


Evaluation of Systemic Antifungal Use in a Latin American General Care Hospital: A Retrospective Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethics Approval and Consent to Participate
3. Results
3.1. Patient Demographics and Comorbidities
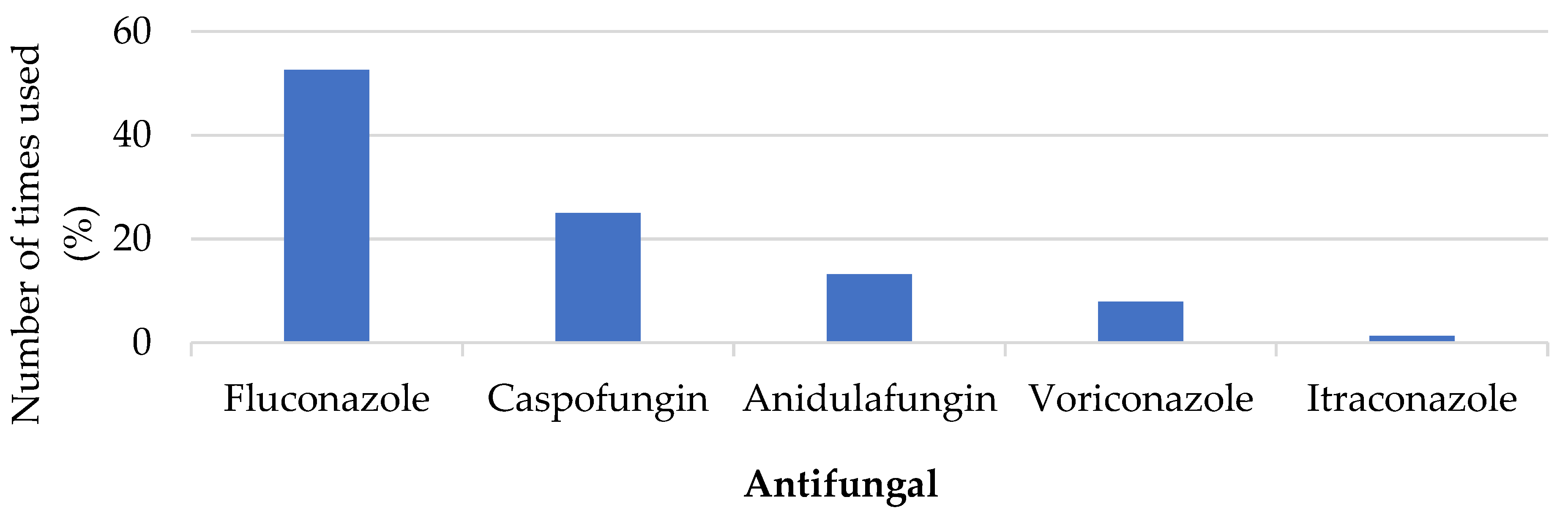
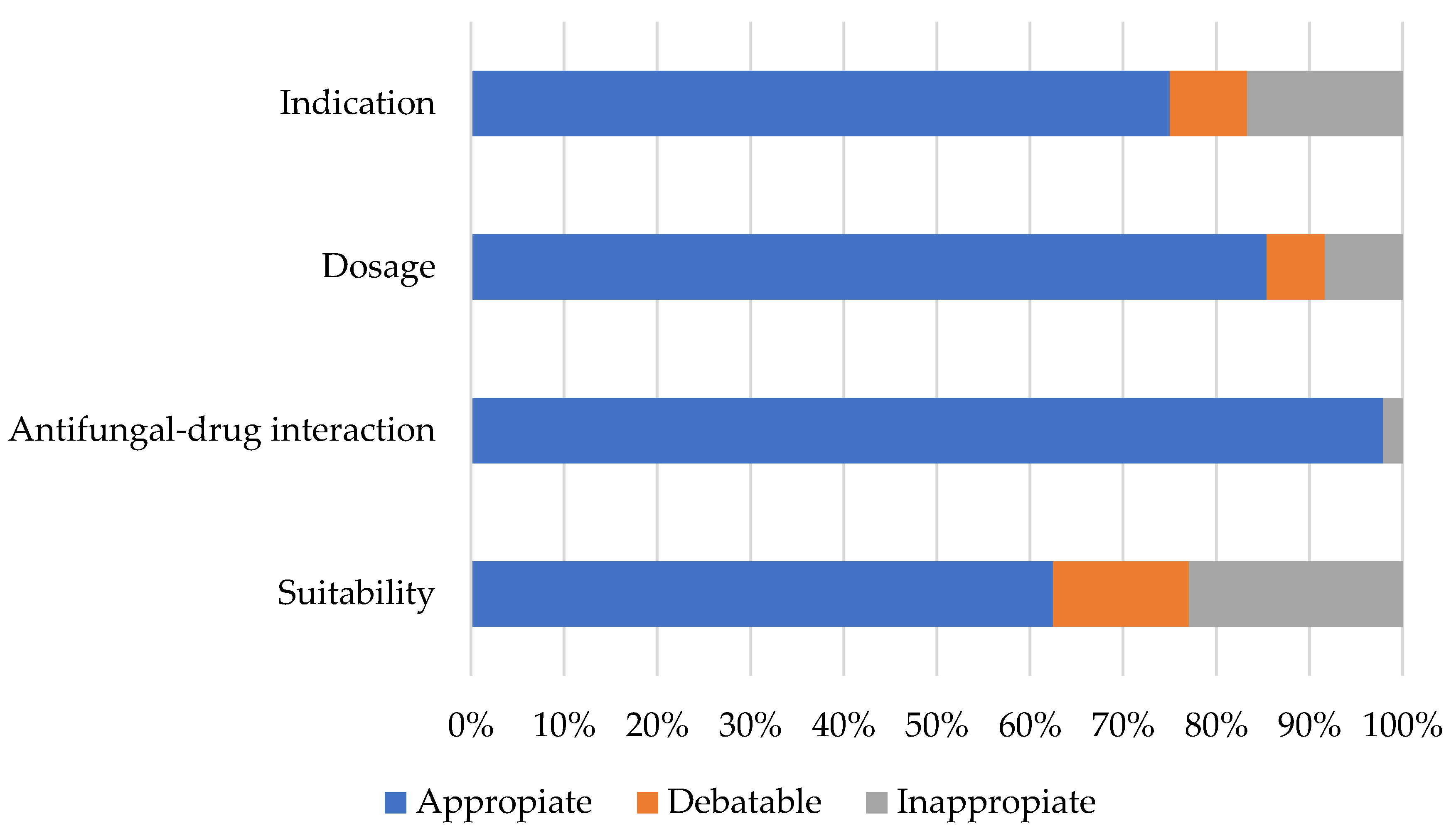
3.2. Antifungal Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Suleyman, G.; Alangaden, G.J. Nosocomial Fungal Infections. Infect. Dis. Clin. N. Am. 2021, 35, 1027–1053. [Google Scholar] [CrossRef] [PubMed]
- Jenks, J.D.; Cornely, O.A.; Chen, S.C.A.; Thompson, G.R.; Hoenigl, M. Breakthrough Invasive Fungal Infections: Who Is at Risk? Mycoses 2020, 63, 1021–1032. [Google Scholar] [CrossRef]
- Wiederhold, N.P. Emerging Fungal Infections: New Species, New Names, and Antifungal Resistance. Clin. Chem. 2021, 68, 83–90. [Google Scholar] [CrossRef]
- Schouten, J.; De Waele, J.; Lanckohr, C.; Koulenti, D.; Haddad, N.; Rizk, N.; Sjövall, F.; Kanj, S.S. Antimicrobial Stewardship in the ICU in COVID-19 Times: The Known Unknowns. Int. J. Antimicrob. Agents 2021, 58, 106409. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Carvalhaes, C.G.; DeVries, S.; Rhomberg, P.R.; Castanheira, M. Impact of COVID-19 on the Antifungal Susceptibility Profiles of Isolates Collected in a Global Surveillance Program That Monitors Invasive Fungal Infections. Med. Mycol. 2022, 60, myac028. [Google Scholar] [CrossRef]
- Spallone, A.; Schwartz, I.S. Emerging Fungal Infections. Infect. Dis. Clin. N. Am. 2021, 35, 261–277. [Google Scholar] [CrossRef] [PubMed]
- Asai, N.; Ohashi, W.; Sakanashi, D.; Suematsu, H.; Kato, H.; Hagihara, M.; Watanabe, H.; Shiota, A.; Koizumi, Y.; Yamagishi, Y.; et al. Combination of Sequential Organ Failure Assessment (SOFA) Score and Charlson Comorbidity Index (CCI) Could Predict the Severity and Prognosis of Candidemia More Accurately than the Acute Physiology, Age, Chronic Health Evaluation II (APACHE II) Score. BMC Infect. Dis. 2021, 21, 77. [Google Scholar] [CrossRef]
- Tunay, B.; Aydin, S. Investigation of Inflammation-Related Parameters in Patients with Candidemia Hospitalized in the Intensive Care Unit: A Retrospective Cohort Study. Sci. Prog. 2022, 105, 003685042211240. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Zhong, M.K.; Xu, H.B.; Li, L. Development and Validation of a Risk Score for Predicting Invasive Fungal Infectious in an Intensive Care Unit. Pharmazie 2013, 68, 459–464. [Google Scholar] [CrossRef]
