
Neuropathic and Psychogenic Components of Burning Mouth Syndrome: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction
2.5. Data Analysis/Statistical Analysis
3. Results
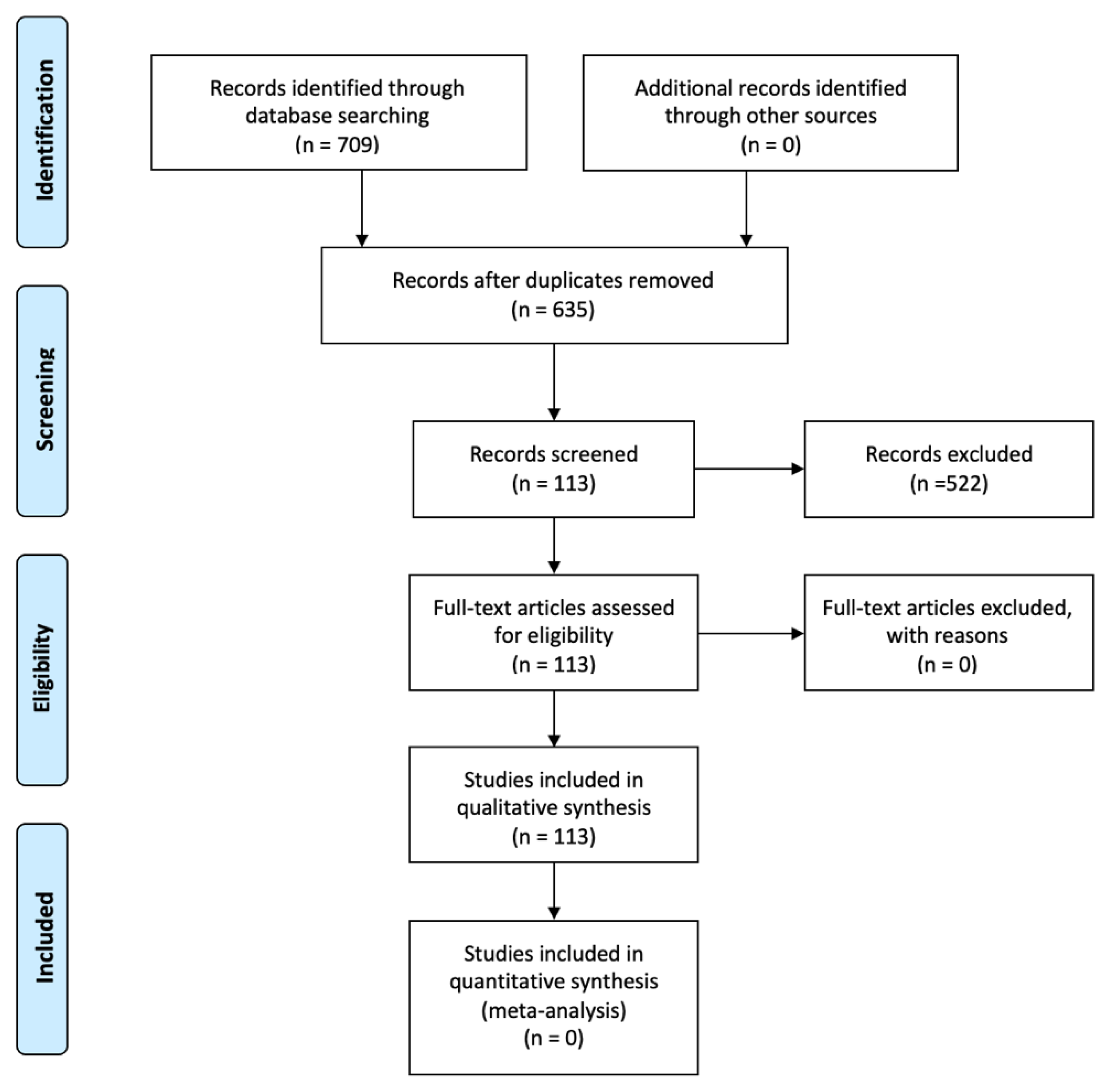
3.1. Study Selection
3.2. Study Characteristics
3.3. Pharmacological and Non-Pharmacological Management Studies
3.3.1. Low Level Laser Therapy (LLLT)
3.3.2. Alpha-Lipoic Acid (ALA)
3.3.3. Capsaicin
3.3.4. Other Pharmacological Treatments
3.4. Neurophysiological Studies
3.4.1. Quantitative Sensory Testing (QST)
3.4.2. Other Neurophysiological Studies
3.4.3. Functional Brain Imaging
3.5. Bio-Histopathological Study
3.5.1. Cytokine Levels
3.5.2. Histological Studies
3.5.3. Other Biological Studies
3.6. Questionnaire-Based Studies

{kind=link}
{kind=link}
| Author/Year | Questionnaire(s) | Significant Results |
|---|---|---|
| Acharya, 2018 [124] | OHIP-14 (Oral Health Impact Profile-14) | OHIP 14 significantly poorer for the BMS group (p < 0.001) |
| Adamo, 2020 [113] | GOHAI (Geriatric Oral Health Assessment Index) OHIP-14 (Oral Health Impact Profile-14) VAS (Visual Analogue Scale) HAM-D and HAM-A (Hamilton Rating Scales for Depression and Anxiety) | Scores from all outcome measurements statistically different between the cases and controls (p < 0.001) with a strong correlation between the GOHAI and the OHIP-14 (p < 0.001). BMS patients: significant improvement in the VAS, HAM-D and HAM-A scores from time 0 to time 1 (p < 0.001), and in the OHIP-14 scores (p < 0.004) after the psychotropic drugs treatment |
| Bogetto, 1998 [121] | BPRS (Brief Psychiatric Rating Scale) | Higher mean BPRS total score (p < 0.005) Higher psychiatric disorders frequency (p < 0.001) |
| Braud, 2013 [130] | DN4 questionnaire VAS (Visual Analogue Scale) | DN4 scores ranged from 2 to 7 (mean score: 3.9 ± 0.3) 59% of the patients: DN4 score ≥ 4. The findings support the use of DN4 as a tool for screening BMS and reinforce the view that BMS is a clinical manifestation of a neuropathic disease |
| Carlson, 2000 [112] | McGill Pain Questionnaire MPI (Multidimensional Pain Inventory) SCL-90R (Symptom Checklist-90-Revised) | Patients did not report significant psychologic distress. Individual cases (7 of 33, or 21%): psychometric data indicated a likelihood of psychologic distress. |
| das Neves de Araújo Lima, 2016 [115] | Lipp’s Inventory of Stress Symptoms for Adults Beck Depression and Anxiety Inventory | Significant differences between groups, which were more prevalent in the BMS group: —in the presence of xerostomia (p = 0.01), —hyposalivation at rest (p < 0.001), —symptoms of depression (p = 0.033). |
| Eli, 1994 [6] | SCL-90 R questionnaire (General Symptomatic Index (GSI), Positive Symptom Total (PST), and Positive Symptom Distress Index (PSDI)) | —Higher psychopathologic profile, especially on the scales of somatization and depression. —Significant correlations between the intensity of pain experienced by the patients and some of the SCL-90 scales (somatization, depression, anxiety, GSI, and PSDI). |
