Service Robots in the Healthcare Sector

 ,
, 
Abstract
:1. Introduction
2. Service Robotics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Application | Ref. | Year of Dev. | Make | Robot Name | Service Area | Success Rate | Specifications |
|---|---|---|---|---|---|---|---|
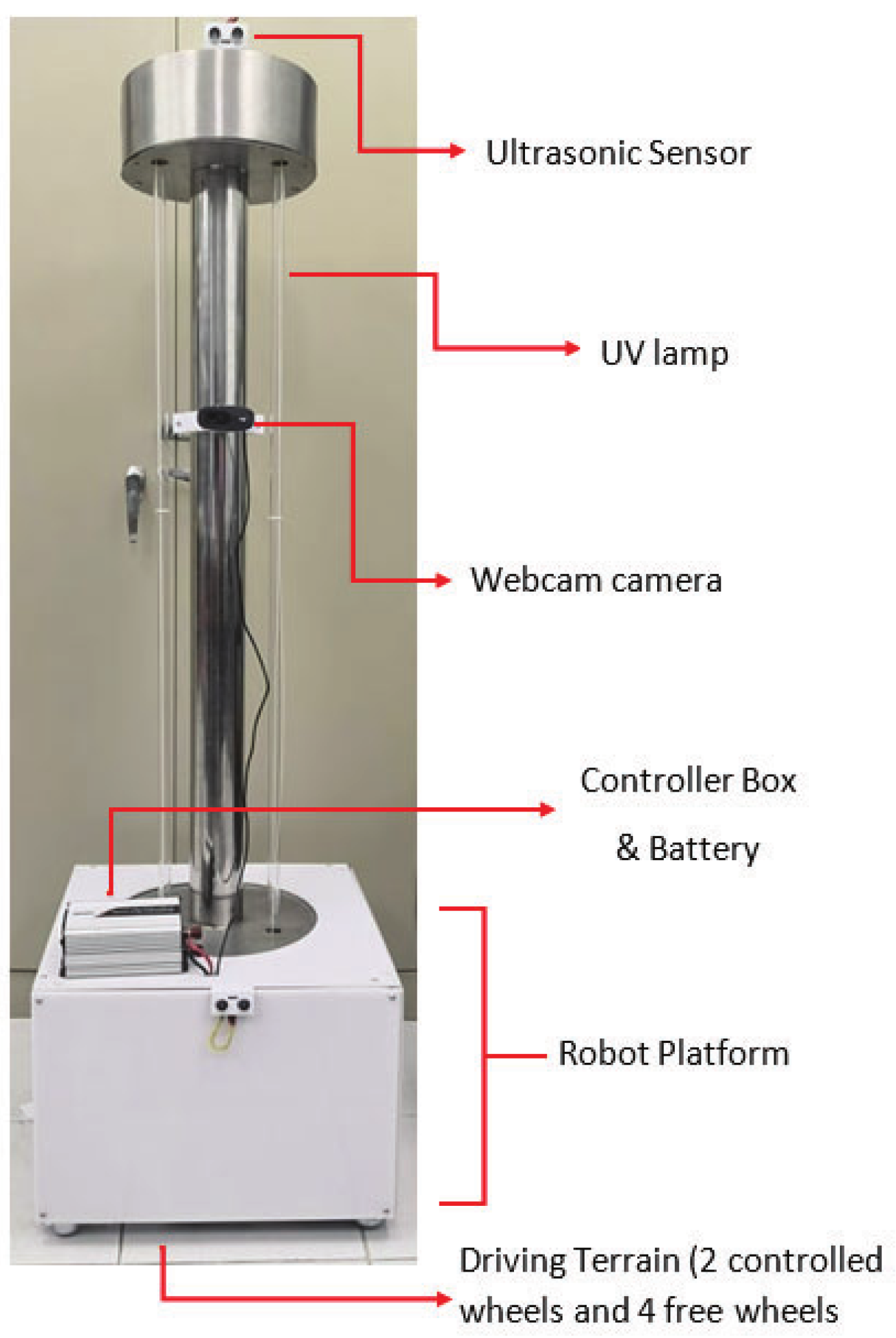
| UVC Sterilisation | [13] | 2019 | Academic/Research based | UV Sterilisation Robot | UV sterilisation for operating rooms | 100% of pathogens after 8 s of exposure (wavelength of 200–280 nm). | 60 × 60 × 142.5 (cm). Three UVC lamps and six ultrasonic sensors. |
| [14] | 2020 | UVD Robotics | Autonomous UV Disinfection Robot | UV sterilisation for hospitals | 99.99% after 10 min of exposure (wavelength of 254 nm). | 93 × 66 × 171 (cm). Mobile base, multiple LiDAR sensors, camera, array of UV lamps | |
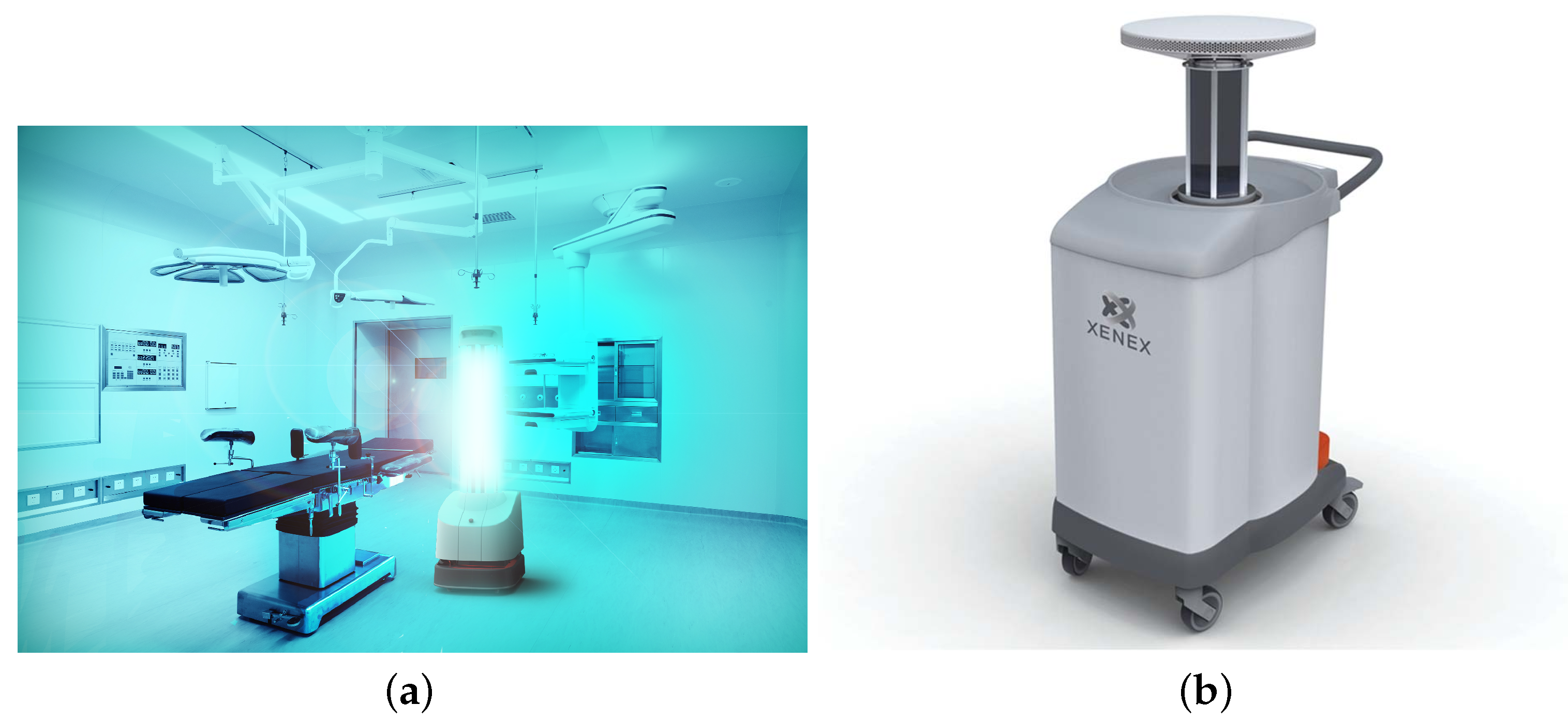
| [15] | 2020 | XENEX | LightStriker | Pulsed UV sterilisation for hospitals | 99.99% after a 2 min cycle (wavelength of 200–325 nm). | 30 × 20 × 38 inches. Data logger, reflector, UV lamps and UV pass filter | |
| [16] | 2020 | OMRON | LD-UVC | UV sterilisation for high contact points | 99.90% (wavelength of 200–280 nm). | 64 × 64 × 72.6 in cm. Eight UV lamps, aluminium reflector, LiDAR sensors, motion sensors | |
| [17] | 2020 | Geek+ | Lavender | UV disinfection for working environment | 99.99% of pathogens (wavelength of 253.5 nm). | 74 × 50 × 180 (cm). Six UV lamps, 3D vision, radar and human sensing | |
| Hydrogen Peroxide Disinfection | [18] | 2006 | Academic/Research based | Hydrogen Peroxide Disinfection robot | dry aerosol of hydrogen peroxide for surgery rooms, ambulances, and medical equipment | 87% in test rooms, 100% in operating department, 62.3% in medical equipment and 100% in ambulance. | Programmable, mobile, pre-set cycles, produces hydrogen peroxide as electrically charged particles. |
| [19] | 2016 | Bioquell | Bioquell BQ-50 | Hydrogen peroxide vapour generator used hospital-wide | deactivated 100% of biological indicators. | Vaporiser Model: 45 × 56 × 46 (cm). Aeration unit: 48 × 33 × 34 (cm). Vaporiser, tracking and reporting, airflow management, and mobile. |
| Application | Ref. | Year of Dev. | Make | Robot Name | Service Area | Success Rate | Specifications |
|---|---|---|---|---|---|---|---|
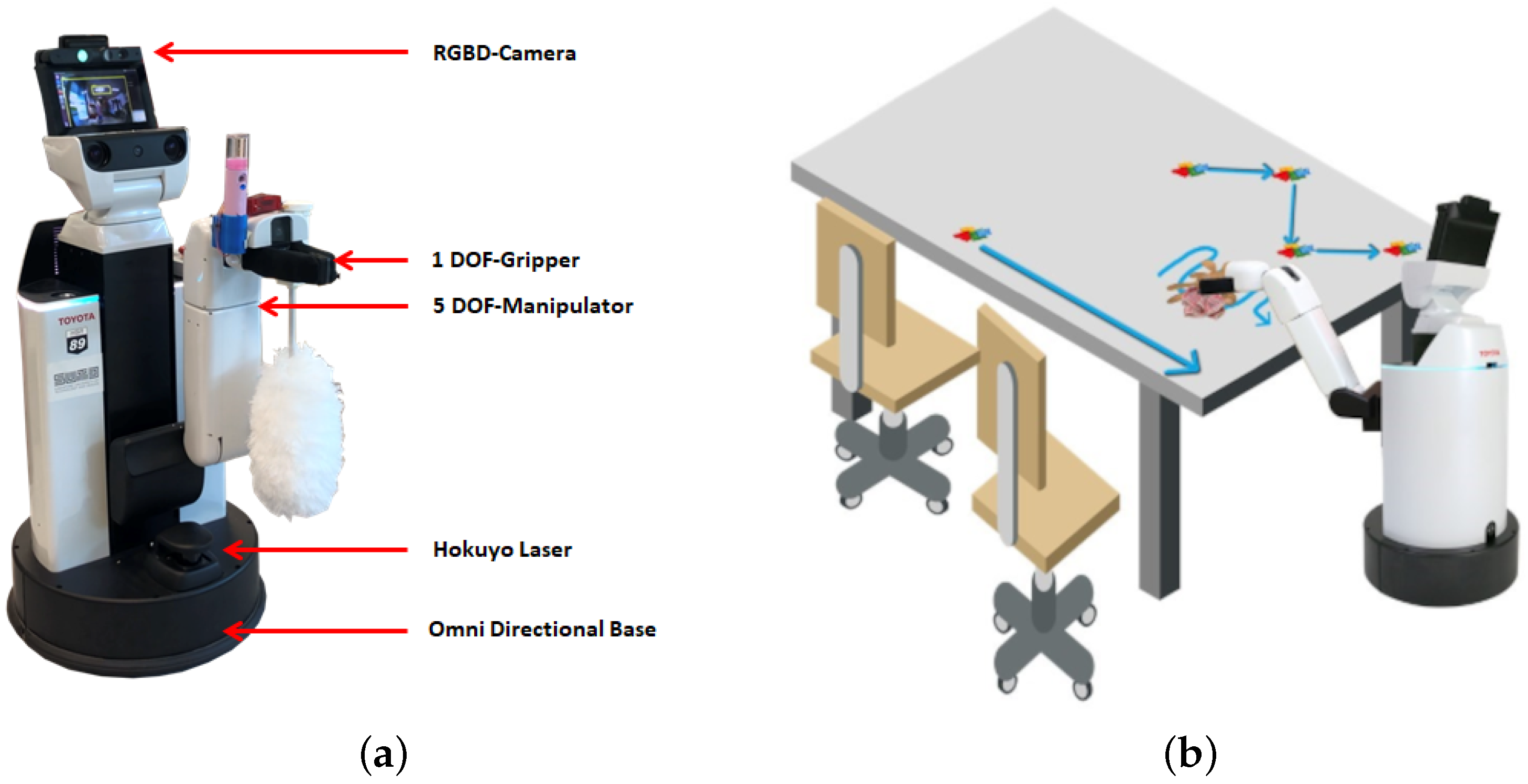
| Disinfecting High Contact Points | [20] | 2020 | Academic/Research based | Human Support Robot | Cleaning and maintenance of door handles | 95% accuracy of image detection in 11 s and in real-time 88–92%. | 43 × 43 × 100 (cm). RGBD camera, arm manipulator, base with LiDAR, pneumatic bumpers. |
| [21] | 2020 | Academic/Research based | Human Support Robot | Clean and inspect tables | 96–97% accuracy of image detection (litter, stains and spills). | 43 × 43 × 100 (cm). RGBD camera, arm manipulator, base with LiDAR, pneumatic bumpers. | |
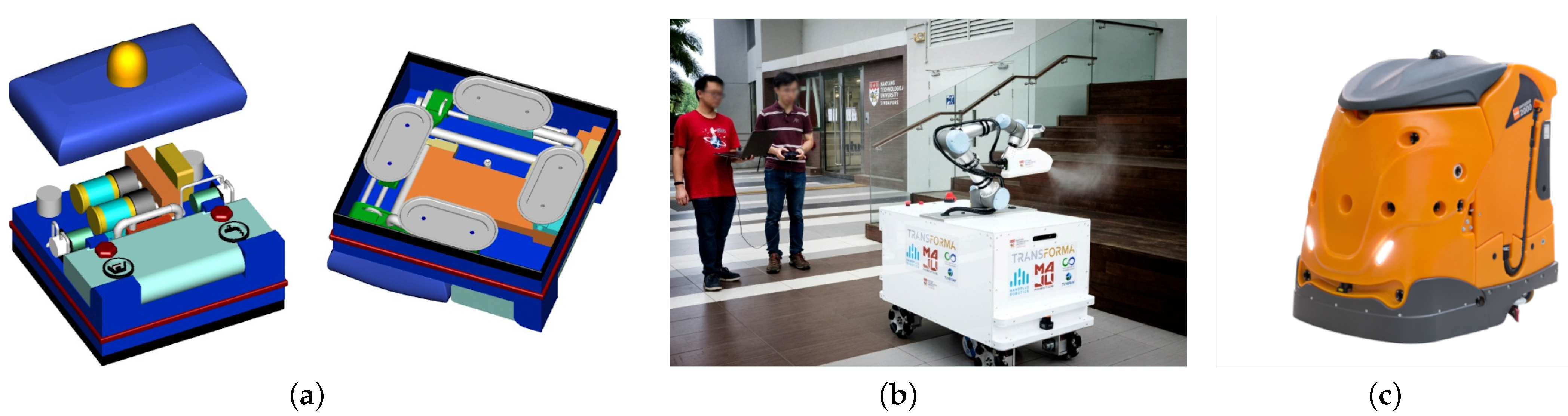
| Sanitising Floor and Wall Surfaces | [22] | 2014 | Academic/Research based | GECKOH13 | Wall and Ceiling cleaning | N/A—Preliminary testing | Four rigid vacuum cups with automatic suspensions, DC motors, pump for drain liquid, resistance boiler and nozzle for spraying disinfectant |
| [23] | 2018 | Diversey | Swingobot 2000 | Scrubber, drier, and floor cleaning | Hygiene standards are compliant with regulations from authorities (WHO and CD). | 135 × 90 × 128.5 (cm). Password protected, scanning laser, ultrasonic sonars, and angular rate sensor. | |
| [24] | 2020 | Academic/Research based | XDBot | disinfection of large surface areas | Disinfects a 20 sqm room within 6 min. No information available on success rate. | Electrostatic-charged nozzle, LiDAR, 3D camera | |
