
Early Use of Corticosteroids following CAR T-Cell Therapy Correlates with Reduced Risk of High-Grade CRS without Negative Impact on Neurotoxicity or Treatment Outcome

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohorts and Study Design
2.2. Patient Stratification, Adverse Event Grading and Response Assessment
2.3. Endpoints and Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
3.2. Therapy and Laboratory Values
3.3. CRS
3.4. ICANS
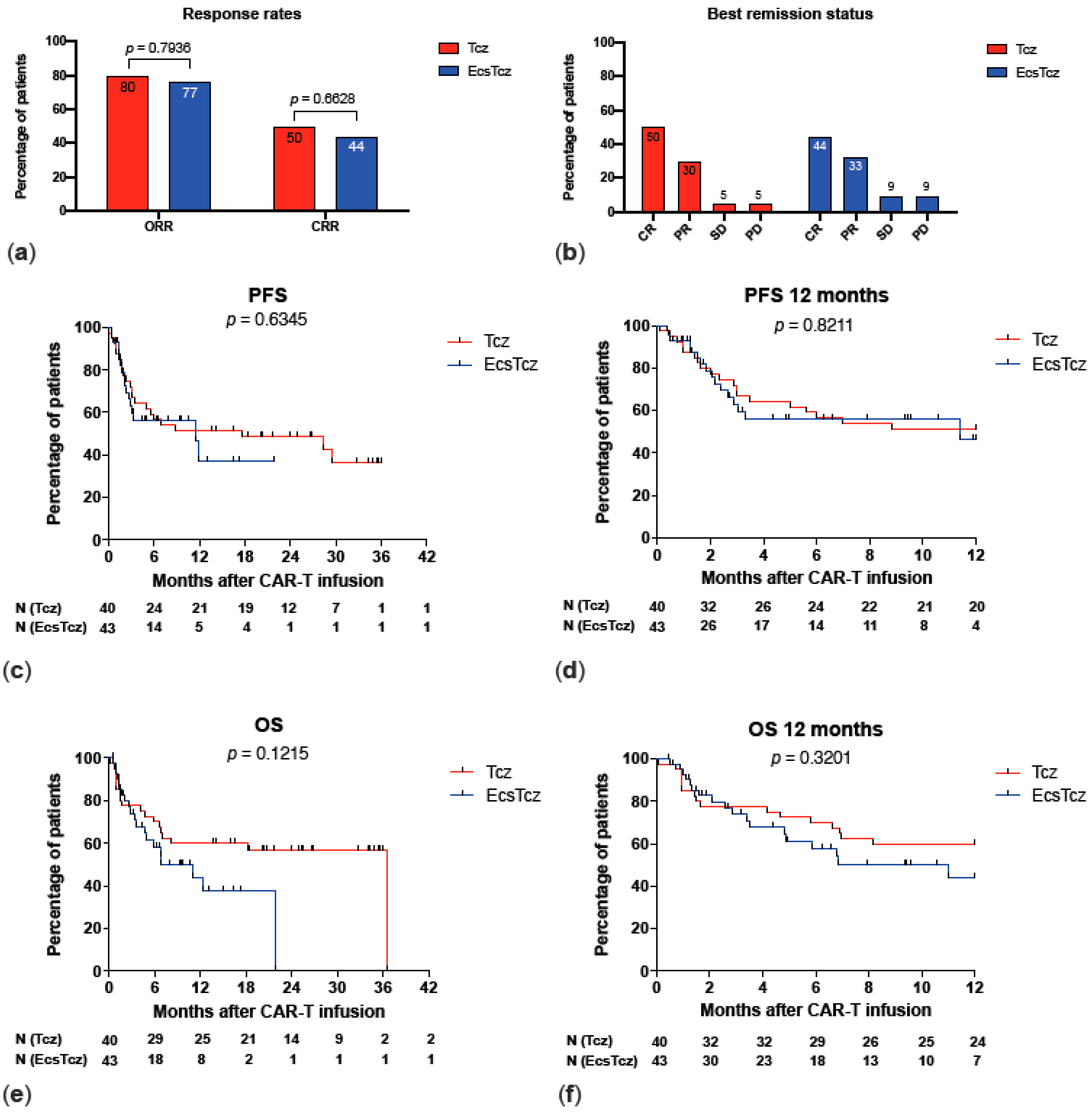
3.5. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gill, S.; Brudno, J.N. CAR T-Cell Therapy in Hematologic Malignancies: Clinical Role, Toxicity, and Unanswered Questions. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e246–e265. [Google Scholar] [CrossRef] [PubMed]
- Gagelmann, N.; Riecken, K.; Wolschke, C.; Berger, C.; Ayuk, F.A.; Fehse, B.; Kröger, N. Development of CAR-T Cell Therapies for Multiple Myeloma. Leukemia 2020, 34, 2317–2332. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Maude, S.L.; Laetsch, T.W.; Buechner, J.; Rives, S.; Boyer, M.; Bittencourt, H.; Bader, P.; Verneris, M.R.; Stefanski, H.E.; Myers, G.D.; et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N. Engl. J. Med. 2018, 378, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef]
- Wang, M.; Munoz, J.; Goy, A.; Locke, F.L.; Jacobson, C.A.; Hill, B.T.; Timmerman, J.M.; Holmes, H.; Jaglowski, S.; Flinn, I.W.; et al. KTE-X19 CAR T-Cell Therapy in Relapsed or Refractory Mantle-Cell Lymphoma. N. Engl. J. Med. 2020, 382, 1331–1342. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.D.; Bishop, M.R.; Oluwole, O.O.; Logan, A.C.; Baer, M.R.; Donnellan, W.B.; O’Dwyer, K.M.; Holmes, H.; Arellano, M.L.; Ghobadi, A.; et al. KTE-X19 Anti-CD19 CAR T-Cell Therapy in Adult Relapsed/Refractory Acute Lymphoblastic Leukemia: ZUMA-3 Phase 1 Results. Blood 2021, 138, 11–22. [Google Scholar] [CrossRef]
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene Maraleucel for Patients with Relapsed or Refractory Large B-Cell Lymphomas (TRANSCEND NHL 001): A Multicentre Seamless Design Study. Lancet 2020, 396, 839–852. [Google Scholar] [CrossRef]
- Raje, N.; Berdeja, J.; Lin, Y.; Siegel, D.; Jagannath, S.; Madduri, D.; Liedtke, M.; Rosenblatt, J.; Maus, M.V.; Turka, A.; et al. Anti-BCMA CAR T-Cell Therapy Bb2121 in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 380, 1726–1737. [Google Scholar] [CrossRef]
- Rentsch, V.; Seipel, K.; Banz, Y.; Wiedemann, G.; Porret, N.; Bacher, U.; Pabst, T. Glofitamab Treatment in Relapsed or Refractory DLBCL after CAR T-Cell Therapy. Cancers 2022, 14, 2516. [Google Scholar] [CrossRef]