| Forssell, 2020 [122] | DEPS (Self-rating Depression Scale) PASS-20 (Pain Anxiety Symptom Scale-20) PVAQ (Pain Vigilance and Awareness Questionnaire) | Patients were divided into groups based on pain severity distribution tertiles: low intensity (NRS ≤ 3.7) or interference (NRS ≤ 2.9) (tertiles 1–2, n = 35) and moderate to intense intensity (NRS > 3.7) or interference (>2.9) (tertile 3, n = 17). Patients in the highest intensity and interference tertiles reported more depression (p = 0.0247 and p = 0.0169) and pain anxiety symptoms (p = 0.0359 and p = 0.0293), and were more preoccupied with pain (p = 0.0004 and p = 0.0003) than patients in the low intensity and interference groups. The score of the pain vigilance questionnaire correlated significantly with pain intensity (p = 0.009) and interference (p = 0.009). Depression (p = 0.003) and pain anxiety symptoms (p = 0.001) correlated with pain interference. |
| Galli, 2017 [23] | Meta-Analysis | All studies but one reported at least some evidence for the involvement of psychological factors in BMS. Anxiety and depression were the most common and the most frequently studied psychopathological disorders among BMS patients. |
| Heo, 2015 [129] | PainDETECT (neuropathic pain questionnaire) DN4, and abbreviated DN4 (DN4i) | Total scores for PainDETECT, DN4, and DN4i in the primary BMS group were significantly associated with pain intensity. |
| Jedel, 2020 [127] | SSP (Swedish universities scales of personality) PSQ (Perceived stress questionnaire) | SSP: subscales Somatic Trait Anxiety, Psychic Trait Anxiety, Stress Susceptibility and Verbal Trait Aggression differed between BMS and controls and the personality factor scores for Neuroticism and Aggressiveness were higher. PSQ: Higher perceived stress. |
| Jerlang, 1997 [116] | Beck’s depression inventory of 42 items Spielberger’s State-Trait Anxiety Scale TAS-20 (Toronto Alexithymic scale questionnaire) | Significant correlations between disability and alexithymic traits (p < 0.05), depressive traits (p < 0.001), state-anxiety (p < 0.05), trait-anxiety (p < 0.05) and VAS well-being (p < 0.01). |
| Kim, 2018 [110] | SCL-90-R (Symptom Checklist-90-Revised) | Patients with psychological problems: —Higher mean age, reduced stimulated whole saliva flow rate, and lower level of education than those without psychological problems —Higher rates and greater severity of various types of BMS-related symptom in most parts of the oral mucosa, higher rates of stress-related symptoms, and greater difficulties in daily activities Psychological problems in BMS patients are associated with an aggravation of BMS symptoms |
| Komiyama, 2012 [128] | Research Diagnostic Criteria for Temporomandibular Disorders | Chronic BMS patients: —Higher somatization score than those with acute BMS (p = 0.027) —Higher depression scores than those with acute BMS (p = 0.001). |
| Lopez-Jornet, 2015 [106] | HADS (Hospital Anxiety and Depression Scale) OHIP-14 (Oral Health Impact Profile-14) PSQI (Pittsburgh Sleep quality index) EES (Epworth Sleepiness Scale) | HADS: Higher level of anxiety (p = 0.008) and depression (p = 0.005) OHIP-14: no significant result Higher poor sleep quality in BMS patients (p ≤ 0.001). Anxiety and depression were identified as significant determinants of poor sleep quality |
