
COVID-19 Patients’ Medication Management during Transition of Care from Hospital to Virtual Care: A Cross-Sectional Survey and Audit

 ,
, 
Abstract
:1. Introduction
- Evaluate patients’ potential medication-related risk factors;
- Explore patients’ medication management during transfer whilst in a virtual model of care;
- Obtain patients’ perspectives on the administration and management of their medicines whilst in a virtual model of care.
2. Methods
2.1. Study Sites/Settings
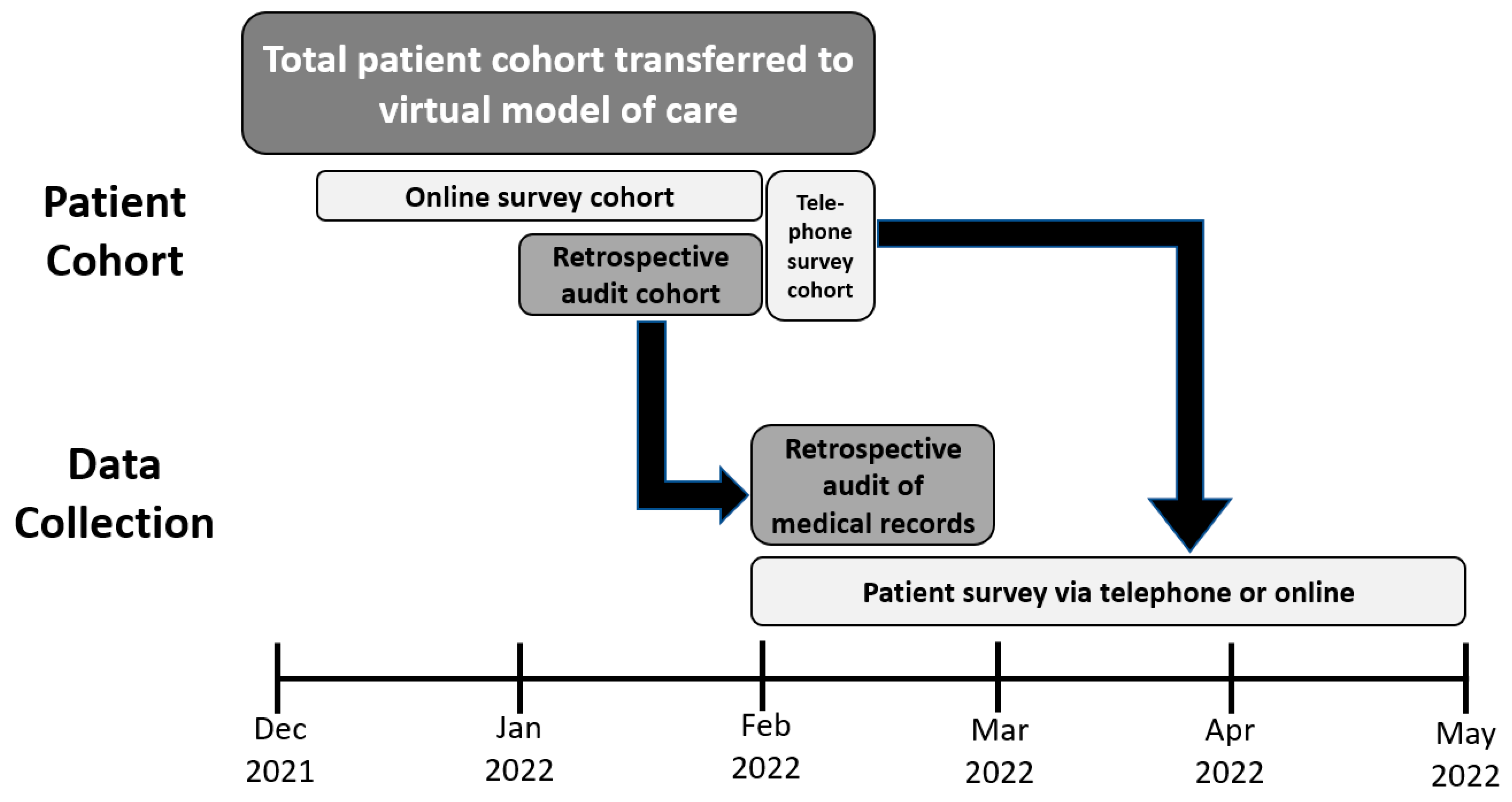
2.2. Data Sources
- 1.
