
Use of Botulinum Toxin for Limb Immobilization for Rehabilitation in Rats with Experimental Stroke
 , and
, and 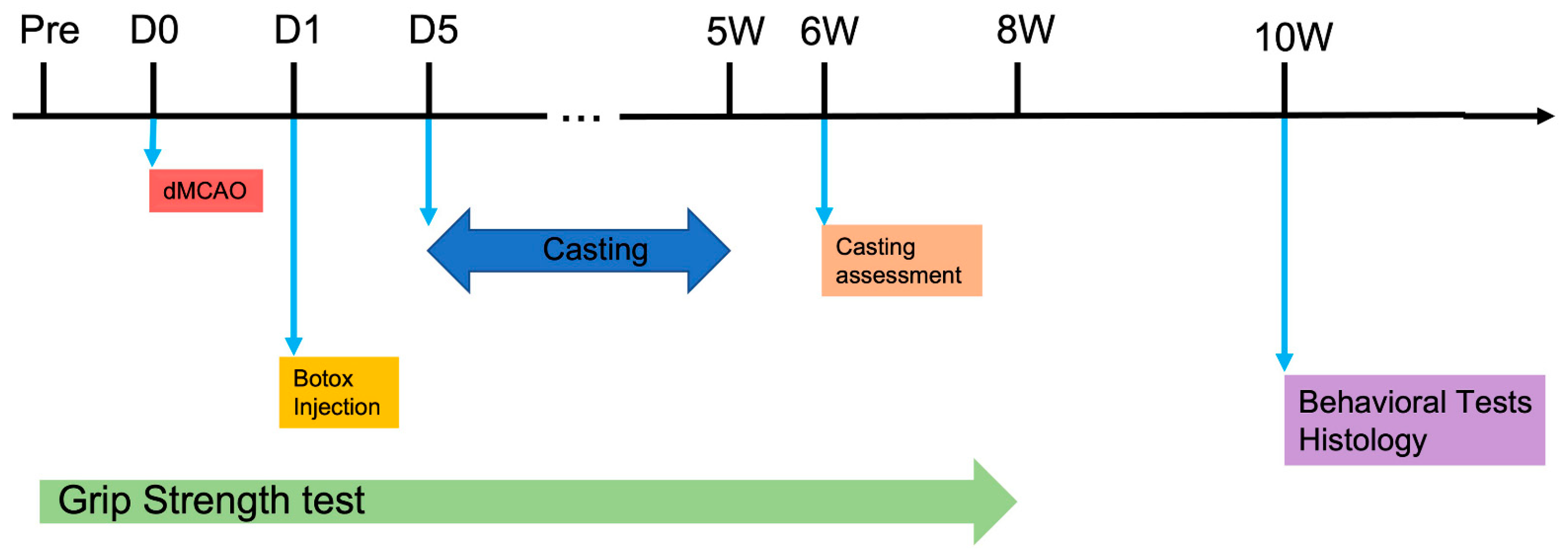{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals, Housing, and General Considerations
2.2. Induction of Distal Middle Cerebral Artery Occlusion
2.3. Casting Induced Constraint
2.4. Botox-Induced Limb Constraint
2.5. Neurobehavioral Assessment
2.5.1. Forelimb Use Asymmetry Test
2.5.2. Ladder Walk Test
2.5.3. Sticky Label Test
2.5.4. Vermicelli Handling Test
2.5.5. Computer-Assisted Method for Gait Analysis
2.6. Brain Preparation and Histological Analysis
2.7. Statistical Analysis and RIGOR
3. Results
3.1. Histological Analysis
3.2. Behavioral Outcomes
3.2.1. Limb Constraint by Casting Reversed Stroke-Induced Limb Preference
3.2.2. Botox Had a Sustained Effect on Weakening the Unaffected Forelimb
3.2.3. Effect of Limb Immobilization by Botox in Experimental Stroke
3.2.4. Botox Reduced Stroke-Induced Forelimb Asymmetry
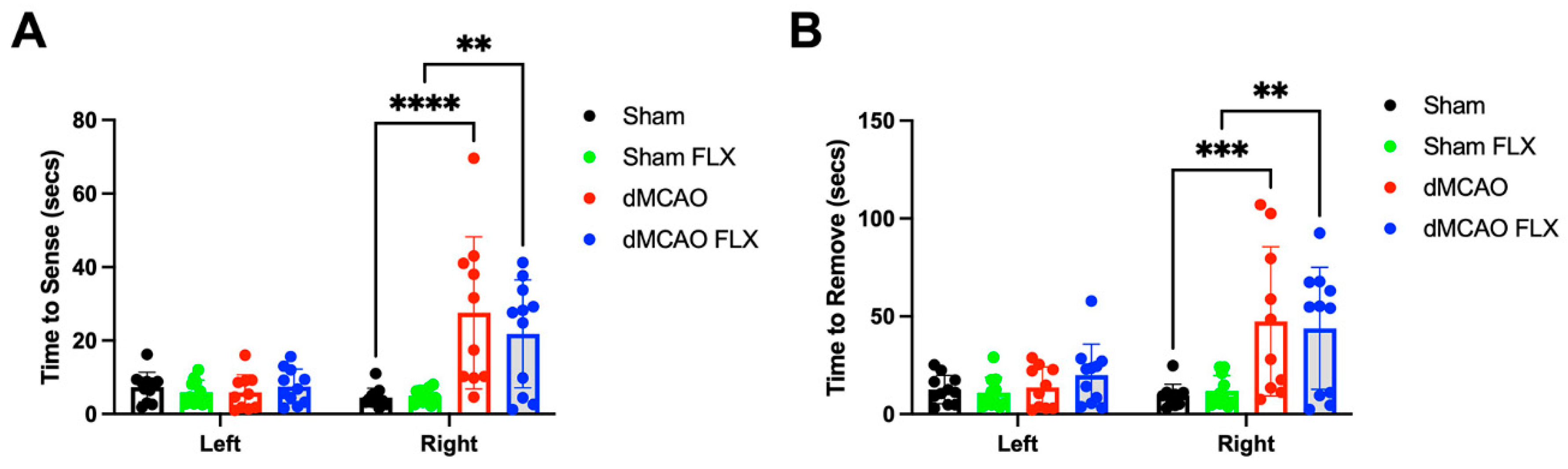
3.2.5. No Effect of Limb Immobilization by Botox and Sensorimotor Function
3.2.6. Botox Did Not Improve Post-Stroke Motor Impairment in Ladder Walking
3.2.7. Limb Immobilization by Botox and Fine Motor Skills
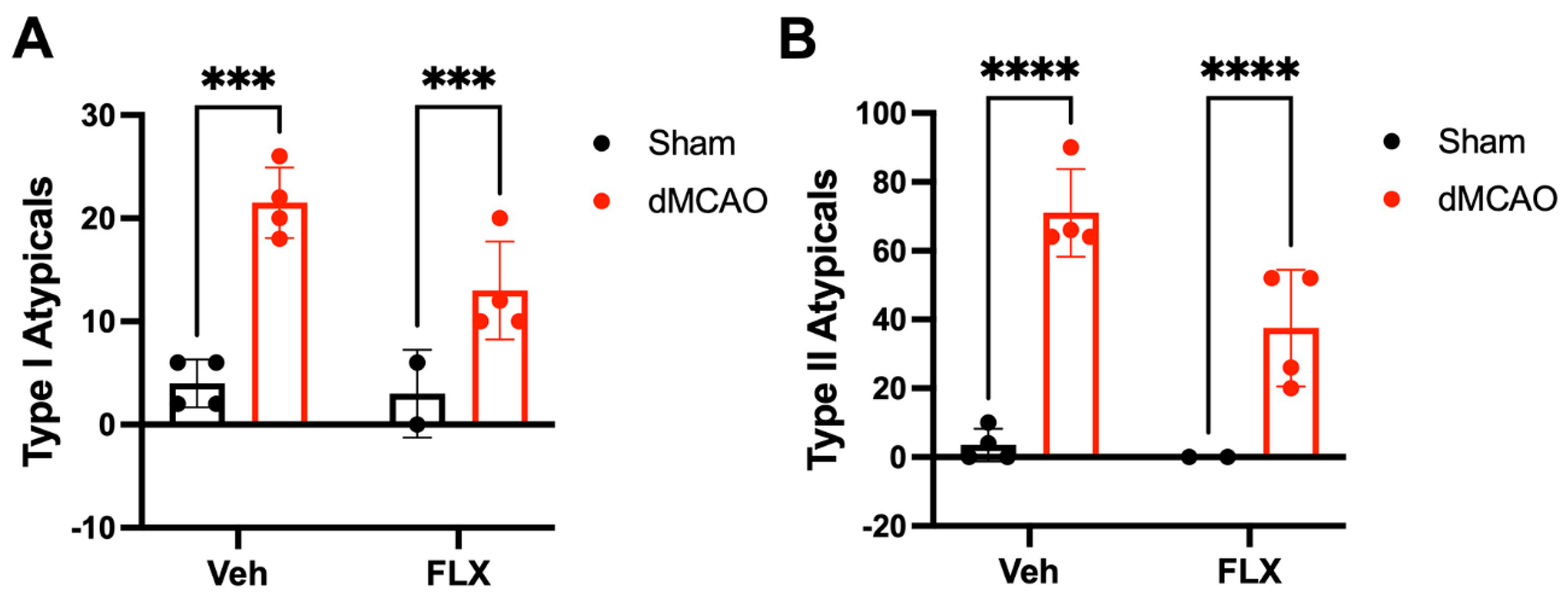
3.2.8. Stroke and Botox Both Affected the Spatial and Temporal Parameters of Paw Placement during Catwalk Test
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y. Heart disease and stroke statistics-2022 update: A report from the American heart association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Xiang, J.; He, Y.; Yuan, M.; Dong, L.; Ye, Z.; Mao, W. The mechanism and clinical application of constraint-induced movement therapy in stroke rehabilitation. Front. Behav. Neurosci. 2022, 16, 828599. [Google Scholar] [CrossRef]
- Shaw, S.E.; Morris, D.M.; Uswatte, G.; McKay, S.; Meythaler, J.M.; Taub, E. Constraint-induced movement therapy for recovery of upper-limb function following traumatic brain injury. J. Rehabil. Res. Dev. 2005, 42, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The excite randomized clinical trial. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Beretta, E.; Piccinini, L.; Turconi, A.C.; Locatelli, F.; Galli, M.; Strazzer, S. Constraint-induced movement therapy for children with hemiplegia after traumatic brain injury: A quantitative study. J. Head Trauma Rehabil. 2012, 27, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Hart, E.; Humanitzki, E.; Schroeder, J.; Woodbury, M.; Coker-Bolt, P.; Dodds, C. Neuromotor rehabilitation interventions after pediatric stroke: A focused review. Semin. Pediatr. Neurol. 2022, 44, 100994. [Google Scholar] [CrossRef]
