
A User-Friendly Nonmotorized Device for Ankle Rehabilitation
 ,
, 
Abstract
:1. Introduction
2. Brief Review of Ankle Kinesiology
3. Mathematical Model of the Novel Ankle Device
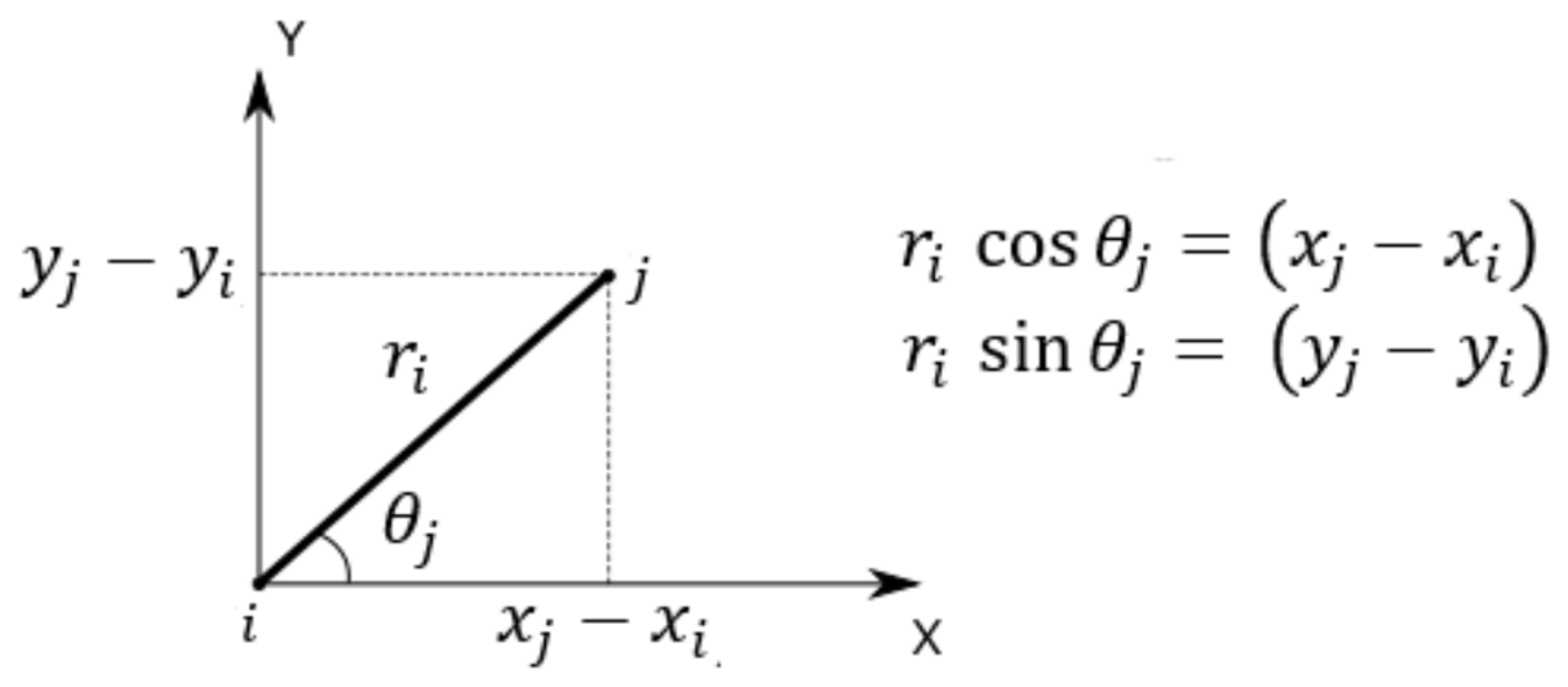
3.1. Kinematic Model
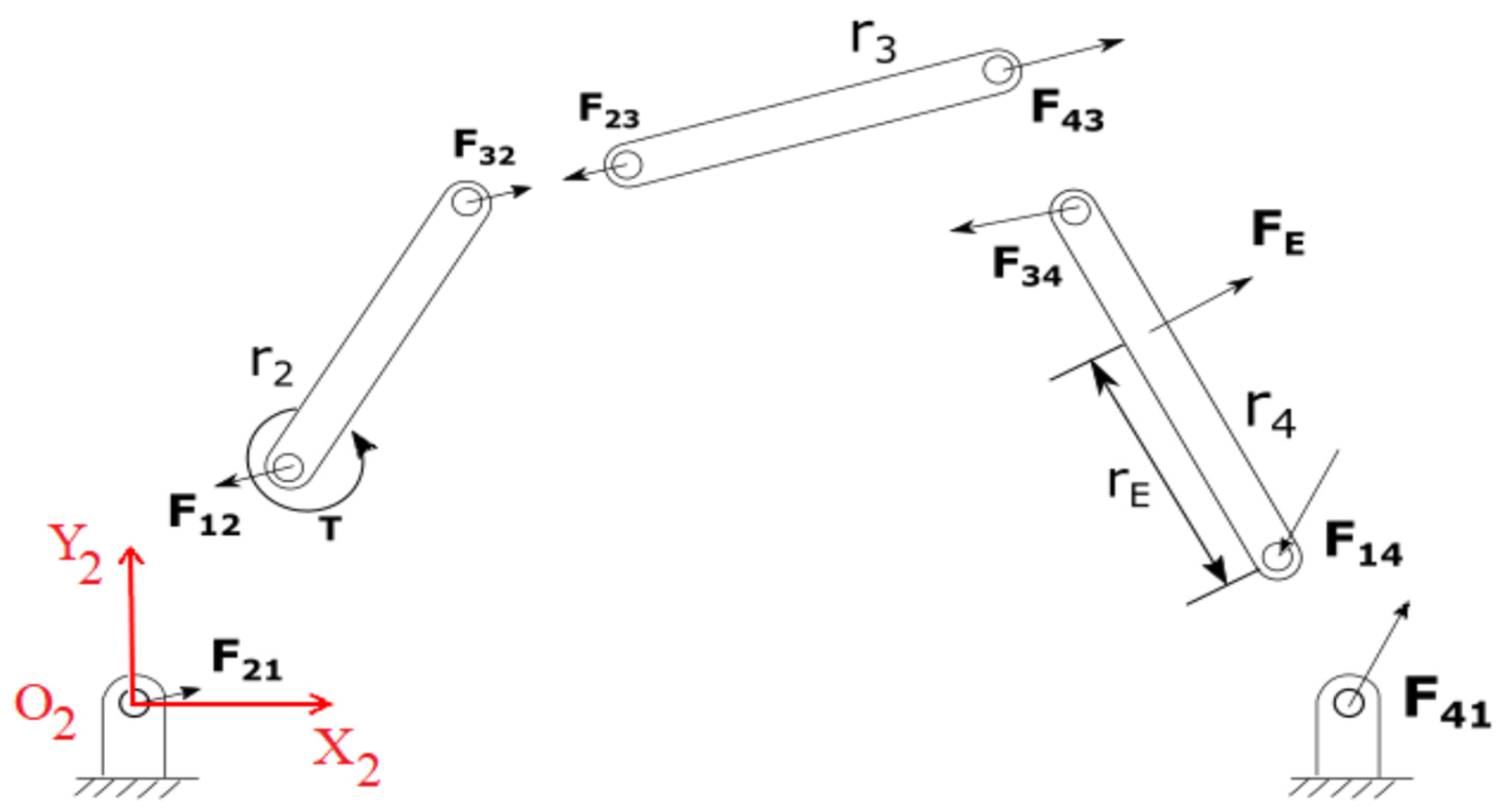
3.2. Static Model
3.3. Singularity Analysis
4. Evolutional Algorithm and Mathematical Results
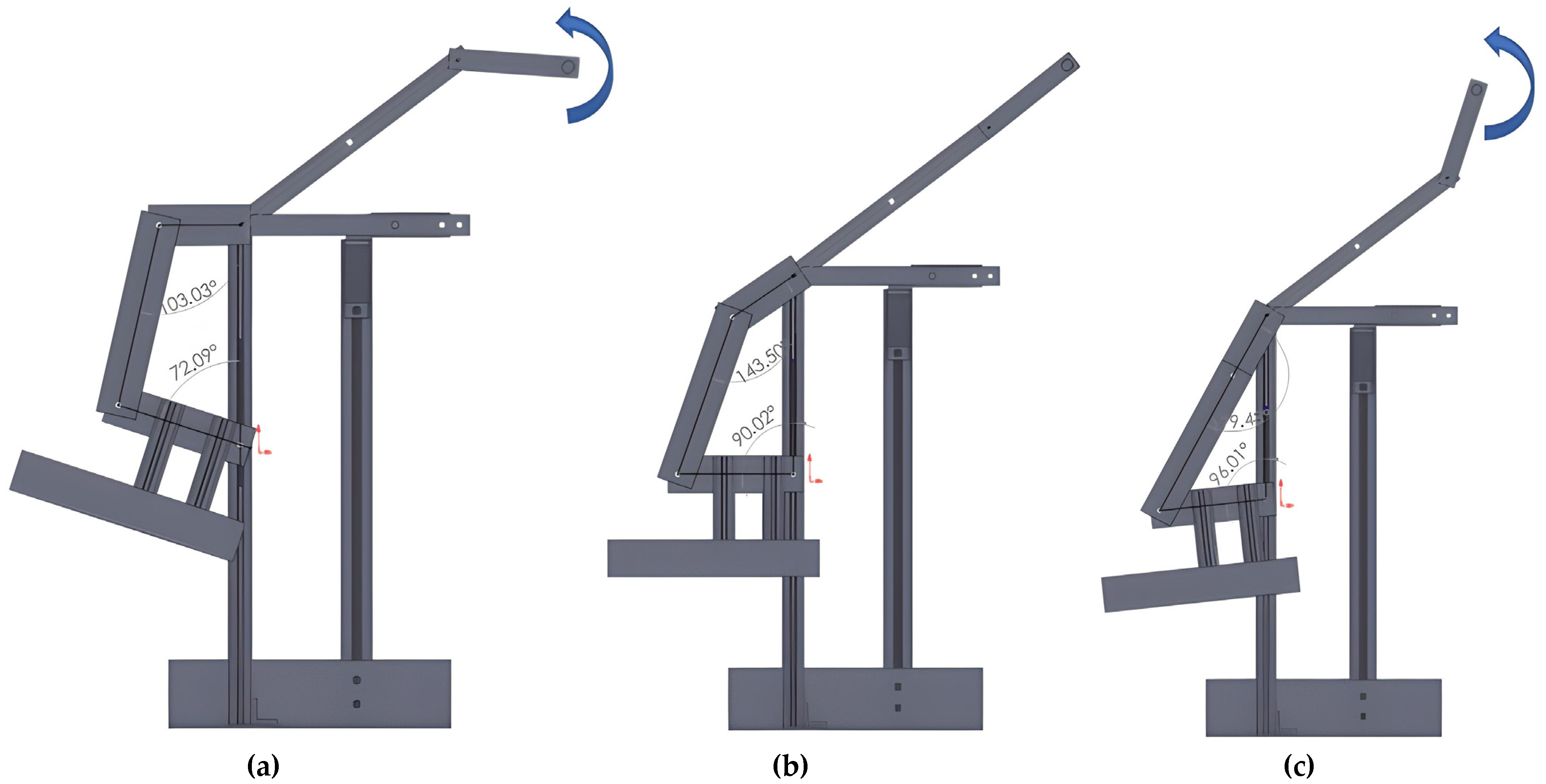
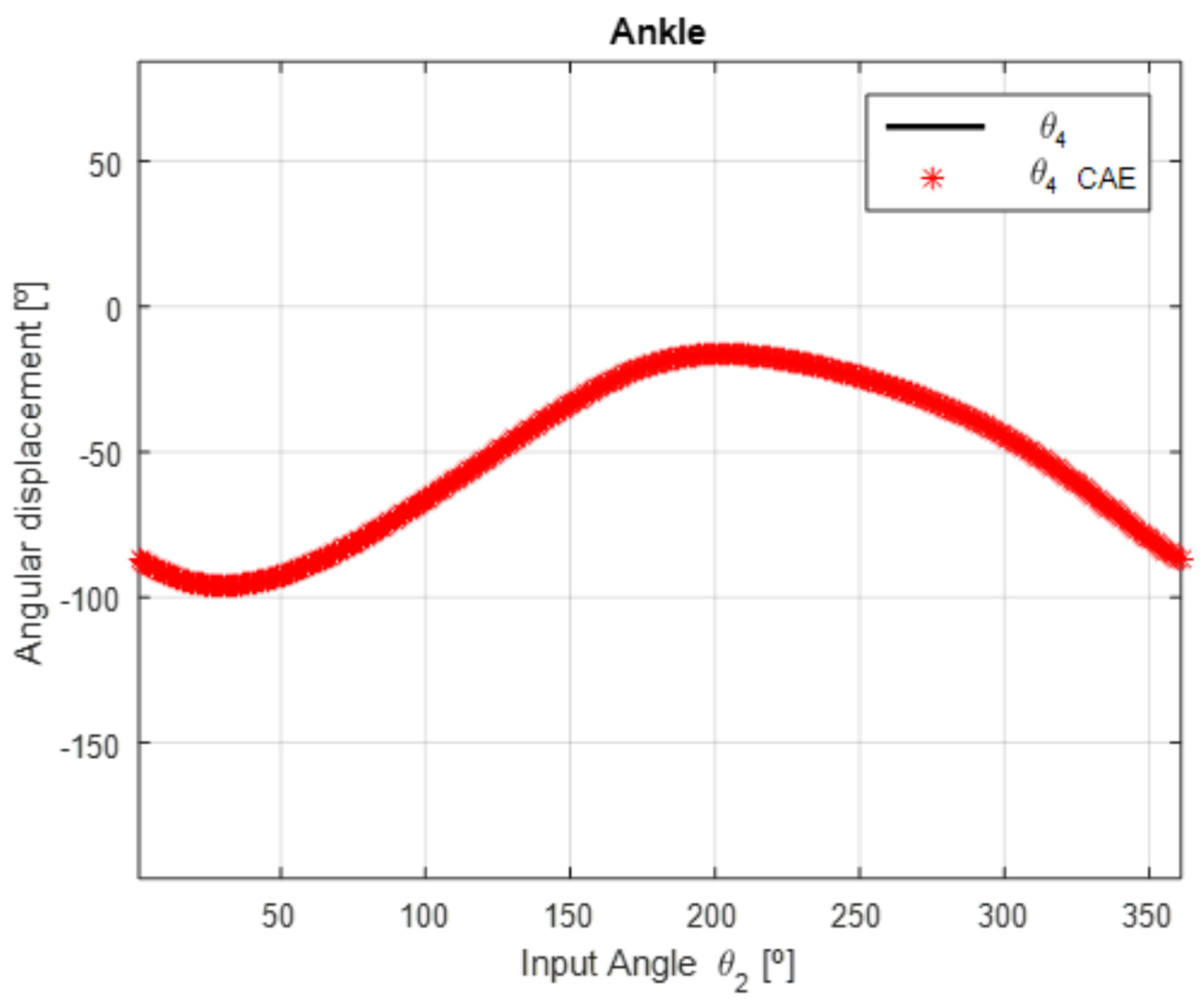
5. CAD/CAE Simulations and Results
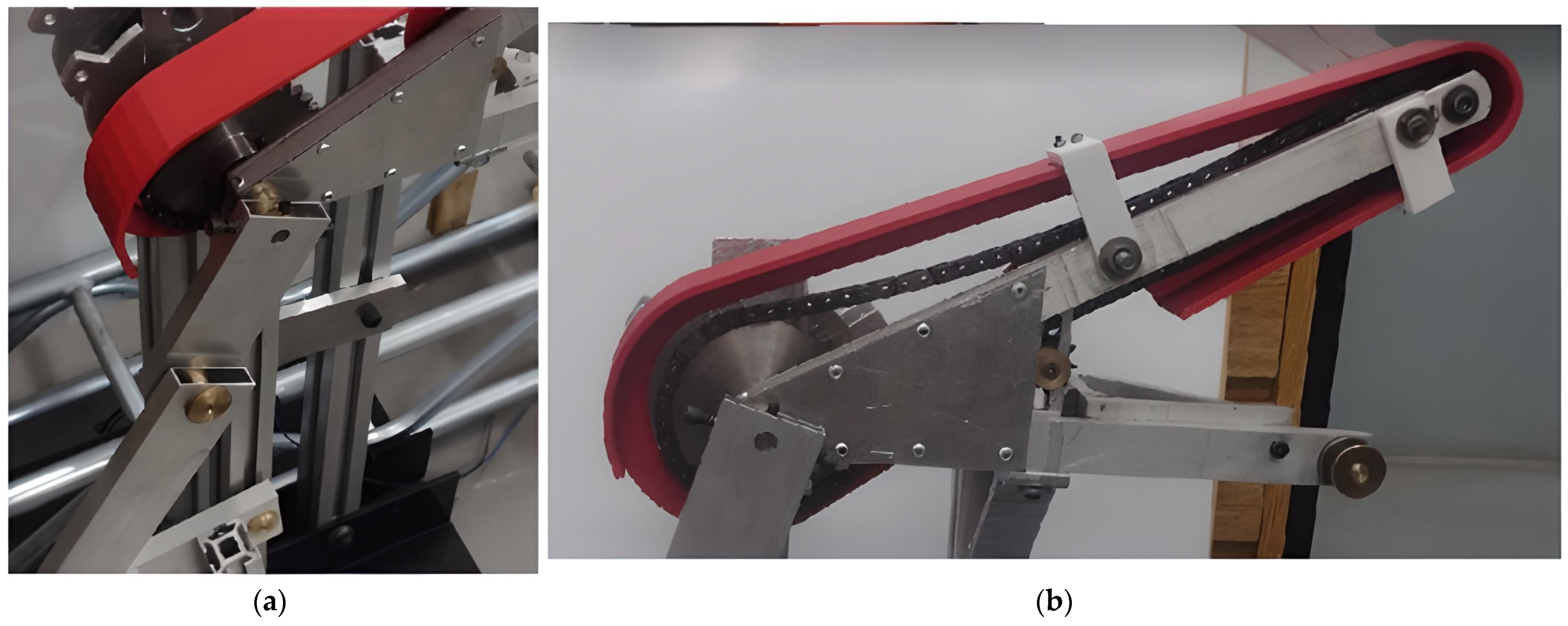
6. Ankle Device Prototype
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mattacola, C.G.; Dwyer, M.K. Rehabilitation of the Ankle After Acute Sprain or Chronic Instability. J. Athl. Train. 2002, 37, 413–429. [Google Scholar] [PubMed]
- Martin, R.L.; Stewart, G.W.; Conti, S.F. Posttraumatic Ankle Arthritis: An Update on Conservative and Surgical Management. J. Orthop. Sport. Phys. Ther. 2007, 37, 253–259. [Google Scholar] [CrossRef]
- Gaddi, D.; Mosca, A.; Piatti, M.; Munegato, D.; Catalano, M.; Di Lorenzo, G.; Turati, M.; Zanchi, N.; Piscitelli, D.; Chui, K.; et al. Acute Ankle Sprain Management: An Umbrella Review of Systematic Reviews. Front. Med. 2022, 9, 868474. [Google Scholar] [CrossRef]