- Ebihara, F.; Maruyama, T.; Kikuchi, K.; Kimura, T.; Hamada, Y. Antifungal Stewardship Task Shifting Required of Pharmacists. Med. Mycol. J. 2022, 63, 109–117. [Google Scholar] [CrossRef]
- Ray, A.; Das, A.; Panda, S. Antifungal Stewardship: What We Need to Know. IJDVL 2022, 89, 5–11. [Google Scholar] [CrossRef]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA Score to Assess the Incidence of Organ Dysfunction/Failure in Intensive Care Units: Results of a Multicenter, Prospective Study. Crit. Care Med. 1998, 26, 1793. [Google Scholar] [CrossRef] [Green Version]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA Score—Development, Utility and Challenges of Accurate Assessment in Clinical Trials. Crit Care 2019, 23, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Issa El-Hussain, F.; Balkhair, A.; Al-Zakwani, I.; Al Za’abi, M. Appropriateness of Antifungal Prescribing in Oman. Pharm. Pract. 2022, 20, 2613. [Google Scholar] [CrossRef] [PubMed]
- Nivoix, Y.; Launoy, A.; Lutun, P.; Moulin, J.-C.; Phai Pang, K.-A.; Fornecker, L.-M.; Wolf, M.; Leveque, D.; Letscher-Bru, V.; Beretz, L.; et al. Adherence to Recommendations for the Use of Antifungal Agents in a Tertiary Care Hospital. J. Antimicrob. Chemother. 2012, 67, 2506–2513. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [Green Version]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [Green Version]
- Kelly, B.T.; Pennington, K.M.; Limper, A.H. Advances in the Diagnosis of Fungal Pneumonias. Expert Rev. Respir. Med. 2020, 14, 703–714. [Google Scholar] [CrossRef]
- Poplin, V.; Boulware, D.R.; Bahr, N.C. Methods for Rapid Diagnosis of Meningitis Etiology in Adults. Biomark. Med. 2020, 14, 459–479. [Google Scholar] [CrossRef] [Green Version]
- Asai, N.; Watanabe, H.; Shiota, A.; Kato, H.; Sakanashi, D.; Hagihara, M.; Koizumi, Y.; Yamagishi, Y.; Suematsu, H.; Mikamo, H. Could QSOFA and SOFA Score Be Correctly Estimating the Severity of Healthcare-Associated Pneumonia? J. Infect. Chemother. 2018, 24, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Rüddel, D.O.; Schlattmann, P.; Pletz, M.; Kurzai, O.; Bloos, F. Risk Factors for Invasive Candida Infection in Critically Ill Patients. Chest 2022, 161, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Lionakis, M.S.; Arendrup, M.C.; Ostrosky-Zeichner, L.; Kullberg, B.J. Invasive Candidiasis. Nat. Rev. Dis. Prim. 2018, 4, 18026. [Google Scholar] [CrossRef]