- Heini, A.D.; Bacher, U.; Porret, N.; Wiedemann, G.; Legros, M.; Stalder Zeerleder, D.; Seipel, K.; Novak, U.; Daskalakis, M.; Pabst, T. Experiences with Glofitamab Administration Following CAR T Therapy in Patients with Relapsed Mantle Cell Lymphoma. Cells 2022, 11, 2747. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT Consensus Grading for Cytokine Release Syndrome and Neurologic Toxicity Associated with Immune Effector Cells. Biol. Blood Marrow Transplant. 2019, 25, 625–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimabukuro-Vornhagen, A.; Gödel, P.; Subklewe, M.; Stemmler, H.J.; Schlößer, H.A.; Schlaak, M.; Kochanek, M.; Böll, B.; Bergwelt-Baildon, M.S. von Cytokine Release Syndrome. J. Immunother. Cancer 2018, 6, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, B.D.; Jacobson, C.A. CAR T-Cell Associated Neurotoxicity: Mechanisms, Clinicopathologic Correlates, and Future Directions. JNCI J. Natl. Cancer Inst. 2019, 111, 646–654. [Google Scholar] [CrossRef]
- Santomasso, B.D.; Nastoupil, L.J.; Adkins, S.; Lacchetti, C.; Schneider, B.J.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated With Chimeric Antigen Receptor T-Cell Therapy: ASCO Guideline. J. Clin. Oncol. 2021, 39, 3978–3992. [Google Scholar] [CrossRef]
- Hayden, P.J.; Roddie, C.; Bader, P.; Basak, G.W.; Bonig, H.; Bonini, C.; Chabannon, C.; Ciceri, F.; Corbacioglu, S.; Ellard, R.; et al. Management of Adults and Children Receiving CAR T-Cell Therapy: 2021 Best Practice Recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann. Oncol. 2022, 33, 259–275. [Google Scholar] [CrossRef]
- Gardner, R.A.; Ceppi, F.; Rivers, J.; Annesley, C.; Summers, C.; Taraseviciute, A.; Gust, J.; Leger, K.J.; Tarlock, K.; Cooper, T.M.; et al. Preemptive Mitigation of CD19 CAR T-Cell Cytokine Release Syndrome without Attenuation of Antileukemic Efficacy. Blood 2019, 134, 2149–2158. [Google Scholar] [CrossRef]
- Oluwole, O.O.; Bouabdallah, K.; Muñoz, J.; De Guibert, S.; Vose, J.M.; Bartlett, N.L.; Lin, Y.; Deol, A.; McSweeney, P.A.; Goy, A.H.; et al. Prophylactic Corticosteroid Use in Patients Receiving Axicabtagene Ciloleucel for Large B-Cell Lymphoma. Br. J. Haematol. 2021, 194, 690–700. [Google Scholar] [CrossRef]
- Caimi, P.F.; Pacheco Sanchez, G.; Sharma, A.; Otegbeye, F.; Ahmed, N.; Rojas, P.; Patel, S.; Kleinsorge Block, S.; Schiavone, J.; Zamborsky, K.; et al. Prophylactic Tocilizumab Prior to Anti-CD19 CAR-T Cell Therapy for Non-Hodgkin Lymphoma. Front. Immunol. 2021, 12, 745320. [Google Scholar] [CrossRef]
- Kadauke, S.; Myers, R.M.; Li, Y.; Aplenc, R.; Baniewicz, D.; Barrett, D.M.; Barz Leahy, A.; Callahan, C.; Dolan, J.G.; Fitzgerald, J.C.; et al. Risk-Adapted Preemptive Tocilizumab to Prevent Severe Cytokine Release Syndrome After CTL019 for Pediatric B-Cell Acute Lymphoblastic Leukemia: A Prospective Clinical Trial. J. Clin. Oncol. 2021, 39, 920–930. [Google Scholar] [CrossRef]