| [25] | 2020 | Geek+ | Jasmin | Spray disinfection in warehouses, offices, schools and hospitals | 99.99% (using hydrogen peroxide, peracetic acid or chlorine). | 74 × 50 × 160 (cm). Vision sensors, 3D radar, human sensing. | |
| [26] | 2020 | Fetch robotics and Build with Robots | BreezyOne | autonomous disinfection for large scale facilities | 99.9999% of pathogens in 100,000 square feet in 1.5 h. | Specification sheets unavailable at this time. |
| Application | Ref. | Year of Dev. | Make | Robot Name | Service Area | Success Rate | Specifications |
|---|---|---|---|---|---|---|---|
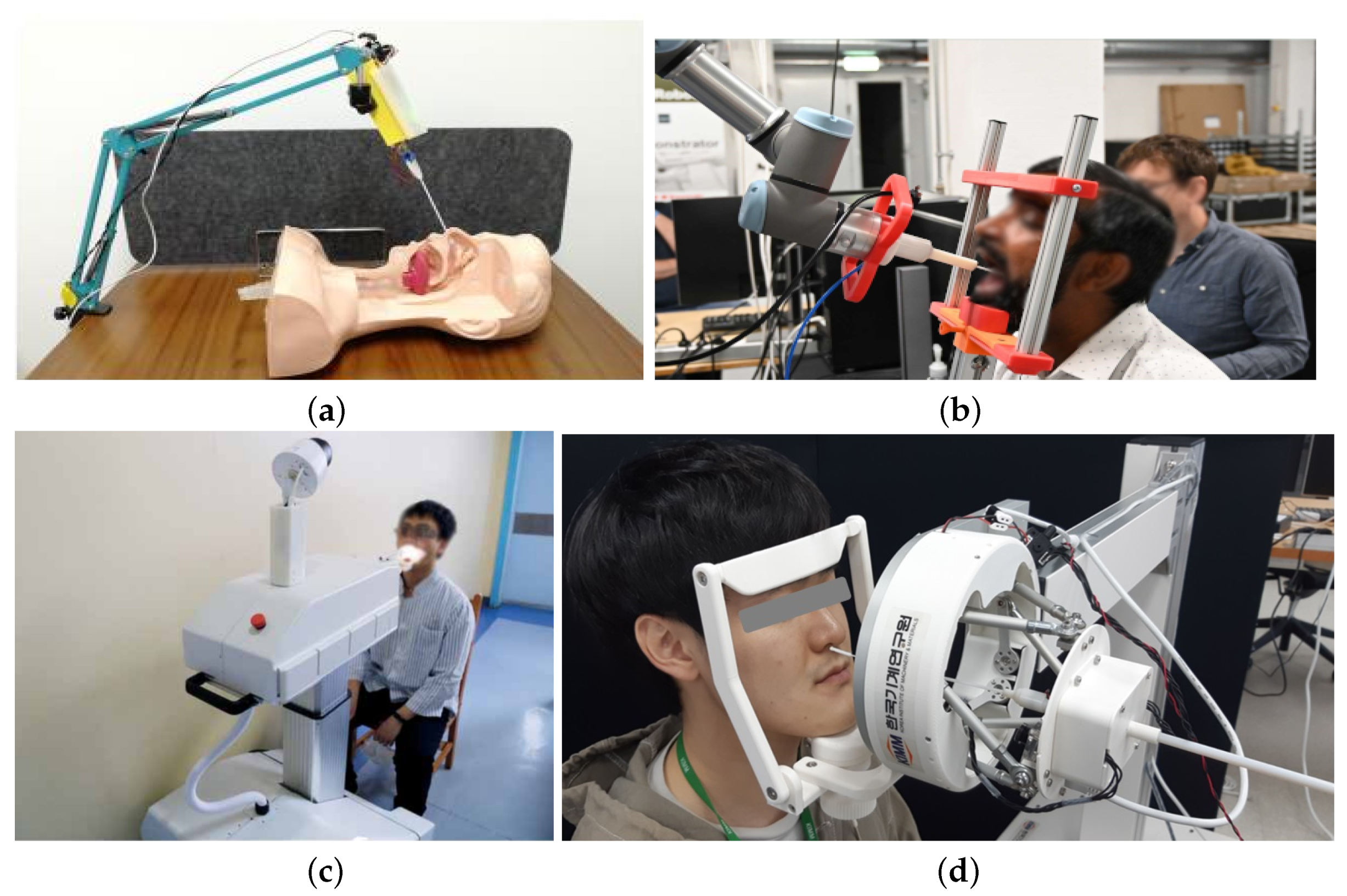
| COVID-19 Testing | [27] | 2020 | Academic/Research based | Nasopharyngeal Sampling Robot | Upper throat swabbing | N/A—Preliminary testing. | 15 × 6 × 4 (cm). Swab gripper, 2 DOF end-effector for actuating swab, and a 6 DOF passive arm for positioning. |
| [28] | 2020 | Lifeline Robotics | Commercial Throat Swabbing Robot | Middle throat swabbing | Gentle and consistent. Swabbing takes 25 s. | UR3 manipulator arm, 3D-printed end-effector, headrest. | |
| [29] | 2020 | Academic/Research based | Semi-automatic Oropharyngeal Swab Robot | Middle throat swabbing | No congestion or injury. If sampling force >40 g, evidence of sore throat. | Binocular endoscope serpentine robot arm manipulator, wireless transmission, and human–robot interaction terminal. | |
| [30] | 2020 | Academic/Research based | Telerobotic system swab robot | Upper respiratory swabbing | N/A—Preliminary testing. | Two wide-angle cameras, two microphone, force sensor, wireless transmission, parallel kinematic manipulator, end-effector and Stewart platform. |
| Application | Ref. | Make | Year of Dev. | Robot Name | Service Area | Specifications |
|---|---|---|---|---|---|---|
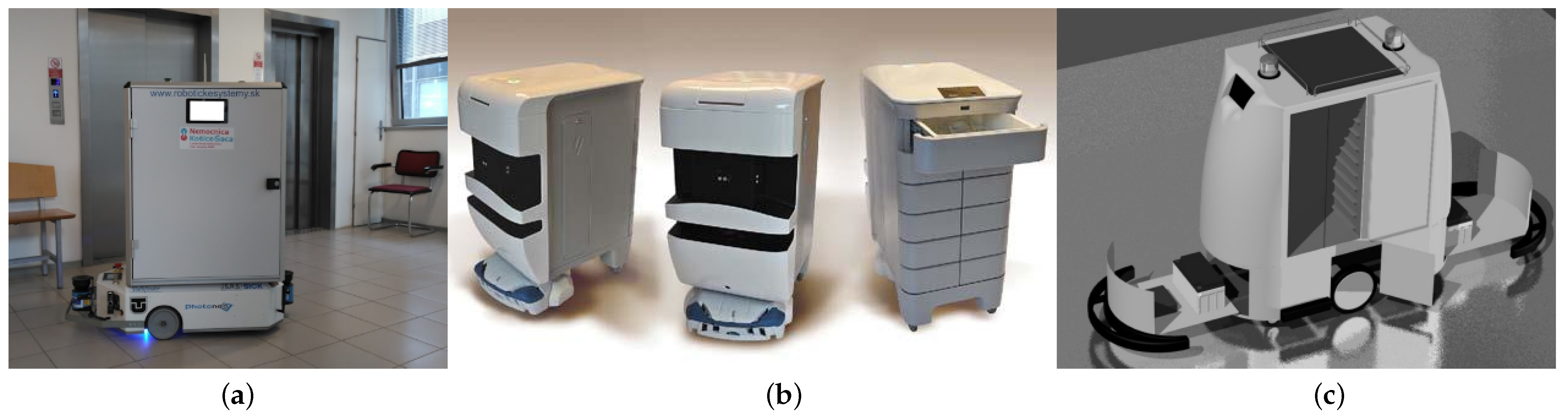
| Delivery | [31] | Helpmate | 1994 | Academic/Research based | Delivery pharmacy supplies and patient records between departments and nursing stations. | Ultrasonic range senors, light sensor, contact bumpers, and dead reckoning navigation. |
| [32] | Pathfinder | 2007 | Academic/Research based | Transport medical supplies between warehouses and clinics around the hospital. | 125 × 27 × 60 (cm). Two LiDars for localisation and mapping (can travel 10 km in 8 h), touch panel interface, Two wide angle cameras, and remote maintenance module. | |
| [33] | TUG | 2004 | Aethon | Transportation of medical supplies, medications, blood, food, linen and waste. | Maximum towing capacity of 1000 lbs, laser, sonar and infrared sensors for navigation, and 10 h battery time. | |
| [34] | HOSPI | 2004 | Panasonic | Delivery of medical supplies in the hospital. | 63 × 72.5 × 138 (cm). 9 h battery life, maximum load of 20 kg, 6 medication trays, pre-programmed hospital map data, obstacle avoidance, camera, security protected. Can moved up to 1 m/s. | |
| [35] | i-MERC | 2006 | Academic/Research based | Meal transportation service in hospitals and healthcare centres. Delivers food to patients and returns dishes to the washroom. | Ultrasonic and optical sensors, LEDs, touch screen and wifi connection for communication, heating system, 10 food trays, and a contact bumper. | |
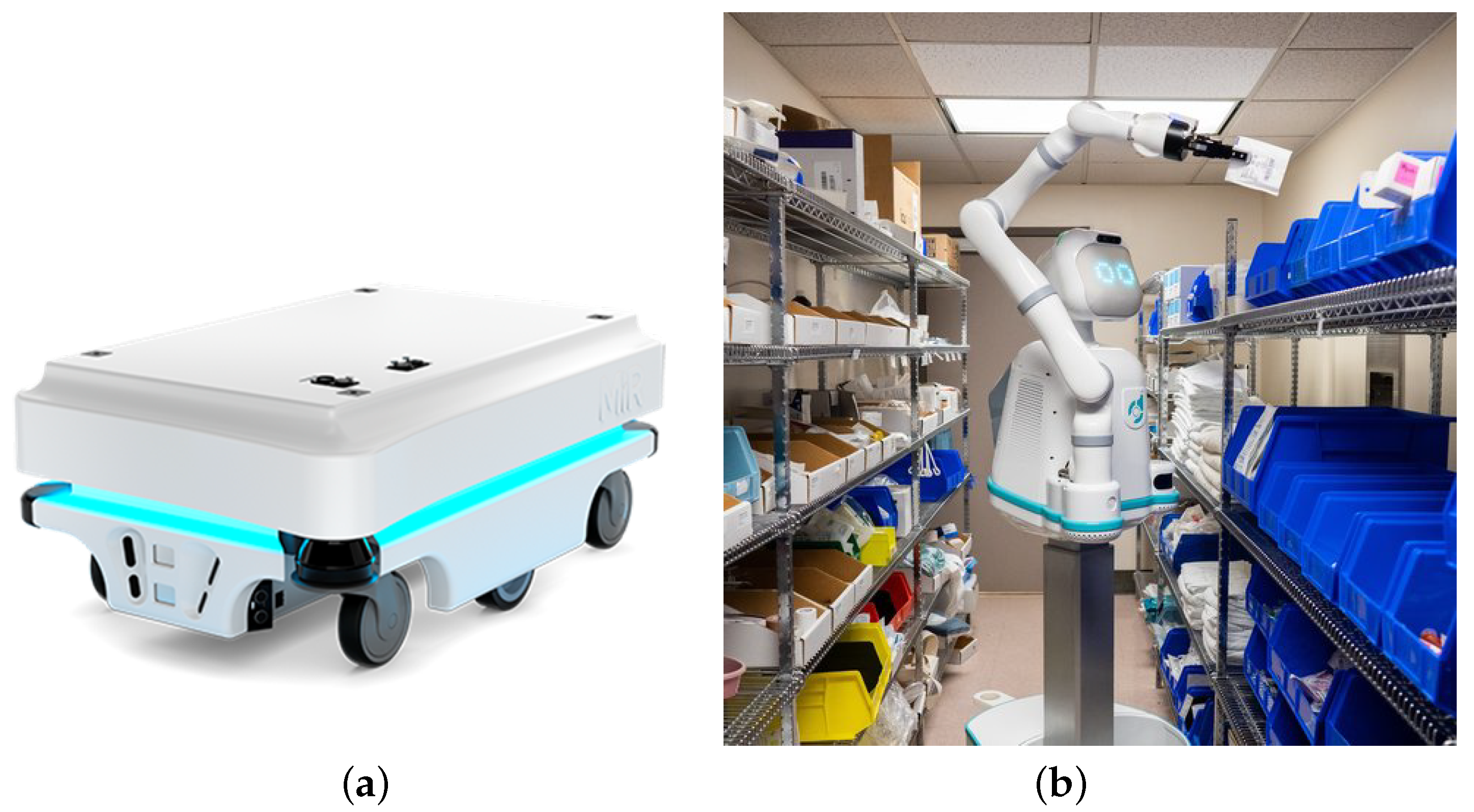
| [36] | Poli | 2016 | Diligent Robotics | Fetches suppliers and materials for nurses. | Arm manipulator and gripper—full specification sheet not available. | |