- Talento, A.F.; Qualie, M.; Cottom, L.; Backx, M.; White, P.L. Lessons from an Educational Invasive Fungal Disease Conference on Hospital Antifungal Stewardship Practices across the UK and Ireland. JoF 2021, 7, 801. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou-Olivgeris, M.; Andrianaki, A.M.; Marangos, M.; Sipsas, N.; Apostolidi, E.A.; Maltezos, E.; Panagopoulos, P.; Karapiperis, D.; Arvaniti, K.; Perdikouri, E.-I.; et al. Hospital-Wide Antifungal Prescription in Greek Hospitals: A Multicenter Repeated Point-Prevalence Study. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 243–248. [Google Scholar] [CrossRef]
- Butts, A.; Reitler, P.; Nishimoto, A.T.; DeJarnette, C.; Estredge, L.R.; Peters, T.L.; Veve, M.P.; Rogers, P.D.; Palmer, G.E. A Systematic Screen Reveals a Diverse Collection of Medications That Induce Antifungal Resistance in Candida Species. Antimicrob. Agents Chemother. 2019, 63, e00054-19. [Google Scholar] [CrossRef] [Green Version]
- Boonstra, J.M.; Märtson, A.G.; Sandaradura, I.; Kosterink, J.G.W.; van der Werf, T.S.; Marriott, D.J.E.; Zijlstra, J.G.; Touw, D.J.; Alffenaar, J.W.C. Optimization of Fluconazole Dosing for the Prevention and Treatment of Invasive Candidiasis Based on the Pharmacokinetics of Fluconazole in Critically Ill Patients. Antimicrob. Agents Chemother. 2021, 65, e01554-20. [Google Scholar] [CrossRef]
- Fischer, M.A.; Winkelmayer, W.C.; Rubin, R.H.; Avorn, J. The Hepatotoxicity of Antifungal Medications in Bone Marrow Transplant Recipients. Clin. Infect. Dis. 2005, 41, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Lamoth, F.; Lewis, R.E.; Kontoyiannis, D.P. Investigational Antifungal Agents for Invasive Mycoses: A Clinical Perspective. Clin. Infect. Dis. 2022, 75, 534–544. [Google Scholar] [CrossRef]
- de Moraes, D.C.; Tessis, A.C.; Rollin-Pinheiro, R.; Princival, J.L.; Villar, J.A.F.P.; Barbosa, L.A.; Barreto-Bergter, E.; Ferreira-Pereira, A. Digoxin Derivatives Sensitize a Saccharomyces Cerevisiae Mutant Strain to Fluconazole by Inhibiting Pdr5p. JoF 2022, 8, 769. [Google Scholar] [CrossRef]
- Hadrich, I.; Ayadi, A. Epidemiology of Antifungal Susceptibility: Review of Literature. J. Mycol. Méd. 2018, 28, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.E.; Cahyame-Zuniga, L.; Leventakos, K.; Chamilos, G.; Ben-Ami, R.; Tamboli, P.; Tarrand, J.; Bodey, G.P.; Luna, M.; Kontoyiannis, D.P. Epidemiology and Sites of Involvement of Invasive Fungal Infections in Patients with