
Are Cell-Based Therapies Safe and Effective in the Treatment of Neurodegenerative Diseases? A Systematic Review with Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. In- and Exclusion Criteria
2.3. Outcome Measures
2.4. Selection Process and Data Extraction
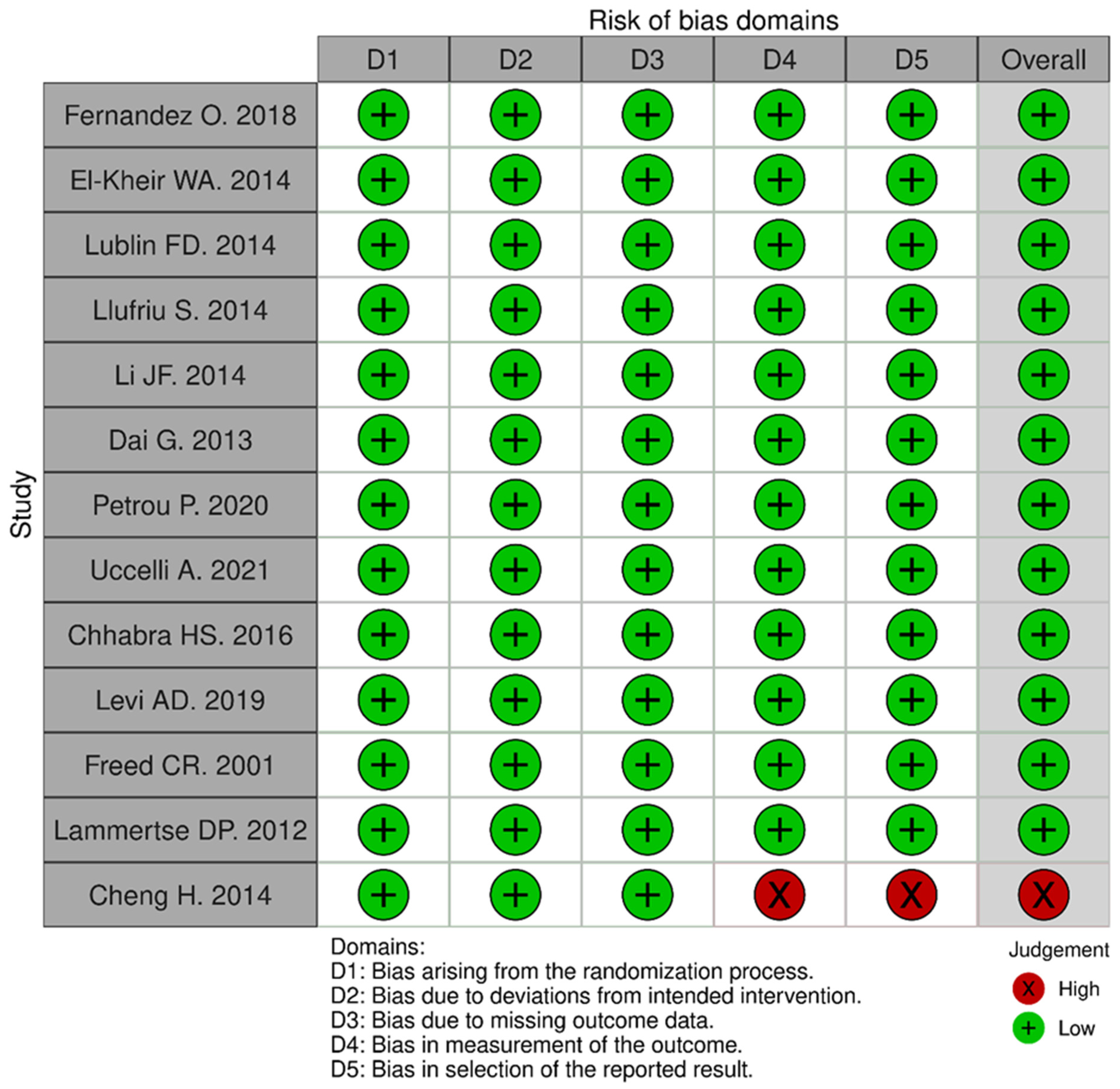
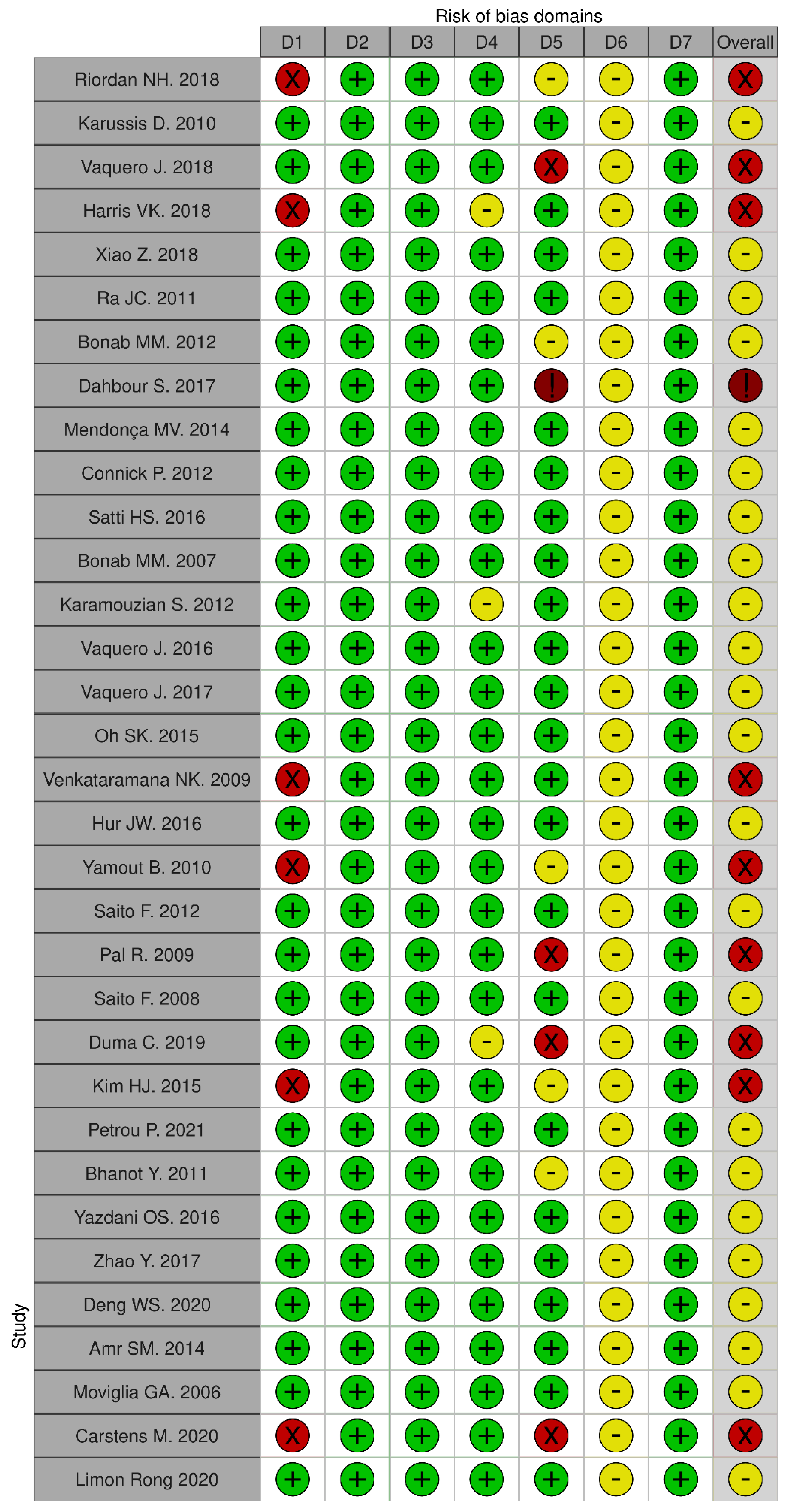
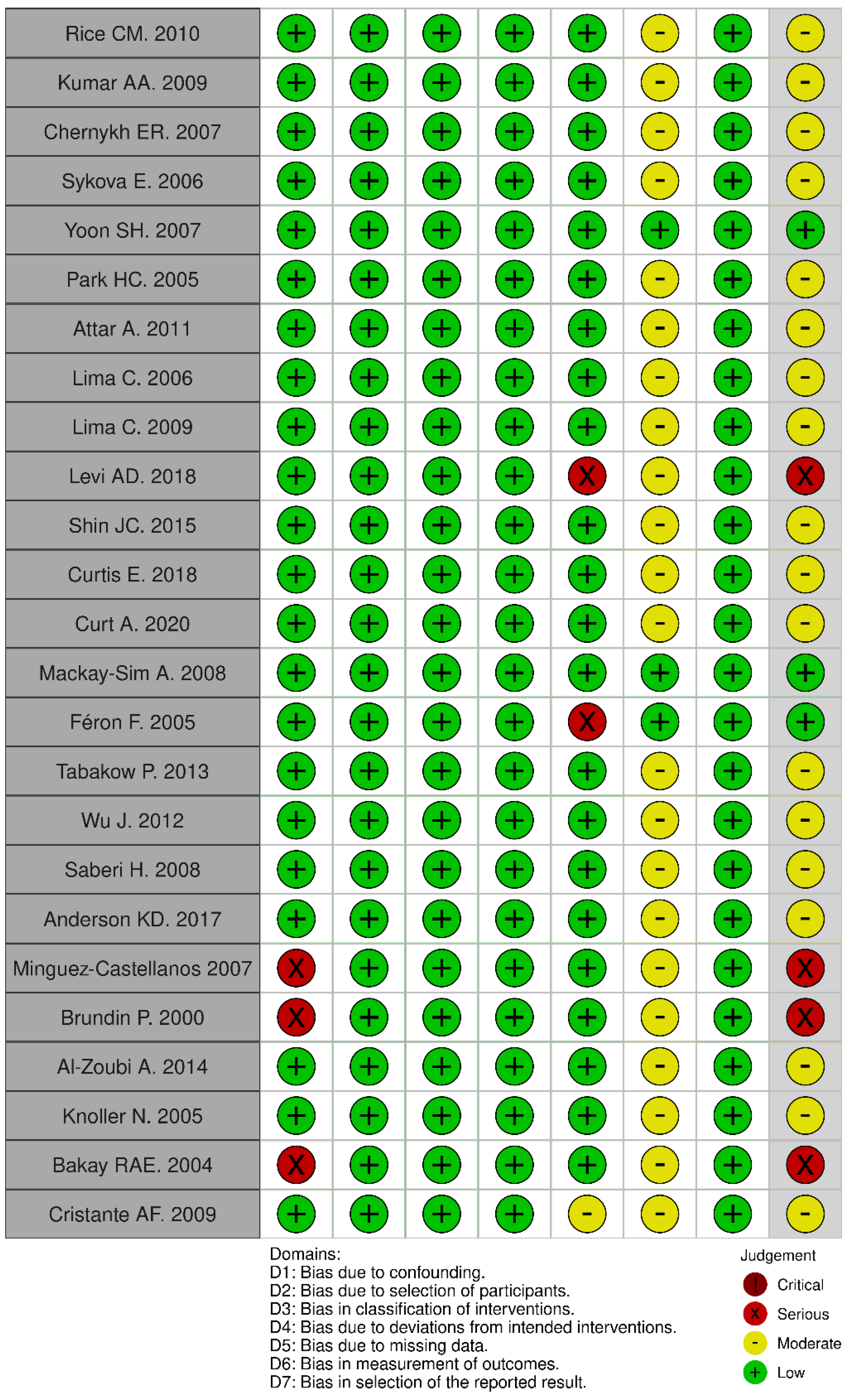
2.5. Study Risk of Bias Assessment
2.6. Data Synthesis and Statistical Analysis
3. Results
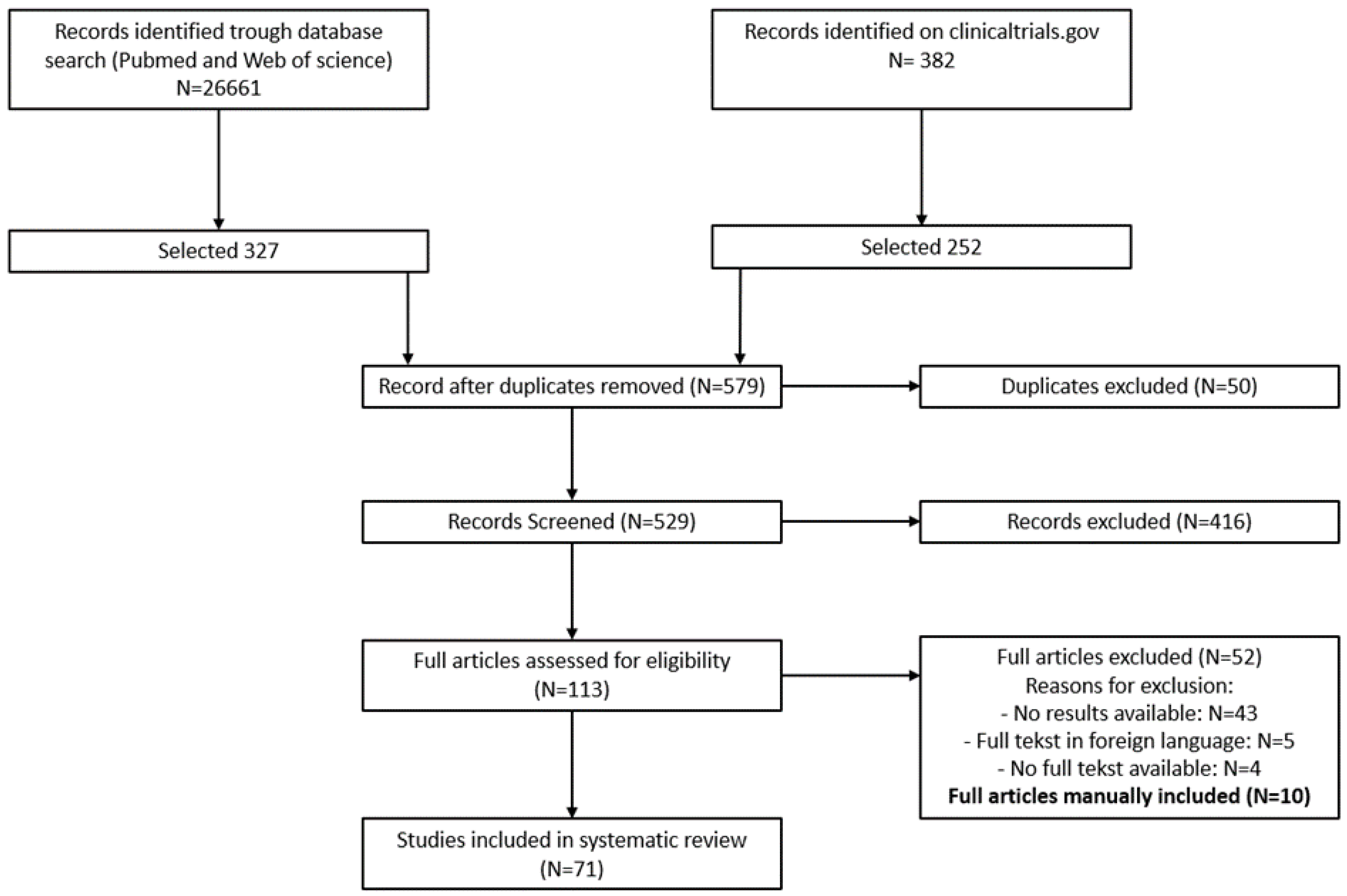
3.1. Seacrch Results
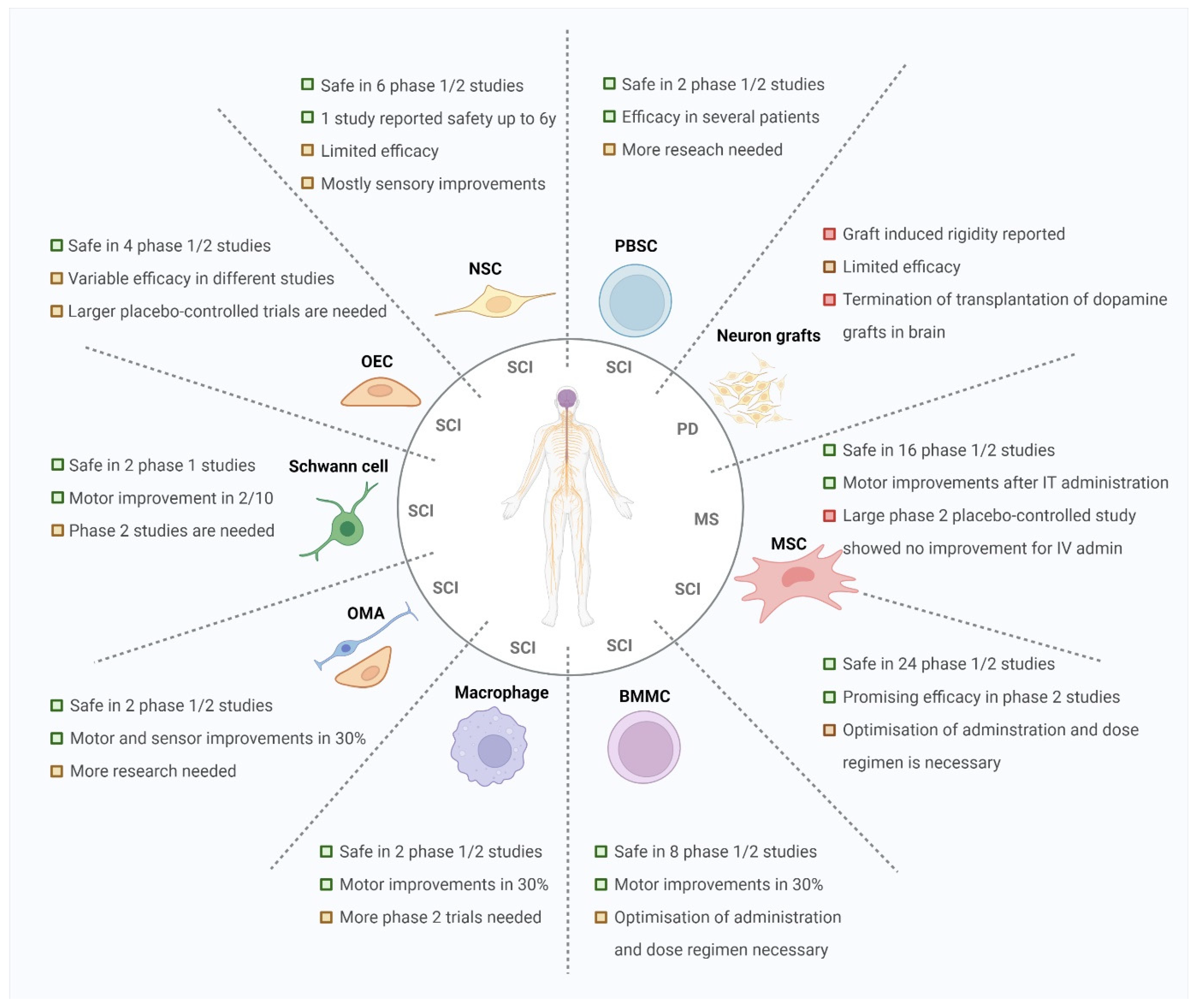
3.2. Mesenchymal Stromal Cells Exert Neuroprotective and Immunomodulatory Properties after Transplantation
3.3. Bone-Marrow and Peripheral Blood Stem Cells Showed Clinical Improvement in Some Patients
3.4. Transplantation of Neural Cells Induces Reorganisation and Repair of the Neural Network
3.5. Quality Assessment Risk of Bias
3.6. Meta-Analysis
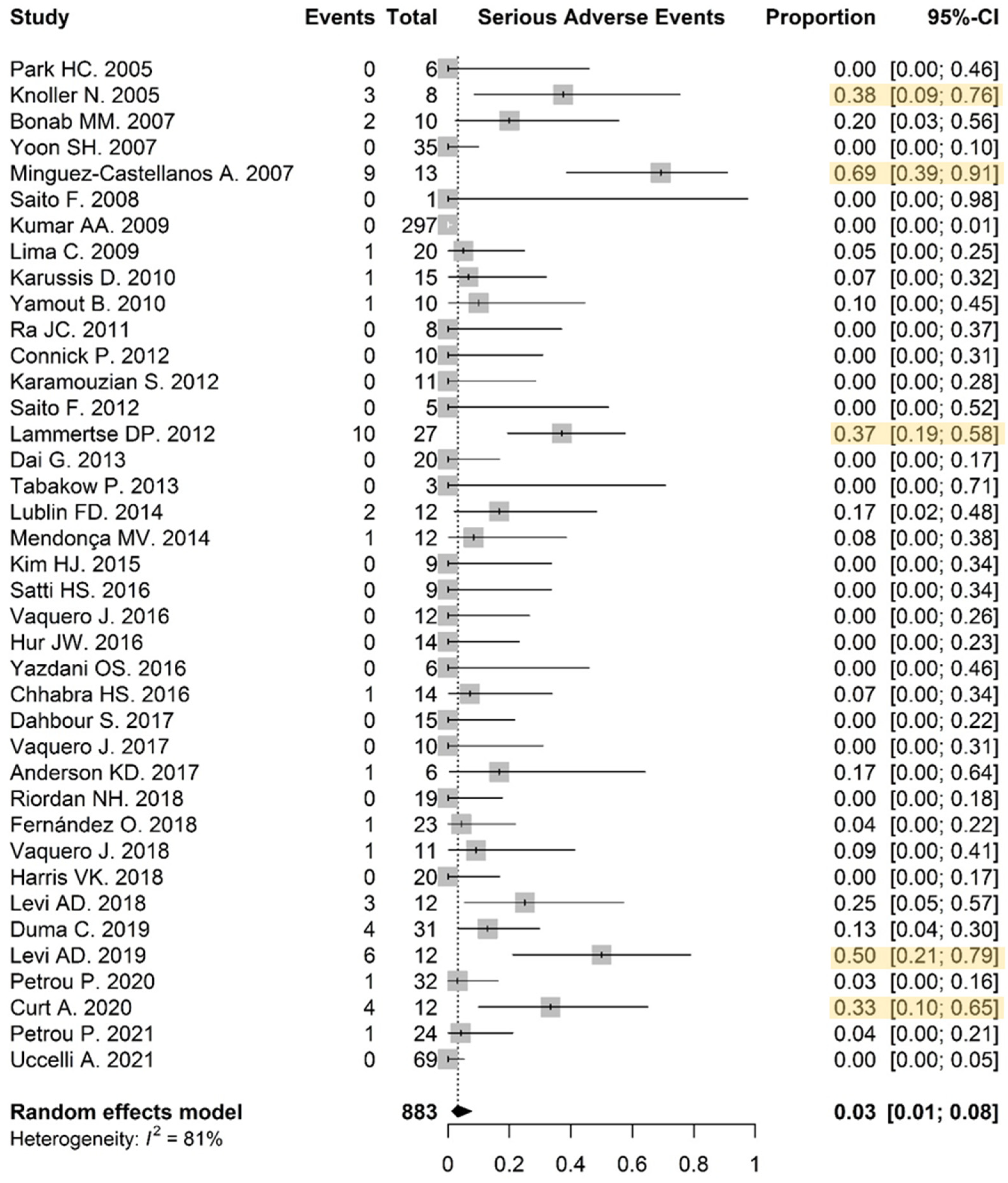
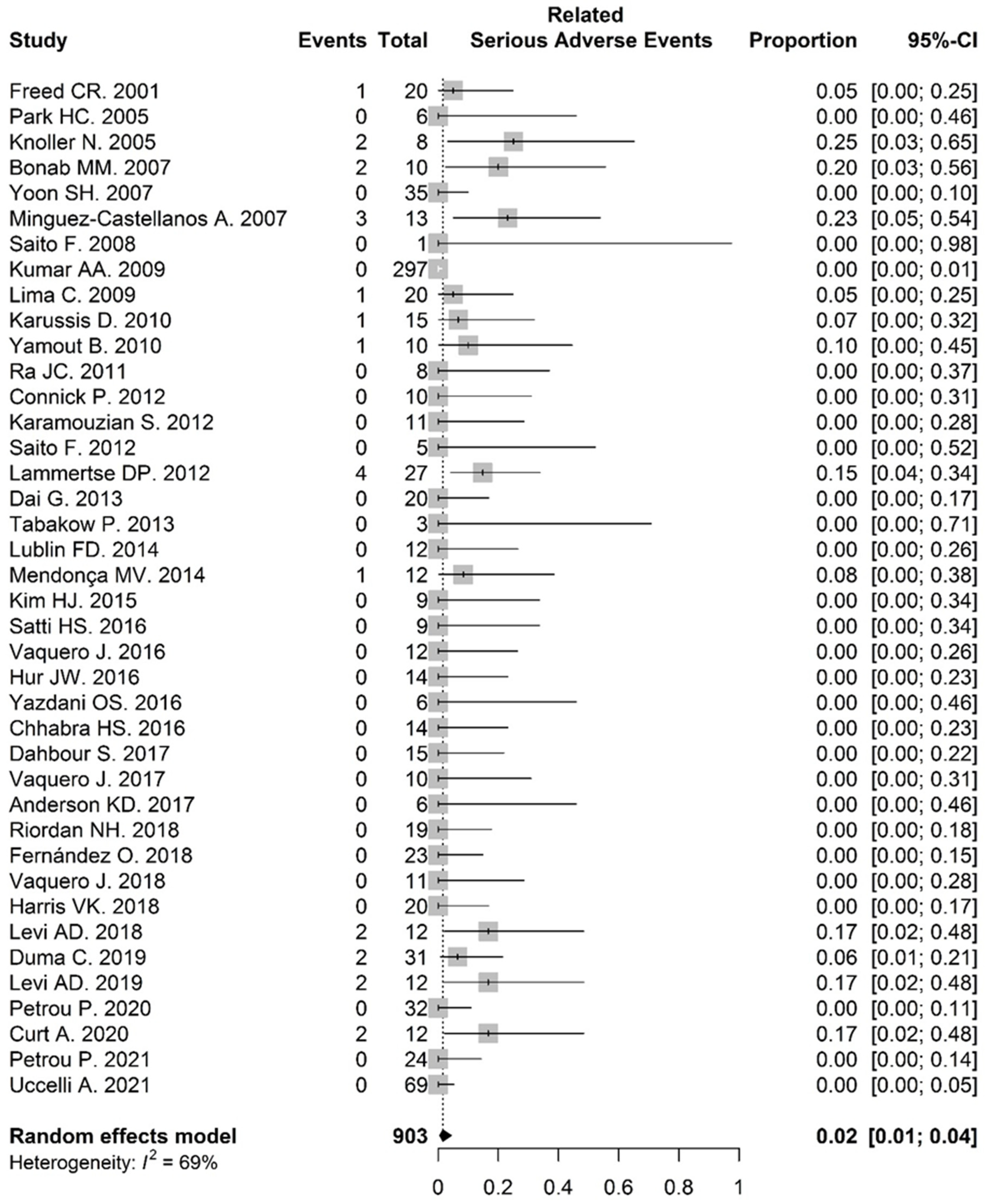
3.6.1. Serious Adverse Events
3.6.2. Adverse Events
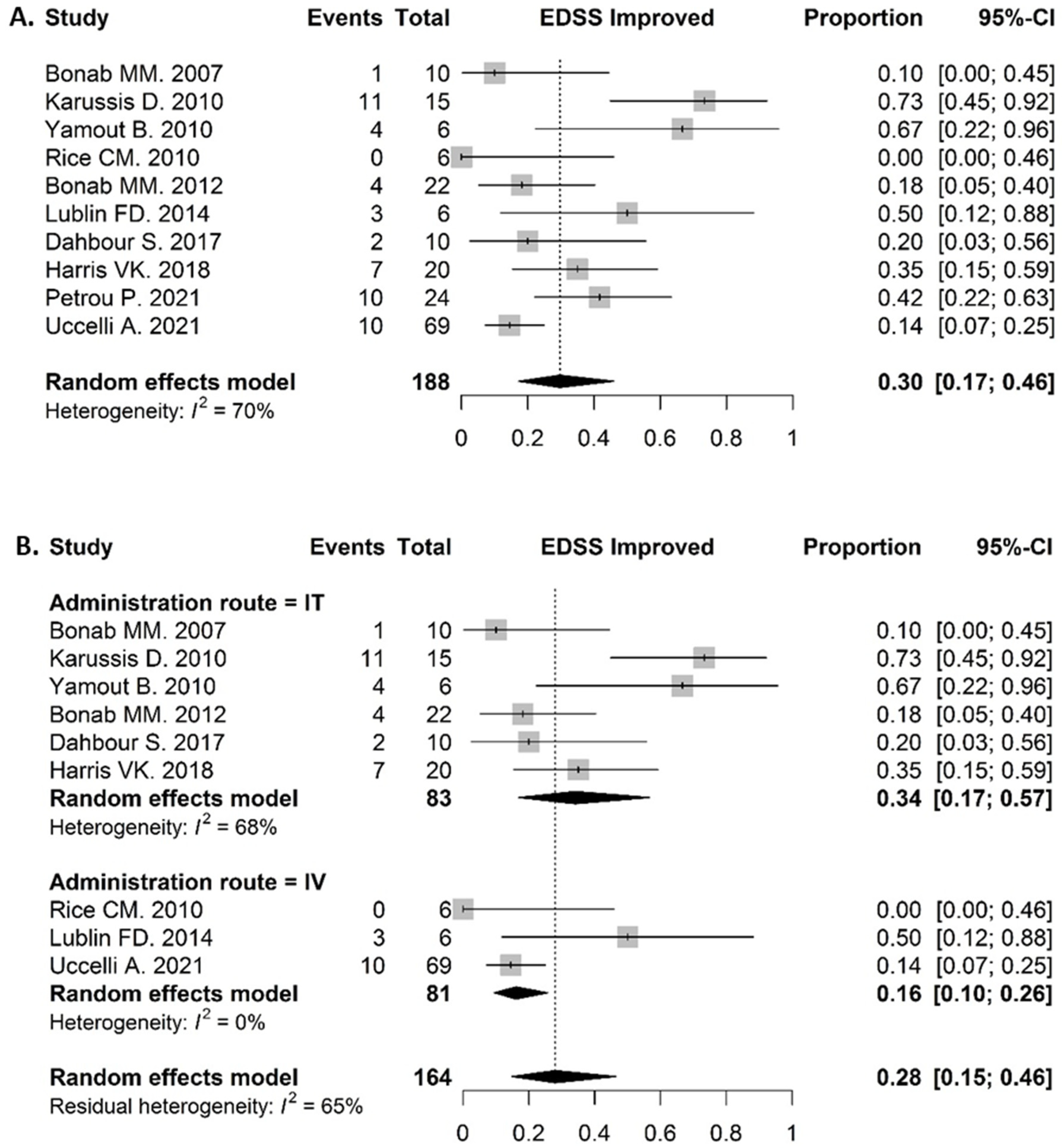
3.6.3. Clinical Response in MS Patients
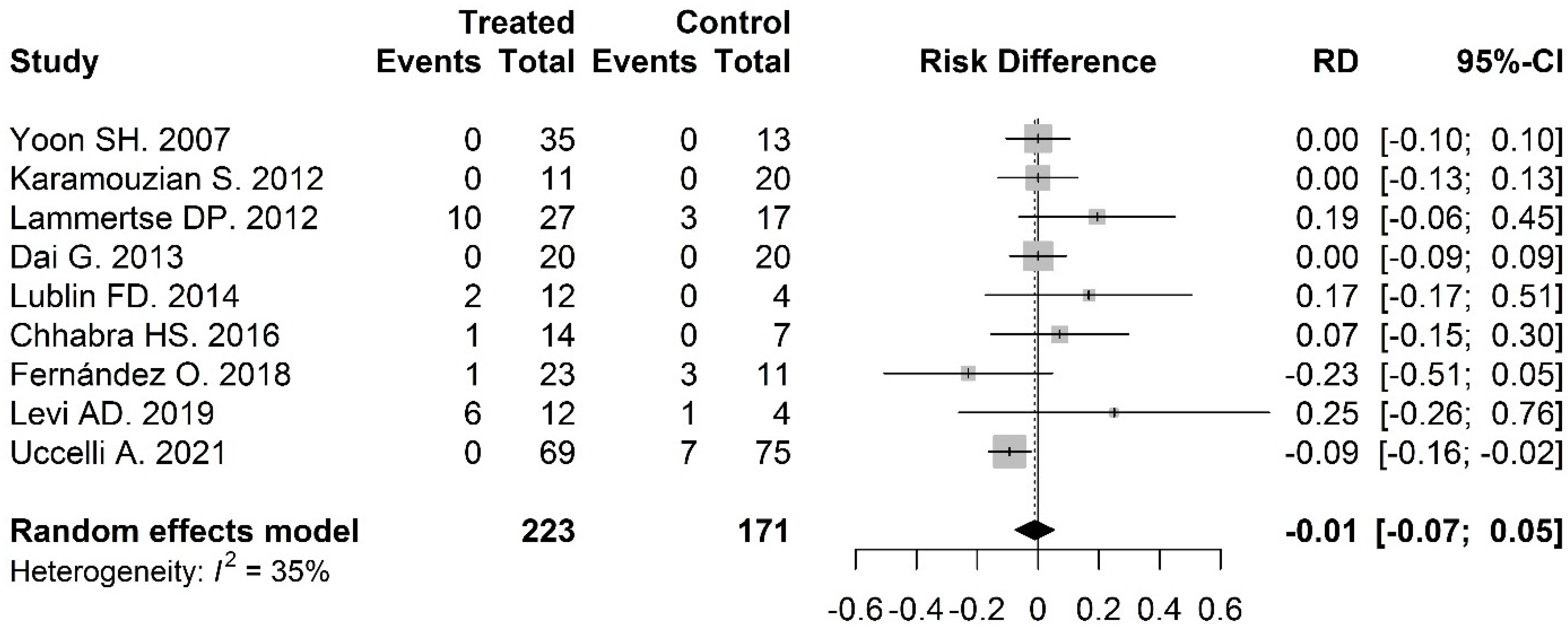
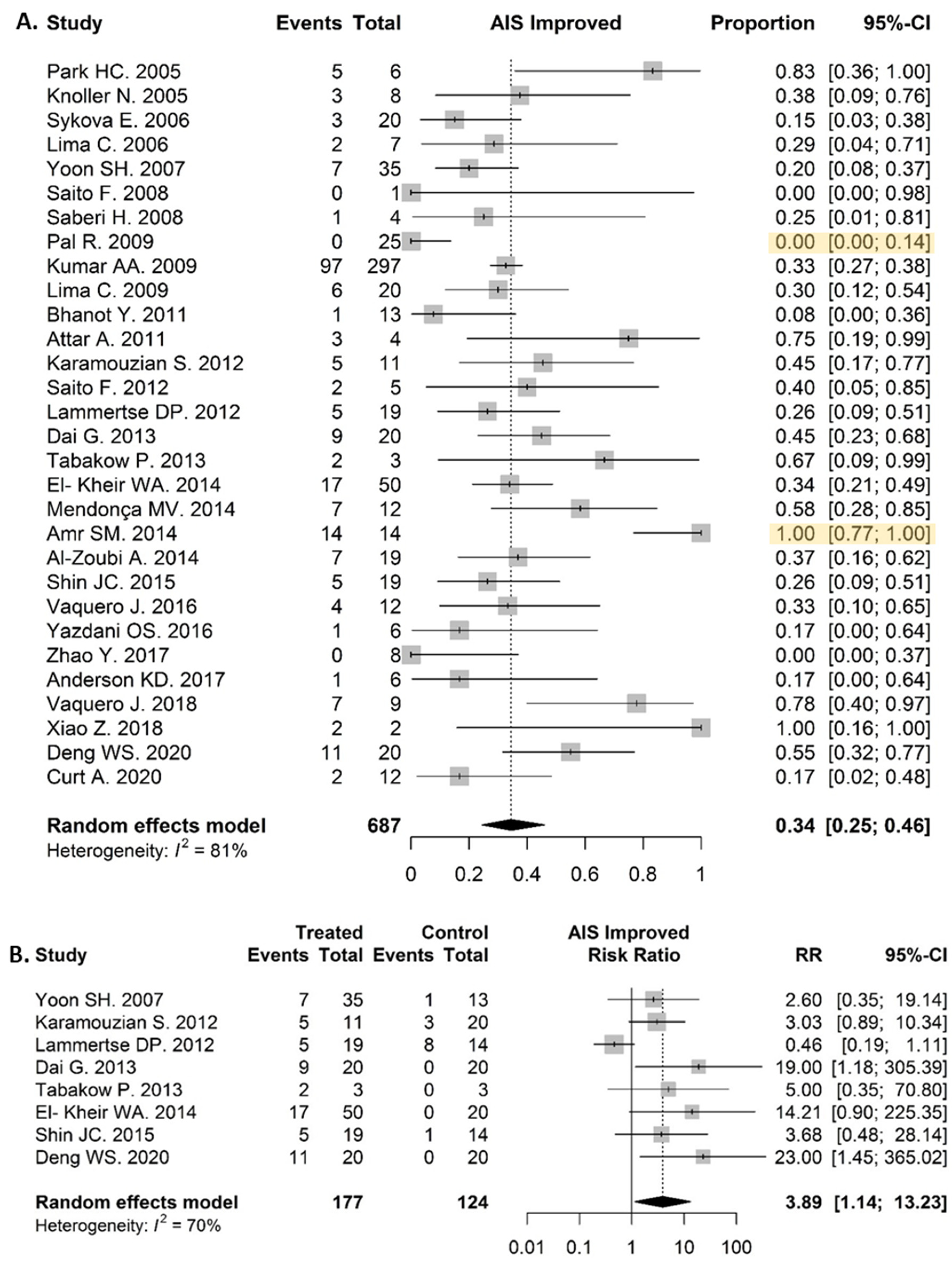
3.6.4. Clinical Response in SCI Patients
4. Discussion
4.1. Cell-Based Therapy in Neurodegenerative Diseases Showed Safety and Feasibility
4.2. Modest Clinical Improvements Were Observed in MS Patients’ EDSS Scores
4.3. AIS Grade Improved in Several SCI Patients after Cell-Based Therapy
4.4. Further Optimisation of Administration Regimen and Dosing Is Necessary
4.5. Several Hurdles Remain to Be Surpassed in Order to Develop a Successful Neuroregenerative Cell-Based Therapy
4.6. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B


Appendix C

Appendix D

References
- Golchin, A.; Shams, F.; Kangari, P.; Azari, A.; Hosseinzadeh, S. Regenerative Medicine: Injectable Cell-Based Therapeutics and Approved Products. Cell Biol. Transl. Med. 2019, 1237, 75–95. [Google Scholar] [CrossRef]
- De Gioia, R.; Biella, F.; Citterio, G.; Rizzo, F.; Abati, E.; Nizzardo, M.; Bresolin, N.; Comi, G.P.; Corti, S. Neural Stem Cell Transplantation for Neurodegenerative Diseases. Int. J. Mol. Sci. 2020, 21, 3103. [Google Scholar] [CrossRef] [PubMed]
- Payne, N.; Siatskas, C.; Barnard, A.; Bernard, C.C.A. The Prospect of Stem Cells as Multi-Faceted Purveyors of Immune Modulation, Repair and Regeneration in Multiple Sclerosis. Curr. Stem Cell Res. Ther. 2011, 6, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Shao, A.; Tu, S.; Lu, J.; Zhang, J. Crosstalk between stem cell and spinal cord injury: Pathophysiology and treatment strategies. Stem Cell Res. Ther. 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Balestrino, R.; Schapira, A.H.V. Parkinson disease. Eur. J. Neurol. 2020, 27, 27–42. [Google Scholar] [CrossRef]
- Sivandzade, F.; Cucullo, L. Regenerative Stem Cell Therapy for Neurodegenerative Diseases: An Overview. Int. J. Mol. Sci. 2021, 22, 2153. [Google Scholar] [CrossRef]
- Ohta, M. Bone marrow stromal cells infused into the cerebrospinal fluid promote functional recovery of the injured rat spinal cord with reduced cavity formation. Exp. Neurol. 2004, 187, 266–278. [Google Scholar] [CrossRef] [Green Version]
- Menezes, K.; Nascimento, M.A.; Gonçalves, J.P.; Cruz, A.S.; Lopes, D.V.; Curzio, B.; Bonamino, M.; De Menezes, J.R.L.; Borojevic, R.; Rossi, M.I.D.; et al. Human Mesenchymal Cells from Adipose Tissue Deposit Laminin and Promote Regeneration of Injured Spinal Cord in Rats. PLoS ONE 2014, 9, e96020. [Google Scholar] [CrossRef]
- Harris, V.K.; Yan, Q.J.; Vyshkina, T.; Sahabi, S.; Liu, X.; Sadiq, S.A. Clinical and pathological effects of intrathecal injection of mesenchymal stem cell-derived neural progenitors in an experimental model of multiple sclerosis. J. Neurol. Sci. 2011, 313, 167–177. [Google Scholar] [CrossRef]
- Akiyama, Y.; Radtke, C.; Honmou, O.; Kocsis, J.D. Remyelination of the spinal cord following intravenous delivery of bone marrow cells. Glia 2002, 39, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Honmou, O.; Akiyama, Y.; Uede, T.; Hashi, K.; Kocsis, J.D. Transplantation of an acutely isolated bone marrow fraction repairs demyelinated adult rat spinal cord axons. Glia 2001, 35, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwatsuki, K.; Yoshimine, T.; Kishima, H.; Aoki, M.; Yoshimura, K.; Ishihara, M.; Ohnishi, Y.; Lima, C. Transplantation of olfactory mucosa following spinal cord injury promotes recovery in rats. NeuroReport 2008, 19, 1249–1252. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Féron, F.; Mackay-Sim, A.; Waite, P.M.E. Olfactory ensheathing cells promote locomotor recovery after delayed transplantation into transected spinal cord. Brain 2002, 125, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramón-Cueto, A.; Cordero, M.I.; Santos-Benito, F.F.; Avila, J. Functional Recovery of Paraplegic Rats and Motor Axon Regeneration in Their Spinal Cords by Olfactory Ensheathing Glia. Neuron 2000, 25, 425–435. [Google Scholar] [CrossRef] [Green Version]
- Cummings, B.J.; Uchida, N.; Tamaki, S.J.; Salazar, D.L.; Hooshmand, M.; Summers, R.; Gage, F.H.; Anderson, A.J. Human neural stem cells differentiate and promote locomotor recovery in spinal cord-injured mice. Proc. Natl. Acad. Sci. USA 2005, 102, 14069–14074. [Google Scholar] [CrossRef] [Green Version]