- Janssen, H.; Speare, S.; Spratt, N.J.; Sena, E.S.; Ada, L.; Hannan, A.J.; McElduff, P.; Bernhardt, J. Exploring the efficacy of constraint in animal models of stroke: Meta-analysis and systematic review of the current evidence. Neurorehabil. Neural Repair. 2013, 27, 3–12. [Google Scholar] [CrossRef]
- Simpson, D.M.; Alexander, D.N.; O’Brien, C.F.; Tagliati, M.; Aswad, A.S.; Leon, J.M.; Gibson, J.; Mordaunt, J.M.; Monaghan, E.P. Botulinum toxin type A in the treatment of upper extremity spasticity: A randomized, double-blind, placebo-controlled trial. Neurology 1996, 46, 1306–1310. [Google Scholar] [CrossRef]
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, V.D.; Marciniak, C.; Do, M.; Lee, C.-H.; Jenkins, S.; Turkel, C. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after a stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef]
- Guettard, E.; Roze, E.; Abada, G.; Lemesle, C.; Vidailhet, M.; Laurent-Vannier, A.; Chevignard, M.P. Management of spasticity and dystonia in children with acquired brain injury with rehabilitation and botulinum toxin A. Dev. Neurorehabil. 2009, 12, 128–138. [Google Scholar] [CrossRef]
- van Kuijk, A.A.; Geurts, A.C.; Bevaart, B.J.; van Limbeek, J. Treatment of upper extremity spasticity in stroke patients by focal neuronal or neuromuscular blockade: A systematic review of the literature. Database Abstr. Rev. Eff. Qual.-Assess. Rev. 2002, 34, 51–61. [Google Scholar]
- McElhinny, E.R.; Reich, I.; Burt, B.; Mancini, R.; Wladis, E.J.; Durairaj, V.D.; Shinder, R. Treatment of pseudoptosis secondary to aberrant regeneration of the facial nerve with botulinum toxin type A. Ophthalmic Plast. Reconstr. Surg. 2013, 29, 175–178. [Google Scholar] [CrossRef]
- Fitoussi, F.; Diop, A.; Maurel, N.; El, M.L.; Ilharreborde, B.; Pennecot, G.F. Upper limb motion analysis in children with hemiplegic cerebral palsy: Proximal kinematic changes after distal botulinum toxin or surgical treatments. J. Child. Orthop. 2011, 5, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasb, M.; Shah, S.Z.A.; Chen, H.; Youssef, A.S.; Li, Z.; Dayoub, L.; Noufal, A.; Allam, A.E.S.; Hassanien, M.; Oumri, A.A.E. Constraint-induced movement therapy combined with botulinum toxin for post-stroke spasticity: A systematic review and meta-analysis. Cureus 2021, 13, e17645. [Google Scholar] [CrossRef] [PubMed]