- Patients’ medical records
- Patients’ demographic details (age, gender), including criteria recorded for their referral to virtual care;
- Medication details on admission to the hospital and transfer to a virtual model;
- If patients were prescribed a new high-risk medicine (i.e., was not prescribed the medicine prior to admission) during hospital admission or a transfer to a virtual model according to the APINCH classification system: anti-infectives, injections of potassium and other electrolytes, insulin, narcotics and other sedatives, chemotherapeutic agents, heparin and anticoagulants [37];
- Medication management services provided by pharmacists:
- ◦
- Pharmacist review during hospital admission;
- ◦
- Discharge medication record when transferred to a virtual model;
- Readmission within 30 days.
- 2.
- Patient surveys
2.3. Recruitment
2.4. Data Analysis
3. Results
3.1. Audit of Medical Records
3.2. Patient Surveys
“Medicine was left in a bag outside room door when left hospital and only instructions were on containers” P4
“I was concerned about getting Clexane® [subcutaneous anticoagulant].”P13
“While in the hospital I felt very supported and my medication was discussed with me by the Dr via phone on day one. He also supplied my daily medication to ensure I had my own supply for when I left quarantine. When transferred there was a lot of confusion and there were days I wasn’t contacted at all and days I was contacted by both the physical ward and virtual ward. Medications were not mentioned again.” P37
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare (AIHW). The First Year of COVID-19 in Australia: Direct and Indirect Health Effects; AIHW: Canberra, Australia, 2021. [Google Scholar]
- Waring, J.; Denis, J.-L.; Reff Pedersen, A.; Tenbensel, T. Organising Care in a Time of COVID-19: Implications for Leadership, Governance and Policy; Springer Nature: Berlin/Heidelberg, Germany, 2021. [Google Scholar] [CrossRef]
- Nicolás, D.; Coloma, E.; Pericàs, J.M. Alternatives to conventional hospitalisation that enhance health systems’ capacity to treat COVID-19. Lancet Infect. Dis. 2021, 21, 591–593. [Google Scholar] [CrossRef] [PubMed]
- de Souza, F.S.H.; Hojo-Souza, N.S.; Batista, B.D.O.; da Silva, C.M.; Guidoni, D.L. On the analysis of mortality risk factors for hospitalized COVID-19 patients: A data-driven study using the major Brazilian database. PLoS ONE 2021, 16, e0248580. [Google Scholar] [CrossRef]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Haugstetter, C.; Mason, R.; Sanmugarajah, J.; Hattingh, H.L. Evaluation of a new emergency department avoidance model of care, the Cancer Urgent Assessment Clinic, in response to the COVID-19 pandemic. Emerg. Cancer Care 2022, 1, 11. [Google Scholar] [CrossRef]
- Weaver, M.J.; Mok, D.; Hughes, I.; Hattingh, H.L. Effect of a senior cardiology nursing role on streamlining assessment of emergency cardiology presentations during COVID-19: An observational study. Heart Lung Circ. 2023, in press. [CrossRef]
- Australian Government Department of Health. Impact of COVID-19. Available online: https://www.health.gov.au/resources/publications/impact-of-covid-19-in-australia-ensuring-the-health-system-can-respond (accessed on 5 June 2023).