- Pearse, D.D.; Sanchez, A.R.; Pereira, F.C.; Andrade, C.M.; Puzis, R.; Pressman, Y.; Golden, K.; Kitay, B.M.; Blits, B.; Wood, P.M.; et al. Transplantation of Schwann cells and/or olfactory ensheathing glia into the contused spinal cord: Survival, migration, axon association, and functional recovery. Glia 2007, 55, 976–1000. [Google Scholar] [CrossRef]
- Bomstein, Y.; Marder, J.B.; Vitner, K.; Smirnov, I.; Lisaey, G.; Butovsky, O.; Fulga, V.; Yoles, E. Features of skin-coincubated macrophages that promote recovery from spinal cord injury. J. Neuroimmunol. 2003, 142, 10–16. [Google Scholar] [CrossRef]
- Bai, L.; Lennon, D.P.; Caplan, A.I.; DeChant, A.; Hecker, J.; Kranso, J.; Zaremba, A.; Miller, R.H. Hepatocyte growth factor mediates mesenchymal stem cell–induced recovery in multiple sclerosis models. Nat. Neurosci. 2012, 15, 862–870. [Google Scholar] [CrossRef] [Green Version]
- Toledo-Aral, J.J.; Méndez-Ferrer, S.; Pardal, R.; Echevarría, M.; López-Barneo, J. Trophic Restoration of the Nigrostriatal Dopaminergic Pathway in Long-Term Carotid Body-Grafted Parkinsonian Rats. J. Neurosci. 2003, 23, 141–148. [Google Scholar] [CrossRef]
- Espejo, E.F.; Montoro, R.J.; Armengol, J.A.; López-Barneo, J. Cellular and Functional Recovery of Parkinsonian Rats after Intrastriatal Transplantation of Carotid Body Cell Aggregates. Neuron 1998, 20, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Björklund, A.; Stenevi, U. Reconstruction of the nigrostriatal dopamine pathway by intracerebral nigral transplants. Brain Res. 1979, 177, 555–560. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Friedenstein, A.J.; Chailakhjan, R.K.; Lalykina, K.S. The development of fibroblast colonies in monolayer cultures of guinea-pig bone marrow and spleen cells. Cell Prolif. 1970, 3, 393–403. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage Cells from Human Adipose Tissue: Implications for Cell-Based Therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef] [Green Version]
- Miao, Z.; Jin, J.; Chen, L.; Zhu, J.; Huang, W.; Zhao, J.; Qian, H.; Zhang, X. Isolation of mesenchymal stem cells from human placenta: Comparison with human bone marrow mesenchymal stem cells. Cell Biol. Int. 2006, 30, 681–687. [Google Scholar] [CrossRef]
- Broxmeyer, H.E.; Douglas, G.W.; Hangoc, G.; Cooper, S.; Bard, J.; English, D.; Arny, M.; Thomas, L.; Boyse, E.A. Human umbilical cord blood as a potential source of transplantable hematopoietic stem/progenitor cells. Proc. Natl. Acad. Sci. USA 1989, 86, 3828–3832. [Google Scholar] [CrossRef] [Green Version]
- Andrzejewska, A.; Lukomska, B.; Janowski, M. Concise review: Mesenchymal stem cells: From roots to boost. Stem Cells 2019, 37, 855–864. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.J.; Bae, Y.K.; Kim, M.; Kwon, S.-J.; Jeon, H.B.; Choi, S.J.; Kim, S.W.; Yang, Y.S.; Oh, W.; Chang, J.W. Comparative Analysis of Human Mesenchymal Stem Cells from Bone Marrow, Adipose Tissue, and Umbilical Cord Blood as Sources of Cell Therapy. Int. J. Mol. Sci. 2013, 14, 17986–18001. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Li, X.; Zhang, Y.; Han, Y.; Chang, F.; Ding, J. Mesenchymal Stem Cells for Regenerative Medicine. Cells 2019, 8, 886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uccelli, A.; Benvenuto, F.; Laroni, A.; Giunti, D. Neuroprotective features of mesenchymal stem cells. Best Pract. Res. Clin. Haematol. 2011, 24, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Ghannam, S.; Pène, J.; Torcy-Moquet, G.; Jorgensen, C.; Yssel, H. Mesenchymal Stem Cells Inhibit Human Th17 Cell Differentiation and Function and Induce a T Regulatory Cell Phenotype. J. Immunol. 2010, 185, 302–312. [Google Scholar] [CrossRef] [Green Version]
- Ra, J.C.; Shin, I.S.; Kim, S.H.; Kang, S.K.; Kang, B.C.; Lee, H.Y.; Kim, Y.J.; Jo, J.Y.; Yoon, E.J.; Choi, H.J.; et al. Safety of Intravenous Infusion of Human Adipose Tissue-Derived Mesenchymal Stem Cells in Animals and Humans. Stem Cells Dev. 2011, 20, 1297–1308. [Google Scholar] [CrossRef]
- Zhou, Z.; Chen, Y.; Zhang, H.; Min, S.; Yu, B.; He, B.; Jin, A. Comparison of mesenchymal stromal cells from human bone marrow and adipose tissue for the treatment of spinal cord injury. Cytotherapy 2013, 15, 434–448. [Google Scholar] [CrossRef]
- Duma, C.; Kopyov, O.; Kopyov, A.; Berman, M.; Lander, E.; Elam, M.; Arata, M.; Weiland, D.; Cannell, R.; Caraway, C.; et al. Human intracerebroventricular (ICV) injection of autologous, non-engineered, adipose-derived stromal vascular fraction (ADSVF) for neurodegenerative disorders: Results of a 3-year phase 1 study of 113 injections in 31 patients. Mol. Biol. Rep. 2019, 46, 5257–5272. [Google Scholar] [CrossRef] [Green Version]
- Kern, S.; Eichler, H.; Stoeve, J.; Klüter, H.; Bieback, K. Comparative Analysis of Mesenchymal Stem Cells from Bone Marrow, Umbilical Cord Blood, or Adipose Tissue. Stem Cells 2006, 24, 1294–1301. [Google Scholar] [CrossRef]
- Madrigal, M.; Rao, K.S.; Riordan, N.H. A review of therapeutic effects of mesenchymal stem cell secretions and induction of secretory modification by different culture methods. J. Transl. Med. 2014, 12, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Mazini, L.; Rochette, L.; Amine, M.; Malka, G. Regenerative Capacity of Adipose Derived Stem Cells (ADSCs), Comparison with Mesenchymal Stem Cells (MSCs). Int. J. Mol. Sci. 2019, 20, 2523. [Google Scholar] [CrossRef] [Green Version]
