
Pathophysiology, Therapeutic Targets, and Future Therapeutic Alternatives in COPD: Focus on the Importance of the Cholinergic System

Abstract
:1. Introduction
2. Epidemiology of COPD
3. Non-Pharmacological Management of COPD
4. Pharmacological Approaches to Stable COPD
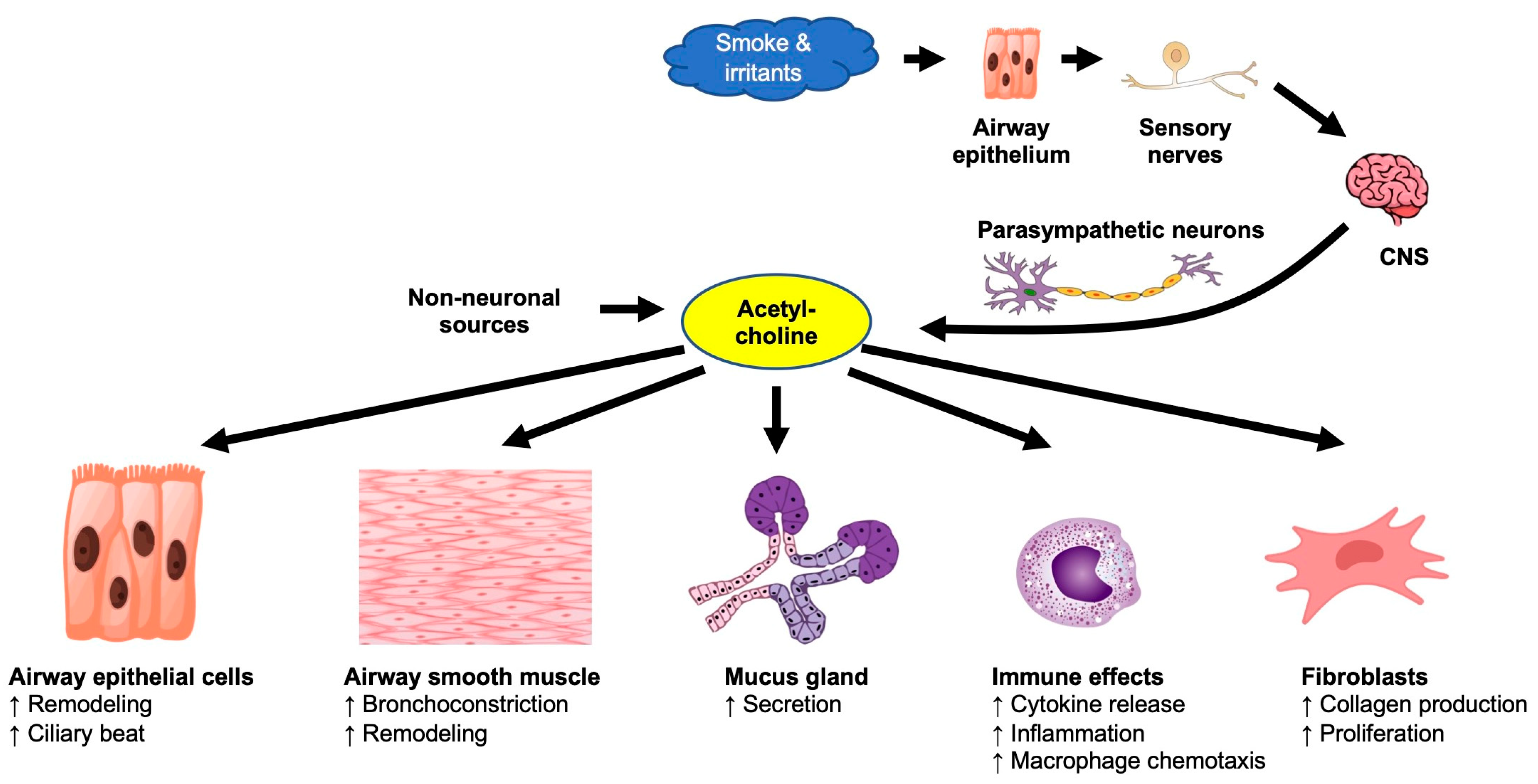
5. The Pulmonary Cholinergic System
5.1. Components of the Cholinergic System
5.2. Non-Neuronal Functions of the Pulmonary Cholinergic System
5.3. The Pathophysiological Role of the Cholinergic System in COPD
5.4. Mucus Plugs and Small Airway Dysfunction in COPD
6. Anticholinergic Medications in the Treatment of COPD