| [37] | Moxi | 2018 | Diligent Robotics | Gathers patient supplies and lab samples, distributes PPE, delivers medications. | Arm manipulator, gripper and freight mobile base—full specification sheet not available. | |
| [38] | MiR100 | 2013 | Mobile Industrial Robots | Delivery of sterile equipment to and from hospital’s sterilisation centre. | 89 × 58 × 35.2 (cm). Maximum payload of 100kg, maximum speed of 1.5 m/s, four ultrasound sensors, two 3D cameras for object detection, and two SICK safety laser scanners. | |
| [39] | Hercules | 2019 | Unity Drive Innovation (UDI) | Contactless food delivery. | 365 × 156 × 195 (cm). Maximum payload of 1000kg, 100km before charge needed, speed of 30 kph for saftety, four LiDAR sensors and four cameras for object detection and navigation, 16 sonars, and a redundant satellite navigation system. | |
| [40] | White Rhino | 2019 | White Rhino Auto | Transport medical supplies and delivery food to healthcare staff. | Top speed of 25 kph, 3D LiDAR and cameras for obstacle avoidance. | |
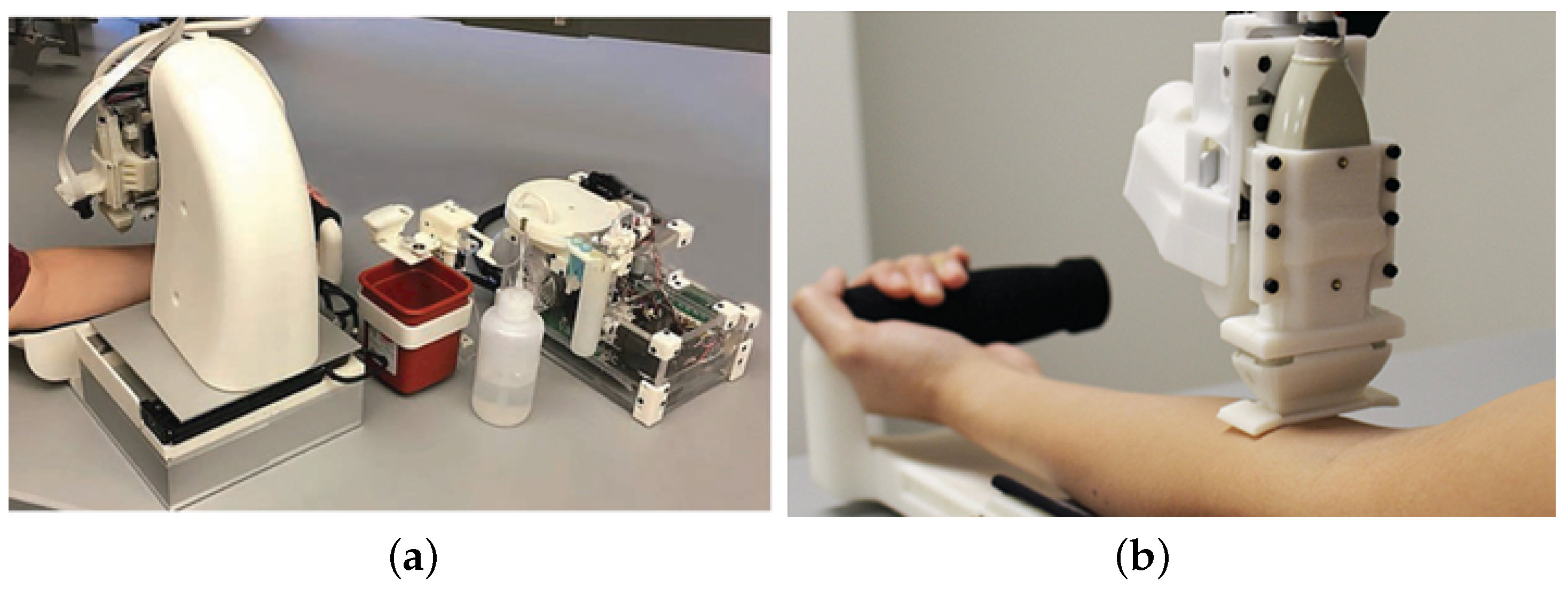
| Testing and Sorting | [41] | Venipuncture Robot | 2018 | Academic/Research based | End-to-end blood testing—drawing blood and providing diagnostic results. | Stereo cameras, transducer, needle manipulator, force sensor, pump switch pump, sample dispenser unit |
| [42] | Hand-held Venipuncture Device | 2019 | Academic/Research based | Rapid venous blood draws. | 2D ultrasound sensors, needle manipulator, electromagnetic needle loader, force sensor, ultrasound probe, and host processor. | |
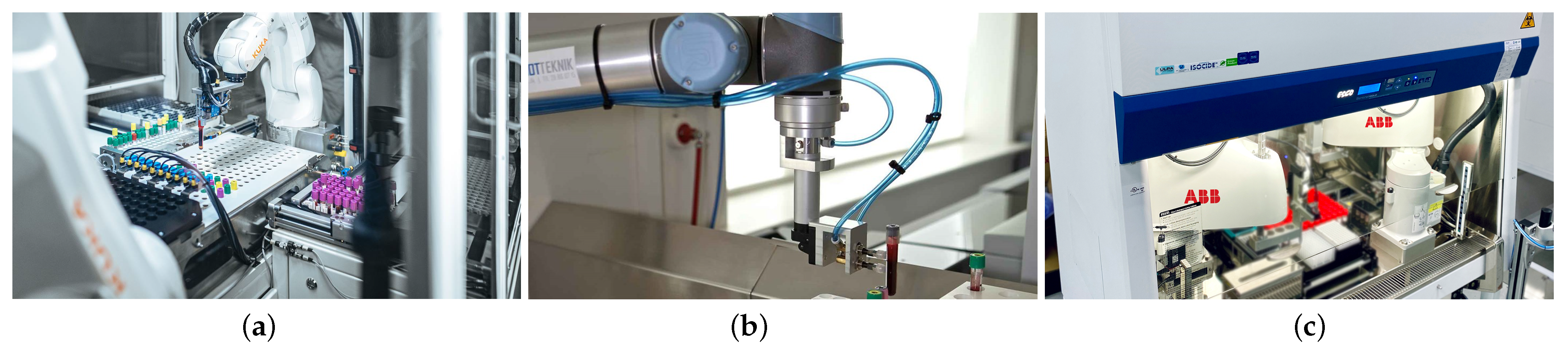
| [43] | KUKA KR3 | 2016 | KUKA Robotics | Open boxes, remove and sort samples. | 17.9 × 17.9 (cm). Reach of 53 cm, maximum payload of 3 kg, six axes, and motion range of 170°–250°, | |
| [44] | UR5 | 2008 | Universal Robotics | Handling and sorting of blood samples. | 47.5 42.3 × 26.8 (cm). Reach of 85 cm, maximum payload of 5 kgs, joint range of 360°. | |
| [45] | Rapid Volume Enhancer (RAVE) | 2020 | ABB | Processing of COVID-19 samples | 16 × 16 (cm). Reach of 45–65 cm, maximum payload of 6 kg, joint range of 280°–300°, | |
| [46] | YuMi | 2015 | ABB | Aiding in serological testing for COVID-19 | 39.9 × 49.7 × 57.1 (cm). Payload of 500 g, reach of 80 cm, 7 axes, and dual arm. |
| Application | Ref. | Year of Dev. | Make | Robot Name | Service Area | Specifications |
|---|---|---|---|---|---|---|
| Social Interaction | [47] | 2014 | SoftBank Robotics | Pepper | Social interaction and entertainment. | 120 × 53.5 × 48.5 (cm). Moves up to 3 kph. Four microphones, RGB camera, two 3D sensors, five touch sensors, two gyro sensors, sonar and laser senors, bumper sensor. |
| [48] | 2018 | Anki/Digital Dream Labs | Vector | Social connectivity, shares daily activities, entertainment. | HD camera, four microphone array, touch sensors, and accelerometer. | |
| [49] | 2020 | Academic/Research based | Lio | Human interaction and personal care. | 79 × 58 × 163 (cm). robotics arm manipulator, two cameras, microphone, ultrasonic sensors, LiDAR, floor sensors, speakers, and display unit. | |
| [50] | 2013 | BlueSky Robotics and MobileRobots | Socially Assistive Robot (SAR) | Socially assistive—social interaction and physical exercise. | USB camera, Humanoid torso: 6 DOF arms, 1 DOF 1 DOF two gripping hands, a 2 DOF pan/tilt neck, 1 DOF expressive eyebrows, and a 2 DOF expressive mouth. Pioneer 2DX mobile base: run time 8–10 h. | |
| [51] | 2015 | PAL Robotics | TIAGo | socially assistive—alarm, reminder, monitors vitals, and locate everyday items. | 54 × 54 × 110 (cm). Maximum payload of 3 kg, 5 h battery duration, RGBD camera, laptop tray, microphone and speaker, and arm manipulator with end-effector. TIAGo base: Maximum payload of 10kg. | |