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. How the COVID-19 pandemic is favoring the adoption of digital technologies in healthcare: A literature review. medRxiv 2020. [Google Scholar] [CrossRef]
- Gunasekeran, D.V.; Tham, Y.-C.; Ting, D.S.; Tan, G.S.; Wong, T.Y. Digital health during COVID-19: Lessons from operationalising new models of care in ophthalmology. Lancet Digit. Health 2021, 3, e124–e134. [Google Scholar] [CrossRef]
- Temesgen, Z.M.; DeSimone, D.C.; Mahmood, M.; Libertin, C.R.; Palraj, B.R.V.; Berbari, E.F. Health care after the COVID-19 pandemic and the influence of telemedicine. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2020; pp. S66–S68. [Google Scholar]
- Crotty, B.H.; Dong, Y.; Laud, P.; Hanson, R.J.; Gershkowitz, B.; Penlesky, A.C.; Shah, N.; Anderes, M.; Green, E.; Fickel, K.; et al. Hospitalization Outcomes Among Patients with COVID-19 Undergoing Remote Monitoring. JAMA Netw. Open 2022, 5, e2221050. [Google Scholar] [CrossRef]
- Leite, H.; Lindsay, C.; Kumar, M. COVID-19 outbreak: Implications on healthcare operations. TQM J. 2020, 33, 247–256. [Google Scholar] [CrossRef]
- Jonnagaddala, J.; Godinho, M.A.; Liaw, S.-T. From telehealth to virtual primary care in Australia? A Rapid scoping review. Int. J. Med. Inform. 2021, 151, 104470. [Google Scholar] [CrossRef] [PubMed]
- Nundy, S.; Patel, K.K. Hospital-at-Home to Support COVID-19 Surge-Time to Bring Down the Walls? JAMA Health Forum 2020, 1, e200504. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health. COVID-19 Vaccines. Available online: https://www.health.gov.au/initiatives-and-programs/covid-19-vaccines/covid-19-vaccines (accessed on 5 June 2023).
- Nester, T.M.; Hale, L.S. Effectiveness of a pharmacist-acquired medication history in promoting patient safety. Am. J. Health Syst. Pharm. 2002, 59, 2221–2225. [Google Scholar] [CrossRef]
- Hung, P.-L.; Chen, J.-Y.; Chen, M.-T.; Li, P.-L.; Li, W.-C.; Wang, Z.-C.; Huang, T.-T.; Liang, Y.-T.; Lin, P.-C. The impact of a medication reconciliation programme at geriatric hospital admission: A pre-/postintervention study. Br. J. Clin. Pharmacol. 2019, 85, 2614–2622. [Google Scholar] [CrossRef]
- Zipf, N.; Grant, L.; Robinson, B.; Teasdale, T.; Grant, G.; Hattingh, H.L. Analysis of inpatient and high-risk medicine pharmacist interventions associated with insulin prescribing for hospital inpatients with diabetes. Int. J. Clin. Pharm. 2021, 43, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Ooi, C.E.; Rofe, O.; Vienet, M.; Elliott, R.A. Improving communication of medication changes using a pharmacist-prepared discharge medication management summary. Int. J. Clin. Pharm. 2017, 39, 394–402. [Google Scholar] [CrossRef]
- Knight, D.A.; Thompson, D.; Mathie, E.; Dickinson, A. Dickinson, A. ‘Seamless care? Just a list would have helped!’ Older people and their carer’s experiences of support with medication on discharge home from hospital. Health Expect. 2013, 16, 277–291. [Google Scholar] [CrossRef]
- Tong, E.Y.; Roman, C.P.; Mitra, B.; Yip, G.S.; Gibbs, H.; Newnham, H.H.; Smit, D.V.; Galbraith, K.; Dooley, M.J. Reducing medication errors in hospital discharge summaries: A randomised controlled trial. Med. J. Aust. 2017, 206, 36–39. [Google Scholar] [CrossRef]
- Michaelsen, M.H.; McCague, P.; Bradley, C.P.; Sahm, L.J.J.P. Medication reconciliation at discharge from hospital: A systematic review of the quantitative literature. Pharmacy 2015, 3, 53–71. [Google Scholar] [CrossRef]
- Mekonnen, A.B.; McLachlan, A.J.; Brien, J.-A.E. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: A systematic review and meta-analysis. BMJ Open 2016, 6, e010003. [Google Scholar] [CrossRef]