- Nellan, A.; McCully, C.M.L.; Cruz Garcia, R.; Jayaprakash, N.; Widemann, B.C.; Lee, D.W.; Warren, K.E. Improved CNS Exposure to Tocilizumab after Cerebrospinal Fluid Compared to Intravenous Administration in Rhesus Macaques. Blood 2018, 132, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Messmer, A.S.; Que, Y.-A.; Schankin, C.; Banz, Y.; Bacher, U.; Novak, U.; Pabst, T. CAR T-Cell Therapy and Critical Care. Wien. Klin. Wochenschr. 2021, 133, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- Topp, M.S.; van Meerten, T.; Houot, R.; Minnema, M.; Milpied, N.; Lugtenburg, P.J.; Thieblemont, C.; Wermke, M.; Song, K.; Avivi, I.; et al. Earlier Steroid Use with Axicabtagene Ciloleucel (Axi-Cel) in Patients with Relapsed/Refractory Large B Cell Lymphoma (R/R LBCL). Biol. Blood Marrow Transplant. 2020, 26, S101. [Google Scholar] [CrossRef]
- Liu, S.; Deng, B.; Yin, Z.; Pan, J.; Lin, Y.; Ling, Z.; Wu, T.; Chen, D.; Chang, A.H.; Gao, Z.; et al. Corticosteroids Do Not Influence the Efficacy and Kinetics of CAR-T Cells for B-Cell Acute Lymphoblastic Leukemia. Blood Cancer J. 2020, 10, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.P.; Peters, C.W.; Quiros, C.; Wang, X.; Klomhaus, A.M.; Yamada, R.E.; Timmerman, J.M.; Moore, T.B.; Nowicki, T.S. Hypophosphatemia Due to Increased Effector Cell Metabolic Activity Is Associated with Neurotoxicity Symptoms in CD19-Targeted CAR T-Cell Therapy. Cancer Immunol. Res. 2022, 10, OF1–OF8. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Tummala, S.; Kebriaei, P.; Wierda, W.; Gutierrez, C.; Locke, F.L.; Komanduri, K.V.; Lin, Y.; Jain, N.; Daver, N.; et al. Chimeric Antigen Receptor T-Cell Therapy—Assessment and Management of Toxicities. Nat. Rev. Clin. Oncol. 2018, 15, 47–62. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Wang, X.S.; Srour, S.A.; Whisenant, M.; Subbiah, I.M.; Chen, T.H.; Ponce, D.; Gonzalez, A.G.; Kamal, M.; Mendoza, T.; Cleland, C.S.; et al. Patient-Reported Symptom and Functioning Status during the First 12 Months after Chimeric Antigen Receptor T Cell Therapy for Hematologic Malignancies. Transplant. Cell. Ther. 2021, 27, 930.e1–930.e10. [Google Scholar] [CrossRef]
- Santomasso, B.; Bachier, C.; Westin, J.; Rezvani, K.; Shpall, E.J. The Other Side of CAR T-Cell Therapy: Cytokine Release Syndrome, Neurologic Toxicity, and Financial Burden. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 433–444. [Google Scholar] [CrossRef]
- Patel, S.; Cenin, D.; Corrigan, D.; Hamilton, B.K.; Kalaycio, M.; Sobecks, R.M.; Anwer, F.; Khouri, J.; Dean, R.M.; Winter, A.; et al. Siltuximab for First-Line Treatment of Cytokine Release Syndrome: A Response to the National Shortage of Tocilizumab. Blood 2022, 140, 5073–5074. [Google Scholar] [CrossRef]
- Wehrli, M.; Gallagher, K.; Chen, Y.-B.; Leick, M.B.; McAfee, S.L.; El-Jawahri, A.R.; DeFilipp, Z.; Horick, N.; O’Donnell, P.; Spitzer, T.; et al. Single-Center Experience Using Anakinra for Steroid-Refractory Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS). J. Immunother. Cancer 2022, 10, e003847. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Deng, B.; Ling, Z.; Song, W.; Xu, J.; Duan, J.; Wang, Z.; Chang, A.H.; Feng, X.; Tan, Y. Ruxolitinib Mitigates Steroid-Refractory CRS during CAR T Therapy. J. Cell. Mol. Med. 2021, 25, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Mestermann, K.; Giavridis, T.; Weber, J.; Rydzek, J.; Frenz, S.; Nerreter, T.; Mades, A.; Sadelain, M.; Einsele, H.; Hudecek, M. The Tyrosine Kinase Inhibitor Dasatinib Acts as a Pharmacologic on/off Switch for CAR-T Cells. Sci. Transl. Med. 2019, 11, eaau5907. [Google Scholar] [CrossRef] [PubMed]
