
Major Adverse Cardiovascular Events and Mortality Prediction by Circulating GDF-15 in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
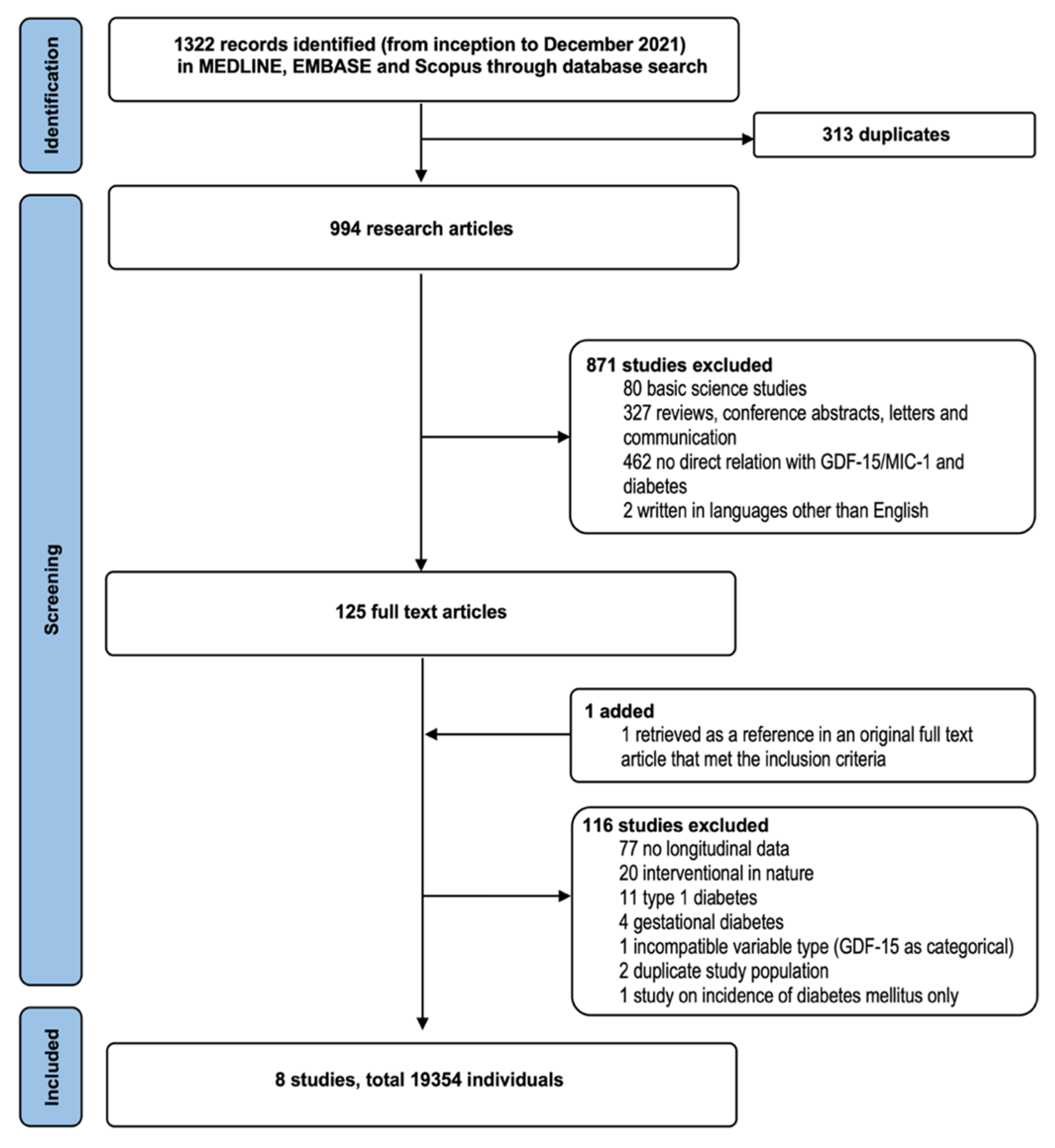
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Definition of Study Endpoints
2.4. Data Extraction
2.5. Data Harmonization and Statistical Analysis
2.6. Assessment of Publication Bias and Study Quality
3. Results
3.1. Characteristics of the Included Prospective Studies
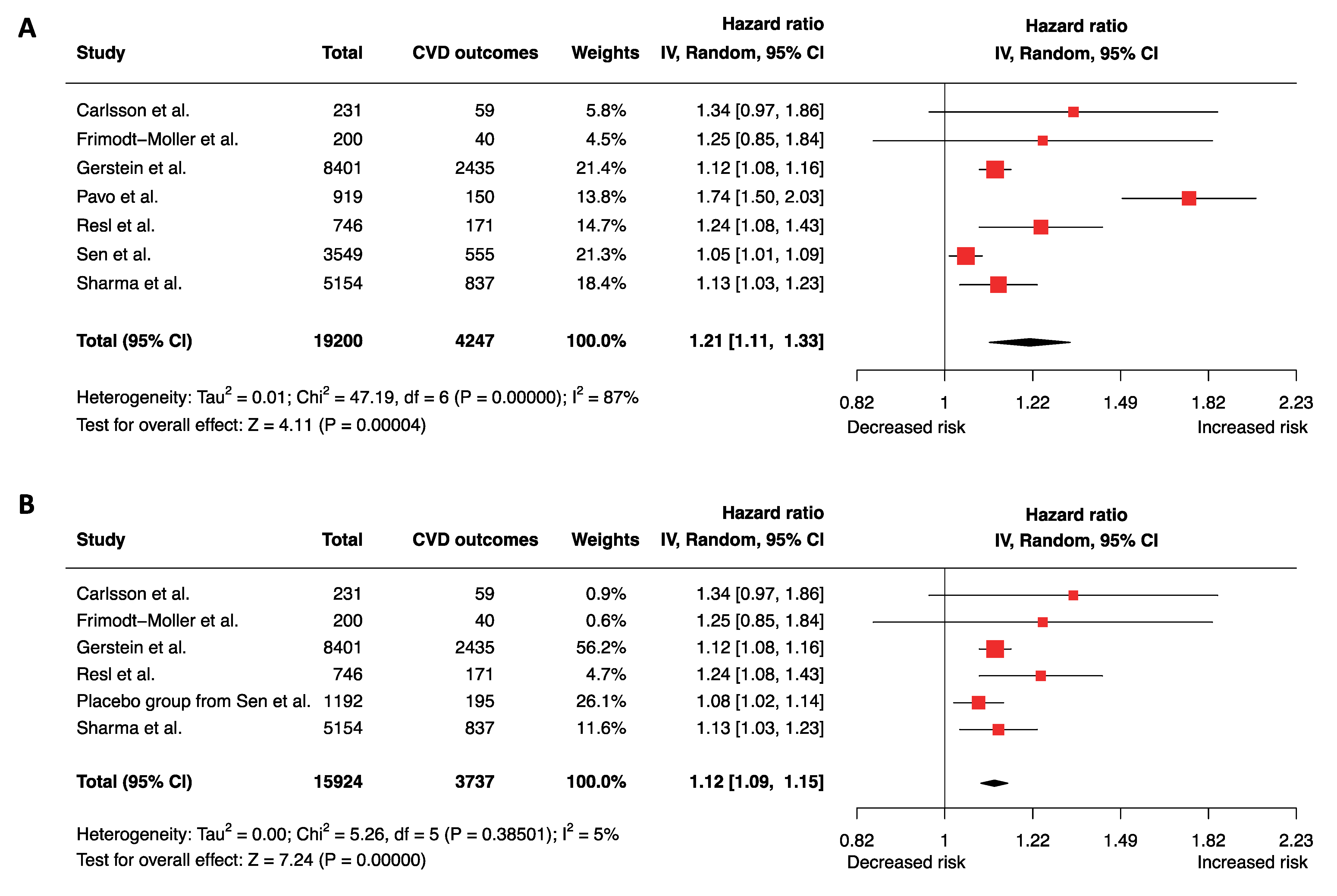
3.2. Elevated GDF-15 and Risks of Future MACE
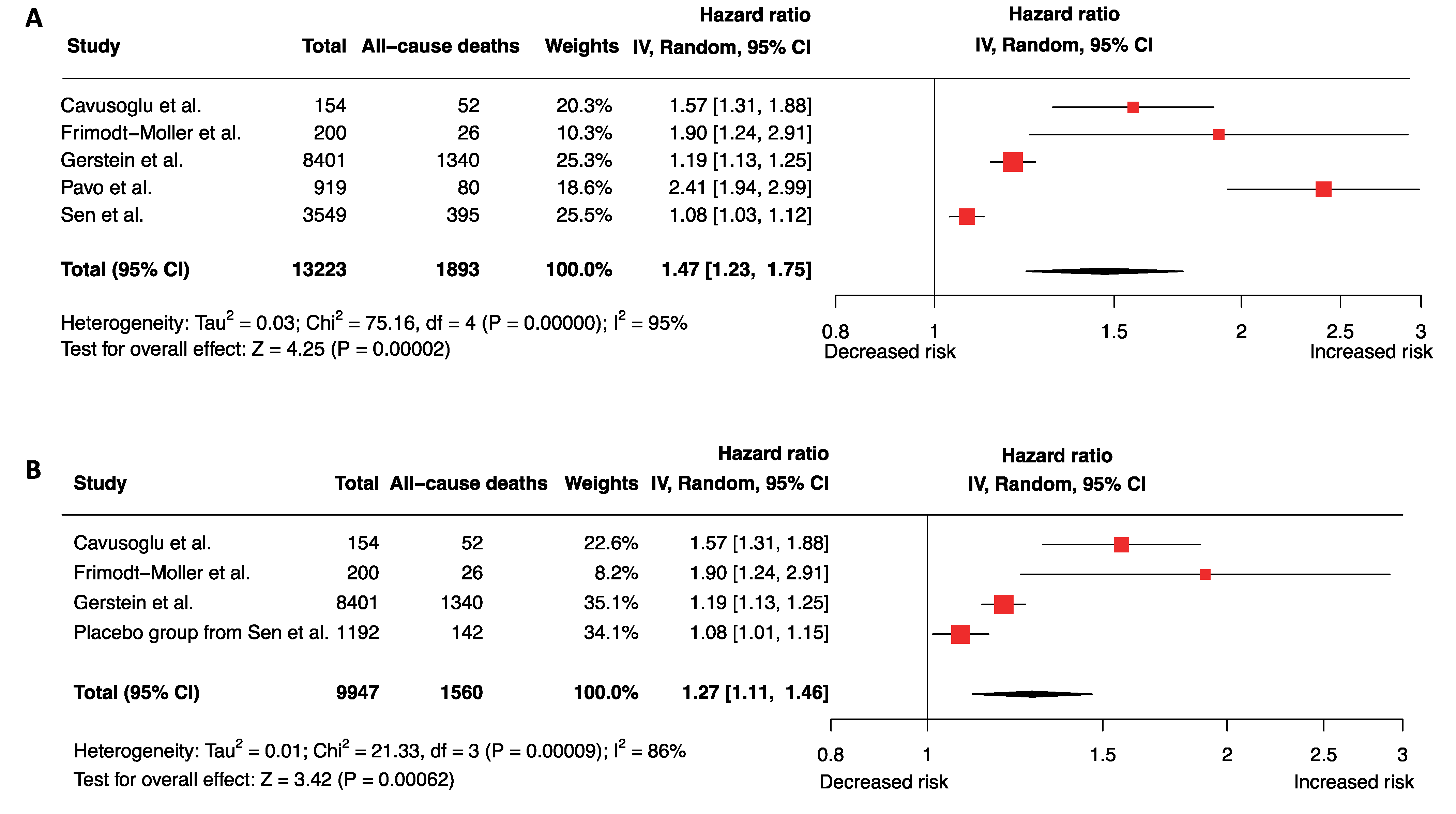
3.3. Elevated GDF-15 and Hazard of All-Cause Mortality
3.4. Ascertainment of Quality of Study and Publicaiton Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsai, V.W.W.; Husaini, Y.; Sainsbury, A.; Brown, D.A.; Breit, S.N. The MIC-1/GDF15-GFRAL Pathway in Energy Homeostasis: Implications for Obesity, Cachexia, and Other Associated Diseases. Cell Metab. 2018, 28, 353–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, V.W.; Lin, S.; Brown, D.A.; Salis, A.; Breit, S.N. Anorexia-cachexia and obesity treatment may be two sides of the same coin: Role of the TGF-b superfamily cytokine MIC-1/GDF15. Int. J. Obes. 2016, 40, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeulen, B.; Schutte, A.E.; Gafane-Matemane, L.F.; Kruger, R. Growth differentiating factor-15 and its association with traditional cardiovascular risk factors: The African-PREDICT study. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Andersson, C.; Enserro, D.; Sullivan, L.; Wang, T.J.; Januzzi, J.L., Jr.; Benjamin, E.J.; Vita, J.A.; Hamburg, N.M.; Larson, M.G.; Mitchell, G.F.; et al. Relations of circulating GDF-15, soluble ST2, and troponin-I concentrations with vascular function in the community: The Framingham Heart Study. Atherosclerosis 2016, 248, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, M.Y.; Kim, J.M.; Kang, Y.E.; Kim, M.K.; Joung, K.H.; Lee, J.H.; Kim, K.S.; Kim, H.J.; Ku, B.J.; Shong, M. Association between Growth Differentiation Factor 15 (GDF15) and Cardiovascular Risk in Patients with Newly Diagnosed Type 2 Diabetes Mellitus. J. Korean Med Sci. 2016, 31, 1413–1418. [Google Scholar] [CrossRef]