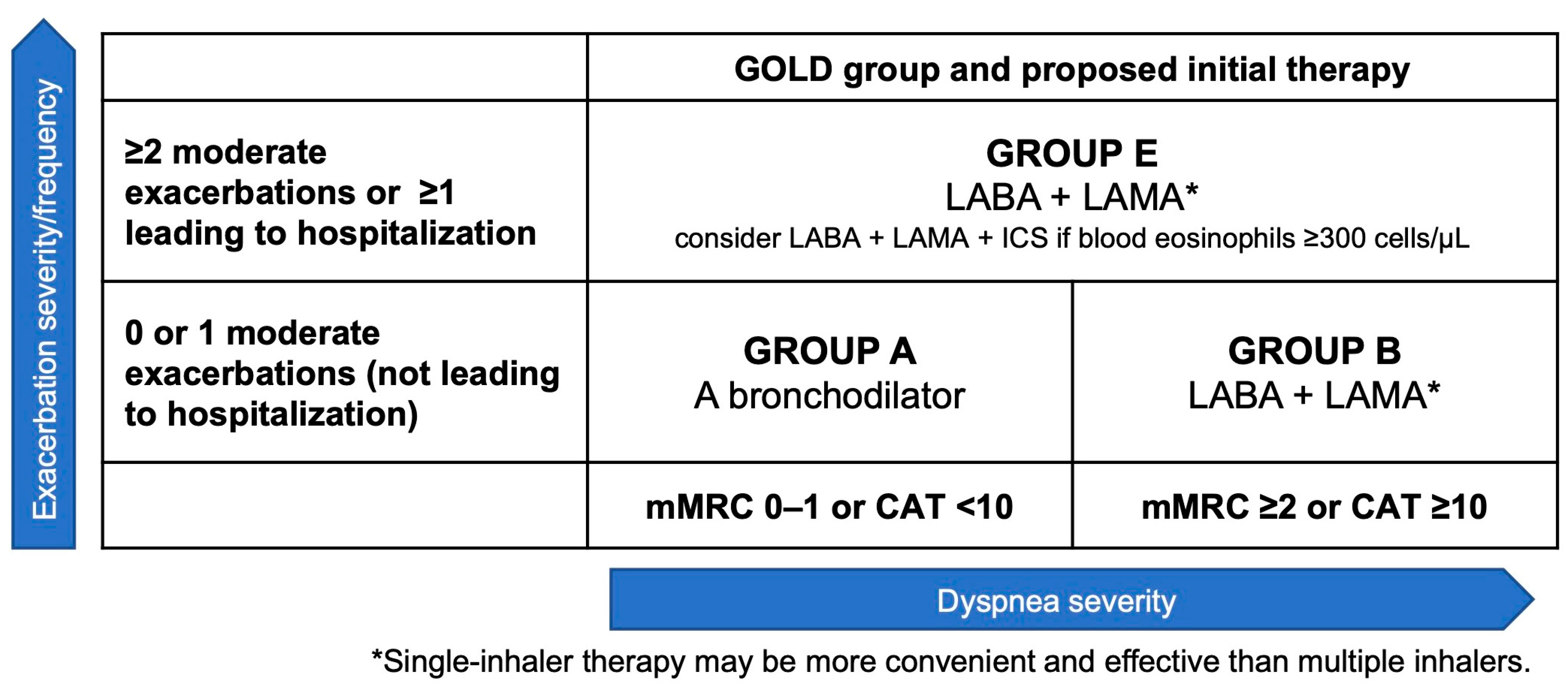
7. Management of COPD Patients with Inhaled Bronchodilators
7.1. Combination of Anticholinergic Drugs with β2 Agonists in COPD
7.2. The Addition of Inhaled Corticosteroids to Single-Bronchodilator Therapy
7.3. Triple Therapy for COPD
8. Non-Cholinergic Targets for COPD Treatment
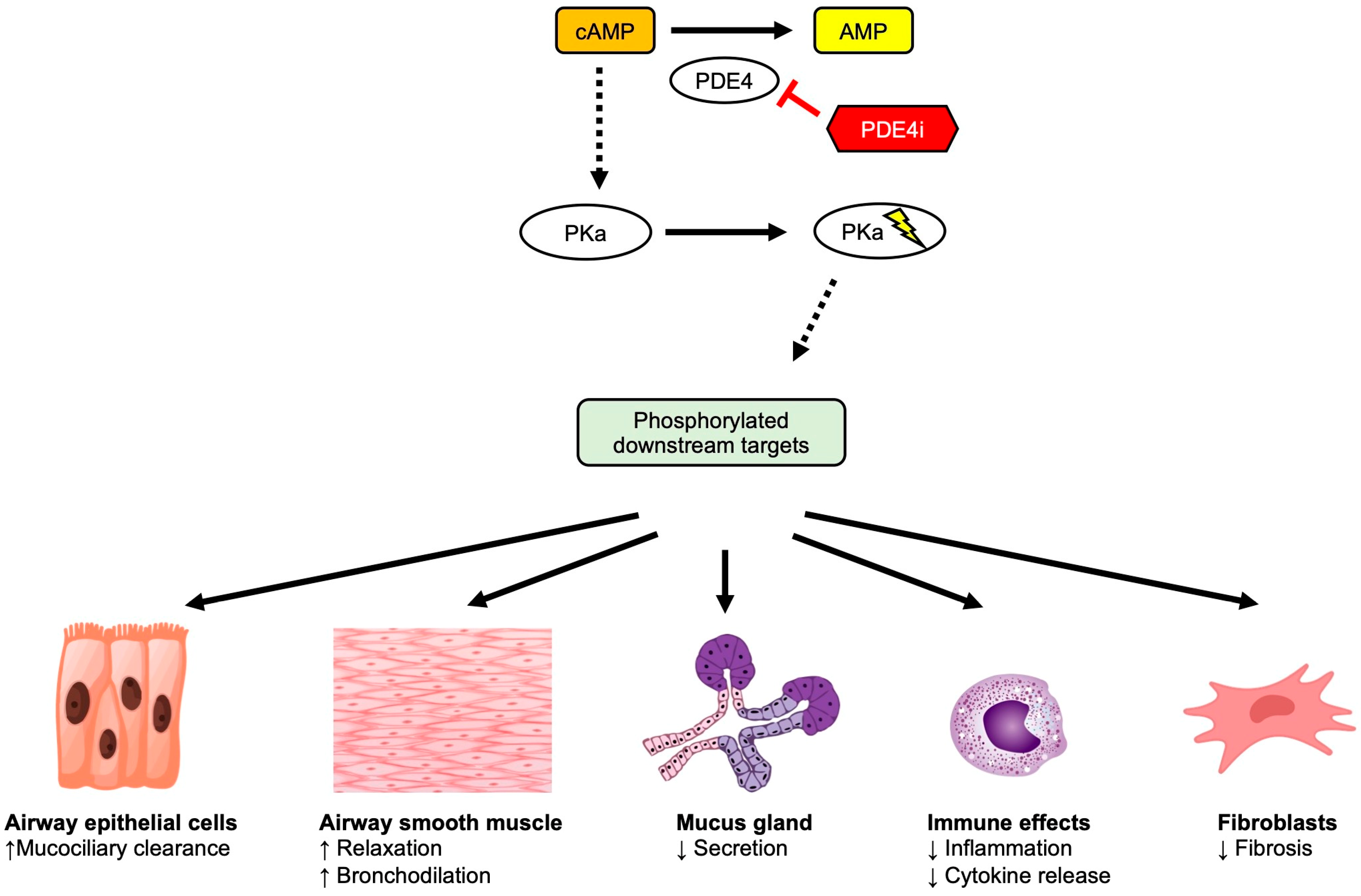
8.1. Therapies Targeting Phosphodiesterase-4 (PDE4) in COPD
8.2. Development of Novel Bronchodilators for COPD
8.3. Monoclonal Antibodies and Biologics for COPD
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 1 December 2022).