- Riordan, N.H.; Morales, I.; Fernández, G.; Allen, N.; Fearnot, N.E.; Leckrone, M.E.; Markovich, D.J.; Mansfield, D.; Avila, D.; Patel, A.N.; et al. Clinical feasibility of umbilical cord tissue-derived mesenchymal stem cells in the treatment of multiple sclerosis. J. Transl. Med. 2018, 16, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.-F.; Zhang, D.-J.; Geng, T.; Chen, L.; Huang, H.; Yin, H.-L.; Zhang, Y.-Z.; Lou, J.-Y.; Cao, B.; Wang, Y.-L. The Potential of Human Umbilical Cord-Derived Mesenchymal Stem Cells as a Novel Cellular Therapy for Multiple Sclerosis. Cell Transplant. 2014, 23, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Seo, S.W.; Chang, J.W.; Lee, J.I.; Kim, C.H.; Chin, J.; Choi, S.J.; Kwon, H.; Yun, H.J.; Lee, J.M.; et al. Stereotactic brain injection of human umbilical cord blood mesenchymal stem cells in patients with Alzheimer’s disease dementia: A phase 1 clinical trial. Alzheimer’s Dementia Transl. Res. Clin. Interv. 2015, 1, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Liu, X.; Hua, R.; Dai, G.; Wang, X.; Gao, J.; An, Y. Clinical observation of umbilical cord mesenchymal stem cell transplantation in treatment for sequelae of thoracolumbar spinal cord injury. J. Transl. Med. 2014, 12, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lublin, F.D.; Bowen, J.D.; Huddlestone, J.; Kremenchutzky, M.; Carpenter, A.; Corboy, J.R.; Freedman, M.S.; Krupp, L.; Paulo, C.; Hariri, R.J.; et al. Human placenta-derived cells (PDA-001) for the treatment of adults with multiple sclerosis: A randomized, placebo-controlled, multiple-dose study. Mult. Scler. Relat. Disord. 2014, 3, 696–704. [Google Scholar] [CrossRef] [Green Version]
- Talwadekar, M.D.; Kale, V.P.; Limaye, L.S. Placenta-derived mesenchymal stem cells possess better immunoregulatory properties compared to their cord-derived counterparts–a paired sample study. Sci. Rep. 2015, 5, 15784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karussis, D.; Karageorgiou, C.; Vaknin-Dembinsky, A.; Gowda-Kurkalli, B.; Gomori, J.M.; Kassis, I.; Bulte, J.W.M.; Petrou, P.; Ben-Hur, T.; Abramsky, O.; et al. Safety and Immunological Effects of Mesenchymal Stem Cell Transplantation in Patients With Multiple Sclerosis and Amyotrophic Lateral Sclerosis. Arch. Neurol. 2010, 67, 1187–1194. [Google Scholar] [CrossRef]
- Yamout, B.; Hourani, R.; Salti, H.; Barada, W.; El-Hajj, T.; Al-Kutoubi, A.; Herlopian, A.; Baz, E.K.; Mahfouz, R.; Khalil-Hamdan, R.; et al. Bone marrow mesenchymal stem cell transplantation in patients with multiple sclerosis: A pilot study. J. Neuroimmunol. 2010, 227, 185–189. [Google Scholar] [CrossRef]
- Bonab, M.M.; Yazdanbakhsh, S.; Lotfi, J.; Alimoghaddom, K.; Talebian, F.; Hooshmand, F.; Ghavamzadeh, A.; Nikbin, B. Does mesenchymal stem cell therapy help multiple sclerosis patients? Report of a pilot study. Iran. J. Immunol. IJI 2007, 4, 50–57. [Google Scholar]
- Mendonça, M.V.P.; Larocca, T.F.; Souza, B.S.D.F.; Villarreal, C.F.; Silva, L.F.M.; Matos, A.C.; Novaes, M.A.; Bahia, C.M.P.; Martinez, A.C.D.O.M.; Kaneto, C.M.; et al. Safety and neurological assessments after autologous transplantation of bone marrow mesenchymal stem cells in subjects with chronic spinal cord injury. Stem Cell Res. Ther. 2014, 5, 126. [Google Scholar] [CrossRef] [Green Version]
- Bonab, M.M.; Sahraian, M.A.; Aghsaie, A.; Karvigh, S.A.; Hosseinian, S.M.; Nikbin, B.; Lotfi, J.; Khorramnia, S.; Motamed, M.R.; Togha, M.; et al. Autologous Mesenchymal Stem Cell Therapy in Progressive Multiple Sclerosis: An Open Label Study. Curr. Stem Cell Res. Ther. 2012, 7, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Strioga, M.; Viswanathan, S.; Darinskas, A.; Slaby, O.; Michalek, J. Same or Not the Same? Comparison of Adipose Tissue-Derived Versus Bone Marrow-Derived Mesenchymal Stem and Stromal Cells. Stem Cells Dev. 2012, 21, 2724–2752. [Google Scholar] [CrossRef] [PubMed]
- Paul, C.; Samdani, A.F.; Betz, R.R.; Fischer, I.; Neuhuber, B. Grafting of Human Bone Marrow Stromal Cells Into Spinal Cord Injury. Spine 2009, 34, 328–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, G.; Liu, X.; Zhang, Z.; Yang, Z.; Dai, Y.; Xu, R. Transplantation of autologous bone marrow mesenchymal stem cells in the treatment of complete and chronic cervical spinal cord injury. Brain Res. 2013, 1533, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Venkataramana, N.K.; Kumar, S.K.; Balaraju, S.; Radhakrishnan, R.C.; Bansal, A.; Dixit, A.; Rao, D.K.; Das, M.; Jan, M.; Gupta, P.K.; et al. Open-labeled study of unilateral autologous bone-marrow-derived mesenchymal stem cell transplantation in Parkinson’s disease. Transl. Res. 2010, 155, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Deng, W.-S.; Ma, K.; Liang, B.; Liu, X.-Y.; Xu, H.-Y.; Zhang, J.; Shi, H.-Y.; Sun, H.-T.; Chen, X.-Y.; Zhang, S. Collagen scaffold combined with human umbilical cord-mesenchymal stem cells transplantation for acute complete spinal cord injury. Neural Regen. Res. 2020, 15, 1686. [Google Scholar] [CrossRef]
- Xiao, Z.; Tang, F.; Zhao, Y.; Han, G.; Yin, N.; Li, X.; Chen, B.; Han, S.; Jiang, X.; Yun, C.; et al. Significant Improvement of Acute Complete Spinal Cord Injury Patients Diagnosed by a Combined Criteria Implanted with NeuroRegen Scaffolds and Mesenchymal Stem Cells. Cell Transplant. 2018, 27, 907–915. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Tang, F.; Xiao, Z.; Han, G.; Wang, N.; Yin, N.; Chen, B.; Jiang, X.; Yun, C.; Han, W.; et al. Clinical Study of NeuroRegen Scaffold Combined with Human Mesenchymal Stem Cells for the Repair of Chronic Complete Spinal Cord Injury. Cell Transplant. 2017, 26, 891–900. [Google Scholar] [CrossRef]