- Hong, J.H.; Choi, Y.K.; Min, B.K.; Park, K.S.; Seong, K.; Lee, I.K.; Kim, J.G. Relationship between hepcidin and GDF15 in anemic patients with type 2 diabetes without overt renal impairment. Diabetes Res. Clin. Pract. 2015, 109, 64–70. [Google Scholar] [CrossRef]
- Hagström, E.; Held, C.; Stewart, R.A.; Aylward, P.E.; Budaj, A.; Cannon, C.P.; Koenig, W.; Krug-Gourley, S.; Mohler, E.R.; Steg, P.G.; et al. Growth differentiation factor 15 predicts all-cause morbidity and mortality in stable coronary heart disease. Clin. Chem. 2017, 63, 325–333. [Google Scholar] [CrossRef]
- Fernandez, C.; Rysä, J.; Ström, K.; Nilsson, J.; Engström, G.; Orho-Melander, M.; Ruskoaho, H.; Melander, O. Circulating protein biomarkers predict incident hypertensive heart failure independently of N-terminal pro-B-type natriuretic peptide levels. ESC Heart Fail. 2020, 7, 1891–1899. [Google Scholar] [CrossRef]
- Xanthakis, V.; Enserro, D.M.; Larson, M.G.; Wollert, K.C.; Januzzi, J.L.; Levy, D.; Aragam, J.; Benjamin, E.; Cheng, S.; Wang, T.; et al. Prevalence, Neurohormonal Correlates, and Prognosis of Heart Failure Stages in the Community. JACC Heart Fail. 2016, 4, 808–815. [Google Scholar] [CrossRef]
- Xie, S.; Lu, L.; Liu, L. Growth differentiation factor-15 and the risk of cardiovascular diseases and all-cause mortality: A meta-analysis of prospective studies. Clin. Cardiol. 2019, 42, 513–523. [Google Scholar] [CrossRef]
- Zeng, X.; Li, L.; Wen, H.; Bi, Q. Growth-differentiation factor 15 as a predictor of mortality in patients with heart failure: A meta-analysis. J. Cardiovasc. Med. 2017, 18, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Dai, D.; Wang, X.; Zhu, H.; Jin, H.; Zhao, R.; Jiang, L.; Lu, Q.; Yi, F.; Wan, X.; et al. Growth differentiation factor–15 predicts the prognoses of patients with acute coronary syndrome: A meta-analysis. BMC Cardiovasc. Disord. 