- Barnes, P.J.; Burney, P.G.; Silverman, E.K.; Celli, B.R.; Vestbo, J.; Wedzicha, J.A.; Wouters, E.F. Chronic obstructive pulmonary disease. Nat. Rev. Dis. Primers 2015, 1, 15076. [Google Scholar] [CrossRef]
- Safiri, S.; Carson-Chahhoud, K.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Ahmadian Heris, J.; Ansarin, K.; Mansournia, M.A.; Collins, G.S.; Kolahi, A.A.; et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: Results from the Global Burden of Disease Study 2019. BMJ 2022, 378, e069679. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Burney, P.; Patel, J.; Minelli, C.; Gnatiuc, L.; Amaral, A.F.S.; Kocabaş, A.; Cherkaski, H.H.; Gulsvik, A.; Nielsen, R.; Bateman, E.; et al. Prevalence and Population-Attributable Risk for Chronic Airflow Obstruction in a Large Multinational Study. Am. J. Respir. Crit. Care Med. 2021, 203, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, B.; McBurnie, M.A.; Vollmer, W.M.; Gudmundsson, G.; Welte, T.; Nizankowska-Mogilnicka, E.; Studnicka, M.; Bateman, E.; Anto, J.M.; Burney, P.; et al. COPD in never smokers: Results from the population-based burden of obstructive lung disease study. Chest 2011, 139, 752–763. [Google Scholar] [CrossRef] [Green Version]
- Mammen, J.R.; Lee, J.E. Understanding the genetics of chronic obstructive pulmonary disease, α1-antitrypsin deficiency, and implications for clinical practice. J. Am. Assoc. Nurse Pract. 2021, 33, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Dirksen, A.; Ferrarotti, I.; Koblizek, V.; Lange, P.; Mahadeva, R.; McElvaney, N.G.; Parr, D.; Piitulainen, E.; Roche, N.; et al. European Respiratory Society statement: Diagnosis and treatment of pulmonary disease in α(1)-antitrypsin deficiency. Eur. Respir. J. 2017, 50, 1700610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, L.; Lv, X.; Wang, Y.; Chu, S.; Dai, Z.; Jing, H.; Tong, Z.; Liao, X.; Liang, L. Developments in smoking cessation interventions for patients with chronic obstructive pulmonary disease in the past 5 years: A scoping review. Expert Rev. Respir. Med. 2022, 16, 749–764. [Google Scholar] [CrossRef]
- Wei, X.; Guo, K.; Shang, X.; Wang, S.; Yang, C.; Li, J.; Li, Y.; Yang, K.; Li, X.; Zhang, X. Effects of different interventions on smoking cessation in chronic obstructive pulmonary disease patients: A systematic review and network meta-analysis. Int. J. Nurs. Stud. 2022, 136, 104362. [Google Scholar] [CrossRef] [PubMed]
- Priego-Jiménez, S.; Torres-Costoso, A.; Guzmán-Pavón, M.J.; Lorenzo-García, P.; Lucerón-Lucas-Torres, M.I.; Álvarez-Bueno, C. Efficacy of Different Types of Physical Activity Interventions on Exercise Capacity in Patients with Chronic Obstructive Pulmonary Disease (COPD): A Network Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 14539. [Google Scholar] [CrossRef]
- Cranston, J.M.; Crockett, A.J.; Moss, J.R.; Alpers, J.H. Domiciliary oxygen for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2005, 2005, CD001744. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Anderson, J.A.; Cowans, N.J.; Crim, C.; Hartley, B.F.; Martinez, F.J.; Morris, A.N.; Quasny, H.; Yates, J.; Vestbo, J.; et al. Pharmacotherapy and Lung Function Decline in Patients with Chronic Obstructive Pulmonary Disease. A Systematic Review. Am. J. Respir. Crit. Care Med. 2021, 203, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, J.; Lips, K.S. The non-neuronal cholinergic system in health and disease. Pharmacology 2013, 92, 286–302. [Google Scholar] [CrossRef] [PubMed]
- Buels, K.S.; Fryer, A.D. Muscarinic receptor antagonists: Effects on pulmonary function. Handb Exp. Pharmacol. 2012, 208, 317–341. [Google Scholar] [CrossRef] [Green Version]
- Kummer, W.; Lips, K.S.; Pfeil, U. The epithelial cholinergic system of the airways. Histochem. Cell Biol. 2008, 130, 219–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diabasana, Z.; Perotin, J.M.; Belgacemi, R.; Ancel, J.; Mulette, P.; Delepine, G.; Gosset, P.; Maskos, U.; Polette, M.; Deslée, G.; et al. Nicotinic Receptor Subunits Atlas in the Adult Human Lung. Int. J. Mol. Sci. 2020, 21, 7446. [Google Scholar] [CrossRef] [PubMed]
- Hollenhorst, M.I.; Krasteva-Christ, G. Nicotinic Acetylcholine Receptors in the Respiratory Tract. Molecules 2021, 26, 6097. [Google Scholar] [CrossRef]
- Myers, A.C. Transmission in autonomic ganglia. Respir. Physiol. 2001, 125, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.K.; Haberberger, R.V.; Hartmann, P.; Faulhammer, P.; Lips, K.S.; Krain, B.; Wess, J.; Kummer, W.; König, P. Muscarinic receptor subtypes in cilia-driven transport and airway epithelial development. Eur. Respir. J. 2009, 33, 1113–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwyer, T.M.; Szebeni, A.; Diveki, K.; Farley, J.M. Transient cholinergic glycoconjugate secretion from swine tracheal submucosal gland cells. Am. J. Physiol. 1992, 262, L418–L426. [Google Scholar] [CrossRef]
