Testosterone Levels and Type 2 Diabetes—No Correlation with Age, Differential Predictive Value in Men and Women

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcome Information
2.3. Laboratory Methods
2.4. Statistical Methods
3. Results
4. Discussion
4.1. Circulating Levels of Total Testosterone
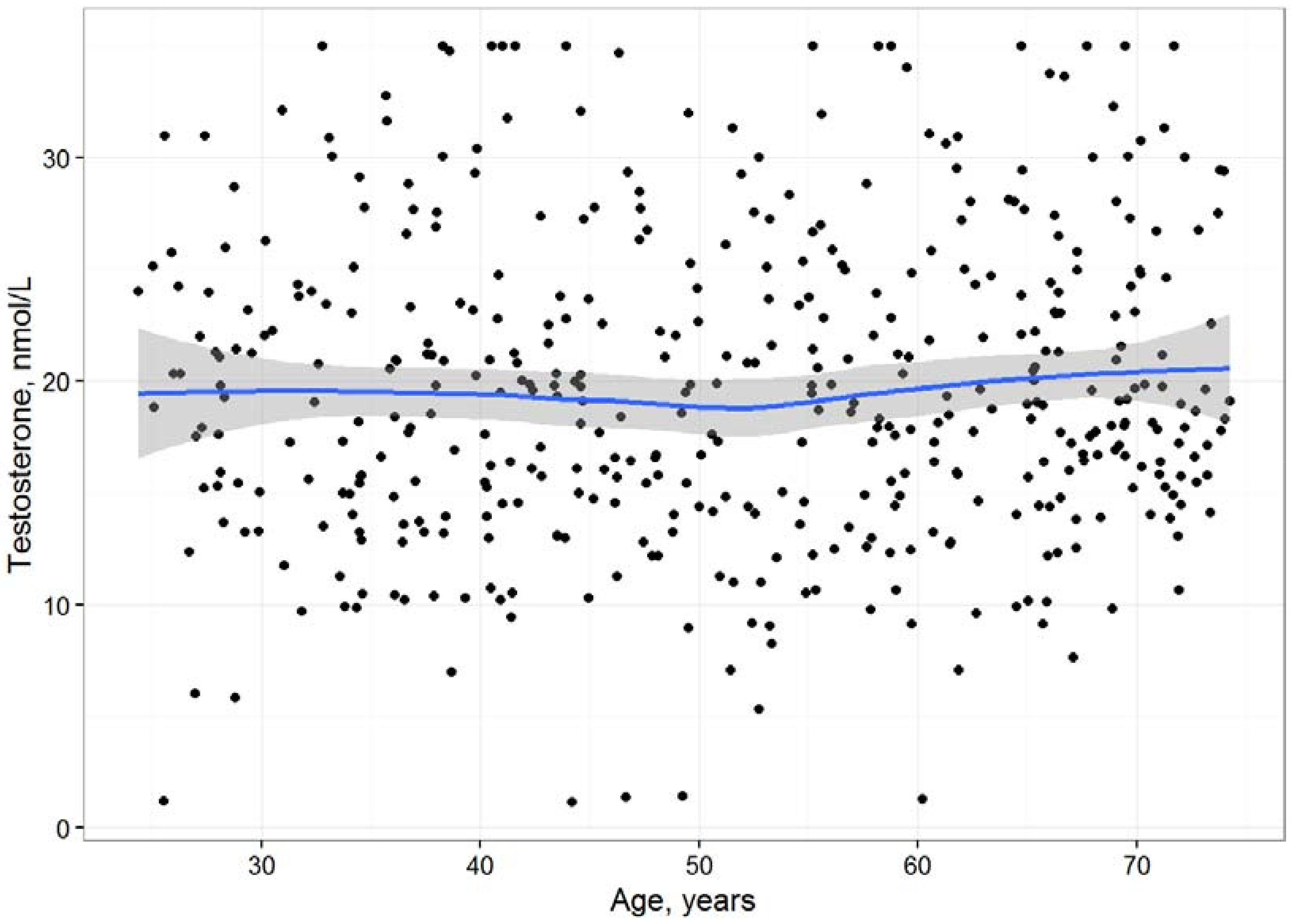
4.2. Correlation of Testosterone with Age
4.3. Association of Testosterone with Incident Type 2 Diabetes and Its Clinical Relevance
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Chan, L.; O’Malley, B.W. Mechanism of action of the sex steroid hormones (first of three parts). N. Engl. J. Med. 1976, 294, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Harman, S.M.; Metter, E.J.; Tobin, J.D.; Pearson, J.; Blackman, M.R. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J. Clin. Endocrinol. Metab. 2001, 86, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Purifoy, F.E.; Koopmans, L.H.; Mayes, D.M. Age differences in serum androgen levels in normal adult males. Hum. Biol. 1981, 53, 499–511. [Google Scholar] [PubMed]
- Gray, A.; Feldman, H.A.; McKinley, J.B.; Longscope, C. Age, disease and changing sex hormone levels in middle-aged men: Longitudinal results from the Massachusettes male aging study. J. Clin. Endocrinol. Metab. 1991, 73, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Swerdloff, R.; Anawalt, B.D. Clinical decisions. Testosterone-replacement therapy. N. Engl. J. Med. 2014, 371, 2032–2034. [Google Scholar] [CrossRef] [PubMed]
- Handelsman, D.J. Mechanisms of action of testosterone–unravelling a Gordian knot. N. Engl. J. Med. 2013, 369, 1058–1059. [Google Scholar] [CrossRef] [PubMed]
- De Keyser, C.E.; de Lima, F.V.; de Jong, F.H.; Hofman, A.; de Rijke, Y.B.; Uitterlinden, A.G.; Visser, L.E.; Stricker, B.H. Use of statins is associated with lower serum total and non-sex hormone-binding globulin-bound testosterone levels in male participants of the Rotterdam Study. Eur. J. Endocrinol. 2015, 173, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sattar, N.; Preiss, D.; Murray, H.M.; Welsh, P.; Buckley, B.M.; de Craen, A.J.; Seshasai, S.R.; McMurray, J.J.; Freeman, D.J.; Jukema, J.W.; et al. Statins and risk of incident diabetes, a collaborative meta-analysis of randomised statin trials. Lancet 2010, 375, 735–742. [Google Scholar] [CrossRef]
- Navarese, E.P.; Buffon, A.; Andreotti, F.; Kozinski, M.; Welton, N.; Fabiszak, T.; Caputo, S.; Grzesk, G.; Kubica, A.; Swiatkiewicz, I.; et al. Meta-analysis of impact of different types and doses of statins on new-onset diabetes mellitus. Am. J. Cardiol. 2013, 111, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Preiss, D.; Seshasai, S.R.; Welsh, P.; Murphy, S.A.; Ho, J.E.; Waters, D.D.; DeMicco, D.A.; Barter, P.; Cannon, C.P.; Sabatine, M.S.; et al. Risk of incident diabetes with intensive-dose compared with moderate-dose statin therapy: A meta-analysis. JAMA 2011, 305, 2556–2564. [Google Scholar] [CrossRef] [PubMed]
- Macedo, A.F.; Douglas, I.; Smeeth, L.; Forbes, H.; Ebrahim, S. Statins and the risk of type 2 diabetes mellitus: Cohort study using the UK clinical practice pesearch datalink. BMC Cardiovasc. Disord. 2014, 14, 85. [Google Scholar] [CrossRef] [PubMed]