- Amr, S.M.; Gouda, A.; Koptan, W.T.; Galal, A.A.; Abdel-Fattah, D.S.; Rashed, L.A.; Atta, H.M.; Abdel-Aziz, M.T. Bridging defects in chronic spinal cord injury using peripheral nerve grafts combined with a chitosan-laminin scaffold and enhancing regeneration through them by co-transplantation with bone-marrow-derived mesenchymal stem cells: Case series of 14 patients. J. Spinal Cord Med. 2013, 37, 54–71. [Google Scholar] [CrossRef] [Green Version]
- Han, S.; Wang, B.; Jin, W.; Xiao, Z.; Chen, B.; Xiao, H.; Ding, W.; Cao, J.; Ma, F.; Li, X.; et al. The collagen scaffold with collagen binding BDNF enhances functional recovery by facilitating peripheral nerve infiltrating and ingrowth in canine complete spinal cord transection. Spinal Cord 2014, 52, 867–873. [Google Scholar] [CrossRef] [Green Version]
- Ashammakhi, N.; Kim, H.-J.; Ehsanipour, A.; Bierman, R.D.; Kaarela, O.; Xue, C.; Khademhosseini, A.; Seidlits, S.K. Regenerative Therapies for Spinal Cord Injury. Tissue Eng. Part B Rev. 2019, 25, 471–491. [Google Scholar] [CrossRef]
- Xu, B.; Zhao, Y.; Xiao, Z.; Wang, B.; Liang, H.; Li, X.; Fang, Y.; Han, S.; Li, X.; Fan, C.; et al. A Dual Functional Scaffold Tethered with EGFR Antibody Promotes Neural Stem Cell Retention and Neuronal Differentiation for Spinal Cord Injury Repair. Adv. Healthc. Mater. 2017, 6, 1601279. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Xiao, Z.; Li, X.; Zhao, H.; Wang, B.; Qiu, Z.; Mei, X.; Xu, B.; Fan, C.; Chen, B.; et al. Human placenta-derived mesenchymal stem cells loaded on linear ordered collagen scaffold improves functional recovery after completely transected spinal cord injury in canine. Sci. China Life Sci. 2017, 61, 2–13. [Google Scholar] [CrossRef]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Bonilla, C.; Aguayo, C.; Montilla, J.; Bustamante, S.; Carballido, J.; Marin, E.; Martinez, F.; et al. An approach to personalized cell therapy in chronic complete paraplegia: The Puerta de Hierro phase I/II clinical trial. Cytotherapy 2016, 18, 1025–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrou, P.; Kassis, I.; Ginzberg, A.; Halimi, M.; Yaghmour, N.; Abramsky, O.; Karussis, D. Long-Term Clinical and Immunological Effects of Repeated Mesenchymal Stem Cell Injections in Patients with Progressive Forms of Multiple Sclerosis. Front. Neurol. 2021, 12, 737. [Google Scholar] [CrossRef] [PubMed]
- Mesentier-Louro, L.A.; Zaverucha-Do-Valle, C.; de Castro, P.H.R.; Silva-Junior, A.J.; Pimentel-Coelho, P.M.; Mendez-Otero, R.; Santiago, M.F. Bone Marrow-Derived Cells as a Therapeutic Approach to Optic Nerve Diseases. Stem Cells Int. 2016, 2016, 5078619. [Google Scholar] [CrossRef] [Green Version]
- Kawada, H.; Takizawa, S.; Takanashi, T.; Morita, Y.; Fujita, J.; Fukuda, K.; Takagi, S.; Okano, H.; Ando, K.; Hotta, T. Administration of Hematopoietic Cytokines in the Subacute Phase After Cerebral Infarction Is Effective for Functional Recovery Facilitating Proliferation of Intrinsic Neural Stem/Progenitor Cells and Transition of Bone Marrow-Derived Neuronal Cells. Circulation 2006, 113, 701–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshizuka, S.; Okada, S.; Okawa, A.; Koda, M.; Murasawa, M.; Hashimoto, M.; Kamada, T.; Yoshinaga, K.; Murakami, M.; Moriya, H.; et al. Transplanted Hematopoietic Stem Cells from Bone Marrow Differentiate into Neural Lineage Cells and Promote Functional Recovery after Spinal Cord Injury in Mice. J. Neuropathol. Exp. Neurol. 2004, 63, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Rice, C.M.; Mallam, E.A.; Whone, A.L.; Walsh, P.; Brooks, D.J.; Kane, N.; Butler, S.R.; Marks, D.I.; Scolding, N.J. Safety and Feasibility of Autologous Bone Marrow Cellular Therapy in Relapsing-Progressive Multiple Sclerosis. Clin. Pharmacol. Ther. 2010, 87, 679–685. [Google Scholar] [CrossRef]
- Chhabra, H.S.; Sarda, K.; Arora, M.; Sharawat, R.; Singh, V.; Nanda, A.; Sangodimath, G.M.; Tandon, V. Autologous bone marrow cell transplantation in acute spinal cord injury—An Indian pilot study. Spinal Cord 2015, 54, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.A.; Kumar, S.R.; Narayanan, R.; Arul, K.; Baskaran, M. Autologous bone marrow derived mononuclear cell ther-apy for spinal cord injury: A phase I/II clinical safety and primary efficacy data. Exp. Clin. Transpl. 2009, 7, 241–248. [Google Scholar]
- Yoon, S.H.; Shim, Y.S.; Park, Y.H.; Chung, J.K.; Nam, J.H.; Kim, M.O.; Park, H.C.; Park, S.R.; Min, B.-H.; Kim, E.Y.; et al. Complete Spinal Cord Injury Treatment Using Autologous Bone Marrow Cell Transplantation and Bone Marrow Stimulation with Granulocyte Macrophage-Colony Stimulating Factor: Phase I/II Clinical Trial. Stem Cells 2007, 25, 2066–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chernykh, E.R.; Stupak, V.V.; Muradov, G.M.; Sizikov, M.Y.; Shevela, E.Y.; Leplina, O.Y.; Tikhonova, M.; Kulagin, A.; Lisukov, I.A.; Ostanin, A.A.; et al. Application of autologous bone marrow stem cells in the therapy of spinal cord injury patients. Bull. Exp. Biol. Med. 2007, 143, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Syková, E.; Homola, A.; Mazanec, R.; Lachmann, H.; Konrádová, L.; Kobylka, P.; Pádr, R.; Neuwirth, J.; Komrska, V.; Vávra, V.; et al. Autologous Bone Marrow Transplantation in Patients with Subacute and Chronic Spinal Cord Injury. Cell Transplant. 2006, 15, 675–687. [Google Scholar] [CrossRef]