- Kolahian, S.; Gosens, R. Cholinergic regulation of airway inflammation and remodelling. J. Allergy 2012, 2012, 681258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, E.; Koyama, S.; Okubo, Y.; Kubo, K.; Sekiguchi, M. Acetylcholine stimulates alveolar macrophages to release inflammatory cell chemotactic activity. Am. J. Physiol. 1998, 274, L970–L979. [Google Scholar] [CrossRef]
- Blanchet, M.R.; Israël-Assayag, E.; Daleau, P.; Beaulieu, M.J.; Cormier, Y. Dimethyphenylpiperazinium, a nicotinic receptor agonist, downregulates inflammation in monocytes/macrophages through PI3K and PLC chronic activation. Am. J. Physiol. Lung Cell Mol. Physiol. 2006, 291, L757–L763. [Google Scholar] [CrossRef] [Green Version]
- Kistemaker, L.E.; Slebos, D.J.; Meurs, H.; Kerstjens, H.A.; Gosens, R. Anti-inflammatory effects of targeted lung denervation in patients with COPD. Eur. Respir. J. 2015, 46, 1489–1492. [Google Scholar] [CrossRef] [Green Version]
- Haag, S.; Matthiesen, S.; Juergens, U.R.; Racké, K. Muscarinic receptors mediate stimulation of collagen synthesis in human lung fibroblasts. Eur. Respir. J. 2008, 32, 555–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthiesen, S.; Bahulayan, A.; Kempkens, S.; Haag, S.; Fuhrmann, M.; Stichnote, C.; Juergens, U.R.; Racké, K. Muscarinic receptors mediate stimulation of human lung fibroblast proliferation. Am. J. Respir. Cell Mol. Biol. 2006, 35, 621–627. [Google Scholar] [CrossRef]
- Pieper, M.P.; Chaudhary, N.I.; Park, J.E. Acetylcholine-induced proliferation of fibroblasts and myofibroblasts in vitro is inhibited by tiotropium bromide. Life Sci. 2007, 80, 2270–2273. [Google Scholar] [CrossRef] [PubMed]
- Gosens, R.; Nelemans, S.A.; Grootte Bromhaar, M.M.; McKay, S.; Zaagsma, J.; Meurs, H. Muscarinic M3-receptors mediate cholinergic synergism of mitogenesis in airway smooth muscle. Am. J. Respir. Cell Mol. Biol. 2003, 28, 257–262. [Google Scholar] [CrossRef]
- Dunican, E.M.; Watchorn, D.C.; Fahy, J.V. Autopsy and Imaging Studies of Mucus in Asthma. Lessons Learned about Disease Mechanisms and the Role of Mucus in Airflow Obstruction. Ann. Am. Thorac. Soc. 2018, 15 (Suppl. S3), S184–S191. [Google Scholar] [CrossRef]
- Tamura, K.; Shirai, T.; Hirai, K.; Nakayasu, H.; Takahashi, S.; Kishimoto, Y.; Akamatsu, T.; Asada, K.; Kato, S. Mucus Plugs and Small Airway Dysfunction in Asthma, COPD, and Asthma-COPD Overlap. Allergy Asthma Immunol. Res. 2022, 14, 196–209. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.H.; Laiken, N. Muscarinic Receptor Agonists and Antagonists. In Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 12th ed.; Brunton, L.L., Chabner, B.A., Knollmann, B.C., Eds.; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- Appleton, S.; Jones, T.; Poole, P.; Pilotto, L.; Adams, R.; Lasserson, T.J.; Smith, B.; Muhammad, J. Ipratropium bromide versus long-acting beta-2 agonists for stable chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2006, 2006, CD006101. [Google Scholar] [CrossRef]
- Karner, C.; Chong, J.; Poole, P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2014, 2014, CD009285. [Google Scholar] [CrossRef]
- Cheyne, L.; Irvin-Sellers, M.J.; White, J. Tiotropium versus ipratropium bromide for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 2015, CD009552. [Google Scholar] [CrossRef]
- Vogelmeier, C.; Hederer, B.; Glaab, T.; Schmidt, H.; Rutten-van Mölken, M.P.; Beeh, K.M.; Rabe, K.F.; Fabbri, L.M. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N. Engl. J. Med. 2011, 364, 1093–1103. [Google Scholar] [CrossRef] [Green Version]
- Decramer, M.L.; Chapman, K.R.; Dahl, R.; Frith, P.; Devouassoux, G.; Fritscher, C.; Cameron, R.; Shoaib, M.; Lawrence, D.; Young, D.; et al. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): A randomised, blinded, parallel-group study. Lancet Respir. Med. 2013, 1, 524–533. [Google Scholar] [CrossRef]
- Karabis, A.; Lindner, L.; Mocarski, M.; Huisman, E.; Greening, A. Comparative efficacy of aclidinium versus glycopyrronium and tiotropium, as maintenance treatment of moderate to severe COPD patients: A systematic review and network meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2013, 8, 405–423. [Google Scholar] [CrossRef] [Green Version]