- Klinefelter, G.R.; Laskey, J.W.; Amann, R.P. Statin drugs markedly inhibit testosterone production by rat Leydig cells in vitro: Implications for men. Reprod. Toxicol. 2014, 45, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Smals, A.G.; Weusten, J.J.; Benraad, T.J.; Kloppenborg, P.W. The HMG-CoA reductase inhibitor simvastatin suppresses human testicular testosterone synthesis in vitro by a selective inhibitory effect on 17-ketosteroid-oxidoreductase enzyme activity. J. Steroid Biochem. Mol. Biol. 1991, 38, 465–468. [Google Scholar] [CrossRef]
- Gu, Q.; Paulose-Ram, R.; Burt, V.L.; Kit, B.K. Prescription Cholesterol-Lowering Medication Use in Adults Aged 40 and Over: United States, 2003–2012; NCHS data brief 177; National Center for Health Statistics: Hyattsville, MD, USA, 2014. [Google Scholar]
- Ding, E.L.; Song, Y.; Malik, V.S.; Liu, S. Sex differences of endogenous sex hormones and risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2006, 295, 1288–1299. [Google Scholar] [CrossRef] [PubMed]
- Grossmann, M. Testosterone and glucose metabolism in men: Current concepts and controversies. J. Endocrinol. 2014, 220, R37–R55. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Monami, M.; Rastrelli, G.; Aversa, A.; Sforza, A.; Lenzi, A.; Forti, G.; Mannucci, E.; Maggi, M. Type 2 diabetes mellitus and testosterone: A meta-analysis study. Int. J. Androl. 2011, 34, 528–540. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.K.; Luk, A.O.; So, W.Y.; Ma, R.C.; Kong, A.P.; Chow, F.C.; Chan, J.C. Testosterone level in men with type 2 diabetes mellitus and related metabolic effects: A review of current evidence. J. Diabetes Investig. 2015, 6, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Vartiainen, E.; Jousilahti, P.; Alfthan, G.; Sundvall, J.; Pietinen, P.; Puska, P. Cardiovascular risk factor changes in Finland 1972–1997. Int. J. Epidemiol. 2000, 29, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Pajunen, P.; Koukkunen, H.; Ketonen, M.; Jerkkola, T.; Immonen-Räihä, P.; Kärjä-Koskenkari, P.; Mähönen, M.; Niemelä, M.; Kuulasmaa, K.; Palomäki, P.; et al. The validity of the Finnish Hospital Discharge Register and Causes of Death Register data on coronary heart disease. Eur. J. Cardiovasc. Prev. Rehabil. 2005, 12, 132–137. [Google Scholar] [PubMed]
- Sund, R. Quality of the Finnish Hospital Discharge Register: A systematic review. Scand. J. Public Health 2012, 40, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. CKD-EPI Investigators. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Hughes, M.; Tuovinen, T.; Schillert, A.; Conrads-Frank, A.; Ruijter, H.; Schnabel, R.B.; Kee, F.; Salomaa, V.; Siebert, U.; et al. BiomarCaRE: Rationale and design of the European BiomarCaRE project including 300,000 participants from 13 European countries. Eur. J. Epidemiol. 2014, 29, 777–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Vesper, H.W.; Wang, Y.; Vidal, M.; Botelho, J.C.; Caudill, S.P. Serum total testosterone concentrations in the US household population from the NHANES 2011–2012 study population. Clin. Chem. 2015, 61, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Schneider, G.; Kirschner, M.A.; Berkowitz, R.; Ertel, N.H. Increased estrogen production in obese men. J. Clin. Endocrinol. Metab. 