| Development of Social Skills | [52] | 2018 | Academic/Research based | Autonomous SAR | Development of social communication skills through games. | Combination of virtual assistant, film camera, tracking camera, touchscreen, and computer monitor. |
| [53] | 2005 | Academic/Research based | Keepon | Development of interpersonal communication skills through playtime. | 12 cm tall, CCD camera, microphone, gimbal for body manipulation. | |
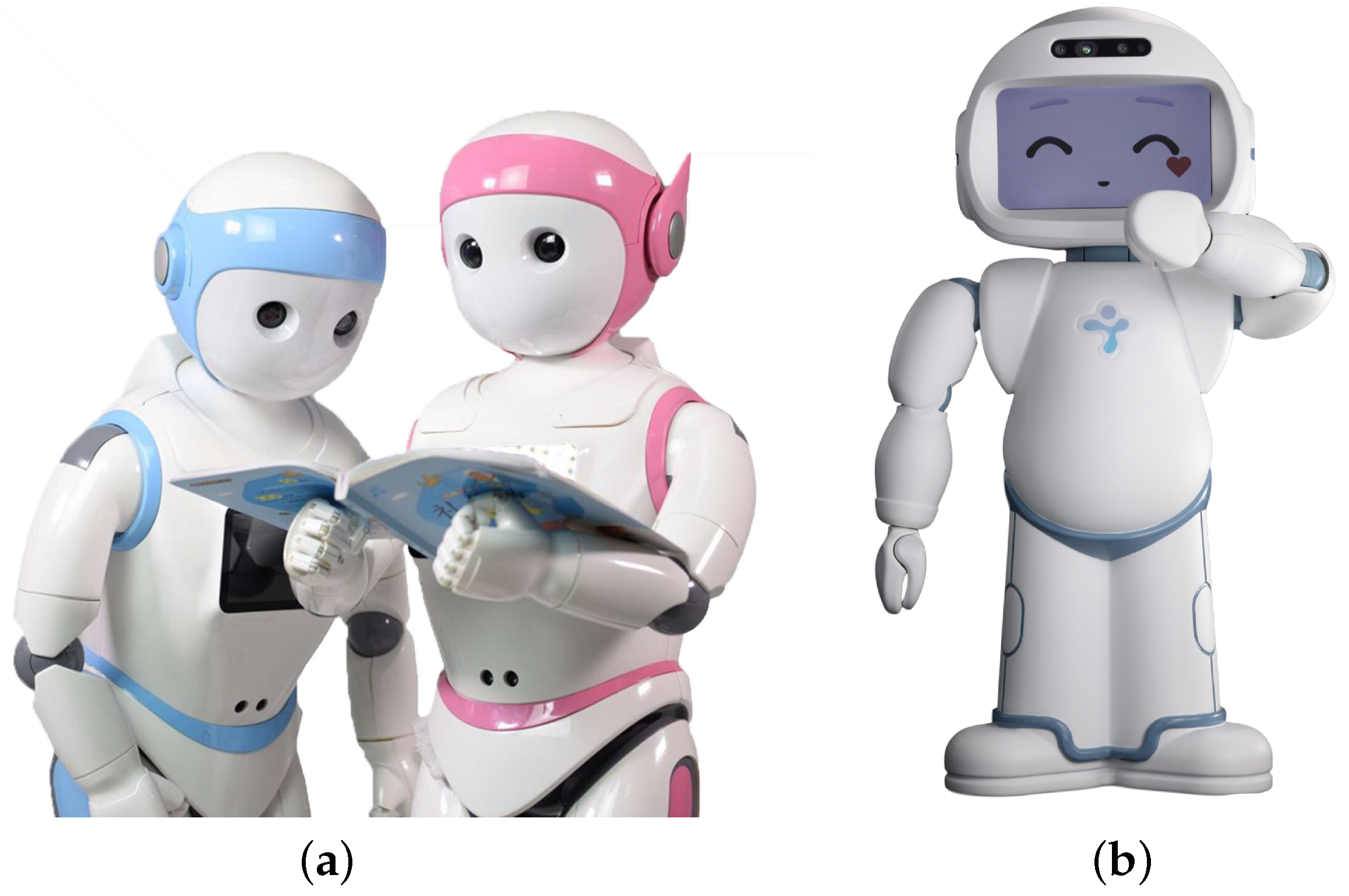
| [54] | 2017 | LuxAI | QTrobot | Robot-assisted therapy for autism. | 63.5 in height (cm). 3D camera, 6 microphones, screen used as face, motors (feedback from position, speed, temperature, load and voltage), and wifi. | |
| [55] | 2017 | AvatarMind | iPal | Robot-assisted therapy for autism. | 106.6 height (cm). LCD display, 4 wheels, camera, 6 microphones, 5 touch sensors, 5 ultrasound sensors, and 3 infrared sensors. |
| Application | Ref. | Year of Dev. | Make | Robot Name | Service Area | Specifications |
|---|---|---|---|---|---|---|
| Patient Monitoring | [56] | 2016 | Academic /Research based | iWard | remote physical condition monitoring for patients. | RGB camera, 3D laser sensor, 3D sensor for object detection, and EQ-01 sensor unit with monitoring belt and sensor electronics module. |
| [57] | 2014 | Academic/Research based | Carebot | Screening of patients in healthcare facility and measuring vital signs. | Based on Yujin Robot’s Charlie [58]: 120 cm tall. Tiltable touch screen, microphones, ultrasonic sensors, bumper sensors, and a laser range finder. | |
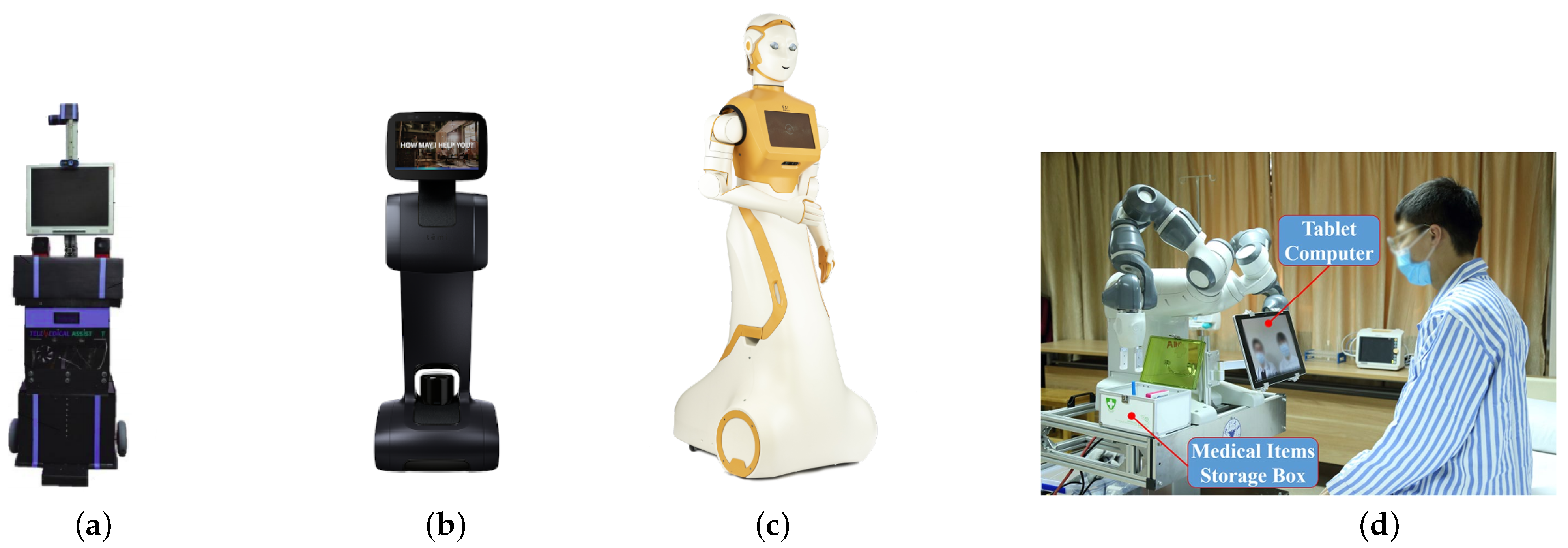
| [59] | 2017 | Academic/Research based | Telemedical Assistant | Record patient’s vitals, dispense medications, and act as a virtual presence to communicate with physicians/family. | HD camera, speakers, medicine and keyboard trays, ultrasonic sensors, solar sensors, and LCD display. | |
| [60] | 2017 | Temi | Temi Robot | Telepresence for the evaluation, monitoring and treatment of patients. | 100 × 35 × 45 (cm). 8 h of operation, moves up to 1 m/s. LiDAR, two depth cameras, RGB camera, five proximity sensors, IMU sensor, six Time of Flight linear sensors, and LCD screen. | |
| [61] | 2019 | PAL Robotics | ARI | Interact with ans screen patients for COVID-19. | 53 × 75 × 165 (cm). Maximum payload of 0.5 kg, operates for 8–12 h, Touch screen, Three cameras, two speakers, and four microphones. | |
| [62] | 2020 | Academic/Research based | Teleoperation Robot System | Daily remote check-ups, remote auscultation and monitoring emotional states. | Dual arm manipulators (YuMi IRB14000), camera, medical storage box, omni-directional chassis, wifi transmission modules, tablet for remote consultation. | |
| [63] | 2020 | Academic/Research based | Cough Detection Robot | COVID-19 screening, recording temperature and any coughing events. | ||
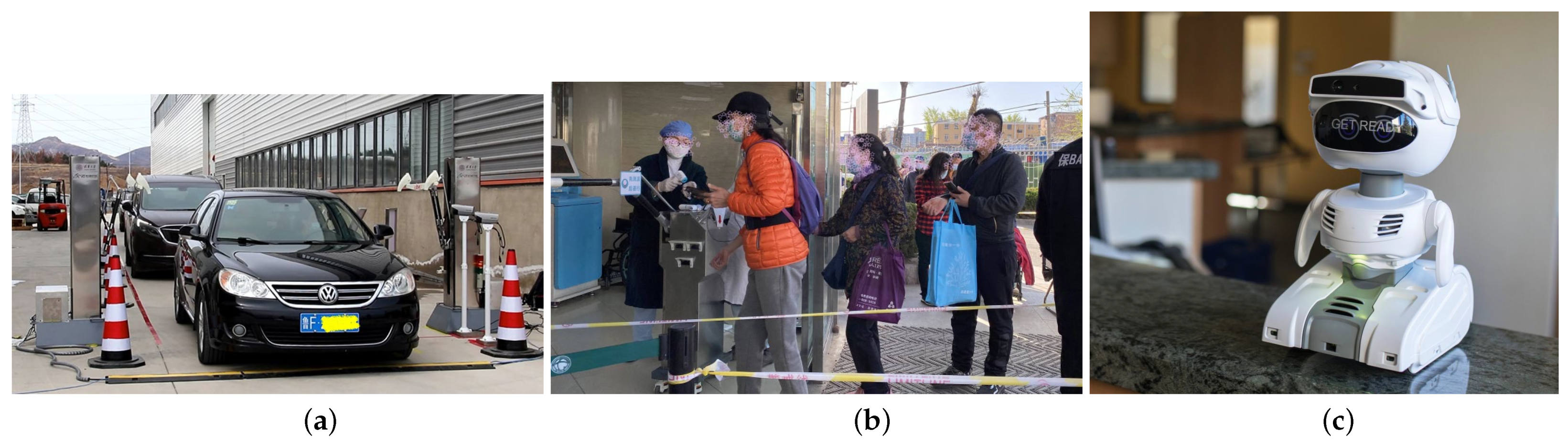
| Mass Monitoring | [64] | 2020 | Academic/Research based | Social Distance Robot | Detection of individuals not complying to social distance measures. | 2D LiDAR, RGBD camera and thermal camera. |
| [65] | 2019 | UBTECH | AIMBOT | temperature measurement, public address system, mask detection, automatic disinfectant. | HD camera, infrared camera, thermal camera, LiDAR, speaker, and disinfection unit with spray nozzle | |
| [66] | 2017 | UBTECH | CRUZR | Point of contact in quarantine areas, remote consultation, mask detection, broadcast health recommendations and vocalise reminders. | LiDAR, sonar sensors, infrared, depth-perception camera, HD camera, speaker, omni-directional wheels, and touchscreen. | |