- Park, H.C.; Shim, Y.S.; Ha, Y.; Yoon, S.H.; Park, S.R.; Choi, B.H.; Park, H.S. Treatment of Complete Spinal Cord Injury Patients by Autologous Bone Marrow Cell Transplantation and Administration of Granulocyte-Macrophage Colony Stimulating Factor. Tissue Eng. 2005, 11, 913–922. [Google Scholar] [CrossRef]
- Attar, A.; Ayten, M.; Ozdemir, M.; Ozgencil, E.; Bozkurt, M.; Kaptanoglu, E.; Beksac, M.; Kanpolat, Y. An attempt to treat patients who have injured spinal cords with intralesional implantation of concentrated autologous bone marrow cells. Cytotherapy 2011, 13, 54–60. [Google Scholar] [CrossRef]
- Bouhy, D.; Malgrange, B.; Multon, S.; Poirrier, A.-L.; Scholtes, F.; Schoenen, J.; Franzen, R. Delayed GM-CSF treatment stimulates axonal regeneration and functional recovery in paraplegic rats via an increased BDNF expression by endogenous macrophages. FASEB J. 2006, 20, 1239–1241. [Google Scholar] [CrossRef]
- Cristante, A.F.; Filho, T.E.P.D.B.; Tatsui, N.; Mendrone, A.; Caldas, J.G.; Camargo, A.; Alexandre, A.; Teixeira, W.G.J.; Oliveira, R.P.; Marcon, R. Stem cells in the treatment of chronic spinal cord injury: Evaluation of somatosensitive evoked potentials in 39 patients. Spinal Cord 2009, 47, 733–738. [Google Scholar] [CrossRef]
- Al-Zoubi, A.; Jafar, E.; Jamous, M.; Al-Twal, F.; Al-Bakheet, S.; Zalloum, M.; Khalifeh, F.; Abu Radi, S.; El-Khateeb, M.; Al-Zoubi, Z. Transplantation of Purified Autologous Leukapheresis-Derived CD34+ and CD133+ Stem Cells for Patients with Chronic Spinal Cord Injuries: Long-Term Evaluation of Safety and Efficacy. Cell Transplant. 2014, 23, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Knoller, N.; Auerbach, G.; Fulga, V.; Zelig, G.; Attias, J.; Bakimer, R.; Marder, J.B.; Yoles, E.; Belkin, M.; Schwartz, M.; et al. Clinical experience using incubated autologous macrophages as a treatment for complete spinal cord injury: Phase I study results. J. Neurosurg. Spine 2005, 3, 173–181. [Google Scholar] [CrossRef]
- Lammertse, D.P.; Jones, L.A.T.; Charlifue, S.B.; Kirshblum, S.C.; Apple, D.F.; Ragnarsson, K.T.; Falci, S.; Heary, R.F.; Choudhri, T.F.; Jenkins, A.L.; et al. Autologous incubated macrophage therapy in acute, complete spinal cord injury: Results of the phase 2 randomized controlled multicenter trial. Spinal Cord 2012, 50, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Levi, A.D.; Anderson, K.D.; Okonkwo, D.O.; Park, P.; Bryce, T.N.; Kurpad, S.N.; Aarabi, B.; Hsieh, J.; Gant, K. Clinical Outcomes from a Multi-Center Study of Human Neural Stem Cell Transplantation in Chronic Cervical Spinal Cord Injury. J. Neurotrauma 2019, 36, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Levi, A.D.; Okonkwo, D.O.; Park, P.; Jenkins, A.L.; Kurpad, S.N.; Parr, A.M.; Ganju, A.; Aarabi, B.; Kim, D.; Casha, S.; et al. Emerging Safety of Intramedullary Transplantation of Human Neural Stem Cells in Chronic Cervical and Thoracic Spinal Cord Injury. Neurosurgery 2017, 82, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Curt, A.; Hsieh, J.; Schubert, M.; Hupp, M.; Friedl, S.; Freund, P.; Huber, E.; Pfyffer, D.; Sutter, R.; Jutzeler, C.; et al. The Damaged Spinal Cord Is a Suitable Target for Stem Cell Transplantation. Neurorehabilit. Neural Repair 2020, 34, 758–768. [Google Scholar] [CrossRef]
- Shin, J.C.; Kim, K.N.; Yoo, J.; Kim, I.-S.; Yun, S.; Lee, H.; Jung, K.; Hwang, K.; Kim, M.; Lee, I.-S.; et al. Clinical Trial of Human Fetal Brain-Derived Neural Stem/Progenitor Cell Transplantation in Patients with Traumatic Cervical Spinal Cord Injury. Neural Plast. 2015, 2015, 630932. [Google Scholar] [CrossRef] [Green Version]
- Curtis, E.; Martin, J.; Gabel, B.; Sidhu, N.; Rzesiewicz, T.K.; Mandeville, R.; Van Gorp, S.; Leerink, M.; Tadokoro, T.; Marsala, S.; et al. A First-in-Human, Phase I Study of Neural Stem Cell Transplantation for Chronic Spinal Cord Injury. Cell Stem Cell 2018, 22, 941–950.e6. [Google Scholar] [CrossRef] [Green Version]
- Tsukamoto, A.; Uchida, N.; Capela, A.; Gorba, T.; Huhn, S. Clinical translation of human neural stem cells. Stem Cell Res. Ther. 2013, 4, 102. [Google Scholar] [CrossRef] [Green Version]
- Olanow, C.W.; Goetz, C.G.; Kordower, J.H.; Stoessl, A.J.; Sossi, V.; Brin, M.F.; Shannon, K.M.; Nauert, G.M.; Perl, D.P.; Godbold, J.; et al. A double-blind controlled trial of bilateral fetal nigral transplantation in Parkinson’s disease. Ann. Neurol. 2003, 54, 403–414. [Google Scholar] [CrossRef]
- Freed, C.R.; Greene, P.E.; Breeze, R.E.; Tsai, W.-Y.; DuMouchel, W.; Kao, R.; Dillon, S.; Winfield, H.; Culver, S.; Trojanowski, J.Q.; et al. Transplantation of Embryonic Dopamine Neurons for Severe Parkinson’s Disease. N. Engl. J. Med. 2001, 344, 710–719. [Google Scholar] [CrossRef]
- Lima, C.; Escada, P.; Pratas-Vital, J.; Aguiar-Branco, C.; Arcangeli, C.A.; Lazzeri, G.; Maia, C.A.S.; Capucho, C.; Hasse-Ferreira, A.; Peduzzi, J.D. Olfactory Mucosal Autografts and Rehabilitation for Chronic Traumatic Spinal Cord Injury. Neurorehabilit. Neural Repair 2009, 24, 10–22. [Google Scholar] [CrossRef]
- Lima, C.; Pratas-Vital, J.; Escada, P.; Hasse-Ferreira, A.; Capucho, C.; Peduzzi, J.D. Olfactory Mucosa Autografts in Human Spinal Cord Injury: A Pilot Clinical Study. J. Spinal Cord Med. 2006, 29, 191–203; discussion 204–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doucette, R. Olfactory ensheathing cells: Potential for glial cell transplantation into areas of CNS injury. Histol. Histopathol. 1995, 10, 503–507. [Google Scholar]