1979, 48, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced Glycation End Products and Oxidative Stress in Type 2 Diabetes Mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Kitade, H.; Ni, Y.; Ota, T. Roles of Chemokines and Chemokine Receptors in Obesity-Associated Insulin Resistance and Nonalcoholic Fatty Liver Disease. Biomolecules 2015, 5, 1563–1579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeller, T.; Altay, A.; Waldeyer, C.; Appelbaum, S.; Ojeda, F.; Ruhe, J.; Schnabel, R.B.; Lackner, K.J.; Blankenberg, S.; Karakas, M. Prognostic Value of Iron-Homeostasis Regulating Peptide Hepcidin in Coronary Heart Disease—Evidence from the Large AtheroGene Study. Biomolecules 2018, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Karavassili, F.; Valmas, A.; Fili, S.; Georgiou, C.D.; Margiolaki, I. In Quest for Improved Drugs against Diabetes: The Added Value of X-ray Powder Diffraction Methods. Biomolecules 2017, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, S.; Cunningham, G.R.; Hayes, F.J.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Montori, V.M. Testosterone therapy in men with androgen deficiency syndromes: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2010, 95, 2536–2559. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.P.; Hirsch, M.S.; Moeny, D.; Kaul, S.; Mohamoud, M.; Joffe, H.V. Testosterone and “Age-Related Hypogonadism”–FDA Concerns. N. Engl. J. Med. 2015, 373, 689–691. [Google Scholar] [CrossRef] [PubMed]
- Glaser, R.; Dimitrakakis, C. Testosterone therapy in women: Myths and misconceptions. Maturitas 2013, 74, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Schnabel, R.B.; Appelbaum, S.; Ojeda, F.; Berisha, F.; Schulte-Steinberg, B.; Brueckmann, B.E.; Kuulasmaa, K.; Jousilahti, P.; Blankenberg, S.; et al. Low testosterone levels are predictive for incident atrial fibrillation and ischaemic stroke in men, but protective in women–results from the FINRISK study. Eur. J. Prev. Cardiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.M.; Caprio, M.; Strollo, F.; Moretti, C.; Frajese, G.; Isidori, A.; Fabbri, A. Leptin and androgens in male obesity: Evidence for leptin contribution to reduced androgen levels. J. Clin. Endocrinol. Metab. 1999, 84, 3673–3680. [Google Scholar] [CrossRef] [PubMed]
- Caprio, M.; Isidori, A.M.; Carta, A.R.; Moretti, C.; Dufau, M.L.; Fabbri, A. Expression of functional leptin receptors in rodent Leydig cells. Endocrinology 1999, 140, 4939–4947. [Google Scholar] [CrossRef] [PubMed]
- Tremellen, K. Gut Endotoxin Leading to a Decline in Gonadal function (GELDING)—A novel theory for the development of late onset hypogonadism in obese men. Basic Clin. Androl. 2016, 26. [Google Scholar] [CrossRef] [PubMed]
- Lakshman, K.M.; Bhasin, S.; Araujo, A.B. Sex hormone-binding globulin as an independent predictor of incident type 2 diabetes mellitus in men. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 503–509. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Men | Women | |
|---|---|---|
| n | 3810 | 3896 |
| Age (years) | 49.0 (37.5; 60.6) | 47.0 (36.4; 57.5) |