- Baur, K.; Heim, D.; Beerlage, A.; Poerings, A.S.; Kopp, B.; Medinger, M.; Dirks, J.C.; Passweg, J.R.; Holbro, A. Dasatinib for Treatment of CAR T-Cell Therapy-Related Complications. J. Immunother. Cancer 2022, 10, e005956. [Google Scholar] [CrossRef] [PubMed]
- Hao, Z.; Li, R.; Meng, L.; Han, Z.; Hong, Z. Macrophage, the Potential Key Mediator in CAR-T Related CRS. Exp. Hematol. Oncol. 2020, 9, 15. [Google Scholar] [CrossRef]
- Xiao, X.; Huang, S.; Chen, S.; Wang, Y.; Sun, Q.; Xu, X.; Li, Y. Mechanisms of Cytokine Release Syndrome and Neurotoxicity of CAR T-Cell Therapy and Associated Prevention and Management Strategies. J. Exp. Clin. Cancer Res. 2021, 40, 367. [Google Scholar] [CrossRef]
- Maus, M.V.; Alexander, S.; Bishop, M.R.; Brudno, J.N.; Callahan, C.; Davila, M.L.; Diamonte, C.; Dietrich, J.; Fitzgerald, J.C.; Frigault, M.J.; et al. Society for Immunotherapy of Cancer (SITC) Clinical Practice Guideline on Immune Effector Cell-Related Adverse Events. J. Immunother. Cancer 2020, 8, e001511. [Google Scholar] [CrossRef]
- Nydegger, A.; Novak, U.; Kronig, M.-N.; Legros, M.; Zeerleder, S.; Banz, Y.; Bacher, U.; Pabst, T. Transformed Lymphoma Is Associated with a Favorable Response to CAR-T-Cell Treatment in DLBCL Patients. Cancers 2021, 13, 6073. [Google Scholar] [CrossRef]
- Gaut, D.; Tang, K.; Sim, M.S.; Duong, T.; Young, P.; Sasine, J. Filgrastim Associations with CAR T-Cell Therapy. Int. J. Cancer 2021, 148, 1192–1196. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Reagan, P.M.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; et al. Comparison of 2-Year Outcomes with CAR T Cells (ZUMA-1) vs Salvage Chemotherapy in Refractory Large B-Cell Lymphoma. Blood Adv. 2021, 5, 4149–4155. [Google Scholar] [CrossRef]
- Pabst, T.; Joncourt, R.; Shumilov, E.; Heini, A.; Wiedemann, G.; Legros, M.; Seipel, K.; Schild, C.; Jalowiec, K.; Mansouri Taleghani, B.; et al. Analysis of IL-6 Serum Levels and CAR T Cell-Specific Digital PCR in the Context of Cytokine Release Syndrome. Exp. Hematol. 2020, 88, 7–14.e3. [Google Scholar] [CrossRef]
- Rubin, D.B.; Al Jarrah, A.; Li, K.; LaRose, S.; Monk, A.D.; Ali, A.B.; Spendley, L.N.; Nikiforow, S.; Jacobson, C.; Vaitkevicius, H. Clinical Predictors of Neurotoxicity After Chimeric Antigen Receptor T-Cell Therapy. JAMA Neurol. 2020, 77, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Berger, S.C.; Fehse, B.; Akyüz, N.; Geffken, M.; Wolschke, C.; Janson, D.; Gagelmann, N.; Luther, M.; Wichmann, D.; Frenzel, C.; et al. Molecular Monitoring of T-Cell Kinetics and Migration in Severe Neurotoxicity after Real-World CD19-Specific Chimeric Antigen Receptor-T Cell Therapy. Haematologica 2023, 108, 444–456. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Tcz | EcsTcz | p-Value |