- Montalto, M.; McElduff, P.; Hardy, K. Home ward bound: Features of hospital in the home use by major Australian hospitals, 2011–2017. Med. J. Aust. 2020, 213, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Caplan, G.A.; Sulaiman, N.S.; Mangin, D.A.; Aimonino Ricauda, N.; Wilson, A.D.; Barclay, L. A meta-analysis of “hospital in the home”. Med. J. Aust. 2012, 197, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Kovačević, M.; Ćulafić, M.; Vezmar Kovačević, S.; Borjanić, S.; Keleč, B.; Miljković, B.; Amidžić, R. Telepharmacy service experience during the COVID-19 pandemic in the Republic of Srpska, Bosnia and Herzegovina. Health Soc. Care Community 2021, 30, e1639–e1650. [Google Scholar] [CrossRef] [PubMed]
- Paudyal, V.; Cadogan, C.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Stewart, D. Provision of clinical pharmacy services during the COVID-19 pandemic: Experiences of pharmacists from 16 European countries. Res. Soc. Adm. Pharm. 2021, 17, 1507–1517. [Google Scholar] [CrossRef]
- Pedersen, C.A.; Schneider, P.J.; Ganio, M.C.; Scheckelhoff, D.J. ASHP national survey of pharmacy practice in hospital settings: Impact of COVID-19 pandemic on pharmacy operations-2020. Am. J. Health Syst. Pharm. 2021, 78, 1701–1712. [Google Scholar] [CrossRef]
- Akour, A.; Elayeh, E.; Tubeileh, R.; Hammad, A.; Ya’Acoub, R.; Al-Tammemi, A.B. Role of community pharmacists in medication management during COVID-19 lockdown. Pathog. Glob. Health 2021, 115, 168–177. [Google Scholar] [CrossRef]
- Zozaya, N.; González-Domínguez, A.; Calvente, N.; de la Plaza, R.; Herranz, A.; Blanes, A.; Tamayo, M. Continuity of care between hospital pharmacies and community pharmacies, and costs avoided: A pilot experience in times of COVID-19 in Spain. Glob. Reg. Health Technol. Assess. 2021, 8, 8–13. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2007, 61, 344–349. [Google Scholar] [CrossRef]
- van Walraven, C.; Dhalla, I.A.; Bell, C.; Etchells, E.; Stiell, I.G.; Zarnke, K.; Austin, P.C.; Forster, A.J. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. CMAJ 2010, 182, 551–557. [Google Scholar] [CrossRef]
- MD+CALC. LACE Index for Readmisison. Available online: https://www.mdcalc.com/ (accessed on 13 August 2022).
- Gruneir, A.; Dhalla, I.A.; van Walraven, C.; Fischer, H.D.; Camacho, X.; Rochon, P.A.; Anderson, G.M. Unplanned readmissions after hospital discharge among patients identified as being at high risk for readmission using a validated predictive algorithm. Open Med. 2011, 5, 104–111. [Google Scholar]
- Clinical Excellence Commisssion. A Pinch. Available online: https://www.cec.health.nsw.gov.au/keep-patients-safe/medication-safety/high-risk-medicines/A-PINCH (accessed on 14 September 2022).
- Rognan, S.E.; Kalvemark-Sporrong, S.; Bengtsson, K.R.; Lie, H.B.; Andersson, Y.; Mowe, M.; Mathiesen, L. Empowering the patient? Medication communication during hospital discharge: A qualitative study at an internal medicines ward in Norway. BMJ Open 2021, 11, e044850. [Google Scholar] [CrossRef] [PubMed]
- Sharara, S.L.; Arbaje, A.I.; Cosgrove, S.E.; Gurses, A.P.; Dzintars, K.; Ladikos, N.; Qasba, S.S.; Keller, S.C. The Voice of the Patient: Patient Roles in Antibiotic Management at the Hospital-to-Home Transition. J. Patient Saf. 2021, 23, 23. [Google Scholar] [CrossRef]
- Queensland Government Queensland Health. Patient Reported Experience Survey—Care for COVID-19. Survey NRCNndNRAI. 2021. Available online: https://www.qld.gov.au/health/services/preom (accessed on 14 September 2022).