- Dong, M.; Zhou, Y.; Li, J.; Rong, X.; Fan, W.; Zhou, X.; Kong, Y. State of the art in parallel ankle rehabilitation robot: A systematic review. J. NeuroEng. Rehabil. 2021, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, R.S.; Rodrigues, L.A.O.; Humbert, R.; Carbone, G. Development of a Nonmotorized Mechanism for Ankle Rehabilitation. Eng. Proc. 2022, 24, 19. [Google Scholar] [CrossRef]
- Alves, T.; Gonçalves, R.S.; Carbone, G. Serious Games Strategies with Cable-Driven Robots for Bimanual Rehabilitation: A Randomized Controlled Trial with PostStroke Patients. Front. Robot. AI 2022, 9, 739088. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Soares, G.; Carvalho, J.C. Conceptual design of a rehabilitation device based on cam-follower and crank-rocker mechanisms hand actioned. J. Braz. Soc. Mech. Sci. Eng. 2019, 41, 277. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Krebs, H.I. MIT-Skywalker: Considerations on the Design of a Body Weight Support System. J. Neuroeng. Rehabil. 2017, 14, 88. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, R.S.; Rodrigues, L.A.O. Development of nonmotorized mechanisms for lower limb rehabilitation. Robotica 2021, 40, 102–119. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Carvalho, J.C.M. Robot Modeling for Physical Rehabilitation. In Service Robots and Robotics: Design and Application; IGI Global: Hershey, PA, USA, 2012; pp. 154–175. [Google Scholar] [CrossRef] [Green Version]