- Hegde, S.S.; Pulido-Rios, M.T.; Luttmann, M.A.; Foley, J.J.; Hunsberger, G.E.; Steinfeld, T.; Lee, T.; Ji, Y.; Mammen, M.M.; Jasper, J.R. Pharmacological properties of revefenacin (TD-4208), a novel, nebulized long-acting, and lung selective muscarinic antagonist, at human recombinant muscarinic receptors and in rat, guinea pig, and human isolated airway tissues. Pharmacol. Res. Perspect 2018, 6, e00400. [Google Scholar] [CrossRef] [PubMed]
- Hvisdas, C. Revefenacin, a once-daily, long-acting muscarinic antagonist, for nebulized maintenance therapy in patients with chronic obstructive pulmonary disease. Am. J. Health Syst. Pharm. 2021, 78, 1184–1194. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xie, Y.; Kwong, J.S.; Ge, L.; He, R.; Zheng, W.; Han, J.; Zhang, R.; Zhao, H.; He, Y.; et al. The Efficacy and Safety of Revefenacin for the Treatment of Chronic Obstructive Pulmonary Disease: A Systematic Review. Front. Pharmacol. 2021, 12, 667027. [Google Scholar] [CrossRef]
- Johnson, M. The beta-adrenoceptor. Am. J. Respir. Crit. Care Med. 1998, 158, S146–S153. [Google Scholar] [CrossRef] [PubMed]
- Gross, N.; Tashkin, D.; Miller, R.; Oren, J.; Coleman, W.; Linberg, S. Inhalation by nebulization of albuterol-ipratropium combination (Dey combination) is superior to either agent alone in the treatment of chronic obstructive pulmonary disease. Dey Combination Solution Study Group. Respiration 1998, 65, 354–362. [Google Scholar] [CrossRef]
- Mammen, M.J.; Pai, V.; Aaron, S.D.; Nici, L.; Alhazzani, W.; Alexander, P.E. Dual LABA/LAMA Therapy versus LABA or LAMA Monotherapy for Chronic Obstructive Pulmonary Disease. A Systematic Review and Meta-analysis in Support of the American Thoracic Society Clinical Practice Guideline. Ann. Am. Thorac. Soc. 2020, 17, 1133–1143. [Google Scholar] [CrossRef]
- Maltais, F.; de la Hoz, A.; Casaburi, R.; O’Donnell, D. Effects of Tiotropium/Olodaterol on Activity-Related Breathlessness, Exercise Endurance and Physical Activity in Patients with COPD: Narrative Review with Meta-/Pooled Analyses. Adv. Ther. 2021, 38, 835–853. [Google Scholar] [CrossRef]
- Barnes, P.J. Inhaled Corticosteroids. Pharmaceuticals 2010, 3, 514–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, I.A.; Clarke, M.S.; Sim, E.H.; Fong, K.M. Inhaled corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2012, 2012, CD002991. [Google Scholar] [CrossRef] [Green Version]
- Calverley, P.M.; Anderson, J.A.; Celli, B.; Ferguson, G.T.; Jenkins, C.; Jones, P.W.; Yates, J.C.; Vestbo, J. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N. Engl. J. Med. 2007, 356, 775–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calverley, P.; Pauwels, R.; Vestbo, J.; Jones, P.; Pride, N.; Gulsvik, A.; Anderson, J.; Maden, C. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: A randomised controlled trial. Lancet 2003, 361, 449–456. [Google Scholar] [CrossRef]
- Calverley, P.M.; Boonsawat, W.; Cseke, Z.; Zhong, N.; Peterson, S.; Olsson, H. Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur. Respir. J. 2003, 22, 912–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szafranski, W.; Cukier, A.; Ramirez, A.; Menga, G.; Sansores, R.; Nahabedian, S.; Peterson, S.; Olsson, H. Efficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary disease. Eur. Respir. J. 2003, 21, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Nannini, L.J.; Lasserson, T.J.; Poole, P. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2012, 2012, CD006829. [Google Scholar] [CrossRef]
- Rodrigo, G.J.; Price, D.; Anzueto, A.; Singh, D.; Altman, P.; Bader, G.; Patalano, F.; Fogel, R.; Kostikas, K. LABA/LAMA combinations versus LAMA monotherapy or LABA/ICS in COPD: A systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 907–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cazzola, M.; Calzetta, L.; Rogliani, P.; Puxeddu, E.; Facciolo, F.; Matera, M.G. Interaction between corticosteroids and muscarinic antagonists in human airways. Pulm. Pharmacol. Ther. 2016, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Matera, M.G.; Rogliani, P.; Cazzola, M. Muscarinic receptor antagonists for the treatment of chronic obstructive pulmonary disease. Expert Opin. Pharmacother. 2014, 15, 961–977. [Google Scholar] [CrossRef] [PubMed]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Jones, C.E.; et al. Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680. [Google Scholar] [CrossRef]
- Papi, A.; Vestbo, J.; Fabbri, L.; Corradi, M.; Prunier, H.; Cohuet, G.; Guasconi, A.; Montagna, I.; Vezzoli, S.; Petruzzelli, S.; et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): A double-blind, parallel group, randomised controlled trial. Lancet 2018, 391, 1076–1084. [Google Scholar] [CrossRef]