- Kawabori, M.; Hokari, M.; Zheng, Z.; Kim, J.Y.; Calosing, C.; Hsieh, C.L.; Nakamura, M.C.; Yenari, M.A. Triggering receptor expressed on myeloid cells-2 correlates to hypothermic neuroprotection in ischemic stroke. Ther. Hypothermia Temp. Manag. 2013, 3, 189–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, H.D.; Hanumanthiah, K.M.; Diederich, K.; Schwab, S.; Schabitz, W.R.; Sommer, C. Brain-derived neurotrophic factor but not forced arm use improves long-term outcome after photothrombotic stroke and transiently upregulates binding densities of excitatory glutamate receptors in the rat brain. Stroke 2008, 39, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.I.; Bingham, D.; Chang, T.J.; Lee, C.C.; Shi, J.; Wang, D.; Massa, S.; Swanson, R.A.; Liu, J. Beneficial effects of minocycline and botulinum toxin-induced constraint physical therapy following experimental traumatic brain injury. Neurorehabil. Neural Repair 2013, 27, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Schallert, T.; Fleming, S.M.; Leasure, J.L.; Tillerson, J.L.; Bland, S.T. Cns plasticity and assessment of forelimb sensorimotor outcome in unilateral rat models of stroke, cortical ablation, parkinsonism and spinal cord injury. Neuropharmacology 2000, 39, 777–787. [Google Scholar] [CrossRef]
- Metz, G.A.; Whishaw, I.Q. Cortical and subcortical lesions impair skilled walking in the ladder rung walking test: A new task to evaluate fore- and hindlimb stepping, placing, and co-ordination. J. Neurosci. Methods 2002, 115, 169–179. [Google Scholar] [CrossRef]
- Schallert, T.; Whishaw, I.Q. Bilateral cutaneous stimulation of the somatosensory system in hemidecorticate rats. Behav. Neurosci. 1984, 98, 518–540. [Google Scholar] [CrossRef]
- Allred, R.P.; Adkins, D.L.; Woodlee, M.T.; Husbands, L.C.; Maldonado, M.A.; Kane, J.R.; Schallert, T.; Jones, T.A. The vermicelli handling test: A simple quantitative measure of dexterous forepaw function in rats. J. Neurosci. Methods 2008, 170, 229–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- d’Avila, J.C.; Lam, T.I.; Bingham, D.; Shi, J.; Won, S.J.; Kauppinen, T.M.; Massa, S.; Liu, J.; Swanson, R.A. Microglial