- Gherman, B.; Birlescu, I.; Plitea, N.; Carbone, G.; Tarnita, D.; Pisla, D. On the singularity-free workspace of a parallel robot for lower-limb rehabilitation. Proceedings of the Romanian Academy Series A–Mathematics Physics Technical Sciences. Inf. Sci. 2019, 20, 383–391. [Google Scholar]
- Alves, T.; Gonçalves, R.S.; Carbone, G. Serious Games Strategies with Cable-Driven Robots for Rehabilitation Tasks. In New Trends in Medical and Service Robotics; Rauter, G., Carbone, G., Cattin, P.C., Zam, A., Pisla, D., Riener, R., Eds.; Springer: New York, NY, USA, 2022; Volume 106. [Google Scholar] [CrossRef]
- Pisla, D.; Nadas, I.; Tucan, P.; Albert, S.; Carbone, G.; Antal, T.; Banica, A.; Gherman, B. Development of a Control System and Functional Validation of a Parallel Robot for Lower Limb Rehabilitation. Actuators 2021, 10, 277. [Google Scholar] [CrossRef]
- Tucan, P.; Ulinici, I.; Pop, N.; Puskas, F.; Carbone, G.; Gherman, B.; Luchian, I.; Pisla, D. Ankle Rehabilitation of Stroke Survivors Using Kuka LBR Iiwa. In New Trends in Medical and Service Robotics; Rauter, G., Cattin, P.C., Zam, A., Riener, R., Carbone, G., Pisla, D., Eds.; Springer: New York, NY, USA, 2021; Volume 93. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Brito, L.S.F.; Moraes, L.P.; Carbone, G.; Ceccarelli, M. A fairly simple mechatronic device for training human wrist motion. Int. J. Adv. Robot. Syst. 2020, 17, 1729881420974286. [Google Scholar] [CrossRef]
- Carbone, G.; Gonçalves, R.S. Editorial: Robot-assisted rehabilitation for neurological disorders. Front. Robot. AI 2022, 9, 1014681. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.; Garnier, M.; Barbas, J.; Chang, S.H.; Charlifue, S.; Field-Fote, E.; Furbish, C.; Tefertiller, C.; Mummidisetty, C.K.; Taylor, H.; et al. Budget impact analysis of robotic exoskeleton use for locomotor training following spinal cord injury in four SCI Model Systems. J. Neuro. Eng. Rehabil. 2020, 17, 4. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Tyson, S.; Weightman, A. Professionals’ Views and Experiences of Using Rehabilitation Robotics with Stroke Survivors: A Mixed Methods Survey. Front. Med. Technol. 2021, 3, 780090. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Qiu, J.; Fong, D.T. The applications of wearable devices in the rehabilitation of ankle injuries: A systematic review and meta-analysis. Med. Nov. Technol. Devices 2023, 17, 100210. [Google Scholar] [CrossRef]
- Zhetenbayev, N.; Zhauyt, A.; Balbayev, G.; Shingissov, B. Robot device for ankle joint rehabilitation: A review. Vibroengineering PROCEDIA 2022, 41, 96–102. [Google Scholar] [CrossRef]