- Lu, J.; Féron, F.; Ho, S.M.; Mackay-Sim, A.; Waite, P.M. Transplantation of nasal olfactory tissue promotes partial recovery in paraplegic adult rats. Brain Res. 2001, 889, 344–357. [Google Scholar] [CrossRef]
- Xiao, M.; Klueber, K.M.; Zhou, J.; Guo, Z.; Lu, C.; Wang, H.; Roisen, F.J. Human adult olfactory neural progenitors promote axotomized rubrospinal tract axonal reinnervation and locomotor recovery. Neurobiol. Dis. 2007, 26, 363–374. [Google Scholar] [CrossRef]
- Féron, F.; Perry, C.; Cochrane, J.; Licina, P.; Nowitzke, A.; Urquhart, S.; Geraghty, T.; Mackay-Sim, A. Autologous olfactory ensheathing cell transplantation in human spinal cord injury. Brain 2005, 128, 2951–2960. [Google Scholar] [CrossRef] [Green Version]
- Mackay-Sim, A.; Feron, F.; Cochrane, J.; Bassingthwaighte, L.; Bayliss, C.; Davies, W.; Fronek, P.; Gray, C.; Kerr, G.; Licina, P.; et al. Autologous olfactory ensheathing cell transplantation in human paraplegia: A 3-year clinical trial. Brain 2008, 131, 2376–2386. [Google Scholar] [CrossRef] [Green Version]
- Tabakow, P.; Jarmundowicz, W.; Czapiga, B.; Fortuna, W.; Miedzybrodzki, R.; Czyz, M.; Huber, J.; Szarek, D.; Okurowski, S.; Szewczyk, P.; et al. Transplantation of Autologous Olfactory Ensheathing Cells in Complete Human Spinal Cord Injury. Cell Transplant. 2013, 22, 1591–1612. [Google Scholar] [CrossRef]
- Wu, J.; Sun, T.; Ye, C.; Yao, J.; Zhu, B.; He, H. Clinical Observation of Fetal Olfactory Ensheathing Glia Transplantation (OEGT) in Patients with Complete Chronic Spinal Cord Injury. Cell Transplant. 2012, 21, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Saberi, H.; Moshayedi, P.; Aghayan, H.R.; Arjmand, B.; Hosseini, S.-K.; Emami-Razavi, S.-H.; Rahimi-Movaghar, V.; Raza, M.; Firouzi, M. Treatment of chronic thoracic spinal cord injury patients with autologous Schwann cell transplantation: An interim report on safety considerations and possible outcomes. Neurosci. Lett. 2008, 443, 46–50. [Google Scholar] [CrossRef]
- Anderson, K.D.; Guest, J.D.; Dietrich, W.D.; Bunge, M.B.; Curiel, R.; Dididze, M.; Green, B.A.; Khan, A.; Pearse, D.D.; Saraf-Lavi, E.; et al. Safety of Autologous Human Schwann Cell Transplantation in Subacute Thoracic Spinal Cord Injury. J. Neurotrauma 2017, 34, 2950–2963. [Google Scholar] [CrossRef]
- Mínguez-Castellanos, A.; Escamilla-Sevilla, F.; Hotton, G.R.; Toledo-Aral, J.J.; Ortega-Moreno, Á.; Méndez-Ferrer, S.; Martín-Linares, J.M.; Katati, M.J.; Mir, P.; Villadiego, J.; et al. Carotid body autotransplantation in Parkinson disease: A clinical and positron emission tomography study. J. Neurol. Neurosurg. Psychiatry 2007, 78, 825–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brundin, P.; Pogarell, O.; Hagell, P.; Piccini, P.; Widner, H.; Schrag, A.; Kupsch, A.; Crabb, L.; Odin, P.; Gustavii, B.; et al. Bilateral caudate and putamen grafts of embryonic mesencephalic tissue treated with lazaroids in Parkinson’s disease. Brain 2000, 123, 1380–1390. [Google Scholar] [CrossRef] [Green Version]
- Roy, A.B.; Bakay, R.A.E.; Raiser, C.D.; Stover, N.P.; Subramanian, T.; Cornfeldt, M.L.; Schweikert, A.W.; Allen, R.C.; Watts, R. Implantation of Spheramine â in advanced Parkinson’s disease (PD). Front. Biosci. 2004, 9, 592–602. [Google Scholar] [CrossRef]
- Dahbour, S.; Jamali, F.; Alhattab, D.; Al-Radaideh, A.; Ababneh, O.; Al-Ryalat, N.; Al Bdour, M.; Hourani, B.; Msallam, M.; Rasheed, M.; et al. Mesenchymal stem cells and conditioned media in the treatment of multiple sclerosis patients: Clinical, ophthalmological and radiological assessments of safety and efficacy. CNS Neurosci. Ther. 2017, 23, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Venkataramana, N.K.; Bansal, A.; Balaraju, S.; Jan, M.; Chandra, R.; Dixit, A.; Rauthan, A.; Murgod, U.; Totey, S. Ex vivo-expanded autologous bone marrow-derived mesenchymal stromal cells in human spinal cord injury/paraplegia: A pilot clinical study. Cytotherapy 2009, 11, 897–911. [Google Scholar] [CrossRef] [PubMed]
- Mahadeva, A.; Tanasescu, R.; Gran, B. Urinary tract infections in multiple sclerosis: Under-diagnosed and under-treated? A clinical audit at a large University Hospital. Am. J. Clin. Exp. Immunol. 2014, 3, 57–67. [Google Scholar] [PubMed]
- Salameh, A.; Al Mohajer, M.; Daroucihe, R.O. Prevention of urinary tract infections in patients with spinal cord injury. Can. Med. Assoc. J. 2015, 187, 807–811. [Google Scholar] [CrossRef] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Meyer-Moock, S.; Feng, Y.-S.; Maeurer, M.; Dippel, F.-W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Confavreux, C.; Vukusic, S. Natural history of multiple sclerosis: A unifying concept. Brain 2006, 129 Pt 3, 606–616. [Google Scholar] [CrossRef] [Green Version]
- Uccelli, A.; Laroni, A.; Ali, R.; Battaglia, M.A.; Blinkenberg, M.; Brundin, L.; Clanet, M.; Fernandez, O.; Marriott, J.; Muraro, P.; et al. Safety, tolerability, and activity of mesenchymal stem cells versus placebo in multiple sclerosis (MESEMS): A phase 2, randomised, double-blind crossover trial. Lancet Neurol. 2021, 20, 917–929. [Google Scholar] [CrossRef]
- Roberts, T.T.; Leonard, G.R.; Cepela, D.J. Classifications in Brief: American Spinal Injury Association (ASIA) Impairment Scale. Clin. Orthop. Relat. Res. 2016, 475, 1499–1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zariffa, J.; Kramer, J.L.K.; Fawcett, J.; Lammertse, D.; Blight, A.R.; Guest, J.; Jones, L.; Burns, S.; Schubert, M.; Bolliger, M.; et al. Characterization of neurological recovery following traumatic sensorimotor complete thoracic spinal cord injury. Spinal Cord 2010, 49, 463–471. [Google Scholar] [CrossRef]