- Chan, A.H.Y.; Horne, R.; Hankins, M.; Chisari, C. The Medication Adherence Report Scale: A measurement tool for eliciting patients’ reports of nonadherence. Br. J. Clin. Pharmacol. 2020, 86, 1281–1288. [Google Scholar] [CrossRef]
- Raffan, F.; Anderson, T.; Sinclair, T.; Shaw, M.; Amanatidis, S.; Thapa, R.; Nilsson, S.J.; Jagers, D.; Wilson, A.; Haigh, F. The Virtual Care Experience of Patients Diagnosed with COVID-19. J. Patient Exp. 2021, 8, 23743735211008310. [Google Scholar] [CrossRef] [PubMed]
- Hammersley, V.; Donaghy, E.; Parker, R.; McNeilly, H.; Atherton, H.; Bikker, A.; Campbell, J.; McKinstry, B. Comparing the content and quality of video, telephone, and face-to-face consultations: A non-randomised, quasi-experimental, exploratory study in UK primary care. Br. J. Gen. Pract. 2019, 69, e595–e604. [Google Scholar] [CrossRef] [PubMed]
- Keesara, S.; Jonas, A.; Schulman, K. COVID-19 and health care’s digital revolution. N. Engl. J. Med. 2020, 382, e82. [Google Scholar] [CrossRef]
- Hollander, J.E.; Carr, B.G. Virtually Perfect? Telemedicine for COVID-19. N. Engl. J. Med. 2020, 382, 1679–1681. [Google Scholar] [CrossRef]
- Pericàs, J.M.; Cucchiari, D.; Torrallardona-Murphy, O.; Calvo, J.; Serralabós, J.; Alvés, E.; Agelet, A.; Hidalgo, J.; Alves, E.; Castells, E.; et al. Hospital at home for the management of COVID-19: Preliminary experience with 63 patients. Infection 2021, 49, 327–332. [Google Scholar] [CrossRef]
- Schwamm, L.H.; Estrada, J.; Erskine, A.; Licurse, A. Virtual care: New models of caring for our patients and workforce. Lancet Digit. Health 2020, 2, e282–e285. [Google Scholar] [CrossRef]
- Grutters, L.A.; Majoor, K.I.; Mattern, E.S.K.; Hardeman, J.A.; van Swol, C.F.P.; Vorselaars, A.D.M. Home telemonitoring makes early hospital discharge of COVID-19 patients possible. J. Am. Med. Inform. Assoc. 2020, 27, 1825–1827. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Medication Safety in Transitions of Care; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Donaldson, L.J.; Kelley, E.T.; Dhingra-Kumar, N.; Kieny, M.-P.; Sheikh, A. Medication without Harm: WHO’s Third Global Patient Safety Challenge. Lancet 2017, 389, 1680–1681. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.J.; Clark, H.D.; Menard, A.; Dupuis, N.; Chernish, R.; Chandok, N.; Khan, A.; Van Walraven, C. Adverse events among medical patients after discharge from hospital. CMAJ 2004, 170, 345–349. [Google Scholar]
- Krumholz, H.M. Post-Hospital Syndrome—An Acquired, Transient Condition of Generalized Risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Parekh, N.; Ali, K.; Page, A.; Roper, T.; Rajkumar, C. Incidence of Medication-Related Harm in Older Adults after Hospital Discharge: A Systematic Review. J. Am. Geriatr. Soc. 2018, 66, 1812–1822. [Google Scholar] [CrossRef] [PubMed]
- Parekh, N.; Ali, K.; Stevenson, J.M.; Davies, J.G.; Schiff, R.; Van der Cammen, T.; Harchowal, J.; Raftery, J.; Rajkumar, C.; on behalf of the PRIME Study Group. Incidence and cost of medication harm in older adults following hospital discharge: A multicentre prospective study in the UK: Incidence and cost of medication harm in older adults. Br. J. Clin. Pharmacol. 2018, 84, 1789–1797. [Google Scholar] [CrossRef]