2016, 16, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frimodt-Møller, M.; Von Scholten, B.J.; Reinhard, H.; Jacobsen, P.K.; Hansen, T.W.; Persson, F.I.; Parving, H.; Rossing, P. Growth differentiation factor-15 and fibroblast growth factor-23 are associated with mortality in type 2 diabetes—An observational follow-up study. PLoS ONE 2018, 13, e0196634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsson, A.C.; Nowak, C.; Lind, L.; Ostgren, C.J.; Nystrom, F.H.; Sundstrom, J.; Carrero, J.J.; Riserus, U.; Ingelsson, E.; Fall, T.; et al. Growth differentiation factor 15 (GDF-15) is a potential biomarker of both diabetic kidney disease and future cardiovascular events in cohorts of individuals with type 2 diabetes: A proteomics approach. Upsala J. Med Sci. 2020, 125, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Hupfeld, C.; Mudaliar, S. Navigating the “MACE” in Cardiovascular Outcomes Trials and decoding the relevance of Atherosclerotic Cardiovascular Disease benefits versus Heart Failure benefits. Diabetes Obes. Metab. 2019, 21, 1780–1789. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Luo, D.; Wan, X.; Liu, Y.; Liu, J.; Bian, Z.; Tong, T. Detecting the skewness of data from the sample size and the five-number summary. arXiv 2020, preprint. arXiv:201005749. [Google Scholar]
- Sen, T.; Li, J.; Neuen, B.L.; Arnott, C.; Neal, B.; Perkovic, V.; Mahaffey, K.W.; Shaw, W.; Canovatchel, W.; Hansen, M.K.; et al. Association Between Circulating GDF-15 and Cardio-Renal Outcomes and Effect of Canagliflozin: Results from the CANVAS Trial. J. Am. Heart Assoc. 2021, 10, e021661. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses 2021. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 May 2022).
- Cavusoglu, E.; Marmur, J.D.; Chhabra, S.; Hojjati, M.R.; Yanamadala, S.; Chopra, V.; Eng, C.; Jiang, X.-C. Elevated baseline plasma phospholipid protein (PLTP) levels are an independent predictor of long-term all-cause mortality in patients with diabetes mellitus and known or suspected coronary artery disease. Atherosclerosis 2015, 239, 503–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstein, H.C.; Paré, G.; McQueen, M.J.; Haenel, H.; Lee, S.F.; Pogue, J.; Maggioni, A.P.; Yusuf, S.; Hess, S. Identifying