Haematological Malignancies: A 20-Year Autopsy Study. Mycoses 2013, 56, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Wee, L.E.; Tan, A.L.; Wijaya, L.; Chlebicki, M.P.; Thumboo, J.; Tan, B.H. Timeliness of Infectious Diseases Referral and Inappropriate Antibiotic Usage Post-Referral in an Asian Tertiary Hospital. Trop. Med. Infect. Dis. 2019, 4, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooda, K.; Canterbury, E.; Bellolio, F. Impact of Pharmacist-Led Antimicrobial Stewardship on Appropriate Antibiotic Prescribing in the Emergency Department: A Systematic Review and Meta-Analysis. Ann. Emerg. Med. 2022, 79, 374–387. [Google Scholar] [CrossRef] [PubMed]
- Parente, D.M.; Morton, J. Role of the Pharmacist in Antimicrobial Stewardship. Med. Clin. N. Am. 2018, 102, 929–936. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factor | Score | Risk Factor | Score |
|---|---|---|---|
| Miocardial infarction | 1 | Diabetes with end organ damage | 2 |
| Peripheral vascular disease | 1 | Moderate or severe renal disease | 2 |
| Cerebrovascular disease | 1 | Hemiplegia | 2 |
| Congestive heart failure | 1 | Any tumor without metastasis | 2 |
| Peptic ulcer disease | 1 | Leukemia | 2 |
| Diabetes | 1 | Lymphoma | 2 |
| Chronic pulmonary disease | 1 | Moderate or severe liver disease | 3 |
| Connective tissue disease | 1 | AIDS | 6 |
| Dementia | 1 | Metastatic solid tumor | 6 |
| Mild liver disease | 1 |
| System | Score | ||||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |
| Respiration PaO2/FiO2, mmHg | ≥400 | 301–399 | 201–300 | 101–200 | ≤100 |
| Coagulation Platelets, ×103 μL−1 | >150 | 101–150 | 51–100 | 21–50 | ≤20 |
| Liver Bilirubin, mg dL−1 | <1.2 | 1.2–1.9 | 2.0–5.9 | 6.0–11.9 | >12.0 |
| Cardiovascular Mean Arterial Pressure, mmHg | Hypotension absent | <70 | On dopamine ≤ 5 mcg/kg/min or any dobutamine | On dopamine > 5 mcg/kg/min, epinephrine ≤ 0.1 mcg/kg/min, or norepinephrine ≤ 0.1 mcg/kg/min | On dopamine > 15 mcg/kg/min, epinephrine > 0.1 mcg/kg/min, or norepinephrine > 0.1 mcg/kg/min |
| Central nervous system Glasgow coma scale | 15 | 13–14 | 10–12 | 6–9 | <6 |
| Renal Creatinine, mg dL−1 | <1.2 | 1.2–1.9 | 2.0–3.4 | 3.5–4.9 | >5 |
| Risk Factor | Score |
|---|---|
| Diabetes | 5 |
| Gastrointestinal surgery | 5 |
| Hematologic malignancies | 4 |
| Broad-spectrum antibiotic therapy ≥ 4 days | 4 |
| Central venous catheter (CVC) | 3 |
| Total parenteral nutrition | 3 |
| Mechanical ventilation ≥ 2 days | 2 |