- Wang, T.; Zhang, B.; Liu, C.; Liu, T.; Han, Y.; Wang, S.; Ferreira, J.P.; Dong, W.; Zhang, X. A Review on the Rehabilitation Exoskeletons for the Lower Limbs of the Elderly and the Disabled. Electronics 2022, 11, 388. [Google Scholar] [CrossRef]
- Shi, B.; Chen, X.; Yue, Z.; Yin, S.; Weng, Q.; Zhang, X.; Wang, J.; Wen, W. Wearable Ankle Robots in Post-stroke Rehabilitation of Gait: A Systematic Review. Front. Neurorobot. 2019, 13, 63. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.J.; Ferris, D. Neural coupling between upper and lower limbs during recumbent stepping. J. Appl. Physiol. 2004, 97, 1299–1308. [Google Scholar] [CrossRef]
- Klarner, T.; Barss, T.S.; Sun, Y.; Kaupp, C.; Loadman, P.M.; Zehr, E.P. Exploiting Interlimb Arm and Leg Connections for Walking Rehabilitation: A Training Intervention in Stroke. Neural Plast. 2016, 2016, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapandji, I. Physiology of the Joints: Lower Limb, 6th ed.; Churchill Livingstone: London, UK, 2010. [Google Scholar]
- Brockett, C.L.; Chapman, G.J. Biomechanics of the ankle. Orthop. Trauma 2016, 30, 232–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uicker, J.J.; Pennock, G.R.; Shigley, J.E.; McCarthy, J.M. Theory of machines and mechanisms. J. Mech. Des. 2003, 125, 650. [Google Scholar] [CrossRef] [Green Version]