| [67] | 2020 | Academic/Research based | SHUYU | Temperature screening for drivers and passengers. | Translational parallel manipulator with a closed passive limb, four high accuracy thermometers, two camera, ultrasonic sensors, voice broadcast system and dual IR camera. | |
| [67] | 2020 | Academic/Research based | SHUYUmini | Temperature screening for pedestrians. | Parallelogram manipulator, high accuracy thermometer, three laser ranging sensors, ultrasonic sensor, and IR camera. | |
| [68] | 2020 | Misty Robotics | Misty II | Temperature screening. | 25.4 × 20.32 (cm). Thermal camera, 4K camera, three microphone arrays, speakers LCD display, bump sensors. | |
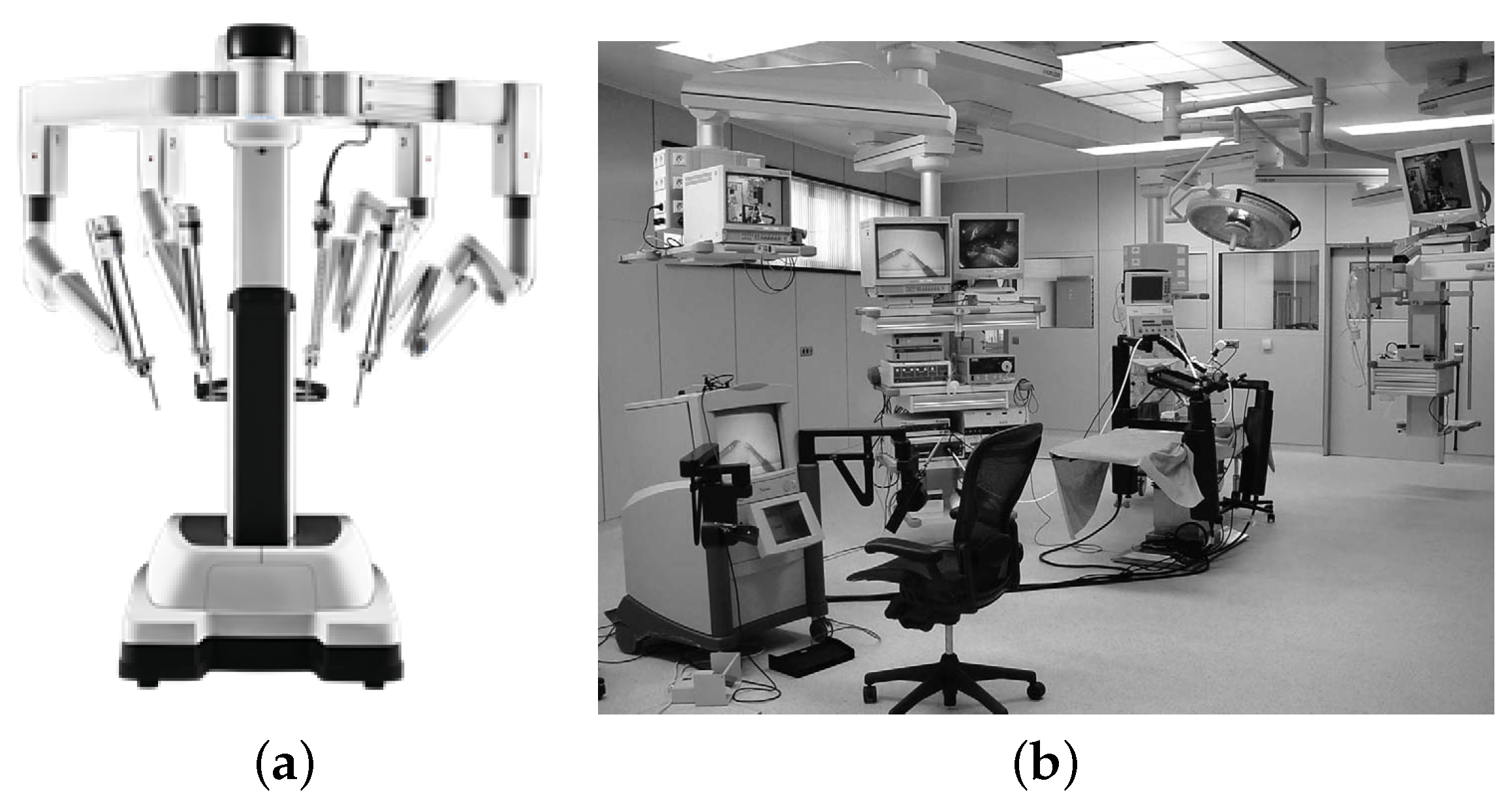
| Remote Surgery | [69] | 1999 | Intuitive Surgical | DaVinci | Minimally invasive surgery. | 91.59 × 127 × 175.3 (cm). Optical and magnetic encoders, hall sensor, IR sensor, and four arm manipulators (as of 2003) |
| [70] | 1995 | Computer Motion | ZEUS | Cardiac, abdominal, gynecology and urology surgeries with a surgeon present. | Three arm manipulators for instrument manipulation and control of a endoscopic camera, and two monitors. | |
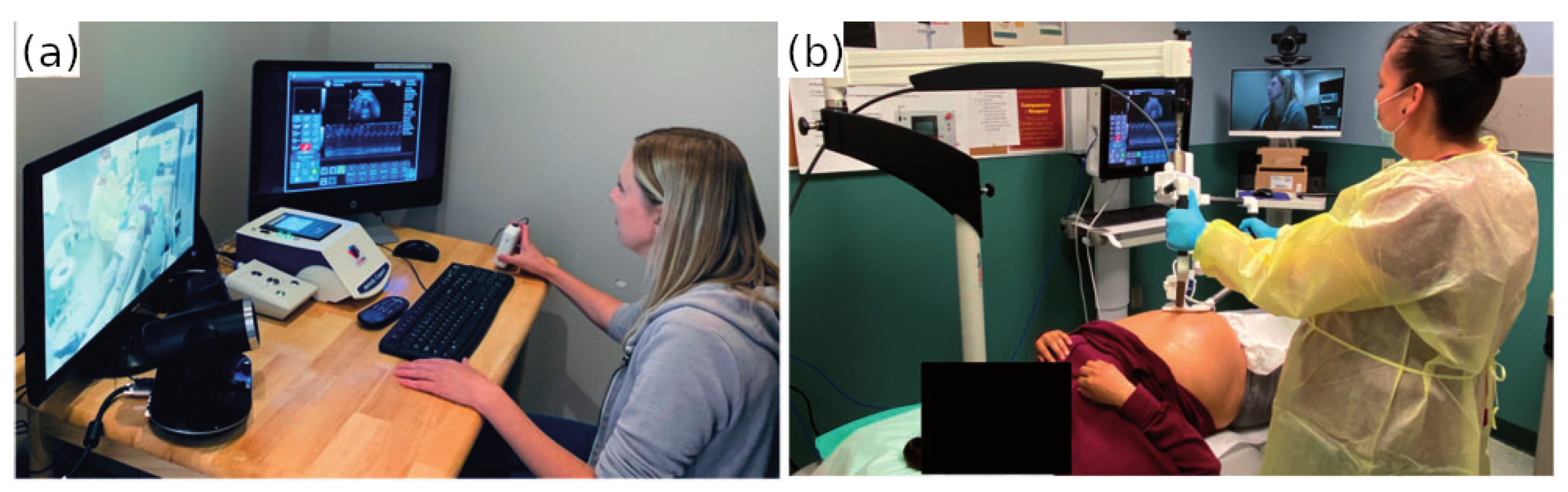
| [71] | 2020 | Academic/Research based | MELODY | Remote ultrasounds. | Three DOF robotic arm manipulator, ultrasound probe, fictive probe and electronic control. | |
| [72] | 2019 | MGI Tech | MGIUS-R3 Tele-echography Robot System | Remote diagnosis of pneumonia. | 108 × 140 × 83 (cm). Two imaging monitors, a fictive transducer, arm manipulator, force sensor with convex and linear array transducers. |
3. Sterilisation
3.1. Ultraviolet Sterilisation

3.2. Hydrogen Peroxide
4. Disinfection
4.1. Disinfecting High Contact Points
4.2. Sanitising Floor and Wall Surfaces
5. COVID-19 Monitoring and Testing
5.1. Monitoring
5.2. Testing
6. Logistics
6.1. Delivery
6.2. Testing and Sorting Blood Samples
7. Social Care
7.1. Social Interaction
7.2. Development of Social Skills
8. Telehealth
8.1. Patient Monitoring
8.2. Remote Surgery
9. Advantages and Challenges
10. Future Areas of Research
11. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vänni, K. Robot applications in communication. Smart Technol. Solut. Support Elder. Contin. Living Their Own Homes. Rep. Minist. Environ. 2017, 7, 44–51. [Google Scholar]
- Centers for Disease Control and Prevention. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Persons Under Investigation (PUIs) for Coronavirus Disease 2019 (COVID-19). Technical Report. 2019. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed on 21 October 2020).
- Christopher Müller. Market for Professional and Domestic Service Robots Booms in 2018. 2019. Available online: https://ifr.org/post/market-for-professional-and-domestic-service-robots-booms-in-2018 (accessed on 13 January 2021).
- Taylor, R.H.; Menciassi, A.; Fichtinger, G.; Fiorini, P.; Dario, P. Medical robotics and computer-integrated surgery. In Springer Handbook of Robotics; Springer: Berlin/Heidelberg, Germany, 2016; pp. 1657–1684. [Google Scholar]
- Schraft, R. Service robot—From vision to realization. Technica 1993, 7, 27–31. [Google Scholar]
- International Standardization Organization. Robots and Robotic Devices—Vocabulary. 2014. Available online: https://www.iso.org/obp/ui/#iso:std:iso:8373:ed-2:v1:en:term:2.10 (accessed on 21 October 2020).
- International Federation of Robotics. Definition of Service Robots. 2014. Available online: http://www.ifr.org/service-robots/ (accessed on 21 October 2020).