| Assessment | Indication | Dosage | Antifungal–Drug Interaction |
|---|---|---|---|
| Appropriate | Follows recommended practices by the infectious diseases team, local procedures, and/or published guidelines. | Appropriate dose x or underdose or overdose by ≤10% to loading dose when recommended. Also, observing the recommended dose limit and dose adjustments for renal dysfunction. | Antifungal has no potential interaction with drugs used concomitantly. Antifungal presents potential interactions with moderate severity but is subjected to clinical monitoring and dose adjustment when required. |
| Debatable | It does not follow protocol, but there is evidence in the literature or no suitable alternative. | Underdose or overdose x by ≤25% or no loading dose or no discontinuation or dose adjustment in case of clinically related adverse events. | Antifungal presents potential interactions with moderate severity, and clinical monitoring or dose adjustment is not performed when required. |
| Inappropriate | Inappropriate antifungal selection concerning the protocol or mycological data, despite the existence of a suitable alternative. | Under or overdose x > 25%; no discontinuation or dose adjustment in case of a clinically related adverse event when an appropriate alternative is available. | Antifungal presents potential interactions with concomitant medications, including severe or contraindicated interactions; the antifungal is used with concomitant drug therapy and results in failure of the antifungal, or there is concomitant use of two antifungals of the same classification. |
| Characteristics | |
|---|---|
| Demographics | |
| Age (years), median (IQR) | 72 ± 19 |
| Male sex, n (%) | 25 (52.1) |
| Outcome | |
| Success | 37 (77.1) |
| Transfer to another facility | 3 (6.2) |
| Death | 8 (16.7) |
| Comorbidities | |
| Miocardial infarction, n (%) | 3 (6.2) |
| Peripheral vascular disease, n (%) | 0 (0.0) |
| Cerebrovascular disease, n (%) | 2 (4.2) |
| Congestive heart failure, n (%) | 5 (10.4) |
| Peptic ulcer disease, n (%) | 8 (16.7) |
| Diabetes, n (%) | 9 (18.8) |
| Chronic pulmonary disease, n (%) | 7 (14.6) |
| Connective tissue disease, n (%) | 0 (0.0) |
| Dementia, n (%) | 4 (8.3) |
| Mild liver disease, n (%) | 1 (2.1) |
| Diabetes with end organ damage | 4 (8.3) |
| Moderate or severe renal disease, n (%) | 8 (16.7) |
| Hemiplegia, n (%) | 0 (0.0) |
| Any tumor without metastasis, n (%) | 10 (20.8) |