- Altuzarra, O.; Pinto, C.; Avilés, R.; Hernández, A. A practical procedure to analyze singular configurations in closed kinematic chains. IEEE Trans. Robot. 2004, 20, 929–940. [Google Scholar] [CrossRef]
- Altuzarra, O.; Salgado, O.; Petuya, V.; Hernández, A. Point-based Jacobian formulation for computational kinematics of manipulators. Mech. Mach. Theory 2006, 41, 1407–1423. [Google Scholar] [CrossRef]
- Vaida, C.; Birlescu, I.; Pisla, A.; Ulinici, I.; Tarnita, D.; Carbone, G.; Pisla, D. Systematic design of a parallel robotic system for lower limb rehabilitation. IEEE Access 2020, 8, 34522–34537. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Carvalho, J.C.M.; Lobato, F.S. Design of a robotic device actuated by cables for human lower limb rehabilitation using self-adaptive differential evolution and robust optimization. Biosci. J. 2016, 32, 1689–1702. [Google Scholar] [CrossRef]
- Davis, J.R. Properties and Selection: Nonferrous Alloys and Special-Purpose Materials. In ASM Handbook; ASM International: Almere, The Netherlands, 2007; Volume 2. [Google Scholar] [CrossRef]
- Neumann, D. Kinesiology of The Musculoskeletal System; Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Freire, B.; Dias, C.P.; Oliveira, L.S.; Goulart, N.B.A.; Lemos, F.A.; Becker, J.; Gomes, I.; Vaz, M.A. Rate of force development and torque production assessment in spastic stroke survivors. Rev. Bras. Cineantropom. Desempenho Hum. 2015, 17, 328–336. [Google Scholar] [CrossRef] [Green Version]
- McCrea, P.H.; Eng, J.J.; Hodgson, A.J. Time and magnitude of torque generation is impaired in both arms following stroke. Muscle Nerve 2003, 28, 46–53. [Google Scholar] [CrossRef]
- Cho, K.H.; Jeon, Y.; Lee, H. Range of Motion of the Ankle According to Pushing Force, Gender and Knee Position. Ann Rehabil. Med. 2016, 40, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Andrade, R.J.; Lacourpaille, S.R.; Freitas, S.R.; McNair, P.J.; Nordez, A. Effects of hip and head position on ankle range of motion, ankle passive torque, and passive gastrocnemius tension. Scand. J. Med. Sci. Sport. 2016, 26, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Laribi, M.A.; Carbone, G.; Zeghloul, S. On the Optimal Design of Cable Driven Parallel Robot with a Prescribed Workspace for Upper Limb Rehabilitation Tasks. J. Bionic. Eng. 2019, 16, 503–513. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Transversal Section (Width/Height/Thickness) | ||||
|---|---|---|---|---|
| 0.42 | 0.45 | 0.49 | 9.52 | 1/2″ × 1″ × 2 mm |
| Measure | Max. Flexion [°] | Max. Extension [°] | Difference [°] |