|---|---|---|---|
| Total, n | 40 | 43 | |
| Female/male sex (ratio) | 21/19 (1.11) | 24/19 (1.26) | 0.8273 |
| Age at diagnosis, median (range) | 63 (20–76) | 59 (17–79) | 0.3957 |
| Age at CAR T-cell infusion, median (range) | 68 (25–79) | 64 (18–82) | 0.3387 |
| Diagnosis | |||
| DLBCL, n (%) | 39 (98) | 39 (91) | 0.3612 |
| Transformed DLBCL, n (%) | 17 (43) | 12 (28) | 0.1765 |
| Transformed from FL, n (%) | 13 (33) | 6 (14) | 0.0660 |
| Transformed from B-CLL/SLL, n (%) | 3 (8) | 2 (5) | 0.6685 |
| Transformed from MZL, n (%) | 1 (3) | 2 (5) | >0.9999 |
| Transformed from BL, n (%) | 0 (0) | 2 (5) | 0.4946 |
| B-ALL (%) | 1 (2) | 4 (9) | 0.3612 |
| Initial Stage (a) | |||
| I, n (%) | 1 (3) | 1 (2) | >0.9999 |
| II, n (%) | 3 (8) | 10 (23) | 0.0697 |
| III, n (%) | 7 (18) | 5 (12) | 0.5395 |
| IV, n (%) | 17 (43) | 15 (35) | 0.5063 |
| Unknown | 11 (28) | 8 (28) | |
| Treatment lines before CAR T-cell therapy | |||
| 2 lines, n (%) | 21 (53) | 28 (65) | 0.2710 |
| 3 lines, n (%) | 12 (30) | 8 (19) | 0.3054 |
| More than 3 lines, n (%) | 4 (10) | 3 (7) | 0.7063 |
| Unknown | 3 (7) | 4 (9) | |
| SCT, n (%) | 27 (68) | 16 (37) | 0.0083 |
| Autologous SCT (ASCT), n (%) | 24 (60) | 15 (35) | 0.0285 |
| Allogenic SCT, n (%) | 3 (8) | 1 (2) | 0.3481 |
| Bridging chemotherapy, n (%) | 11 (28) | 20 (47) | 0.1114 |
| Bridging radiotherapy, n (%) | 5 (13) | 11 (26) | 0.1683 |
| Remission status before CAR T-cell infusion | |||
| CR, n (%) | 1 (3) | 4 (9) | 0.3612 |
| PR, n (%) | 9 (23) | 12 (28) | 0.6207 |
| SD, n (%) | 9 (23) | 11 (26) | 0.8013 |
| PD, n (%) | 20 (50) | 16 (37) | 0.2734 |
| Unknown | 1 (1) | 0 (0) | |
| CNS involvement, n (%) | 4 (10) | 7 (16) | 0.5226 |
| LDH elevation before CAR T-cell infusion, n (%) | 9 (23) | 5 (12) | 0.2448 |
| Months from diagnosis to CAR T-cell infusion, median (range) | 61 (6–330) | 60 (6–311) | 0.9460 |
| Parameter | Tcz | EcsTcz | p-Value |
|---|---|---|---|
| Total, n | 40 | 43 | |
| CAR T-cell product | |||
| Tisagenlecleucel (Kymriah®), n (%) | 29 (73) | 29 (67) | 0.6406 |
| Axicabtagene-Ciloleucel (Yescarta®), n (%) | 11 (27) | 14 (33) | |
| Early corticosteroids, n (%) | 0 (0) | 31 (72) | <0.0001 |
| Cumulative dose in mg, median (range) | - | 40 (10–40) | |
| Tocilizumab (Actemra®), n (%) | 20 (50) | 32 (74) | 0.0253 |
| Days from CAR T-cell infusion to application of first tocilizumab dose, median (range) | 3 (0–12) | 2 (0–9) | 0.5114 |
| Number of applications, median (range) | 4 (3–6) | 4 (1–8) | 0.1017 |
| Cumulative dose in mg, median (range) | 3200 (1800–4800) | 2400 (400–4000) | 0.0054 |
| Use of filgrastim (G-CSF), n (%) | 25 (63) | 17 (100) | <0.0001 |
| Subsequent corticosteroids (a), n (%) | 12 (30) | 17 (40) | 0.4899 |
| Dose escalation of subsequent corticosteroids (b), n (%) | 3 (8) | 6 (14) | 0.4835 |