- Karabegović, I.; Doleček, V. The role of service robots and robotic systems in the treatment of patients in medical institutions. In Advanced Technologies, Systems, and Applications; Springer: Berlin/Heidelberg, Germany, 2017; pp. 9–25. [Google Scholar]
- Wirtz, J.; Patterson, P.G.; Kunz, W.H.; Gruber, T.; Lu, V.N.; Paluch, S.; Martins, A. Brave new world: Service robots in the frontline. J. Serv. Manag. 2018, 29, 907–931. [Google Scholar] [CrossRef] [Green Version]
- Belanche, D.; Casaló, L.V.; Flavián, C.; Schepers, J. Service robot implementation: A theoretical framework and research agenda. Serv. Ind. J. 2020, 40, 203–225. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Gründel, L.; Seßner, J.; Meiners, M.; Lieret, M.; Lechler, T.; Konrad, C.; Franke, J. Camera-based fall detection system with the service robot sanbot ELF. In Smart Public Building 2018 Conference Proceedings; University of Applied Sciences Stuttgart: Stuttgart, Germany, 2018; pp. 15–28. [Google Scholar]
- Cresswell, K.; Cunningham-Burley, S.; Sheikh, A. Health Care Robotics: Qualitative Exploration of Key Challenges and Future Directions. J. Med. Internet Res. 2018, 20, e10410. [Google Scholar] [CrossRef]
- Chanprakon, P.; Sae-Oung, T.; Treebupachatsakul, T.; Hannanta-Anan, P.; Piyawattanametha, W. An Ultra-violet sterilization robot for disinfection. In Proceedings of the 2019 5th International Conference on Engineering, Applied Sciences and Technology (ICEAST), Luang Prabang, Laos, 2–5 July 2019; pp. 1–4. [Google Scholar]
- UVD Robotics. Reduce Hospital Acquired Infections with the UV Disinfection Robot. Available online: http://www.uvd-robots.com (accessed on 21 October 2020).
- XENEX Disinfection Services. LightStrike Germ-Zapping Robots: Intensity Matters. Available online: https://www.xenex.com/our-solution/lightstrike/ (accessed on 21 October 2020).
- OMRON. LD UVC: Automating UV Disinfection Process Safely and Wisely. 2015. Available online: https://web.omron-ap.com/th/ld-uvc (accessed on 15 January 2021).
- Geek+. Smart UVC Disinfection Robot: The Public Health Guardian. 2020. Available online: https://www.geekplus.com/product-2/smart-uvc-disinfection-robot (accessed on 15 January 2021).
- Andersen, B.; Rasch, M.; Hochlin, K.; Jensen, F.H.; Wismar, P.; Fredriksen, J.E. Decontamination of rooms, medical equipment and ambulances using an aerosol of hydrogen peroxide disinfectant. J. Hosp. Infect. 2006, 62, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Bioquell. Bioquell BQ-50. Available online: https://www.bioquell.com/healthcare/systems-and-services/bioquell-bq-50/ (accessed on 21 October 2020).
- Ramalingam, B.; Yin, J.; Rajesh Elara, M.; Tamilselvam, Y.K.; Mohan Rayguru, M.; Muthugala, M.; Félix Gómez, B. A Human Support Robot for the Cleaning and Maintenance of Door Handles Using a Deep-Learning Framework. Sensors 2020, 20, 3543. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Apuroop, K.G.S.; Tamilselvam, Y.K.; Mohan, R.E.; Ramalingam, B.; Le, A.V. Table Cleaning Task by Human Support Robot Using Deep Learning Technique. Sensors 2020, 20, 1698. [Google Scholar] [CrossRef] [Green Version]
- Cepolina, F.E.; Muscolo, G.G. Design of a robot for hygienization of walls in hospital environments. In ISR/Robotik 2014; 41st International Symposium on Robotics; VDE: Frankfurt, Germany, 2014; pp. 1–7. [Google Scholar]
- Diversey. TASKI Intellibot: The Leader in Autonomous Hands-Free Cleaning. Available online: https://diversey.com/en/solutions/taski-intellibot-robotics (accessed on 21 October 2020).
- The Engineer. XDBOT Set for Covid-19 Cleaning Duties in Singapore. 2020. Available online: https://www.theengineer.co.uk/xdbot-set-for-covid-19-cleaning-duties-in-singapore/ (accessed on 21 October 2020).
- euRobotics. Geek+ Launches Disinfection Robots to Help with cOronavirus Cleanup. 2020. Available online: https://roboticsandautomationnews.com/2020/05/25/geek-launches-disinfection-robots-to-help-with-corona (accessed on 15 January 2021).
- Build With Robots. Breezy One. 2020. Available online: https://buildwithrobots.com/breezyone/ (accessed on 15 January 2021).
- Wang, S.; Wang, K.; Liu, H.; Hou, Z. Design of a Low-cost Miniature Robot to Assist the COVID-19 Nasopharyngeal Swab Sampling. arXiv 2020, arXiv:2005.12679. [Google Scholar]
- LifeLine Robotics. World’s First Automatic Swab Robot. Available online: https://www.lifelinerobotics.com/ (accessed on 21 October 2020).
- Li, S.Q.; Guo, W.L.; Liu, H.; Wang, T.; Zhou, Y.Y.; Yu, T.; Wang, C.Y.; Yang, Y.M.; Zhong, N.S.; Zhang, N.F.; et al. Clinical application of an intelligent oropharyngeal swab robot: Implication for the COVID-19 pandemic. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.; Shim, S.; Park, H.; Baek, J.; Cho, J.H.; Kim, N.H. Development of Robot-Assisted Untact Swab Sampling System for Upper Respiratory Disease. Appl. Sci. 2020, 10, 7707. [Google Scholar] [CrossRef]
- Evans, J.M. HelpMate: An autonomous mobile robot courier for hospitals. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS’94), Munich, Germany, 12–16 September 1994; Volume 3, pp. 1695–1700. [Google Scholar] [CrossRef]
- Bačík, J.; Ďurovskỳ, F.; Biroš, M.; Kyslan, K.; Perdukova, D.; Padmanaban, S. Pathfinder–development of automated guided vehicle for hospital logistics. IEEE Access 2017, 5, 26892–26900. [Google Scholar] [CrossRef]
- Aethon. TUG: Smart Autonomous Mobile Robot. Available online: https://aethon.com/wp-content/uploads/2018/10/TUG_in_healthcare.pdf (accessed on 21 October 2020).
- Panasonic. Panasonic Autonomous Delivery Robots—HOSPI—Aid Hospital Operations at Changi General Hospital. 2015. Available online: https://news.panasonic.com/global/topics/2015/44009.html (accessed on 21 October 2020).
- Carreira, F.; Canas, T.; Silva, A.; Cardeira, C. I-Merc: A mobile robot to deliver meals inside health services. In Proceedings of the 2006 IEEE Conference on Robotics, Automation and Mechatronics, Bangkok, Thailand, 7–9 June 2006; pp. 1–8. [Google Scholar]
- IEEE Spectrum. Diligent Robotics Bringing Autonomous Mobile Manipulation to Hospitals. 2018. Available online: https://spectrum.ieee.org/automaton/robotics/industrial-robots/diligent-robotics-bringing-autonomous-mobile-manipulation-to-hospitals (accessed on 18 January 2021).
- Diligent Robotics. Care is a Team Effort. Available online: https://diligentrobots.com/moxi (accessed on 18 January 2021).
- Mobile Industrial Robotics. Mobile Robot Transports Sterile Goods in Hospital. 2018. Available online: https://www.mobile-industrial-robots.com/en/insights/case-studies/mobile-robot-transports-sterile-goods-in-hospital/ (accessed on 19 January 2021).
- Unity Drive Innovation. Beyond Autonomous Driving. 2020. Available online: https://unity-drive.com (accessed on 15 January 2021).
- United Nations Industrial Development Organization. In China, Robot Delivery Vehicles Deployed to Help with COVID-19 Emergency. 2020. Available online: https://www.unido.org/stories/china-robot-delivery-vehicles-deployed-help-covid-19-emergency (accessed on 15 January 2021).
- Balter, M.; Leipheimer, J.; Chen, A.; Shrirao, A.; Maguire, T.; Yarmush, M. Automated end-to-end blood testing at the point-of-care: Integration of robotic phlebotomy with downstream sample processing. Technology 2018, 6, 59–66. [Google Scholar] [CrossRef]
- Leipheimer, J.M.; Balter, M.L.; Chen, A.I.; Pantin, E.J.; Davidovich, A.E.; Labazzo, K.S.; Yarmush, M.L. First-in-human evaluation of a hand-held automated venipuncture device for rapid venous blood draws. Technology 2019, 7, 98–107. [Google Scholar] [CrossRef] [PubMed]
- KUKA. Hospital 4.0: KUKA Lab Robots Sort Up to 3000 Blood Samples per Day. Available online: https://www.kuka.com/en-de/industries/solutions-database/2020/03/hospital-4-0_kuka-lab-robots-sort-blood-samples (accessed on 21 October 2020).
- Universal Robotics. Two UR5 Universal Robots Ensure Faster Delivery of Blood Sample Results. Available online: https://www.universal-robots.com/case-stories/gentofte-hospital/ (accessed on 21 October 2020).
- ABB. ABB Robots Accelerate COVID-19 Testing in Singapore. 2020. Available online: https://new.abb.com/news/detail/68679/abb-robots-accelerate-covid-19-testing-in-singapore (accessed on 14 January 2021).
- Politecnico Di Milano. COVID-19: YuMi, a Collaborative Robot Helps Analyse a Higher Number of Serological Tests. 2020. Available online: https://www.mynewsdesk.com/it/politecnico-di-milano/pressreleases/covid-19-yumi-a-collaborative-robot-helps-analyse-a-higher-number-of-serological-tests-3034336 (accessed on 14 January 2021).
- SoftBank Robotics. Pepper. Available online: https://www.softbankrobotics.com/emea/en/pepper (accessed on 18 January 2021).
- Digital Dream Labs. Meet Vector. Available online: https://www.digitaldreamlabs.com/pages/meet-vector (accessed on 18 January 2021).
- Mišeikis, J.; Caroni, P.; Duchamp, P.; Gasser, A.; Marko, R.; Mišeikienė, N.; Zwilling, F.; de Castelbajac, C.; Eicher, L.; Früh, M.; et al. Lio-a personal robot assistant for human-robot interaction and care applications. IEEE Robot. Autom. Lett. 2020, 5, 5339–5346. [Google Scholar] [CrossRef]
- Fasola, J.; Matarić, M.J. A socially assistive robot exercise coach for the elderly. J. Hum.-Robot Interact. 2013, 2, 3–32. [Google Scholar] [CrossRef] [Green Version]
- IEEE Spectrum. TIAGo: The Robot That Fits and Adapts to Your Research, Not the Other Way Around. 2020. Available online: https://pal-robotics.com/robots/tiago/ (accessed on 18 January 2021).
- Scassellati, B.; Boccanfuso, L.; Huang, C.M.; Mademtzi, M.; Qin, M.; Salomons, N.; Ventola, P.; Shic, F. Improving social skills in children with ASD using a long-term, in-home social robot. Sci. Robot. 2018, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozima, H.; Nakagawa, C.; Yasuda, Y. Interactive robots for communication-care: A case-study in autism therapy. In ROMAN 2005. IEEE International Workshop on Robot and Human Interactive Communication; IEEE: Piscataway, NJ, USA, 2005; pp. 341–346. [Google Scholar]
- LuxAI. QTrobot For Autism. Available online: https://luxai.com/qt-robot-for-autism/ (accessed on 28 January 2021).
- AvatarMind. iPAL Robot Family: For Senior Care, Retail/Hospitality, and Children’s Education. Available online: https://www.ipalrobot.com/ (accessed on 28 January 2021).
- Mamun, K.A.; Sharma, A.; Islam, F.; Hoque, A.; Szecsi, T. Patient Condition Monitoring Modular Hospital Robot. JSW 2016, 11, 768–786. [Google Scholar] [CrossRef]
- Ahn, H.S.; Lee, M.H.; MacDonald, B.A. Healthcare robot systems for a hospital environment: CareBot and ReceptionBot. In Proceedings of the 2015 24th IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Kobe, Japan, 31 August–4 September 2015; pp. 571–576. [Google Scholar]
- Ahn, H.S.; Kuo, I.H.; Datta, C.; Stafford, R.; Kerse, N.; Peri, K.; Broadbent, E.; MacDonald, B.A. Design of a kiosk type healthcare robot system for older people in private and public places. In International Conference on Simulation, Modeling, and Programming for Autonomous Robots; Springer: Berlin/Heidelberg, Germany, 2014; pp. 578–589. [Google Scholar]
- Arif, D.; Ahmad, A.; Bakar, M.A.; Ihtisham, M.H.; Winberg, S. Cost effective solution for minimization of medical errors and acquisition of vitals by using autonomous nursing robot. In Proceedings of the 2017 International Conference on Information System and Data Mining, Charleston, SC, USA, 1–3 April 2017; pp. 134–138. [Google Scholar]
- Robotemi. Temi: The Personal Robot. Available online: https://www.robotemi.com/specs/ (accessed on 21 October 2020).