|---|---|---|---|
| 1 | 173.49 | 86.96 | 86.53 |
| 2 | 171.11 | 87.44 | 83.67 |
| 3 | 173.97 | 88.39 | 85.58 |
| 4 | 172.54 | 87.20 | 85.34 |
| 5 | 174.68 | 86.96 | 87.72 |
| 6 | 172.54 | 86.96 | 85.58 |
| 7 | 173.97 | 88.15 | 85.82 |
| 8 | 173.73 | 87.20 | 86.53 |
| 9 | 173.73 | 87.43 | 86.30 |
| 10 | 171.82 | 87.67 | 84.15 |
| 11 | 173.73 | 89.58 | 84.15 |
| 12 | 168.72 | 88.15 | 80.57 |
| 13 | 171.58 | 89.58 | 82.00 |
| 14 | 172.06 | 90.05 | 82.01 |
| 15 | 169.92 | 88.39 | 81.53 |
| 16 | 173.73 | 89.82 | 83.91 |
| 17 | 169.92 | 89.34 | 80.58 |
| 18 | 169.68 | 89.58 | 80.10 |
| Mean = 84.00° std = 2.36° | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonçalves, R.S.; Rodrigues, L.A.O.; Humbert, R.; Carbone, G. A User-Friendly Nonmotorized Device for Ankle Rehabilitation. Robotics 2023, 12, 32. https://doi.org/10.3390/robotics12020032
Gonçalves RS, Rodrigues LAO, Humbert R, Carbone G. A User-Friendly Nonmotorized Device for Ankle Rehabilitation. Robotics. 2023; 12(2):32. https://doi.org/10.3390/robotics12020032
Chicago/Turabian StyleGonçalves, Rogério Sales, Lucas Antônio Oliveira Rodrigues, René Humbert, and Giuseppe Carbone. 2023. "A User-Friendly Nonmotorized Device for Ankle Rehabilitation" Robotics 12, no. 2: 32. https://doi.org/10.3390/robotics12020032