Novel Biomarkers for Cardiovascular Events or Death in People with Dysglycemia. Circulation 2015, 132, 2297–2304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavo, N.; Wurm, R.; Neuhold, S.; Adlbrecht, C.; Vila, G.; Strunk, G.; Clodi, M.; Resl, M.; Brath, H.; Prager, R.; et al. GDF-15 is associated with cancer incidence in patients with type 2 diabetes. Clin. Chem. 2016, 62, 1612–1620. [Google Scholar] [CrossRef]
- Resl, M.; Clodi, M.; Vila, G.; Luger, A.; Neuhold, S.; Wurm, R.; Adlbrecht, C.; Strunk, G.; Fritzer-Szekeres, M.; Prager, R.; et al. Targeted multiple biomarker approach in predicting cardiovascular events in patients with diabetes. Heart 2016, 102, 1963–1968. [Google Scholar] [CrossRef]
- Sharma, A.; Vaduganathan, M.; Ferreira, J.P.; Liu, Y.; Bakris, G.L.; Cannon, C.P.; White, W.B.; Zannad, F. Clinical and Biomarker Predictors of Expanded Heart Failure Outcomes in Patients with Type 2 Diabetes Mellitus After a Recent Acute Coronary Syndrome: Insights from the EXAMINE Trial. J. Am. Heart Assoc. 2020, 9, e012797. [Google Scholar] [CrossRef]
- Wang, T.J.; Wollert, K.C.; Larson, M.G.; Coglianese, E.; McCabe, E.L.; Cheng, S.; Ho, J.; Fradley, M.G.; Ghorbani, A.; Xanthakis, V.; et al. Prognostic Utility of Novel Biomarkers of Cardiovascular Stress. Circulation 2012, 126, 1596–1604. [Google Scholar] [CrossRef] [Green Version]
- Mullican, S.E.; Lin-Schmidt, X.; Chin, C.N.; Chavez, J.A.; Furman, J.L.; Armstrong, A.A.; Beck, S.C.; South, V.J.; Dinh, T.Q.; Cash-Mason, T.D.; et al. GFRAL is the receptor for GDF15 and the ligand promotes weight loss in mice and nonhuman primates. Nat. Med. 2017, 23, 1150–1157. [Google Scholar] [CrossRef]
- Emmerson, P.J.; Wang, F.; Du, Y.; Liu, Q.; Pickard, R.T.; Gonciarz, M.D.; Coskun, T.; Hamang, M.J.; Sindelar, D.K.; Ballman, K.K.; et al. The metabolic effects of GDF15 are mediated by the orphan receptor GFRAL. Nat. Med. 2017, 23, 1215–1219. [Google Scholar] [CrossRef]
