain assessment tools as a first step toward effective and individualized treatments [
57], and as a way to systematize pain management work.
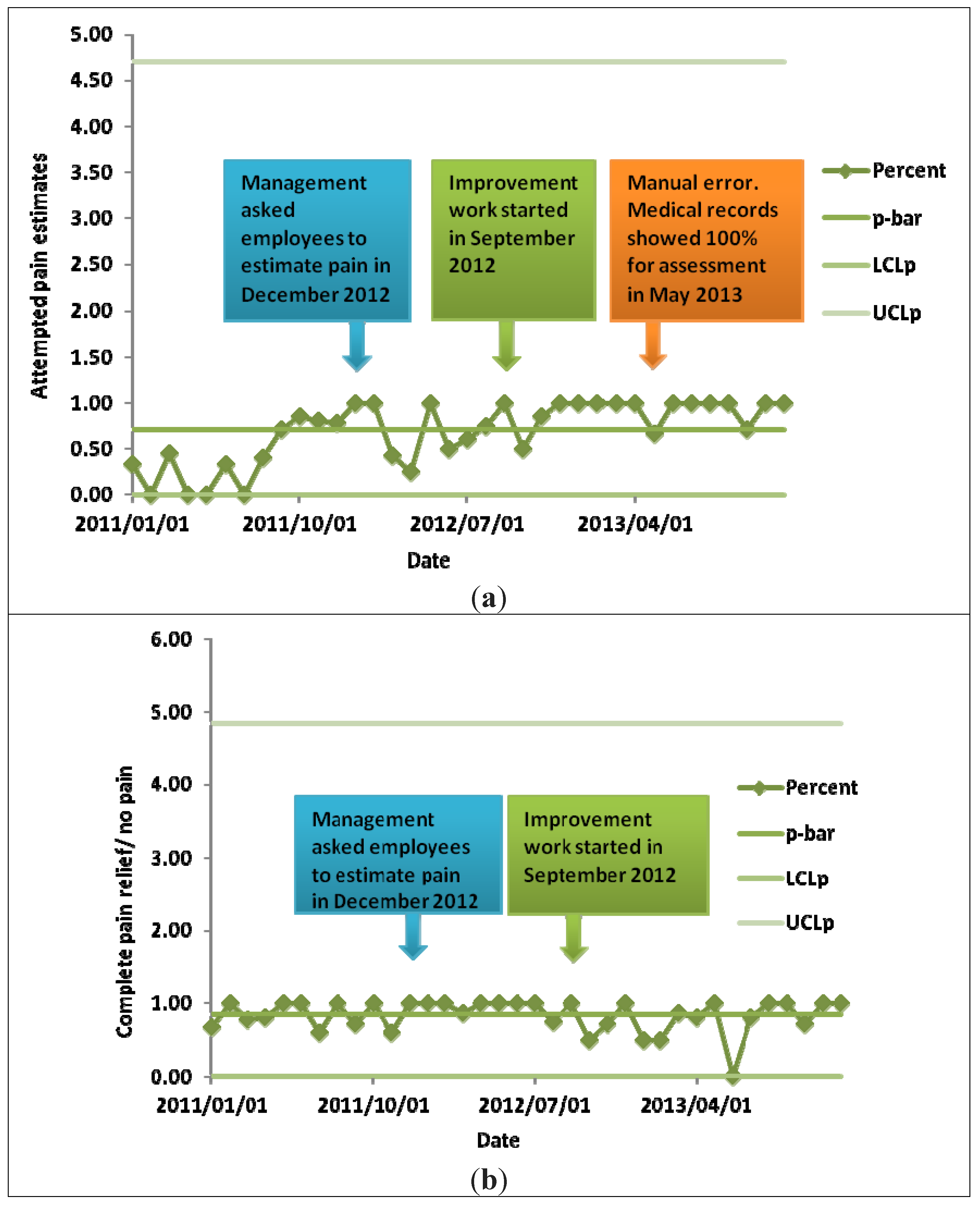
An interesting observation from the Swedish Palliative Registry [
41] was that 100% pain relief last week in life was reported for seven out of eight months. One issue to be addressed is what the results about patient pain relief would have been if pain assessments had not been performed. One hypothesis is that the staff would have responded based on their perceptions of patients’ pain.
An error occurred when the mortality surveys were manually uploaded to the Swedish Palliative Registry [
41]. The error resulted in an output of 67%–87% instead of 100% and illustrated the challenge for health care to handle errors in different systems to minimize mistakes concerning patient security [
57]. Research [
1,
4,
5,
6,
7,
8,
10] shows that the manual handling of activities in health systems contributes to increased mistakes with risks for patient security. The number of errors could be minimized by using mobile solutions that provide access to data as well as send data directly to the patient’s medical record for registration. Furthermore, patient empowerment could be achieved when patients can access their medical records through e-health from home and, hence, actively partake in their pain management. Researchers [
58,
59] highlight that there are challenges and opportunities associated with the use of new technologies and e-health applications. They advocate caution concerning the use of technological innovations and highlight that such innovations should be driven by users’ (patients’ and staff’s) needs instead of business people. Another perspective is the challenge of electronic systems in pain management. Here, further investigations, policies, and guidance are needed to investigate the monitoring and storage of data. Age-related differences concerning staff skills and use of technical solutions, as well as funding, working conditions,
etc., also need to be considered. Even though e-health offers opportunities for patients concerning pain management, the staff and managers must handle it with care [
49,
50,
51,
52].
In Sweden, 93% of the population has access to the Internet [
60]. Therefore, it is important to increase people’s awareness of reliable and trustworthy information on the Internet [
61]. A platform for e-health is being developed to coordinate the development of safe and effective health and social care. To improve health care, there is need for a national e-health infrastructure focusing on promoting public involvement and providing support for professionals and decision-makers [
62,
63]. Health professionals could help patients navigate through the abundance of pain information by posting evidence-based information on the Web.


{kind=link}
{kind=link}
{kind=link}