| Lopez-Jornet, 2017 [109] | PainDETECT (neuropathic pain questionnaire) HADS (Hospital Anxiety and Depression Scale), VAS (Visual Analogue Scale) | Pain-VAS: Higher in BMS group PainDETECT obtained total scores >19 in 21% of BMS patients, indicating the presence of neuropathic pain Almost a third of BMS patients present neuropathic pain, which is strongly associated with the intensity of pain measured using VAS. |
| Malik, 2012 [107] | HADS (Hospital Anxiety and Depression Scale) GHQ-28 (General Health Questionnaire-28) VAS (Visual Analogue Scale) | Significant increase in the levels of anxiety and depression in the BMS group. |
| Marino, 2015 [114] | TAS-20 (Toronto Alexithymic scale questionnaire) HAM-A (Hamilton Rating Scales for Anxiety) Montgomery–Asberg Depression Rating Scale | 79.3% of alexithymic patients (vs. 6.9%) (p < 0.001) |
| Merigo, 2007 [126] | MMPI-II (Minnesota Multiphasic Personality Inventory-2) | No significant differences on the MMPI-II scales |
| Mignogna, 2011 [132] | Oral symptoms collected by specialist in oral medicine and general dentist. Data concerning unexplained extraoral symptoms gathered by each specialist ward, i.e., ophthalmology, gynaecology, otolaryngology, gastroenterology, neurology, cardiology, internal medicine, and dermatology. | BMS group: —98 (96.1%) patients reported unexplained extraoral symptoms. —4 (3.9%) patients reported only oral symptoms. —Higher painful symptomatology in different bodily regions frequency (p < 0.0001). The differences in the overall unexplained extraoral symptoms between BMS (96.1%) and OLP patients (9.3%) (p < 0.0001) and between BMS (96.1%) and healthy patients (15.7%) (p < 0.0001) were statistically significant. |
| Miyaoka, 1996 [123] | EPQ (Eysenck Personality Questionnaire) TAS (Toronto Alexithymia Scale) GHQ (General Health Questionnaire) | EPQ: significantly lower on BMS patients TAS: significantly higher on BMS patients GHQ: no significant difference |
| Ott, 1992 [120] | Erlangen depression scale Scale for general somatic symptoms Anxiety-aggression scale Self-rating scale for state of wellbeing Self-rating depression scale | Psychiatrically relevant disorder, usually depression, for the majority of BMS patients |
| Schiavone, 2012 [111] | SCL-90-R (Symptom Checklist-90-Revised) STAI (State-Trait Anxiety Inventory Form Y 1–2) HAM-D (Hamilton Rating Scale for Depression) | —STAI: higher scores of anxiety (STAI Y1, p = 0.026 and STAI Y2, p = 0.046). —HAM-D: higher scores of depression (p < 0.001). —SCL-90-R: higher scores on somatization (p = 0.036) and hostility dimensions (p = 0.028). Pain is affected by depression (p < 0.005). Depression is affected by anxiety (p < 0.001). |
| Sevrain, 2016 [108] | DN4i HADS (Hospital Anxiety and Depression Scale) QDSA (French adaptation of the McGill Pain Questionnaire) | —31% had a DN4i score in favour of neuropathic pain. —34.3% had a HADS overall score in favour of anxiety and depressive disorder. |
| Taiminen, 2011 [125] | SCID-I and II (Structured Clinical Interview for DSM-IV) | No differences in the rates of psychiatric and personality disorders between BMS and AFP patients. |