- Rabe, K.F.; Martinez, F.J.; Ferguson, G.T.; Wang, C.; Singh, D.; Wedzicha, J.A.; Trivedi, R.; St Rose, E.; Ballal, S.; McLaren, J.; et al. Triple Inhaled Therapy at Two Glucocorticoid Doses in Moderate-to-Very-Severe COPD. N. Engl. J. Med. 2020, 383, 35–48. [Google Scholar] [CrossRef]
- Martinez, F.J.; Rabe, K.F.; Ferguson, G.T.; Wedzicha, J.A.; Singh, D.; Wang, C.; Rossman, K.; St Rose, E.; Trivedi, R.; Ballal, S.; et al. Reduced All-Cause Mortality in the ETHOS Trial of Budesonide/Glycopyrrolate/Formoterol for Chronic Obstructive Pulmonary Disease. A Randomized, Double-Blind, Multicenter, Parallel-Group Study. Am. J. Respir. Crit. Care Med. 2021, 203, 553–564. [Google Scholar] [CrossRef]
- Vestbo, J.; Fabbri, L.; Papi, A.; Petruzzelli, S.; Scuri, M.; Guasconi, A.; Vezzoli, S.; Singh, D. Inhaled corticosteroid containing combinations and mortality in COPD. Eur. Respir. J. 2018, 52, 1801230. [Google Scholar] [CrossRef]
- Suissa, S. Perplexing mortality data from triple therapy trials in COPD. Lancet Respir. Med. 2021, 9, 684–685. [Google Scholar] [CrossRef]
- Contreras, S.; Milara, J.; Morcillo, E.; Cortijo, J. Selective Inhibition of Phosphodiesterases 4A, B, C and D Isoforms in Chronic Respiratory Diseases: Current and Future Evidences. Curr. Pharm. Des. 2017, 23, 2073–2083. [Google Scholar] [CrossRef]
- Joskova, M.; Mokry, J.; Franova, S. Respiratory Cilia as a Therapeutic Target of Phosphodiesterase Inhibitors. Front. Pharmacol. 2020, 11, 609. [Google Scholar] [CrossRef]
- Hansen, G.; Jin, S.; Umetsu, D.T.; Conti, M. Absence of muscarinic cholinergic airway responses in mice deficient in the cyclic nucleotide phosphodiesterase PDE4D. Proc. Natl. Acad. Sci. USA 2000, 97, 6751–6756. [Google Scholar] [CrossRef] [Green Version]
- Mokry, J.; Joskova, M.; Mokra, D.; Christensen, I.; Nosalova, G. Effects of selective inhibition of PDE4 and PDE7 on airway reactivity and cough in healthy and ovalbumin-sensitized guinea pigs. Adv. Exp. Med. Biol. 2013, 756, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Townsend, E.A.; Emala, C.W.S. Quercetin acutely relaxes airway smooth muscle and potentiates β-agonist-induced relaxation via dual phosphodiesterase inhibition of PLCβ and PDE4. Am. J. Physiol. Lung Cell Mol. Physiol. 2013, 305, L396–L403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calverley, P.M.; Rabe, K.F.; Goehring, U.M.; Kristiansen, S.; Fabbri, L.M.; Martinez, F.J. Roflumilast in symptomatic chronic obstructive pulmonary disease: Two randomised clinical trials. Lancet 2009, 374, 685–694. [Google Scholar] [CrossRef]
- Cilli, A.; Bal, H.; Gunen, H. Efficacy and safety profile of roflumilast in a real-world experience. J. Thorac. Dis. 2019, 11, 1100–1105. [Google Scholar] [CrossRef]
- Yu, T.; Fain, K.; Boyd, C.M.; Singh, S.; Weiss, C.O.; Li, T.; Varadhan, R.; Puhan, M.A. Benefits and harms of roflumilast in moderate to severe COPD. Thorax 2014, 69, 616–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giembycz, M.A. 4D or not 4D—The emetogenic basis of PDE4 inhibitors uncovered? Trends Pharmacol. Sci. 2002, 23, 548. [Google Scholar] [CrossRef]
- Facchinetti, F.; Civelli, M.; Singh, D.; Papi, A.; Emirova, A.; Govoni, M. Tanimilast, A Novel Inhaled Pde4 Inhibitor for the Treatment of Asthma and Chronic Obstructive Pulmonary Disease. Front. Pharmacol. 2021, 12, 740803. [Google Scholar] [CrossRef]
- Herrmann, F.E.; Hesslinger, C.; Wollin, L.; Nickolaus, P. BI 1015550 is a PDE4B Inhibitor and a Clinical Drug Candidate for the Oral Treatment of Idiopathic Pulmonary Fibrosis. Front. Pharmacol. 2022, 13, 838449. [Google Scholar] [CrossRef]
- Richeldi, L.; Azuma, A.; Cottin, V.; Hesslinger, C.; Stowasser, S.; Valenzuela, C.; Wijsenbeek, M.S.; Zoz, D.F.; Voss, F.; Maher, T.M. Trial of a Preferential Phosphodiesterase 4B Inhibitor for Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2022, 386, 2178–2187. [Google Scholar] [CrossRef]
- Cazzola, M.; Calzetta, L.; Rogliani, P.; Matera, M.G. Ensifentrine (RPL554): An investigational PDE3/4 inhibitor for the treatment of COPD. Expert Opin. Investig. Drugs 2019, 28, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Abbott-Banner, K.; Bengtsson, T.; Newman, K. The short-term bronchodilator effects of the dual phosphodiesterase 3 and 4 inhibitor RPL554 in COPD. Eur. Respir. J. 2018, 52, 1801074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verona Pharma PLC. Verona Pharma Announces Ensifentrine Meets Primary and Key Secondary Endpoints in Phase 3 ENHANCE-1 Trial for COPD. Available online: https://www.veronapharma.com/media/verona-pharma-announces-ensifentrine-meets-primary-and-key (accessed on 4 January 2023).