| Duration of subsequent corticosteroids, days, median (range) | 27 (1–208) | 29 (12–98) | 0.8359 |
| Cumulative dose of subsequent corticosteroids in mg, median (range) | 428 (30–1640) | 492 (150–1116) | 0.3956 |
| Application of siltuximab (Sylvant®), n (%) | 7 (18) | 5 (12) | 0.5395 |
| Peak CRP, mg/L, median (range) | 57 (3–328) | 27 (3–272) | 0.1006 |
| Days from CAR T-cell infusion to peak CRP, median (range) | 3 (0–98) | 3 (0–12) | 0.1662 |
| Peak IL-6, pg/mL, median (range) | 179 (7–157,117) | 677 (4–16,863) | 0.8615 |
| Days from CAR T-cell infusion to peak IL-6, median (range) | 4 (0–98) | 4 (1–32) | 0.6612 |
| Peak IL-1β, pg/mL, median (range) | 0 (0–74.2) | 0.5 (0–13.9) | 0.4752 |
| Days from CAR T-cell infusion to peak IL-1β, median (range) | 9 (4–21) | 5.5 (0–87) | 0.9791 |
| Peak ferritin, median (range) | 1450 (99–12,398) | 1209 (175–35,199) | 0.5234 |
| Days from CAR T-cell infusion to peak ferritin, median (range) | 8 (0–44) | 10 (0–45) | 0.5249 |
| Peak expansion of CAR T-cells, copies/μg DNA, median (range) | 4636 (54–127,942) | 3227 (37–49,166) | 0.2645 |
| Days to peak expansion of CAR-T cells, median (range) | 10 (1–37) | 9 (5–22) | 0.4157 |
| Parameter | Tcz | EcsTcz | p-Value |
|---|---|---|---|
| Total, n | 40 | 43 | |
| CRS | |||
| All grades (1–4), n (%) | 28 (70) | 39 (91) | 0.0249 |
| High-grade (3–4), n (%) | 4 (10) | 0 (0) | 0.0497 |
| Grade 1, n (%) | 13 (33) | 29 (67) | 0.0021 |
| Grade 2, n (%) | 11 (28) | 10 (23) | 0.8013 |
| Grade 3, n (%) | 3 (8) | 0 (0) | 0.1075 |
| Grade 4, n (%) | 1 (3) | 0 (0) | 0.4819 |
| Days from CAR T-cell infusion until CRS, median (range) | 3.5 (0–12) | 2 (0–13) | 0.2547 |
| Rebound CRS, n (%) | 0 (0) | 3 (7) | 0.2418 |
| ICANS | |||
| All grades (1–4), n (%) | 12 (30) | 14 (33) | 0.8177 |
| High-grade (3–4), n (%) | 8 (20) | 6 (14) | 0.5624 |
| Grade 1, n (%) | 3 (8) | 4 (9) | >0.9999 |
| Grade 2, n (%) | 1 (3) | 5 (12) | 0.2033 |
| Grade 3, n (%) | 6 (15) | 5 (12) | 0.7515 |
| Grade 4, n (%) | 2 (5) | 1 (2) | >0.9999 |
| Days from CAR T-cell infusion until ICANS, median (range) | 5.5 (1–15) | 6 (2–11) | 0.9474 |
| Rebound ICANS, n (%) | 2 (5) | 2 (5) | >0.9999 |
| CARTOX-10 score | |||
| 10, n (%) | 27 (73) | 32 (74) | >0.9999 |
| 7–9, n (%) | 1 (3) | 5 (12) | 0.2089 |
| 3–6, n (%) | 0 (0) | 2 (5) | 0.4965 |
| 1–2, n (%) | 2 (5) | 1 (2) | 0.5933 |
| 0, n (%) | 7 (19) | 3 (7) | 0.1743 |
| Days until lowest score, median (range) | 7 (1–29) | 9 (3–37) | 0.7500 |
| Days until recovery, median (range) | 2 (0–8) | 1 (0–16) | 0.9378 |
| Additional diagnostics due to ICANS, n (%) | 12 (30) | 11 (26) | 0.8067 |
| MRT, n (%) | 1 (3) | 7 (16) | 0.0586 |
| CT, n (%) | 3 (8) | 2 (5) | 0.6685 |
| MRT and CT, n (%) | 8 (20) | 4 (9) | 0.2173 |
| Abnormalities in MRT and CT, n (%) | 2 (5) | 2 (5) | >0.9999 |
| Abnormalities in EEG, n (%) | 2 (5) | 7 (16) | 0.1579 |
| ICU transfer, n (%) | 8 (20) | 5 (12) | 0.3709 |
| Days of hospitalization, median (range) | 22 (14–52) | 21 (16–46) | 0.7611 |