| Takenoshita, 2010 [118] | ICD-10 (International Statistical Classification of Disease and Related Health Problems, Tenth Revision (F0–F9)) Zung’s Self-Rating Depression Scale SF-MPQ (Short-form Mcgill Pain Questionnaire) Present Pain Intensity (PPI) scale | The proportion of F4 classification (neurotic, stress-related, and somatoform disorders) in AO patients was significantly higher than in BMS patients. BMS patients were more frequently given a F3 classification (mood/affective disorders). 50.8% of BMS patients and 33.3% of AO patients had no specific psychiatric diagnoses. Depression rating: —21.4%: normal; —46.4%: neurotic tendency; —32.1%: depressive tendency. |
| Tokura, 2015 [117] | TCI (Temperament and Character Inventory) BDI (Beck Depression Inventory) | TCI: —Lower novelty seeking (NS) (p = 0.009); —Lower self-directedness (p = 0.039); —Higher harm avoidance (p < 0.001). BDI: Higher depression level |
| Trikkas, 1996 [7] | Zung’s Self-Rating Scale for Depression STAI (Spielberger’s State-Trait Anxiety Inventory) EPQ (Eysenck’s Personality Questionnaire) HDHQ (Fould’s Hostility and Direction of Hostility Questionnaire) SSPS (Schalling–Sifneos’ Personality Scale) | —Significantly higher values in the N (neuroticism) and the L (lie) factors of the EPQ. —Significantly higher rates of psychosomatic morbidity. —Significantly differentiated from controls with respect to all factors of HDHQ. |
| Tu, 2018 [119] | Short-Form McGill Pain Questionnaire (SF-MPQ) Zung Self-Rating Depression Scale | AO-BMS patients rated overall pain score and present pain intensity significantly higher than did the AO-only patients (p = 0.033 and p = 0.034). Patients having comorbid psychiatric disorders had a higher proportion of sleep disturbance in both groups and a higher proportion of depressive state in the AO-only group. |
| Zakrzewska, 2019 [131] | Visual Imagery investigate how photographic images (Pain Cards) co-created by an artist and chronic pain patients could be used in groups of patients with burning mouth syndrome to facilitate characterization of their pain and its impact on quality of life. | The choice of Pain Card and words used to explain the choice implied a neuropathic type of pain. Themes that were common included those of isolation, loss of confidence, low mood, and decrease in activities and socialization. |
4. Discussion
4.1. Arguments for Neuropathic Pathogenesis
4.2. Arguments for a Psychogenic Pathogenesis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Jaaskelainen, S.K. Pathophysiology of primary burning mouth syndrome. Clin. Neurophysiol. 2012, 123, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Grushka, M.; Epstein, J.B.; Gorsky, M. Burning mouth syndrome. Am. Fam. Physician 2002, 65, 615–620. [Google Scholar]
- Formaker, B.K.; Frank, M.E. Taste function in patients with oral burning. Chem. Senses. 2000, 25, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Scala, A.; Checchi, L.; Montevecchi, M.; Marini, I.; Giamberardino, M.A. Update on burning mouth syndrome: Overview and patient management. Crit. Rev. Oral Biol. Med. 2003, 14, 275–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eli, I.; Baht, R.; Littner, M.M.; Kleinhauz, M. Detection of psychopathologic trends in glossodynia patients. Psychosom. Med. 1994, 56, 389–394. [Google Scholar] [CrossRef]