- Cazzola, M.; Ora, J.; Calzetta, L.; Rogliani, P.; Matera, M.G. The future of inhalation therapy in chronic obstructive pulmonary disease. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100092. [Google Scholar] [CrossRef]
- Crim, C.; Gotfried, M.; Spangenthal, S.; Watkins, M.; Emmett, A.; Crawford, C.; Baidoo, C.; Castro-Santamaria, R. A randomized, controlled, repeat-dose study of batefenterol/fluticasone furoate compared with placebo in the treatment of COPD. BMC Pulm. Med. 2020, 20, 119. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Beier, J.; Astbury, C.; Belvisi, M.G.; Da Silva, C.A.; Jauhiainen, A.; Jimenez, E.; Lei, A.; Necander, S.; Smith, J.A.; et al. The novel bronchodilator navafenterol: A phase 2a, multicentre, randomised, double-blind, placebo-controlled crossover trial in COPD. Eur. Respir. J. 2022, 59, 2100972. [Google Scholar] [CrossRef]
- Ora, J.; Coppola, A.; Cazzola, M.; Calzetta, L.; Rogliani, P. Long-Acting Muscarinic Antagonists Under Investigational to Treat Chronic Obstructive Pulmonary Disease. J. Exp. Pharmacol. 2020, 12, 559–574. [Google Scholar] [CrossRef]
- Perikleous, E.P.; Steiropoulos, P.; Nena, E.; Paraskakis, E. Biologic Therapies in Pediatric Asthma. J. Pers. Med. 2022, 12, 999. [Google Scholar] [CrossRef]
- Mayor, A.; Thibert, B.; Huille, S.; Respaud, R.; Audat, H.; Heuzé-Vourc’h, N. Inhaled antibodies: Formulations require specific development to overcome instability due to nebulization. Drug Deliv. Transl. Res. 2021, 11, 1625–1633. [Google Scholar] [CrossRef]
- Maspero, J.; Adir, Y.; Al-Ahmad, M.; Celis-Preciado, C.A.; Colodenco, F.D.; Giavina-Bianchi, P.; Lababidi, H.; Ledanois, O.; Mahoub, B.; Perng, D.W.; et al. Type 2 inflammation in asthma and other airway diseases. ERJ Open Res. 2022, 8, 00576-2021. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Ora, J.; Cavalli, F.; Rogliani, P.; Matera, M.G. An Overview of the Safety and Efficacy of Monoclonal Antibodies for the Chronic Obstructive Pulmonary Disease. Biologics 2021, 15, 363–374. [Google Scholar] [CrossRef]
- Donovan, T.; Milan, S.J.; Wang, R.; Banchoff, E.; Bradley, P.; Crossingham, I. Anti-IL-5 therapies for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2020, 12, CD013432. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, A.; Ibrahim, W.; Greening, N.J.; Brightling, C.E. T2 Biologics for Chronic Obstructive Pulmonary Disease. J. Allergy Clin. Immunol. Pract. 2019, 7, 1405–1416. [Google Scholar] [CrossRef]
- Pavord, I.D.; Chanez, P.; Criner, G.J.; Kerstjens, H.A.M.; Korn, S.; Lugogo, N.; Martinot, J.B.; Sagara, H.; Albers, F.C.; Bradford, E.S.; et al. Mepolizumab for Eosinophilic Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2017, 377, 1613–1629. [Google Scholar] [CrossRef]
- Brightling, C.E.; Bleecker, E.R.; Panettieri, R.A.J.; Bafadhel, M.; She, D.; Ward, C.K.; Xu, X.; Birrell, C.; van der Merwe, R. Benralizumab for chronic obstructive pulmonary disease and sputum eosinophilia: A randomised, double-blind, placebo-controlled, phase 2a study. Lancet Respir. Med. 2014, 2, 891–901. [Google Scholar] [CrossRef] [Green Version]
- Vatrella, A.; Fabozzi, I.; Calabrese, C.; Maselli, R.; Pelaia, G. Dupilumab: A novel treatment for asthma. J. Asthma Allergy 2014, 7, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, S.F.; Roan, F.; Bell, B.D.; Stoklasek, T.A.; Kitajima, M.; Han, H. The biology of thymic stromal lymphopoietin (TSLP). Adv. Pharmacol. 2013, 66, 129–155. [Google Scholar] [CrossRef] [Green Version]