- Pharmaceutical Society of Australia. Medicine Safety: Take Care; Pharmaceutical Society of Australia: Canberra, Australia, 2019. [Google Scholar]
- Bishop, M.A.; Cohen, B.A.; Billings, L.K.; Thomas, E.V. Reducing errors through discharge medication reconciliation by pharmacy services. Am. J. Health Syst. Pharm. 2015, 72, S120–S126. [Google Scholar] [CrossRef]
- Sebaaly, J.; Parsons, L.B.; Pilch, N.A.; Bullington, W.; Hayes, G.L.; Piasterling, H.J.H.P. Clinical and financial impact of pharmacist involvement in discharge medication reconciliation at an academic medical center: A prospective pilot study. Hosp. Pharm. 2015, 50, 505–513. [Google Scholar] [CrossRef]
- Berry, D.C.; Raynor, D.K.; Knapp, P.; Bersellini, E. Patients’ Understanding of Risk Associated with Medication Use. Drug Saf. 2003, 26, 1–11. [Google Scholar] [CrossRef]
- Taitel, M.; Jiang, J.; Rudkin, K.; Ewing, S.; Duncan, I. The impact of pharmacist face-to-face counseling to improve medication adherence among patients initiating statin therapy. Patient Prefer. Adherence 2012, 6, 323–329. [Google Scholar] [CrossRef]
- van Erkel, F.M.; Pet, M.J.; Bossink, E.H.; van de Graaf, C.F.M.; Hodes, M.T.J.; van Ogtrop, S.N.; Mourits, M.J.E.; Welker, G.A.; Halmos, G.B.; van Leeuwen, B.; et al. Experiences of patients and health care professionals on the quality of telephone follow-up care during the COVID-19 pandemic: A large qualitative study in a multidisciplinary academic setting. BMJ Open 2022, 12, e058361. [Google Scholar] [CrossRef]
- Merks, P.; Cameron, J.D.; Balcerzak, M.; Religioni, U.; Świeczkowski, D.; Konstanty, M.; Hering, D.; Szymański, F.M.; Jaguszewski, M.; Vaillancourt, R. Evaluation of a pharmacist-led intervention to improve medication adherence in patients initiating dabigatran treatment: A comparison with standard pharmacy practice in Poland. BMC Prim. Care 2022, 23, 210. [Google Scholar] [CrossRef] [PubMed]
- Wise, S.; Coleshill, M.J.; Taylor, N.; Le, M.; Debono, D.; Day, R.O.; Melocco, T.; Baysari, M.; Laba, T.; Carland, J.E. Australian hospital outpatient pharmacies: Service adaptations during the 2020 national coronavirus disease 2019 lockdown. J. Pharm. Pract. Res. 2022, 52, 326–328. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Mean | SD |
|---|---|---|
| Age (years) | 58.8 | 19.8 |
| Length of stay | Mean | SD |
| In hospital (days) | 3.0 | 1.7 |
| In virtual ward (days) | 4.4 | 2.1 |
| Virtual model of care | n/% | |
| Virtual ward | 86 | |
| Hospital-In-The-Hotel | 14 | |
| Number of patients with risk factors for medication-related harm (some had multiple) | n/% | |
| Vision impairment | 3 | |
| Mobility/Dexterity impairment/Frail/Pressure injury risk | 32 | |
| Fall risk | 15 | |
| Communication difficulty | 6 | |
| Cognitive impairment/Dementia/Mental health issues | 5 | |
| Number of patients with risk factors for medication-related harm | n/% | |
| No risk factors | 58 | |