- Yang, L.; Chang, C.C.; Sun, Z.; Madsen, D.; Zhu, H.; Padkjær, S.B.; Wu, X.; Huang, T.; Hultman, K.; Paulsen, S.J.; et al. GFRAL is the receptor for GDF15 and is required for the anti-obesity effects of the ligand. Nat. Med. 2017, 23, 1158–1166. [Google Scholar] [CrossRef]
- Xu, J.; Kimball, T.R.; Lorenz, J.N.; Brown, D.A.; Bauskin, A.R.; Klevitsky, R.; Hewett, T.E.; Breit, S.N.; Molkentin, J.D. GDF15/MIC-1 functions as a protective and antihypertrophic factor released from the myocardium in association with SMAD protein activation. Circ. Res. 2006, 98, 342–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.Y.; Nie, Y.; Wang, F.F.; Bai, Y.; Lv, Z.Z.; Zhang, Y.Y.; Li, Z. Growth differentiation factor (GDF)-15 blocks norepinephrine-induced myocardial hypertrophy via a novel pathway involving inhibition of epidermal growth factor receptor transactivation. J. Biol. Chem. 2014, 289, 10084–10094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, V.; Zhang, H.; Manandhar, R.; Lee-Ng, K.; Lebhar, H.; Marquis, C.; Husaini, Y.; Sainsbury, A.; Brown, D.A.; Breit, S.N. Treatment with the TGF-b superfamily cytokine MIC-1/GDF15 reduces the adiposity and corrects the metabolic dysfunction of mice with diet-induced obesity. Int. J. Obes. 2018, 42, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Coll, A.P.; Chen, M.; Taskar, P.; Rimmington, D.; Patel, S.; Tadross, J.A.; Cimino, I.; Yang, M.; Welsh, P.; Virtue, S.; et al. GDF15 mediates the effects of metformin on body weight and energy balance. Nature 2020, 578, 444–448. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Pare, G.; Hess, S.; Ford, R.J.; Sjaarda, J.; Raman, K.; McQueen, M.; Lee, S.; Haenel, H.; Steinberg, G.R. Growth Differentiation Factor 15 as a Novel Biomarker for Metformin. Diabetes Care 2017, 40, 280–283. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.E.; Mahajan, A.; Chen, M.H.; Larson, M.G.; McCabe, E.L.; Ghorbani, A.; Cheng, S.; Johnson, A.D.; Lindgren, C.M.; Kempf, T.; et al. Clinical and genetic correlates of growth differentiation factor 15 in the community. Clin. Chem. 2012, 58, 1582–1591. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.; Thalamuthu, A.; Ho, J.E.; Mahajan, A.; Ek, W.E.; Brown, D.A.; Breit, S.N.; Wang, T.J.; Gyllensten, U.; Chen, M.H.; et al. A Meta-Analysis of Genome-Wide Association Studies of Growth Differentiation Factor-15 Concentration in Blood. Front. Genet. 2018, 9, 97. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Yang, F.; Ma, M.; Bao, Q.; Shen, J.; Ye, F.; Xie, X. The impact of growth differentiation factor 15 on the risk of cardiovascular diseases: Two-sample Mendelian randomization study. BMC Cardiovasc. Disord. 2020, 20, 462. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study, Year of Publication, Reference no. | Carlsson et al. 2020 [14] | Cavusoglu et al. 2015 [23] | Frimodt-Møller et al. 2018 [13] | Gerstein et al. 2015 [24] | Pavo et al. 2016 [25] | Resl et al. 2016 [26] | Sen et al. 2021 [20] | Sharma et al. 2020 [27] |
|---|---|---|---|---|---|---|---|---|
| Country | Sweden | USA | Denmark | Canada | Austria | Austria | Int’l | Int’l |
| Sample size, n | 231 | 154 | 200 | 8401 | 919 | 746 | 3549 | 5154 |
| Study type | Prospective | Prospective | Prospective | Prospective | Prospective | Prospective | Prospective | Prospective |
| Statistical adjustment (Cox) | Multivariate | Multivariate | Multivariate | Multivariate | Univariate | Multivariate | Multivariate | Multivariate |
| Median follow-up time, y | 7.9 | 5.0 | 6.1 | 6.2 | 5.0 | 5.0 | 6.1 | 1.5 |
| Age, y | 68 | – | 59 | 63.2 | 62 † | – | 62.8 | 61 † |
| Male, n (%) | 169 (73.0) | – | 152 (76.0) | 5928 (70.6) | 511 (55.6) | 420 (56.3) | 2374 (66.9) | 3491(67.7) |
| BMI, kg/m2 | 30 | – | – | – | 28.1 † | – | 32.7 † | 29.5 |
| Smoking, n (%) | 123 (15.0) | – | 59 (29.5) | 1050 (12.5) | 358 (39.0) | – | – | – |
| Hypertension, n (%) | – | – | – | 6638 (79.0) | 614 (66.9) | 508 (68.0) | – | 4291 (83.3) |
| Heart failure, n (%) | – | 46 (29.9) | – | – | 0 (0) | – | 473 (13.3) | 1442 (28.0) |
| Atrial fibrillation, n (%) | – | 7 (4.5) | – | – | 14 (1.6) | – | – | – |
| Coronary artery disease, n (%) | – | 130 (84.4) | – | – | 105 (11.5) | – | – | – |
| Myocardial infarction, n (%) | – | 54 (35.1) | – | – | – | – | 4534 (88.0) | – |