| CRS | ICANS | |||
|---|---|---|---|---|
| Predictors | Multivariable OR * (95% CI) | p-Value | Multivariable OR * (95% CI) | p-Value |
| Male sex | 1.92 (0.53–7.72) | 0.3285 | 0.65 (0.14–2.70) | 0.5539 |
| Age > median (61 years) | 1.74 (0.31–10.52) | 0.5428 | 10.16 (1.86–74.91) | 0.0123 |
| Transformed DLBCL | 0.71 (0.17–3.10) | 0.6237 | 0.39 (0.06–2.14) | 0.2920 |
| Initial stage at diagnosis | 0.88 (0.35–1.94) | 0.8244 | 1.57 (0.72–3.65) | 0.2621 |
| Lines of therapy before CAR T-cell therapy | 0.82 (0.41–1.55) | 0.5857 | 1.11 (0.40–2.74) | 0.8315 |
| ASCT | 1.06 (0.21–5.56) | 0.9593 | 1.84 (0.34–11.51) | 0.4872 |
| Bridging chemotherapy | 1.61 (0.41–7.19) | 0.5021 | 0.74 (0.17–2.89) | 0.6743 |
| Bridging radiotherapy | 4.88 (0.60–118.75) | 0.2092 | 0.52 (0.05–4.35) | 0.5578 |
| Remission status before CAR T-cell infusion | 1.20 (0.57–2.57) | 0.6419 | 1.47 (0.63–3.88) | 0.3940 |
| CNS involvement | 1.25 (0.17–13.95) | 0.8409 | 1.70 (0.26–11.44) | 0.5722 |
| LDH elevation before CAR T-cell infusion | 0.55 (0.09–3.00) | 0.4851 | 1.19 (0.18–7.63) | 0.8503 |
| Axicabtagene-ciloleucel vs. tisagenlecleucel | 0.41 (0.08–2.01) | 0.2716 | 1.00 (0.20–4.79) | 0.9997 |
| G-CSF application | 10.29 (1.90–73.67) | 0.0107 | 2.27 (0.27–33.14) | 0.4689 |
| Early corticosteroid application | - | - | 0.75 (0.12–4.46) | 0.7562 |
| High-grade CRS | - | - | 0.70 (0.04–13.25) | 0.8113 |
| IL-6 > median (41 mg/l) | - | - | 5.11 (0.99–33.14) | 0.0620 |
| CRP > median (44 pg/l) | - | - | 3.32 (0.81–15.83) | 0.1071 |
| Ferritin > median (1257 pg/l) | - | - | 2.80 (0.65–13.32) | 0.1736 |
| IL1-β > median (0.45 μg/mL) | - | - | 1.54 (0.27–9.19) | 0.6220 |
| Parameter | Tcz | EcsTcz | p-Value |
|---|---|---|---|
| Total, n | 40 | 43 | |
| Best response | |||
| CR, n (%) | 20 (50) | 19 (44) | 0.6628 |
| PR, n (%) | 12 (30) | 14 (33) | 0.8177 |
| SD, n (%) | 2 (5) | 4 (9) | 0.6770 |
| PD, n (%) | 2 (5) | 4 (9) | 0.6770 |
| Remission status at last follow-up | |||
| CR, n (%) | 20 (50) | 18 (42) | 0.5126 |
| PR, n (%) | 7 (18) | 8 (19) | >0.9999 |
| SD, n (%) | 0 (0) | 2 (5) | 0.4946 |
| PD, n (%) | 9 (23) | 12 (28) | 0.6207 |
| Overall response rate | 32 (80) | 33 (77) | 0.7936 |
| Complete response rate | 20 (50) | 19 (44) | 0.6628 |
| PFS | |||
| Median survival, months, curve comparison | 17.6 | 11.4 | 0.6345 |
| Median follow-up, months | 26.6 | 6.25 | |
| PFS at 12 months | |||
| Median survival, months, curve comparison | n/a | 11.41 | 0.8221 |
| Median follow-up, months | 12 | 6.25 | |
| OS | |||
| Median survival, months, curve comparison | 36.49 | 10.98 | 0.1215 |
| Median follow-up, months | 25.22 | 9.44 | |
| OS at 12 months | |||
| Median survival, months, curve comparison | n/a | 10.98 | 0.3201 |
| Median follow-up, months | 12 | 9.44 |
| PFS | OS | |||
|---|---|---|---|---|
| Predictors | Multivariable HR * (95% CI) | p-Value | Multivariable * HR (95% CI) | p-Value |