- Trikkas, G.; Nikolatou, O.; Samara, C.; Bazopoulou-Kyrkanidou, E.; Rabavilas, A.D.; Christodoulou, G.N. Glossodynia: Personality characteristics and psychopathology. Psychother. Psychosom. 1996, 65, 163–168. [Google Scholar] [CrossRef]
- Eli, I.; Kleinhauz, M.; Baht, R.; Littner, M. Antecedents of burning mouth syndrome (glossodynia)—Recent life events vs. psychopathologic aspects. J. Dent. Res. 1994, 73, 567–572. [Google Scholar] [CrossRef]
- Albuquerque, R.J.; de Leeuw, R.; Carlson, C.R.; Okeson, J.P.; Miller, C.S.; Andersen, A.H. Cerebral activation during thermal stimulation of patients who have burning mouth disorder: An fMRI study. Pain 2006, 122, 223–234. [Google Scholar] [CrossRef]
- Jääskeläinen, S.K. Clinical neurophysiology and quantitative sensory testing in the investigation of orofacial pain and sensory function. J. Orofac. Pain 2004, 18, 85–107. [Google Scholar]
- Lauria, G.; Majorana, A.; Borgna, M.; Lombardi, R.; Penza, P.; Padovani, A.; Sapelli, P. Trigeminal small-fiber sensory neuropathy causes burning mouth syndrome. Pain 2005, 115, 332–337. [Google Scholar] [CrossRef]
- Jääskeläinen, S.K.; Forssell, H.; Tenovuo, O. Abnormalities of the blink reflex in burning mouth syndrome. Pain 1997, 73, 455–460. [Google Scholar] [CrossRef]
- Yilmaz, Z.; Renton, T.; Yiangou, Y.; Zakrzewska, J.; Chessell, I.P.; Bountra, C.; Anand, P. Burning mouth syndrome as a trigeminal small fibre neuropathy: Increased heat and capsaicin receptor TRPV1 in nerve fibres correlates with pain score. J. Clin. Neurosci. 2007, 14, 864–871. [Google Scholar] [CrossRef]
- Orofacial, T. International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia 2020, 40, 129–221. [Google Scholar] [CrossRef] [Green Version]
- Zakrzewska, J.M.; Forssell, H.; Glenny, A.M. Interventions for the treatment of burning mouth syndrome. Cochrane Database Syst. Rev. 2005, CD002779. [Google Scholar] [CrossRef]
- Slebioda, Z.; Lukaszewska-Kuska, M.; Dorocka-Bobkowska, B. Evaluation of the efficacy of treatment modalities in burning mouth syndrome-A systematic review. J. Oral Rehabil. 2020, 47, 1435–1447. [Google Scholar] [CrossRef] [PubMed]
- McMillan, R.; Forssell, H.; Buchanan, J.A.; Glenny, A.M.; Weldon, J.C.; Zakrzewska, J.M. Interventions for treating burning mouth syndrome. Cochrane Database Syst. Rev. 2016, 11, CD002779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kisely, S.; Forbes, M.; Sawyer, E.; Black, E.; Lalloo, R. A systematic review of randomized trials for the treatment of burning mouth syndrome. J. Psychosom. Res. 2016, 86, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Haggman-Henrikson, B.; Alstergren, P.; Davidson, T.; Hogestatt, E.D.; Ostlund, P.; Tranaeus, S.; Vitols, S.; List, T. Pharmacological treatment of oro-facial pain-health technology assessment including a systematic review with network meta-analysis. J. Oral Rehabil. 2017, 44, 800–826. [Google Scholar] [CrossRef] [PubMed]