activation induced by brain trauma is suppressed by post-injury treatment with a parp inhibitor. J. Neuroinflammation 2012, 9, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, M.; Wang, Y.; Kim, S.; Hong, S.M.; Jeng, L.; Bilgen, M.; Liu, J. Assessing gait impairment following experimental traumatic brain injury in mice. J. Neurosci. Methods. 2009, 176, 34–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Bontempi, B.; Hong, S.M.; Mehta, K.; Weinstein, P.R.; Abrams, G.M.; Liu, J. A comprehensive analysis of gait impairment after experimental stroke and the therapeutic effect of environmental enrichment in rats. J. Cereb. Blood Flow Metab. 2008, 28, 1936–1950. [Google Scholar] [CrossRef] [Green Version]
- He, J.-W.; Rabiller, G.; Nishijima, Y.; Akamatsu, Y.; Khateeb, K.; Yazdan-Shahmorad, A.; Liu, J. Experimental cortical stroke induces aberrant increase of sharp-wave-associated ripples in the hippocampus and disrupts cortico-hippocampal communication. J. Cereb. Blood Flow Metab. 2020, 40, 1778–1796. [Google Scholar] [CrossRef]
- Reddy, R.S.; Gular, K.; Dixit, S.; Kandakurti, P.K.; Tedla, J.S.; Gautam, A.P.; Sangadala, D.R. Impact of constraint-induced movement therapy (cimt) on functional ambulation in stroke patients-a systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2022, 19, 12809. [Google Scholar] [CrossRef] [PubMed]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Liu, J.; Bingham, D.; Orr, A.; Kawabori, M.; Kim, J.Y.; Zheng, Z.; Lam, T.I.; Massa, S.M.; Swanson, R.A.; et al. Use of Botulinum Toxin for Limb Immobilization for Rehabilitation in Rats with Experimental Stroke. Biomolecules 2023, 13, 512. https://doi.org/10.3390/biom13030512
Zhang H, Liu J, Bingham D, Orr A, Kawabori M, Kim JY, Zheng Z, Lam TI, Massa SM, Swanson RA, et al. Use of Botulinum Toxin for Limb Immobilization for Rehabilitation in Rats with Experimental Stroke. Biomolecules. 2023; 13(3):512. https://doi.org/10.3390/biom13030512
Chicago/Turabian StyleZhang, Hongxia, Jialing Liu, Deborah Bingham, Adrienne Orr, Masahito Kawabori, Jong Youl Kim, Zhen Zheng, Tina I. Lam, Stephen M. Massa, Raymond A. Swanson, and et al. 2023. "Use of Botulinum Toxin for Limb Immobilization for Rehabilitation in Rats with Experimental Stroke" Biomolecules 13, no. 3: 512. https://doi.org/10.3390/biom13030512