| One risk factor | 25 | |
| Two risk factors | 15 | |
| Three risk factors | 2 | |
| Medication use | Mean | SD |
| Number of medicines at admission per patient | 4.3 | 4.0 |
| Number of new high-risk medicine in hospital per patient | 2.5 | 1.6 |
| Number of new high-risk medicine in virtual model of care per patient | 0.5 | 0.7 |
| Patients on new high-risk medicines whilst in hospital | n/% | |
| No high-risk medicines | 8 | |
| One high-risk medicine | 22 | |
| Two high-risk medicines | 25 | |
| Three high-risk medicines | 19 | |
| Four high-risk medicines | 12 | |
| Five high-risk medicines | 7 | |
| Six high-risk medicines | 7 | |
| Type of high-risk medicine (some on multiple) | ||
| Anti-infectives | 47 | |
| Injections of potassium and other electrolytes | 13 | |
| Insulin | 13 | |
| Narcotics/sedatives | 36 | |
| Chemotherapeutic agents | 0 | |
| Heparin and other anticoagulants | 80 | |
| Patients on new high-risk medicines whilst in virtual model | n/% | |
| No high-risk medicines | 60 | |
| One high-risk medicine | 31 | |
| Two high-risk medicines | 7 | |
| Three high-risk medicines | 2 | |
| Type of high-risk medicine (some on multiple) | ||
| Anti-infectives | 27 | |
| Injections of potassium and other electrolytes | 0 | |
| Insulin | 4 | |
| Narcotics/sedatives | 11 | |
| Chemotherapeutic agents | 0 | |
| Heparin and other anticoagulants | 4 | |
| Medication management services | ||
| Received pharmacist review | 43 | |
| Received discharge medicine list | 29 | |
| Received discharge summary | 48 | |
| Risk Factor for Medication-Related Harm | No. with Risk Factor | Received Pharmacist Review (%) | Received Pharmacist Discharge Medication List (%) | ||||
|---|---|---|---|---|---|---|---|
| n (%) | 95% Confidence Interval | * p-Value | n (%) | 95% Confidence Interval | * p-Value | ||
| Vision impairment | 3 | 0 | - | 0.257 | 0 | - | 0.554 |
| Mobility/Dexterity impairment/Frail/Pressure injury risk | 32 | 14 (43.8%) | 0.273; 0.617 | 1.000 | 9 (28.1%) | 0.149; 0.466 | 1.000 |
| Fall risk | 15 | 6 (40.0%) | 0.177; 0.674 | 1.000 | 3 (20.0%) | 0.059; 0.500 | 0.543 |
| Communication difficulty | 6 | 2 (33.3%) | 0.051; 0.822 | 0.697 | 2 (33.3%) | 0.051; 0.822 | 1.000 |
| Cognitive impairment/Dementia/Mental health issues | 5 | 2 (40.0%) | 0.050; 0.894 | 1.000 | 2 (40.0%) | 0.050; 0.894 | 0.626 |
| Stroke | 3 | 2 (66.7%) | 0.010; 0.997 | 0.576 | 1 (33.3%) | 0.003; 0.990 | 1.000 |
| Any risk factor | 42 | 17 (40.5% | 0.265; 0.562 | 0.688 | 12 (28.6%) | 0.167; 0.444 | 1.000 |
| New High-Risk Medicine (HRM) | Hospital Admission/Inpatient Unit Stay | Transfer to Virtual Model | ||||||
|---|---|---|---|---|---|---|---|---|
| No. on New HRM | No. Received Pharmacist Medication Review (%) | 95% Confidence Interval | * p-Value | No. on New HRM | No. Received Pharmacist Discharge Medication List (%) | 95% Confidence Interval | * p-Value | |
| Anti-infectives | 47 | 23 (48.9%) | 0.348; 0.633 | 0.313 | 27 | 11 (40.7%) | 0.235; 0.606 | 0.139 |
| Injections of potassium and other electrolytes | 13 | 8 (61.5%) | 0.316; 0.847 | 0.229 | 0 | 0 | - | - |