| Leukemia, n (%) | 1 (2.1) |
| Lymphoma, n (%) | 3 (6.2) |
| Moderate or severe liver disease, n (%) | 3 (6.2) |
| AIDS, n (%) | 0 (0.0) |
| Metastatic solid tumor, n (%) | 1 (2.1) |
| Charlson comorbidity index | |
| Mild comorbidity, n (%) | 8 (16.7) |
| Moderate comorbidity, n (%) | 16 (33.3) |
| Severe comorbidity, n (%) | 24 (50.0) |
| Characteristics | |
|---|---|
| SOFA score | |
| 0–6 points/mortality <10%, n (%) | 36 (75.0) |
| 7–9 points/mortality 15–20%, n (%) | 4 (8.3) |
| 10–12 points/mortality 40–50%, n (%) | 6 (12.5) |
| 13–14 points/mortality 50–60%, n (%) | 1 (2.1) |
| 15–24 points/mortality ≥90%, n (%) | 1 (2.1) |
| Risk Factors for Invasive Fungal Infection | |
| Diabetes, n (%) | 9 (18.8) |
| Gastrointestinal surgery, n (%) | 12 (25.0) |
| Hematologic malignancies, n (%) | 2 (4.2) |
| Broad-spectrum antibiotic therapy ≥4 days, n (%) | 36 (75.0) |
| Central venous catheter (CVC), n (%) | 26 (54.2) |
| Total parenteral nutrition, n (%) | 13 (27.1) |
| Mechanical ventilation ≥2 days, n (%) | 10 (20.1) |
| Invasive Fungal Infection Risk | |
| Low risk, n (%) | 24 (50.0) |
| Moderate risk, n (%) | 13 (27.1) |
| High risk, n (%) | 11 (22.9) |
| Characteristics | |
|---|---|
| Patients with cultures for fungi, n (%) | 15 (31.2) |
| Total of cultures for fungi, n (%) | 23 (100) |
| Positive cultures for fungi, n (%) | 11 (47.8) |
| Positive cultures according to each fungal species found | |
| Candida albicans, n (%) | 7 (63.6) |
| Candida tropicalis, n (%) | 3 (27.3) |
| Candida glabrata, n (%) | 1 (9.1) |
| Saccharomyces cerevisiae, n (%) | 1 (9.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fallas-Mora, A.; Díaz-Madriz, J.P.; Chaverri-Fernández, J.M.; Zavaleta-Monestel, E. Evaluation of Systemic Antifungal Use in a Latin American General Care Hospital: A Retrospective Study. Pharmacy 2023, 11, 108. https://doi.org/10.3390/pharmacy11040108
Fallas-Mora A, Díaz-Madriz JP, Chaverri-Fernández JM, Zavaleta-Monestel E. Evaluation of Systemic Antifungal Use in a Latin American General Care Hospital: A Retrospective Study. Pharmacy. 2023; 11(4):108. https://doi.org/10.3390/pharmacy11040108
Chicago/Turabian StyleFallas-Mora, Abigail, Jose Pablo Díaz-Madriz, Jose Miguel Chaverri-Fernández, and Esteban Zavaleta-Monestel. 2023. "Evaluation of Systemic Antifungal Use in a Latin American General Care Hospital: A Retrospective Study" Pharmacy 11, no. 4: 108. https://doi.org/10.3390/pharmacy11040108