| Male sex | 3.35 (1.29–8.75) | 0.0134 | 1.39 (0.61–3.18) | 0.4290 |
| Age > median (61 years) | 0.32 (0.09–1.17) | 0.0854 | 2.50 (0.81–7.68) | 0.1102 |
| Transformed DLBCL | 1.47 (0.52–4.18) | 0.4724 | 0.37 (0.11–1.20) | 0.0972 |
| Initial disease stage at diagnosis | 0.62 (0.38–0.99) | 0.0475 | 1.11 (0.71–1.75) | 0.6385 |
| Treatment lines before CAR T-cell therapy | 1.14 (0.74–1.76) | 0.5450 | 1.17 (0.41–2.96) | 0.4406 |
| ASCT | 0.41 (0.14–1.20) | 0.1036 | 1.05 (0.42–2.64) | 0.9111 |
| Bridging chemotherapy | 2.44 (0.98–6.08) | 0.0554 | 2.06 (0.99–4.29) | 0.0526 |
| Bridging radiotherapy | 0.50 (0.16–1.62) | 0.2499 | 0.76 (0.24–2.43) | 0.6476 |
| Remission status before CAR T-cell infusion | 1.60 (0.95–2.69) | 0.0780 | 1.24 (0.72–2.13) | 0.4403 |
| CNS involvement | 0.41 (0.06–2.65) | 0.3465 | 0.87 (0.28–2.69) | 0.8147 |
| LDH elevation before CAR T-cell infusion | 0.30 (0.08–1.13) | 0.0745 | 0.86 (0.33–2.20) | 0.7490 |
| Axicabtagene-Ciloleucel vs. Tisagenlecleucel | 0.46 (0.19–1.10) | 0.0792 | 0.31 (0.12–0.77) | 0.0122 |
| G-CSF application | 5.09 (1.12–23.05) | 0.0348 | 2.04 (0.44–9.44) | 0.3621 |
| Early corticosteroid application | 0.56 (0.20–1.58) | 0.2737 | 1.29 (0.43–3.85) | 0.6531 |
| Subsequent corticosteroid application | 4.67 (0.83–26.13) | 0.0795 | 4.03 (1.08–14.99) | 0.0374 |
| CRS | 0.35 (0.08–1.42) | 0.1402 | 0.73 (0.16–3.29) | 0.6786 |
| ICANS | 0.40 (0.09–1.88) | 0.2486 | 0.60 (0.18–2.01) | 0.4122 |
| Duration of hospitalization | 1.06 (0.98–1.14) | 0.1562 | 1.02 (0.96–1.09) | 0.5199 |
| IL-6 > median (41 mg/l) | 1.79 (0.37–8.71) | 0.4700 | 1.05 (0.35–3.13) | 0.9251 |
| CRP > median (44 pg/l) | 1.73 (0.72–4.15) | 0.2199 | 1.79 (0.77–4.17) | 0.1738 |
| Ferritin > median (1257 pg/l) | 2.91 (1.03–8.17) | 0.0430 | 1.70 (0.71–4.09) | 0.2326 |
| IL1-β > median (0.45 μg/mL) | 0.67 (0.21–2.16) | 0.4978 | 1.03 (0.37–2.88) | 0.9556 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakomy, T.; Akhoundova, D.; Nilius, H.; Kronig, M.-N.; Novak, U.; Daskalakis, M.; Bacher, U.; Pabst, T. Early Use of Corticosteroids following CAR T-Cell Therapy Correlates with Reduced Risk of High-Grade CRS without Negative Impact on Neurotoxicity or Treatment Outcome. Biomolecules 2023, 13, 382. https://doi.org/10.3390/biom13020382
Lakomy T, Akhoundova D, Nilius H, Kronig M-N, Novak U, Daskalakis M, Bacher U, Pabst T. Early Use of Corticosteroids following CAR T-Cell Therapy Correlates with Reduced Risk of High-Grade CRS without Negative Impact on Neurotoxicity or Treatment Outcome. Biomolecules. 2023; 13(2):382. https://doi.org/10.3390/biom13020382
Chicago/Turabian StyleLakomy, Tim, Dilara Akhoundova, Henning Nilius, Marie-Noëlle Kronig, Urban Novak, Michael Daskalakis, Ulrike Bacher, and Thomas Pabst. 2023. "Early Use of Corticosteroids following CAR T-Cell Therapy Correlates with Reduced Risk of High-Grade CRS without Negative Impact on Neurotoxicity or Treatment Outcome" Biomolecules 13, no. 2: 382. https://doi.org/10.3390/biom13020382