| Insulin | 13 | 7 (53.9%) | 0.258; 0.797 | 0.550 | 4 | 0 | - | 0.320 |
| Narcotics/sedatives | 36 | 15 (41.7%) | 0.264; 0.587 | 1.000 | 11 | 3 (27.3%) | 0.766; 0.629 | 1.000 |
| Chemotherapeutic agents | 0 | 0 | - | - | 0 | 0 | - | - |
| Heparin and other anticoagulants | 80 | 34 (42.5%) | 0.320; 0.537 | 1.000 | 4 | 2 (50%) | 0.040; 0.060 | 0.578 |
| Any high-risk medicine | 92 | 41 (44.6%) | 0.346; 0.549 | 0.460 | 40 | 14 (35.0%) | 0.216; 0.513 | 0.369 |
| Question | Yes | No | Unsure | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Did one of the staff members talk to you about how to use your medicines when you left the hospital ward? (n = 95) | 51 | 53.7 | 39 | 41.1 | 5 | 5.3 |
| Did you receive a written list of your medicines with instructions on how to use them when you left the hospital ward? (n = 95) | 37 | 39.0 | 49 | 51.6 | 9 | 9.5 |
| Did your medicines change whilst you were in hospital? (n = 95) | 35 | 36.8 | 49 | 51.6 | 11 | 11.6 |
| Do you believe that the information you received from the hospital about your medicines when you were transferred was adequate for you to know how to take your medicine? (n = 94) | 66 | 70.2 | 19 | 20.2 | 9 | 9.6 |
| Did you have enough supply of your medicines whilst at home or hotel? (n = 94) | 67 | 71.3 | 18 | 19.2 | 9 | 9.6 |
| Did you receive advice about how to take your medicines while at home or in the hotel? (n = 94) | 52 | 55.3 | 33 | 35.1 | 9 | 9.6 |
| Did you have the opportunity to ask questions about your medicines whilst at home or in the hotel? (n = 92) | 47 | 51.1 | 34 | 37.0 | 11 | 12.0 |
| Do you have a special way to help you remember to take your medicines? (n = 92) | 29 | 31.5 | 54 | 58.7 | 9 | 9.8 |
| Did you miss any medicine doses whilst at home or in the hotel? (n = 92) | 8 | 8.7 | 77 | 83.7 | 7 | 7.6 |
| Did you know how to contact a hospital pharmacist for assistance while you were at home or in the hotel if you needed support? (n = 92) | 49 | 53.3 | 36 | 39.1 | 7 | 7.6 |
| Was there a time you wanted to speak to a hospital pharmacist about your medicines while you were at home or in the hotel, but failed to make contact? (n = 92) | 6 | 6.5 | 76 | 82.6 | 10 | 10.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hattingh, H.L.; Edmunds, C.; Buksh, S.; Cronin, S.; Gillespie, B.M. COVID-19 Patients’ Medication Management during Transition of Care from Hospital to Virtual Care: A Cross-Sectional Survey and Audit. Pharmacy 2023, 11, 157. https://doi.org/10.3390/pharmacy11050157
Hattingh HL, Edmunds C, Buksh S, Cronin S, Gillespie BM. COVID-19 Patients’ Medication Management during Transition of Care from Hospital to Virtual Care: A Cross-Sectional Survey and Audit. Pharmacy. 2023; 11(5):157. https://doi.org/10.3390/pharmacy11050157
Chicago/Turabian StyleHattingh, H. Laetitia, Catherine Edmunds, Saberina Buksh, Sean Cronin, and Brigid M. Gillespie. 2023. "COVID-19 Patients’ Medication Management during Transition of Care from Hospital to Virtual Care: A Cross-Sectional Survey and Audit" Pharmacy 11, no. 5: 157. https://doi.org/10.3390/pharmacy11050157