- Fawcett, J.; Curt, A.; Steeves, J.D.; Coleman, W.P.; Tuszynski, M.H.; Lammertse, D.; Bartlett, P.F.; Blight, A.R.; Dietz, V.; Ditunno, J.; et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: Spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord 2006, 45, 190–205. [Google Scholar] [CrossRef] [Green Version]
- Bakshi, A.; Hunter, C.; Swanger, S.; Lepore, A.; Fischer, I. Minimally invasive delivery of stem cells for spinal cord injury: Advantages of the lumbar puncture technique. J. Neurosurg. Spine 2004, 1, 330–337. [Google Scholar] [CrossRef]
- Petrou, P.; Kassis, I.; Levin, N.; Paul, F.; Backner, Y.; Benoliel, T.; Oertel, F.C.; Scheel, M.; Hallimi, M.; Yaghmour, N.; et al. Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis. Brain 2020, 143, 3574–3588. [Google Scholar] [CrossRef]
- Glass, J.D.; Hertzberg, V.S.; Boulis, N.M.; Riley, J.; Federici, T.; Polak, M.; Bordeau, J.; Fournier, C.; Johe, K.; Hazel, T.; et al. Transplantation of spinal cord–derived neural stem cells for ALS. Neurology 2016, 87, 392–400. [Google Scholar] [CrossRef] [Green Version]
- Petrou, P.; Gothelf, Y.; Argov, Z.; Gotkine, M.; Levy, Y.S.; Kassis, I.; Vaknin-Dembinsky, A.; Ben-Hur, T.; Offen, D.; Abramsky, O.; et al. Safety and Clinical Effects of Mesenchymal Stem Cells Secreting Neurotrophic Factor Transplantation in Patients With Amyotrophic Lateral Sclerosis: Results of Phase 1/2 and 2a Clinical Trials. JAMA Neurol. 2016, 73, 337–344. [Google Scholar] [CrossRef]
- Berry, J.D.; Cudkowicz, M.E.; Windebank, A.J.; Staff, N.P.; Owegi, M.; Nicholson, K.; McKenna-Yasek, D.; Levy, Y.S.; Abramov, N.; Kaspi, H.; et al. NurOwn, phase 2, randomized, clinical trial in patients with ALS. Neurology 2019, 93, e2294–e2305. [Google Scholar] [CrossRef] [Green Version]
- Vaquero, J.; Zurita, M.; Rico, M.A.; Aguayo, C.; Bonilla, C.; Marin, E.; Tapiador, N.; Sevilla, M.; Vazquez, D.; Carballido, J.; et al. Intrathecal administration of autologous mesenchymal stromal cells for spinal cord injury: Safety and efficacy of the 100/3 guideline. Cytotherapy 2018, 20, 806–819. [Google Scholar] [CrossRef]
- Freund, T.F.; Bolam, J.P.; Björklund, A.; Stenevi, U.; Dunnett, S.; Powell, J.F.; Smith, A.D. Efferent synaptic connections of grafted dopaminergic neurons reinnervating the host neostriatum: A tyrosine hydroxylase immunocytochemical study. J. Neurosci. 1985, 5, 603–616. [Google Scholar] [CrossRef] [Green Version]
- Lindvall, O.; Sawle, G.; Widner, H.; Rothwell, J.C.; Björklund, A.; Brooks, D.; Brundin, P.; Frackowiak, R.; Marsden, C.D.; Odin, P.; et al. Evidence for long-term survival and function of dopaminergic grafts in progressive Parkinson’s disease. Ann. Neurol. 1994, 35, 172–180. [Google Scholar] [CrossRef]
- Freed, C.R.; Breeze, R.E.; Rosenberg, N.L.; Schneck, S.A.; Kriek, E.; Qi, J.-X.; Lone, T.; Zhang, Y.-B.; Snyder, J.A.; Wells, T.H.; et al. Survival of Implanted Fetal Dopamine Cells and Neurologic Improvement 12 to 46 Months after Transplantation for Parkinson’s Disease. N. Engl. J. Med. 1992, 327, 1549–1555. [Google Scholar] [CrossRef]
- McGeer, P.L.; Yasojima, K.; McGeer, E.G. Inflammation in Parkinson’s disease. Adv. Neurol. 2001, 86, 83–89. [Google Scholar]
- Piquet, A.L.; Venkiteswaran, K.; Marupudi, N.; Berk, M.; Subramanian, T. The immunological challenges of cell transplantation for the treatment of Parkinson’s disease. Brain Res. Bull. 2012, 88, 320–331. [Google Scholar] [CrossRef] [Green Version]
- Plemel, J.; Liu, W.-Q.; Yong, V.W. Remyelination therapies: A new direction and challenge in multiple sclerosis. Nat. Rev. Drug Discov. 2017, 16, 617–634. [Google Scholar] [CrossRef]
- Lau, L.W.; Cua, R.; Keough, M.B.; Haylock-Jacobs, S.; Yong, V.W. Pathophysiology of the brain extracellular matrix: A new target for remyelination. Nat. Rev. Neurosci. 2013, 14, 722–729. [Google Scholar] [CrossRef]
- Janssens, I.; Cools, N. Regulating the regulators: Is introduction of an antigen-specific approach in regulatory T cells the next step to treat autoimmunity? Cell. Immunol. 2020, 358, 104236. [Google Scholar] [CrossRef]
- Wens, I.; Janssens, I.; Derdelinckx, J.; Meena, M.; Willekens, B.; Cools, N. Made to Measure: Patient-Tailored Treatment of Multiple Sclerosis Using Cell-Based Therapies. Int. J. Mol. Sci. 2021, 22, 7536. [Google Scholar] [CrossRef]
- Ou, K.; Hamo, D.; Schulze, A.; Roemhild, A.; Kaiser, D.; Gasparoni, G.; Salhab, A.; Zarrinrad, G.; Amini, L.; Schlickeiser, S.; et al. Strong Expansion of Human Regulatory T Cells for Adoptive Cell Therapy Results in Epigenetic Changes Which May Impact Their Survival and Function. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef]
- Campillo-Davo, D.; De Laere, M.; Roex, G.; Versteven, M.; Flumens, D.; Berneman, Z.; Van Tendeloo, V.; Anguille, S.; Lion, E. The Ins and Outs of Messenger RNA Electroporation for Physical Gene Delivery in Immune Cell-Based Therapy. Pharmaceutics 2021, 13, 396. [Google Scholar] [CrossRef]
- Janssens, I.; Campillo Davó, D.; Van den Bos, J.; De Reu, H.; Berneman, Z.N.; Wens, I.; Cools, N. Engineering of regulatory T cells by means of mRNA electroporation in a GMP-compliant manner. Cytotherapy 2022, in press. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author + Year | Cell Type | Administration Route | Disease | #Patients | %Improved |
|---|---|---|---|---|---|
| Riordan NH. 2018 | MSC (UC) | IV | MS (RR,PP,SP) | T: 17 | NA |