| Duration of diabetes, y | – | – | 14.7 | 5.3 † | – | 12.0† | 13.5 † | – |
| HbA1c, % | 7.0 | – | – | – | 7.1 † | – | 8.2 † | 8.0 |
| eGFR, mL/min/1.73 m² | 70.0 | – | 91.1 | – | 73.3 † | 72.7 † | 77.0 † | 70.9 |
| hsTnT †, ng/L | – | – | – | – | 8 | 0.0008 | – | 9 |
| NT-proBNP †, pg/mL | – | – | – | – | 62 | 67 | – | 422 |
| GDF-15 †, pg/mL | – | – | 1533 | – | 1391 | 1474 | 1774 | 1246 |
| Medications: | ||||||||
| Aspirin, n (%) | – | 129 (83.8) | 193 (91.5) | – | 292 (32.0) | – | – | 4683 (90.9) |
| Statin, n (%) | 415 (51.0) | 98 (63.6) | 189 (95.0) | 6638 (79.0) | 371 (40.4) | 317 (42.5) | – | 4672 (90.6) |
| ACEI/ARB, n (%) | – | 110 (71.4) | – | 5793 (69.0) | – | 408 (54.7) | – | 4247 (82.4) |
| Beta-blocker, n (%) | – | 116 (75.3) | – | 4526 (53.9) | – | 203 (27.2) | – | 4240 (82.3) |
| Any OHA, n (%) | 152 (65.8) | 104 (67.5) | 170 (85.0) | – | 484 (52.7) | – | – | – |
| Metformin, n (%) | – | 55 (35.7) | – | 2317 (27.6) | 412 (44.8) | 339 (45.4) | – | 3412 (66.2) |
| Sulfonylurea, n (%) | – | – | – | – | 226 (24.8) | 196 (26.3) | – | 2393 (46.4) |
| Insulin, n (%) | 209 (26.0) | 42 (27.3) | 124 (62.0) | – | 597 (65.0) | 508 (68.0) | – | 1540 (29.9) |
| Study (Year) | Endpoint | Definition of MACE | Adjusted Confounders | Ref. |
|---|---|---|---|---|
| Carlsson et al. (2020) | MACE |
| Age, sex, frailty, microalbuminuria, renal function, CVD at baseline, smoking, LDL, and SBP | [14] |
| All-cause death | – | – | ||
| Cavusoglu et al. (2015) | MACE | – | – | [23] |
| All-cause death | – | Age, HF or MI at presentation, extent of angiographic CAD, eGFR, metformin use, TZD use, and ST2 | ||
| Frimodt-Møller et al. (2018) | MACE |
| Age, sex, smoking status, systolic BP, LDL, HbA1c, plasma creatinine, and urinary albumin excretion rate | [13] |
| All-cause death | – | Age, sex, smoking status, systolic BP, LDL, HbA1c, plasma creatinine, and urinary albumin excretion rate | ||
| Gerstein et al. (2015) | MACE |
| Age, sex, smoking status, prior DM, HT and CV events, LDL/HDL, albuminuria, and levels of serum creatinine, NT-proBNP, chromogranin A, Ang-2, GSTA, apolipoprotein B and tissue inhibitor of metalloproteinase 1 | [24] |