- De Pedro, M.; Lopez-Pintor, R.M.; de la Hoz-Aizpurua, J.L.; Casanas, E.; Hernandez, G. Efficacy of Low-Level Laser Therapy for the Therapeutic Management of Neuropathic Orofacial Pain: A Systematic Review. J. Oral Facial Pain Headache 2020, 34, 13–30. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Javed, F.; Kalakonda, B.; AlAizari, N.A.; Al-Soneidar, W.; Al-Akwa, A. Efficacy of low level laser therapy in the treatment of burning mouth syndrome: A systematic review. Photodiagnosis Photodyn. Ther. 2017, 17, 188–193. [Google Scholar] [CrossRef]
- Liu, Y.F.; Kim, Y.; Yoo, T.; Han, P.; Inman, J.C. Burning mouth syndrome: A systematic review of treatments. Oral Dis. 2018, 24, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Galli, F.; Lodi, G.; Sardella, A.; Vegni, E. Role of psychological factors in burning mouth syndrome: A systematic review and meta-analysis. Cephalalgia 2017, 37, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Madariaga, V.I.; Tanaka, H.; Ernberg, M. Psychophysical characterisation of burning mouth syndrome-A systematic review and meta-analysis. J. Oral Rehabil. 2020, 47, 1590–1605. [Google Scholar] [CrossRef] [PubMed]
- Moisset, X.; Calbacho, V.; Torres, P.; Gremeau-Richard, C.; Dallel, R. Co-occurrence of Pain Symptoms and Somatosensory Sensitivity in Burning Mouth Syndrome: A Systematic Review. PLoS ONE 2016, 11, e0163449. [Google Scholar] [CrossRef]
- Catley, M.J.; O’Connell, N.E.; Berryman, C.; Ayhan, F.F.; Moseley, G.L. Is tactile acuity altered in people with chronic pain? A systematic review and meta-analysis. J. Pain 2014, 15, 985–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishore, J.; Shaikh, F.; Mirza, S.; Raffat, M.A.; Ikram, S.; Akram, Z. Cytokine levels and their role in the etiopathogenesis of Burning Mouth Syndrome: A systematic review. Cephalalgia 2019, 39, 1586–1594. [Google Scholar] [CrossRef]
- Da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, N.G.; Gonzaga, A.K.G.; de Sena Fernandes, L.L.; da Fonseca, A.G.; Queiroz, S.; Lemos, T.; da Silveira, E.J.D.; de Medeiros, A.M.C. Evaluation of laser therapy and alpha-lipoic acid for the treatment of burning mouth syndrome: A randomized clinical trial. Lasers Med. Sci. 2018, 33, 1255–1262. [Google Scholar] [CrossRef]
- Arbabi-Kalati, F.; Bakhshani, N.M.; Rasti, M. Evaluation of the efficacy of low-level laser in improving the symptoms of burning mouth syndrome. J. Clin. Exp. Dent. 2015, 7, e524–e527. [Google Scholar] [CrossRef]
- Spanemberg, J.C.; Lopez Lopez, J.; de Figueiredo, M.A.; Cherubini, K.; Salum, F.G. Efficacy of low-level laser therapy for the treatment of burning mouth syndrome: A randomized, controlled trial. J. Biomed. Opt. 2015, 20, 098001. [Google Scholar] [CrossRef]
- Spanemberg, J.C.; Segura-Egea, J.J.; Rodriguez-de Rivera-Campillo, E.; Jane-Salas, E.; Salum, F.G.; Lopez-Lopez, J. Low-level laser therapy in patients with Burning Mouth Syndrome: A double-blind, randomized, controlled clinical trial. J. Clin. Exp. Dent. 2019, 11, e162–e169. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, S.; Lopez-Jornet, P. Effects of low-level laser therapy on burning mouth syndrome. J. Oral Rehabil. 2017, 44, 125–132. [Google Scholar] [CrossRef]