- PAL Robotics. ARI. Available online: https://pal-robotics.com/robots/ari/ (accessed on 18 January 2021).
- Yang, G.; Lv, H.; Zhang, Z.; Yang, L.; Deng, J.; You, S.; Du, J.; Yang, H. Keep Healthcare Workers Safe: Application of Teleoperated Robot in Isolation Ward for COVID-19 Prevention and Control. Chin. J. Mech. Eng. 2020, 33, 1–4. [Google Scholar] [CrossRef]
- Wei, W.; Wang, J.; Ma, J.; Cheng, N.; Xiao, J. A Real-time Robot-based Auxiliary System for Risk Evaluation of COVID-19 Infection. arXiv 2020, arXiv:2008.07695. [Google Scholar]
- Sathyamoorthy, A.J.; Patel, U.; Savle, Y.A.; Paul, M.; Manocha, D. COVID-Robot: Monitoring Social Distancing Constraints in Crowded Scenarios. arXiv 2020, arXiv:2008.06585. [Google Scholar]
- UBTECH Robotics. Aimbot: Ubtech’s Anti-Epidemic Solution. 2020. Available online: https://www.ubtrobot.com/products/anti-epidemic-solution (accessed on 21 October 2020).
- Bogue, R. Robots in a contagious world. Ind. Robot. Int. J. Robot. Res. Appl. 2020, 47, 642–673. [Google Scholar] [CrossRef]
- Gong, Z.; Jiang, S.; Meng, Q.; Ye, Y.; Li, P.; Xie, F.; Zhao, H.; Lv, C.; Wang, X.; Liu, X. SHUYU Robot: An Automatic Rapid Temperature Screening System. Chin. J. Mech. Eng. 2020, 33, 1–4. [Google Scholar] [CrossRef]
- Misty Robotics. Say “Hello” to Your New Temperature Screening Assistant. Available online: https://temperature.mistyrobotics.com/ (accessed on 14 January 2021).
- Ewing, D.R.; Pigazzi, A.; Wang, Y.; Ballantyne, G.H. Robots in the operating room—The history. In Seminars in laparoscopic Surgery; Sage Publications: Thousand Oaks, CA, USA, 2004; Volume 11, pp. 63–71. [Google Scholar]
- Marescaux, J.; Rubino, F. The ZEUS robotic system: Experimental and clinical applications. Surg. Clin. 2003, 83, 1305–1315. [Google Scholar] [CrossRef]
- Adams, S.J.; Burbridge, B.; Chatterson, L.; McKinney, V.; Babyn, P.; Mendez, I. Telerobotic ultrasound to provide obstetrical ultrasound services remotely during the COVID-19 pandemic. J. Telemed. Telecare 2020, 1357633X20965422. [Google Scholar] [CrossRef]
- Wang, J.; Peng, C.; Zhao, Y.; Ye, R.; Hong, J.; Huang, H.; Chen, L. Application of a Robotic Tele-Echography System for COVID-19 Pneumonia. J. Ultrasound Med. 2021, 40, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, A.; Ottria, G.; Amicizia, D.; Perdelli, F.; Cristina, M.L. Operating theatre quality and prevention of surgical site infections. J. Prev. Med. Hyg. 2013, 54, 131–137. [Google Scholar]
- Arnold, C. Rethinking Sterile: The Hospital Microbiome; Environmental Health Perspectives: Durham, NC, USA, 2014; pp. A182–A187. [Google Scholar] [CrossRef]
- Vickery, K.; Deva, A.; Jacombs, A.; Allan, J.; Valente, P.; Gosbell, I.B. Presence of biofilm containing viable multiresistant organisms despite terminal cleaning on clinical surfaces in an intensive care unit. J. Hosp. Infect. 2012, 80, 52–55. [Google Scholar] [CrossRef]
- Carling, P.C.; Huang, S.S. Improving Healthcare Environmental Cleaning and Disinfection Current and Evolving Issues. Infect. Control Hosp. Epidemiol. 2013, 34, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.Z.; Nelson, B.J.; Murphy, R.R.; Choset, H.; Christensen, H.; Collins, S.H.; Dario, P.; Goldberg, K.; Ikuta, K.; Jacobstein, N.; et al. Combating COVID-19—The Role of Robotics in Managing Public Health and Infectious Diseases. 2020. Available online: https://robotics.sciencemag.org/content/robotics/5/40/eabb5589.full.pdf (accessed on 11 January 2021).
- McKeen, L. Introduction to Food Irradiation and Medical Sterilization. In The Effect of Sterilization on Plastics and Elastomers, 3rd ed.; McKeen, L., Ed.; Plastics Design Library, William Andrew Publishing: Boston, MA, USA, 2012; pp. 1–40. [Google Scholar] [CrossRef]
- Casini, B.; Tuvo, B.; Cristina, M.L.; Spagnolo, A.M.; Totaro, M.; Baggiani, A.; Privitera, G.P. Evaluation of an ultraviolet C (UVC) light-emitting device for disinfection of high touch surfaces in hospital critical areas. Int. J. Environ. Res. Public Health 2019, 16, 3572. [Google Scholar] [CrossRef] [Green Version]
- Lindblad, M.; Tano, E.; Lindahl, C.; Huss, F. Ultraviolet-C decontamination of a hospital room: Amount of UV light needed. Burns 2020, 46, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Beal, A.; Mahida, N.; Staniforth, K.; Vaughan, N.; Clarke, M.; Boswell, T. First UK trial of Xenex PX-UV, an automated ultraviolet room decontamination device in a clinical haematology and bone marrow transplantation unit. J. Hosp. Infect. 2016, 93, 164–168. [Google Scholar] [CrossRef]
- Narita, K.; Asano, K.; Naito, K.; Ohashi, H.; Sasaki, M.; Morimoto, Y.; Igarashi, T.; Nakane, A. Ultraviolet C light with wavelength of 222 nm inactivates a wide spectrum of microbial pathogens. J. Hosp. Infect. 2020, 105, 459–467. [Google Scholar] [CrossRef]
- Buonanno, M.; Randers-Pehrson, G.; Bigelow, A.W.; Trivedi, S.; Lowy, F.D.; Spotnitz, H.M.; Hammer, S.M.; Brenner, D.J. 207-nm UV light-a promising tool for safe low-cost reduction of surgical site infections. I: In vitro studies. PLoS ONE 2013, 8, e76968. [Google Scholar] [CrossRef] [Green Version]
- Buonanno, M.; Stanislauskas, M.; Ponnaiya, B.; Bigelow, A.W.; Randers-Pehrson, G.; Xu, Y.; Shuryak, I.; Smilenov, L.; Owens, D.M.; Brenner, D.J. 207-nm UV light—A promising tool for safe low-cost reduction of surgical site infections. II: In-vivo safety studies. PLoS ONE 2016, 11, e0138418. [Google Scholar]
- Buonanno, M.; Ponnaiya, B.; Welch, D.; Stanislauskas, M.; Randers-Pehrson, G.; Smilenov, L.; Lowy, F.D.; Owens, D.M.; Brenner, D.J. Germicidal efficacy and mammalian skin safety of 222-nm UV light. Radiat. Res. 2017, 187, 493–501. [Google Scholar] [CrossRef] [Green Version]
- Ponnaiya, B.; Buonanno, M.; Welch, D.; Shuryak, I.; Randers-Pehrson, G.; Brenner, D.J. Far-UVC light prevents MRSA infection of superficial wounds in vivo. PLoS ONE 2018, 13, e0192053. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, D. Ultraviolet Light Fights New Virus. Engineering 2020, 6, 851–853. [Google Scholar] [CrossRef]
- Healthe. Cleanse Portal. Available online: https://healthelighting.com/collections/cleanse-products/products/cleanse-portal (accessed on 21 October 2020).
- Nerandzic, M.M.; Thota, P.; Sankar, T.; Jencson, A.; Cadnum, J.L.; Ray, A.J.; Salata, R.A.; Watkins, R.R.; Donskey, C.J. Evaluation of a pulsed xenon ultraviolet disinfection system for reduction of healthcare-associated pathogens in hospital rooms. Infect. Control Hosp. Epidemiol. 2015, 36, 192–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilhunen, S.; Sillanpää, M. Recent developments in photochemical and chemical AOPs in water treatment: A mini-review. Rev. Environ. Sci. Bio Technol. 2010, 9, 323–330. [Google Scholar] [CrossRef]
- Gomez-Lopez, V.M.; Ragaert, P.; Debevere, J.; Devlieghere, F. Pulsed light for food decontamination: A review. Trends Food Sci. Technol. 2007, 18, 464–473. [Google Scholar] [CrossRef]
- McDonald, K.F.; Curry, R.D.; Clevenger, T.E.; Unklesbay, K.; Eisenstark, A.; Golden, J.; Morgan, R.D. A comparison of pulsed and continuous ultraviolet light sources for the decontamination of surfaces. IEEE Trans. Plasma Sci. 2000, 28, 1581–1587. [Google Scholar] [CrossRef]
- Nyangaresi, P.O.; Qin, Y.; Chen, G.; Zhang, B.; Lu, Y.; Shen, L. Comparison of the performance of pulsed and continuous UVC-LED irradiation in the inactivation of bacteria. Water Res. 2019, 157, 218–227. [Google Scholar] [CrossRef]
- McLeod, A.; Hovde Liland, K.; Haugen, J.E.; Sørheim, O.; Myhrer, K.S.; Holck, A.L. Chicken fillets subjected to UV-C and pulsed UV light: Reduction of pathogenic and spoilage bacteria, and changes in sensory quality. J. Food Saf. 2018, 38, e12421. [Google Scholar] [CrossRef] [Green Version]
- Holck, A.L.; Liland, K.H.; Drømtorp, S.M.; Carlehög, M.; McLeod, A. Comparison of UV-C and pulsed UV light treatments for reduction of Salmonella, Listeria monocytogenes, and enterohemorrhagic Escherichia coli on eggs. J. Food Prot. 2018, 81, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Otaki, M.; Okuda, A.; Tajima, K.; Iwasaki, T.; Kinoshita, S.; Ohgaki, S. Inactivation differences of microorganisms by low pressure UV and pulsed xenon lamps. Water Sci. Technol. 2003, 47, 185–190. [Google Scholar] [CrossRef]
- Bates, C.; Pearse, R. Use of hydrogen peroxide vapour for environmental control during a Serratia outbreak in a neonatal intensive care unit. J. Hosp. Infect. 2005, 61, 364–366. [Google Scholar] [CrossRef]
- Jeanes, A.; Rao, G.; Osman, M.; Merrick, P. Eradication of persistent environmental MRSA. J. Hosp. Infect. 2005, 61, 85–86. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M.; Havill, N.L.; Otter, J.A.; McDonald, L.C.; Adams, N.M.; Cooper, T.; Thompson, A.; Wiggs, L.; Killgore, G.; Tauman, A.; et al. Impact of hydrogen peroxide vapor room decontamination on Clostridium difficile environmental contamination and transmission in a healthcare setting. Infect. Control Hosp. Epidemiol. 2008, 29, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.; Gent, P.; Kumar, V. Efficacy, efficiency and safety aspects of hydrogen peroxide vapour and aerosolized hydrogen peroxide room disinfection systems. J. Hosp. Infect. 2012, 80, 199–205. [Google Scholar] [CrossRef]
- Bioquell. Aerosolised Versus Bioquell’s Hydrogen Peroxide Vapour. Available online: https://www.bioquell.com/healthcare/aerosolized-versus-bioquells-hydrogen-peroxide-vapor/ (accessed on 21 October 2020).
- Kovach, C.R.; Taneli, Y.; Neiman, T.; Dyer, E.M.; Arzaga, A.J.A.; Kelber, S.T. Evaluation of an ultraviolet room disinfection protocol to decrease nursing home microbial burden, infection and hospitalization rates. BMC Infect. Dis. 2017, 17, 186. [Google Scholar] [CrossRef] [Green Version]
- Taski. TASKI Has Led the Automation Revolution and Will Continue to Bring Disruptive Technologies. Available online: https://taski.com/products-innovations-solutions/products/robotics/ (accessed on 9 March 2021).
- NED Directory. Robot Protectors for COVID-19. 2020. Available online: https://directory.newequipment.com/classified/robot-protectors-for-covid-19-253752.html (accessed on 15 January 2021).