| All-cause death | – | Age, sex, smoking status, prior DM, HT and CV event, LDL/HDL, albuminuria, and levels of serum creatinine, NT-proBNP, chromogranin A, Ang-2, GSTA, trefoil factor 3, α-2-macroglobulin, tenascin, selenoprotein P, macrophage derived chemokine, YKL-40 and IGF binding protein 2 | ||
| Pavo et al. (2016) | MACE |
| – | [25] |
| All-cause death | – | – | ||
| Resl et al. (2016) | MACE |
| Age, sex, and log-transformed duration of DM, BP, eGFR, LDL, total cholesterol, HbA1c, urinary albumin excretion and NT-proBNP | [26] |
| All-cause death | – | – | ||
| Sen et al. (2021) | MACE |
| Age, sex, race, and randomized treatment assignment (canagliflozin or placebo) *, history of CVD, HbA1c, systolic and diastolic BP, BMI, LDL cholesterol, eGFR and UACR | [20] |
| All-cause death | – | Age, sex, treatment assignment, UACR, eGFR, and CVD history | ||
| Sharma et al. (2020) | MACE |
| Age, sex, smoking status, systolic BP, history of HF, duration of DM, prior MI, HT, hyperlipidemia, and eGFR | [27] |
| All-cause death | – | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, S.; Li, Q.; Luk, A.O.Y.; Lan, H.-Y.; Chan, P.K.S.; Bayés-Genís, A.; Chan, F.K.L.; Fung, E. Major Adverse Cardiovascular Events and Mortality Prediction by Circulating GDF-15 in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Biomolecules 2022, 12, 934. https://doi.org/10.3390/biom12070934
Xie S, Li Q, Luk AOY, Lan H-Y, Chan PKS, Bayés-Genís A, Chan FKL, Fung E. Major Adverse Cardiovascular Events and Mortality Prediction by Circulating GDF-15 in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Biomolecules. 2022; 12(7):934. https://doi.org/10.3390/biom12070934
Chicago/Turabian StyleXie, Suyi, Qi Li, Andrea O. Y. Luk, Hui-Yao Lan, Paul K. S. Chan, Antoni Bayés-Genís, Francis K. L. Chan, and Erik Fung. 2022. "Major Adverse Cardiovascular Events and Mortality Prediction by Circulating GDF-15 in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis" Biomolecules 12, no. 7: 934. https://doi.org/10.3390/biom12070934