| Fernández O. 2018 | MSC (Ad) | IV | MS (SP) | T: 19 Co: 10 | T: NA Co: NA |
| Karussis D. 2010 | MSC (BM) | IT | MS (V) | T: 15 | 73 |
| Harris VK. 2018 | MSC (BM) | IT | MS (PP,SP) | T: 20 | 35 |
| Xiao Z. 2018 | MSC (UC) | Injury Site | SCI (A) | T: 2 | 100 |
| Ra JC. 2011 | MSC (Ad) | IV | SCI (C) | T: 8 | 13 |
| El-Kheir WA. 2014 | MSC (BM) | IT | SCI (C) | T: 50 Co: 20 | T: 34 Co: 0 |
| Bonab MM. 2012 | MSC (BM) | IT | MS (SP,PR) | T: 22 | 18 |
| Dahbour S. 2017 | MSC (Ad) | IT | MS (SP,RR) | T: 10 | 20 |
| Lublin FD. 2014 | MSC (PD) | IV | MS (RR,SP) | T: 12 Co: 4 | T: 42 Co: 25 |
| Llufriu S. 2014 | MSC (BM) | IV | MS (RR) | T: 8 | NA |
| Mendonça MV. 2014 | MSC (BM) | Injury Site | SCI (C) | T: 12 | 58 |
| Connick P. 2012 | MSC (BM) | IV | MS (SP) | T: 10 | NA |
| Cheng H. 2014 | MSC (UC) | IT | SCI (C) | T: 10 | NA |
| Li JF. 2014 | MSC (UC) | IV | MS (RR,SP) | T: 13 Co: 10 | T: NA Co: NA |
| Satti HS. 2016 | MSC (BM) | IT | SCI (C) | T: 9 | NA |
| Bonab MM. 2007 | MSC (BM) | IT | MS (SP,PP) | T: 10 | 10 |
| Dai G. 2013 | MSC (BM) | Injury Site | SCI (C) | T: 20 Co: 20 | 45 0 |
| Karamouzian S. 2012 | MSC (BM) | IT | SCI (A,SA) | T: 11 Co: 20 | T: 45 Co: 15 |
| Vaquero J. 2016 | MSC (BM) | IT + Injury site | SCI (C) | T: 12 | 33 |
| Vaquero J. 2017 | MSC (BM) | IT | SCI (C) | T: 10 | NA |
| Vaquero J. 2018 | MSC (BM) | IT | SCI (V) | T: 9 | 79 |
| Oh SK. 2015 | MSC (BM) | Injury site | SCI (C) | T: 16 | NA |
| Hur JW. 2016 | MSC (Ad) | IT | SCI (C) | T: 14 | NA |
| Yamout B. 2010 | MSC (BM) | IT | MS (SP,RR) | T: 7 | 57 |
| Saito F. 2012 | MSC (BM) | IT | SCI (A) | T: 5 | 40 |
| Venktataramana NK. 2010 | MSC (BM) | Surgery | PD | T: 7 | 43 |
| Pal R. 2009 | MSC (BM) | IT | SCI (C) | T: 25 | 0 |
| Saito F. 2008 | MSC (BM) | IT | SCI (A) | T: 1 | 0 |
| Duma C. 2019 | MSC (Ad) | CSF | SCI,MS,PD,AD | T: 31 | NA |
| Kim HJ. 2015 | MSC (UC) | Surgery | AD | T: 9 | 0 |
| Petrou P. 2020 | MSC (BM) | IT or IV | MS (SP,PP) | T: 32 Co: 16 | T: NA Co: NA |
| Petrou P. 2021 | MSC (BM) | IT and/or IV | MS (SP,PP) | T: 24 | 42 |
| Uccelli A. 2021 | MSC (BM) | IV | MS (RR,SP,PP) | T: 69 Co: 75 | T: 15 Co: 14 |
| Bhanot Y. 2011 | MSC (BM) | IT + Injury site | SCI (C) | T: 13 | 8 |
| Yazdani OS. 2016 | MSC (BM) + SC | IT | SCI (C) | T: 6 | 17 |
| Zhao Y. 2017 | MSC (UC) | Injury site | SCI (C) | T: 8 | 0 |
| Deng WS. 2020 | MSC (UC) | Injury site | SCI (A) | T: 20 Co: 20 | T: 55 Co: 0 |
| Amr SM. 2014 | MSC (BM) | Injury site | SCI (C) | T: 14 | 100 |
| Rong L. 2020 | MSC (UC) | IT | SCI (C) | T: 24 | NA |
| Moviglia GA. 2006 | MSC (BM) | Injury site | SCI (C) | T: 2 | NA |
| Carstens M. 2020 | MSC (Ad) | Facial | PD | T: 2 | NA |
| Rice CM. 2010 | BMMC | IV | MS (RP) | T: 6 | 0 |
| Chhabra HS. 2016 | BMMC | IT + Injury site | SCI (A) | T: 14 Co: 7 | NA NA |
| Kumar AA. 2009 | BMMC | IT | SCI (C) | T: 297 | 33 |
| Yoon SH. 2007 | BMMC | Injury site | SCI (V) | T: 35 Co: 13 | T: 20 Co: 8 |
| Chernykh ER. 2007 | BMMC | IV + Injury site | SCI (C) | T: 18 Co: 18 | NA NA |
| Syková E. 2006 | BMMC | IV + IA | SCI (V) | T: 20 | 15 |
| Park HC. 2005 | BMMC | Injury site | SCI (A) | T: 6 | 83 |
| Attar A. 2011 | BMMC | Injury site | SCI (A) | T: 4 | 75 |
| Lima C. 2006 | OMA | Injury site | SCI (C) | T: 7 | 29 |
| Lima C. 2009 | OMA | Injury site | SCI (C) | T: 20 | 30 |
| Curtis E. 2018 | NSC | Injury site | SCI (C) | T: 4 | NA |
| Levi AD. 2018 | NSC | Injury site | SCI (C) | T: 39 | NA |
| Levi AD. 2019 | NSC | Injury site | SCI (C) | T: 12 Co: 4 | NA NA |
| Shin JC. 2015 | NSC | Injury site | SCI (V) | T: 19 Co: 15 | T: 26 Co: 7 |
| Curt A. 2020 | NSC | Injury site | SCI (C) | T: 14 | 14 |
| Mackay-Sim A. 2008 | OEC | Injury site | SCI (C) | T: 3 Co: 3 | T: 0 Co: 0 |
| Féron F. 2005 | OEC | Injury site | SCI (C) | T: 3 Co: 3 | NA NA |
| Tabakow P. 2013 | OEC | Injury site | SCI (C) | T: 3 Co: 3 | T: 67 Co: 0 |
| Wu J. 2012 | OEC | Injury site | SCI (C) | T: 11 | NA |
| Saberi H. 2008 | Schwann | Injury site | SCI (C) | T: 4 | 25 |
| Anderson KD. 2017 | Schwann | Injury Site | SCI (C) | T: 6 | 17 |
| Freed CR. 2001 | Neuron | Surgery | PD | T: 20 Co: 20 | T: NA Co: NA |
| Minguez-Castellanos 2007 | Carotic Body | Surgery | PD | T: 12 | 83 |
| Brundin P. 2000 | Mesencephalic | Surgery | PD | T: 5 | 80 |
| Al-Zoubi A. 2014 | PBSC | IT + Injury site | SCI (C) | T: 19 | 37 |
| Christante AF. 2009 | PBSC | IA | SCI (C) | T: 39 | NA |
| Lammertse DP. 2012 | Macrophage | Injury site | SCI (A) | T: 19 Co: 14 | T: 26 Co: 57 |
| Knoller N. 2005 | Macrophage | Injury site | SCI (A) | T: 8 | 38 |
| Bakay RAE. 2004 | Spheramine © | Surgery | PD | T: 6 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van den Bos, J.; Ouaamari, Y.E.; Wouters, K.; Cools, N.; Wens, I. Are Cell-Based Therapies Safe and Effective in the Treatment of Neurodegenerative Diseases? A Systematic Review with Meta-Analysis. Biomolecules 2022, 12, 340. https://doi.org/10.3390/biom12020340
Van den Bos J, Ouaamari YE, Wouters K, Cools N, Wens I. Are Cell-Based Therapies Safe and Effective in the Treatment of Neurodegenerative Diseases? A Systematic Review with Meta-Analysis. Biomolecules. 2022; 12(2):340. https://doi.org/10.3390/biom12020340
Chicago/Turabian StyleVan den Bos, Jasper, Yousra El Ouaamari, Kristien Wouters, Nathalie Cools, and Inez Wens. 2022. "Are Cell-Based Therapies Safe and Effective in the Treatment of Neurodegenerative Diseases? A Systematic Review with Meta-Analysis" Biomolecules 12, no. 2: 340. https://doi.org/10.3390/biom12020340