- Fetch Robotics. Build With Robots, Fetch Robotics and the City of Albuquerque Launch the Breezy One, Autonomous Disinfecting Robot at Albuquerque International Sunport. 2020. Available online: https://fetchrobotics.com/fetch-robotics-blog/build-with-robots-fetch-robotics-and-the-city-of-albuquerque-launch-the-breezy-one-autonomous-disinfecting-robot-at-albuquerque-international-sunport/ (accessed on 15 January 2021).
- Jeon, S.; Lee, J. Multi-robot Control Architecture for Hospital Delivery Service in Unstable Network Environment. In ICINCO (2); SciTePress: Setúbal, Portugal, 2017; pp. 270–277. [Google Scholar]
- Bloss, R. Mobile hospital robots cure numerous logistic needs. Ind. Robot 2011, 38, 567–571. [Google Scholar] [CrossRef]
- World Health Organisation Europe. CINDI Dietary Guide. Technical Report. 2000. Available online: https://www.euro.who.int/__data/assets/pdf_file/0010/119926/E70041.pdf (accessed on 21 October 2020).
- IEEE Spectrum. Moxi Prototype from Diligent Robotics Starts Helping Out in Hospitals. 2018. Available online: https://spectrum.ieee.org/automaton/robotics/industrial-robots/moxi-prototype-from-diligent-robotics-starts-helping-out-in-hospitals (accessed on 18 January 2021).
- IEEE Spectrum. Robot Vehicles Make Contactless Deliveries Amid Coronavirus Quarantine. 2020. Available online: https://spectrum.ieee.org/automaton/transportation/self-driving/robot-vehicles-make-contactless-deliveries-amid-coronavirus-quarantine (accessed on 15 January 2021).
- White Rhino Auto. Unmanned: Make Items Arrive Faster. 2020. Available online: http://www.white-rhino.auto/ (accessed on 15 January 2021).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Mushtaq, R.; Shoib, S.; Shah, T.; Mushtaq, S. Relationship between loneliness, psychiatric disorders and physical health? A review on the psychological aspects of loneliness. J. Clin. Diagn. Res. JCDR 2014, 8, WE01. [Google Scholar] [CrossRef] [PubMed]
- Ikeuchi, T.; Sakurai, R.; Furuta, K.; Kasahara, Y.; Imamura, Y.; Shinkai, S. Utilizing social robot to reduce workload of healthcare professionals in a psychiatric hospital: A preliminary study. Innov. Aging 2018, 2, 695–696. [Google Scholar] [CrossRef]
- Odekerken-Schröder, G.; Mele, C.; Russo-Spena, T.; Mahr, D.; Ruggiero, A. Mitigating loneliness with companion robots in the COVID-19 pandemic and beyond: An integrative framework and research agenda. J. Serv. Manag. 2020, 31, 1149–1162. [Google Scholar] [CrossRef]
- PAL Robotics. Enrichme. 2019. Available online: https://pal-robotics.com/collaborative-projects/enrichme/ (accessed on 19 January 2021).
- Coşar, S.; Fernandez-Carmona, M.; Agrigoroaie, R.; Pages, J.; Ferland, F.; Zhao, F.; Yue, S.; Bellotto, N.; Tapus, A. ENRICHME: Perception and Interaction of an Assistive Robot for the Elderly at Home. Int. J. Soc. Robot. 2020, 12, 779–805. [Google Scholar] [CrossRef] [Green Version]
- RobotLab. RobotLab Autism Mobile Solution: Robot-Assisted Therapy for Autism. Available online: https://www.robotlab.com/store/autism-mobile-solution (accessed on 29 January 2021).
- RobotLab. iPal Robot Autism Pack: Robot-Assisted Therapy for Autism. Available online: https://www.robotlab.com/store/ipal-autism-pack (accessed on 29 January 2021).
- Tuckson, R.V.; Edmunds, M.; Hodgkins, M.L. Telehealth. New Engl. J. Med. 2017, 377, 1585–1592. [Google Scholar] [CrossRef]
- Tavakoli, M.; Carriere, J.; Torabi, A. Robotics, smart wearable technologies, and autonomous intelligent systems for healthcare during the COVID-19 pandemic: An analysis of the state of the art and future vision. Adv. Intell. Syst. 2020, 2, 2000071. [Google Scholar] [CrossRef]
- Broadbent, E.; Tamagawa, R.; Patience, A.; Knock, B.; Kerse, N.; Day, K.; MacDonald, B.A. Attitudes towards health-care robots in a retirement village. Australas. J. Ageing 2012, 31, 115–120. [Google Scholar] [CrossRef] [PubMed]
- IEEE Spectrum. PAL Robotics Customizable Bots Could Be the Next Frontline Workers. 2020. Available online: https://spectrum.ieee.org/news-from-around-ieee/the-institute/ieee-member-news/pal-robotics-customizable-bots-could-be-the-next-frontline-workers (accessed on 18 January 2021).
- PAL Robotics. COVID-19 and Our Robots: Ready to Help Fight Coronavirus in Hospitals. 2020. Available online: https://blog.pal-robotics.com/covid-19-and-our-robots-ready-to-help-fight-coronavirus-in-hospitals/ (accessed on 18 January 2021).
- Kaiser, M.S.; Al Mamun, S.; Mahmud, M.; Tania, M.H. Healthcare Robots to Combat COVID-19. In COVID-19: Prediction, Decision-Making, and Its Impacts; Springer: Berlin/Heidelberg, Germany, 2020; pp. 83–97. [Google Scholar]
- Khan, Z.H.; Siddique, A.; Lee, C.W. Robotics Utilization for Healthcare Digitization in Global COVID-19 Management. Int. J. Environ. Res. Public Health 2020, 17, 3819. [Google Scholar] [CrossRef]
- Moawad, G.N.; Rahman, S.; Martino, M.A.; Klebanoff, J.S. Robotic surgery during the COVID pandemic: Why now and why for the future. J. Robot. Surg. 2020, 14, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Butner, S.E.; Ghodoussi, M. Transforming a surgical robot for human telesurgery. IEEE Trans. Robot. Autom. 2003, 19, 818–824. [Google Scholar] [CrossRef]
- Cuschieri, A.; Dubois, F.; Mouiel, J.; Mouret, P.; Becker, H.; Buess, G.; Trede, M.; Troidl, H. The European experience with laparoscopic cholecystectomy. Am. J. Surg. 1991, 161, 385–387. [Google Scholar] [CrossRef]
- Reichenspurner, H.; Damiano, R.J.; Mack, M.; Boehm, D.H.; Gulbins, H.; Detter, C.; Meiser, B.; Ellgass, R.; Reichart, B. Use of the voice-controlled and computer-assisted surgical system ZEUS for endoscopic coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 1999, 118, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Mottrie, A.; De Naeyer, G.; Schatteman, P.; Carpentier, P.; Sangalli, M.; Ficarra, V. Impact of the learning curve on perioperative outcomes in patients who underwent robotic partial nephrectomy for parenchymal renal tumours. Eur. Urol. 2010, 58, 127–133. [Google Scholar] [CrossRef]
- Marescaux, J.; Leroy, J.; Rubino, F.; Smith, M.; Vix, M.; Simone, M.; Mutter, D. Transcontinental robot-assisted remote telesurgery: Feasibility and potential applications. Ann. Surg. 2002, 235, 487. [Google Scholar] [CrossRef]
- Nguan, C.; Miller, B.; Patel, R.; Luke, P.P.; Schlachta, C.M. Pre-clinical remote telesurgery trial of a da Vinci telesurgery prototype. Int. J. Med Robot. Comput. Assist. Surg. 2008, 4, 304–309. [Google Scholar] [CrossRef]
- Haidegger, T.; Sándor, J.; Benyó, Z. Surgery in space: The future of robotic telesurgery. Surg. Endosc. 2011, 25, 681–690. [Google Scholar] [CrossRef]
- Vilchis, A.; Masuda, K.; Troccaz, J.; Cinquin, P. Robot-based tele-echography: The TER system. Stud. Health Technol. Inform. 2003, 95, 212–217. [Google Scholar] [PubMed]
- Takeuchi, R.; Harada, H.; Masuda, K.; Ota, G.i.; Yokoi, M.; Teramura, N.; Saito, T. Field testing of a remote controlled robotic tele-echo system in an ambulance using broadband mobile communication technology. J. Med. Syst. 2008, 32, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Watt, B.E.; Proudfoot, A.T.; Vale, J.A. Hydrogen peroxide poisoning. Toxicol. Rev. 2004, 23, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Ford, M. Rise of the Robots: Technology and the Threat of a Jobless Future; Basic Books: New York, NY, USA, 2015. [Google Scholar]
- Bodenhagen, L.; Suvei, S.D.; Juel, W.K.; Brander, E.; Krüger, N. Robot technology for future welfare: Meeting upcoming societal challenges–an outlook with offset in the development in Scandinavia. Health Technol. 2019, 9, 197–218. [Google Scholar] [CrossRef]
- Shen, Y.; Guo, D.; Long, F.; Mateos, L.A.; Ding, H.; Xiu, Z.; Hellman, R.B.; King, A.; Chen, S.; Zhang, C.; et al. Robots under COVID-19 Pandemic: A Comprehensive Survey. IEEE Access 2021, 9, 1590–1615. [Google Scholar] [CrossRef]
- Barabas, C.; Bavitz, C.; Matias, J.N.; Xie, C.; Xu, J. Legal and Ethical Issues in the Use of Telepresence Robots: Best Practices and Toolkit; We Robot 2015 Fourth Annual Conference on Robotics, Law & Policy, University of Washington School of Law; University of Washington: Seattle, WA, USA; Available online: https://hdl.handle.net/1721.1/123454 (accessed on 20 January 2021).
- Cohen, P.; Cheyer, A.; Horvitz, E.; El Kaliouby, R.; Whittaker, S. On the future of personal assistants. In Proceedings of the 2016 CHI Conference Extended Abstracts on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 1032–1037. [Google Scholar]
- Mende, M.; Scott, M.L.; van Doorn, J.; Grewal, D.; Shanks, I. Service robots rising: How humanoid robots influence service experiences and elicit compensatory consumer responses. J. Mark. Res. 2019, 56, 535–556. [Google Scholar] [CrossRef]
- Sheridan, T.B. Human–robot interaction: Status and challenges. Hum. Factors 2016, 58, 525–532. [Google Scholar] [CrossRef]
- Sillice, M.A.; Morokoff, P.J.; Ferszt, G.; Bickmore, T.; Bock, B.C.; Lantini, R.; Velicer, W.F. Using relational agents to promote exercise and sun protection: Assessment of participants’ experiences with two interventions. J. Med. Internet Res. 2018, 20, e48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConachie, D.; Dobson, A.; Ruan, M.; Berenson, D. Manipulating Deformable Objects by Interleaving Prediction, Planning, and Control. arXiv 2020, arXiv:2001.09950. [Google Scholar] [CrossRef]
- Joo, H.; Simon, T.; Cikara, M.; Sheikh, Y. Towards social artificial intelligence: Nonverbal social signal prediction in a triadic interaction. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; pp. 10873–10883. [Google Scholar]
- Yang, G.Z.; Bellingham, J.; Dupont, P.E.; Fischer, P.; Floridi, L.; Full, R.; Jacobstein, N.; Kumar, V.; McNutt, M.; Merrifield, R.; et al. The grand challenges of Science Robotics. Sci. Robot. 2018, 3, eaar7650. [Google Scholar] [CrossRef] [PubMed]
- Joo, H. Sensing, Measuring, and Modeling Social Signals in Nonverbal Communication. Ph.D. Thesis, Carnegie Mellon University, Pittsburgh, PA, USA, 2019. [Google Scholar]


















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holland, J.; Kingston, L.; McCarthy, C.; Armstrong, E.; O’Dwyer, P.; Merz, F.; McConnell, M. Service Robots in the Healthcare Sector. Robotics 2021, 10, 47. https://doi.org/10.3390/robotics10010047
Holland J, Kingston L, McCarthy C, Armstrong E, O’Dwyer P, Merz F, McConnell M. Service Robots in the Healthcare Sector. Robotics. 2021; 10(1):47. https://doi.org/10.3390/robotics10010047
Chicago/Turabian StyleHolland, Jane, Liz Kingston, Conor McCarthy, Eddie Armstrong, Peter O’Dwyer, Fionn Merz, and Mark McConnell. 2021. "Service Robots in the Healthcare Sector" Robotics 10, no. 1: 47. https://doi.org/10.3390/robotics10010047