- van der Vaart, H.; Koëter, G.H.; Postma, D.S.; Kauffman, H.F.; ten Hacken, N.H. First study of infliximab treatment in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 172, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Rennard, S.I.; Fogarty, C.; Kelsen, S.; Long, W.; Ramsdell, J.; Allison, J.; Mahler, D.; Saadeh, C.; Siler, T.; Snell, P.; et al. The safety and efficacy of infliximab in moderate to severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2007, 175, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Aaron, S.D.; Vandemheen, K.L.; Maltais, F.; Field, S.K.; Sin, D.D.; Bourbeau, J.; Marciniuk, D.D.; FitzGerald, J.M.; Nair, P.; Mallick, R. TNFα antagonists for acute exacerbations of COPD: A randomised double-blind controlled trial. Thorax 2013, 68, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Rogliani, P.; Calzetta, L.; Ora, J.; Matera, M.G. Canakinumab for the treatment of chronic obstructive pulmonary disease. Pulm. Pharmacol. Ther. 2015, 31, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Calverley, P.M.A.; Sethi, S.; Dawson, M.; Ward, C.K.; Finch, D.K.; Penney, M.; Newbold, P.; van der Merwe, R. A randomised, placebo-controlled trial of anti-interleukin-1 receptor 1 monoclonal antibody MEDI8968 in chronic obstructive pulmonary disease. Respir. Res. 2017, 18, 153. [Google Scholar] [CrossRef] [Green Version]
- Mahler, D.A.; Huang, S.; Tabrizi, M.; Bell, G.M. Efficacy and safety of a monoclonal antibody recognizing interleukin-8 in COPD: A pilot study. Chest 2004, 126, 926–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritzmann, F.; Beisswenger, C. Preclinical studies and the function of IL-17 cytokines in COPD. Ann. Anat. 2021, 237, 151729. [Google Scholar] [CrossRef] [PubMed]
- Eich, A.; Urban, V.; Jutel, M.; Vlcek, J.; Shim, J.J.; Trofimov, V.I.; Liam, C.K.; Kuo, P.H.; Hou, Y.; Xiao, J.; et al. A Randomized, Placebo-Controlled Phase 2 Trial of CNTO 6785 in Chronic Obstructive Pulmonary Disease. COPD 2017, 14, 476–483. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Drug Class | Drug(s) | Inhaler Type | Duration of Action (h) |
|---|---|---|---|
| Short-acting muscarinic antagonist (SAMA) | Ipratropium bromide | MDI | 6–8 |
| Oxitropium bromide | MDI | 7–9 | |
| Long-acting muscarinic antagonist (LAMA) | Aclidinium bromide | DPI, MDI | 12 |
| Glycopyrronium bromide | DPI | 12–24 | |
| Tiotropium | DPI, SMI, MDI | 24 | |
| Umeclidinium | DPI | 24 | |
| Glycopyrrolate | (nebulizer only) | 12 | |
| Revefenacin | (nebulizer only) | 24 | |
| Combination short-acting β2 agonist + short-acting muscarinic antagonist (SABA + SAMA) | Fenoterol/ipratropium | SMI | 6–8 |
| Salbutamol/ipratropium | SMI, MDI | 6–8 | |
| Combination long-acting β2 agonist + long-acting muscarinic antagonist (LABA + LAMA) | Formoterol/aclidinium | DPI | 12 |
| Formoterol/glycopyrronium | MDI | 12 | |
| Indacaterol/glycopyrronium | DPI | 12–24 | |
| Vilanterol/umeclidinium | DPI | 24 | |
| Olodaterol/tiotropium | DPI | 24 | |
| Combination long-acting β2 agonist + long-acting muscarinic antagonist + inhaled corticosteroid (Triple therapy) | Fluticasone/umeclidinium/ vilanterol | DPI | 24 |
| Beclometasone/formoterol/ glycopyrronium | MDI | 12 | |
| Budesonide/formoterol/ glycopyrrolate | MDI | 12 |
| Antibody | Target | Results in COPD to Date | Ongoing Studies |
|---|---|---|---|
| Mepolizumab | IL-5 | Reduced exacerbation rates in patients with high eosinophil counts [87] | MATINEE (NCT04133909) COPD-HELP (NCT04075331) |
| Benralizumab | IL-5R | Reduced exacerbation rates in patients with high eosinophil counts [88] | RESOLUTE (NCT04053634) ABRA (NCT04098718) |
| Dupilumab | IL-4 | BOREAS (NCT03930732) NOTUS (NCT04456673) | |
| Tezepelumab | TSLP | COURSE (NCT04039113) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, F.; Cheng, S.-L. Pathophysiology, Therapeutic Targets, and Future Therapeutic Alternatives in COPD: Focus on the Importance of the Cholinergic System. Biomolecules 2023, 13, 476. https://doi.org/10.3390/biom13030476
Gomes F, Cheng S-L. Pathophysiology, Therapeutic Targets, and Future Therapeutic Alternatives in COPD: Focus on the Importance of the Cholinergic System. Biomolecules. 2023; 13(3):476. https://doi.org/10.3390/biom13030476
Chicago/Turabian StyleGomes, Felisbela, and Shih-Lung Cheng. 2023. "Pathophysiology, Therapeutic Targets, and Future Therapeutic Alternatives in COPD: Focus on the Importance of the Cholinergic System" Biomolecules 13, no. 3: 476. https://doi.org/10.3390/biom13030476