| BMI (kg/m²) | 26.5 (24.2; 29.0) | 25.4 (22.7; 28.8) |
| Waist-hip-ratio | 0.93 (0.88; 0.97) | 0.79 (0.75; 0.84) |
| Current smoker (%) | 26.5 | 17.5 |
| Hypertension medication (%) | 16.9 | 13.8 |
| HDL-C (mmol/L) | 1.23 (1.04; 1.43) | 1.51 (1.28; 1.75) |
| Total-Cholesterol (mmol/L) | 5.4 (4.8; 6.2) | 5.4 (4.7; 6.1) |
| Systolic blood pressure (mmHg) | 137 (126; 151) | 129 (117; 145) |
| Testosterone (nmol/L) | 17.12 (12.91; 22.02) | 1.15 (0.87; 1.56) |
| Clinical Variable | Men | Women |
|---|---|---|
| Time of day of the blood draw | −0.11 <0.001 | −0.03 <0.001 |
| Age (crude analysis) | 0.02 0.19 | 0.04 0.012 |
| Smoking | 0.09 <0.001 | −0.01 0.69 |
| Total cholesterol | 0.009 0.98 | −0.01 0.43 |
| HDL-C | 0.21 <0.001 | −0.03 0.052 |
| Systolic Blood Pressure | −0.04 0.025 | 0.04 0.046 |
| eGFR | 0.009 0.96 | −0.05 0.007 |
| BMI | −0.23 <0.001 | 0.03 0.13 |
| WHR | −0.21 <0.001 | 0.03 0.098 |
| Quarter 1 (Highest) | Quarter 2 | Quarter 3 | Quarter 4 (Lowest) | p-Value (Highest vs. Lowest Quarter) | p-Value for Trend | |
|---|---|---|---|---|---|---|
| Men | ||||||
| Model 1 | 1 | 1.19 (0.80–1.76) | 1.93 (1.37–2.73) | 2.66 (1.91–3.72) | <0.001 | <0.001 |
| Model 2 | 1 | 0.99 (0.67–1.48) | 1.33 (0.94–1.89) | 1.56 (1.10–2.21) | 0.003 | 0.005 |
| Women | ||||||
| Model 1 | 1 | 0.66 (0.46–0.95) | 0.77 (0.55–1.08) | 0.53 (0.37–0.77) | 0.003 | 0.003 |
| Model 2 | 1 | 0.80 (0.55–1.16) | 0.98 (0.69–1.38) | 0.72 (0.49–1.05) | 0.090 | 0.200 |
| Testosterone Quarters 1–3 | Testosterone Quarter 4 (Lowest) | p-Value | |
|---|---|---|---|
| Men | |||
| Individuals <50 years developing T2DM | 70/1486 (3.5%) | 39/525 (1.9%) | 0.90 |
| Individuals 506–5 years developing T2DM | 115/879 (10.0%) | 67/278 (5.8%) | 1.00 |
| Individuals >65 years developing T2DM | 44/492 (6.9%) | 28/150 (4.3%) | 0.99 |
| Women | |||
| Individuals <50 years developing T2DM | 56/1738 (2.5%) | 9/520 (0.4%) | 0.76 |
| Individuals 506–5 years developing T2DM | 89/898 (6.8%) | 31/397 (2.4%) | 0.60 |
| Individuals >65 years developing T2DM | 45/272 (13.1%) | 6/71 (1.8%) | 0.78 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karakas, M.; Schäfer, S.; Appelbaum, S.; Ojeda, F.; Kuulasmaa, K.; Brückmann, B.; Berisha, F.; Schulte-Steinberg, B.; Jousilahti, P.; Blankenberg, S.; et al. Testosterone Levels and Type 2 Diabetes—No Correlation with Age, Differential Predictive Value in Men and Women. Biomolecules 2018, 8, 76. https://doi.org/10.3390/biom8030076
Karakas M, Schäfer S, Appelbaum S, Ojeda F, Kuulasmaa K, Brückmann B, Berisha F, Schulte-Steinberg B, Jousilahti P, Blankenberg S, et al. Testosterone Levels and Type 2 Diabetes—No Correlation with Age, Differential Predictive Value in Men and Women. Biomolecules. 2018; 8(3):76. https://doi.org/10.3390/biom8030076
Chicago/Turabian StyleKarakas, Mahir, Sarina Schäfer, Sebastian Appelbaum, Francisco Ojeda, Kari Kuulasmaa, Burkhard Brückmann, Filip Berisha, Benedikt Schulte-Steinberg, Pekka Jousilahti, Stefan Blankenberg, and et al. 2018. "Testosterone Levels and Type 2 Diabetes—No Correlation with Age, Differential Predictive Value in Men and Women" Biomolecules 8, no. 3: 76. https://doi.org/10.3390/biom8030076