- Bardellini, E.; Amadori, F.; Conti, G.; Majorana, A. Efficacy of the photobiomodulation therapy in the treatment of the burning mouth syndrome. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e787–e791. [Google Scholar] [CrossRef] [PubMed]
- Arduino, P.G.; Cafaro, A.; Garrone, M.; Gambino, A.; Cabras, M.; Romagnoli, E.; Broccoletti, R. A randomized pilot study to assess the safety and the value of low-level laser therapy versus clonazepam in patients with burning mouth syndrome. Lasers Med. Sci. 2016, 31, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Vcev, A.; Siber, S.; Vucicevic Boras, V.; Rotim, Z.; Matijevic, M. The Efficacy of Low-Level Laser Therapy in Burning Mouth Syndrome—A Pilot Study. Acta Clin. Croat. 2018, 57, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Pezelj-Ribaric, S.; Kqiku, L.; Brumini, G.; Urek, M.M.; Antonic, R.; Kuis, D.; Glazar, I.; Stadtler, P. Proinflammatory cytokine levels in saliva in patients with burning mouth syndrome before and after treatment with low-level laser therapy. Lasers Med. Sci. 2013, 28, 297–301. [Google Scholar] [CrossRef] [PubMed]
- De Pedro, M.; Lopez-Pintor, R.M.; Casanas, E.; Hernandez, G. Effects of photobiomodulation with low-level laser therapy in burning mouth syndrome: A randomized clinical trial. Oral Dis. 2020, 26, 1764–1776. [Google Scholar] [CrossRef]
- Cavalcanti, D.R.; da Silveira, F.R. Alpha lipoic acid in burning mouth syndrome—A randomized double-blind placebo-controlled trial. J. Oral Pathol. Med. 2009, 38, 254–261. [Google Scholar] [CrossRef]
- Carbone, M.; Pentenero, M.; Carrozzo, M.; Ippolito, A.; Gandolfo, S. Lack of efficacy of alpha-lipoic acid in burning mouth syndrome: A double-blind, randomized, placebo-controlled study. Eur. J. Pain 2009, 13, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Femiano, F.; Scully, C. Burning mouth syndrome (BMS): Double blind controlled study of alpha-lipoic acid (thioctic acid) therapy. J. Oral Pathol. Med. 2002, 31, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, M.R.; Pedersen, A.M. Analgesic effect of topical oral capsaicin gel in burning mouth syndrome. Acta Odontol. Scand. 2017, 75, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Petruzzi, M.; Lauritano, D.; De Benedittis, M.; Baldoni, M.; Serpico, R. Systemic capsaicin for burning mouth syndrome: Short-term results of a pilot study. J. Oral Pathol. Med. 2004, 33, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Formaker, B.K.; Mott, A.E.; Frank, M.E. The effects of topical anesthesia on oral burning in burning mouth syndrome. Ann. N. Y. Acad. Sci 1998, 855, 776–780. [Google Scholar] [CrossRef]
- Kato, I.T.; Pellegrini, V.D.; Prates, R.A.; Ribeiro, M.S.; Wetter, N.U.; Sugaya, N.N. Low-level laser therapy in burning mouth syndrome patients: A pilot study. Photomed. Laser. Surg. 2010, 28, 835–839. [Google Scholar] [CrossRef]
- Romeo, U.; Del Vecchio, A.; Capocci, M.; Maggiore, C.; Ripari, M. The low level laser therapy in the management of neurological burning mouth syndrome. A pilot study. Ann. Stomatol. 2010, 1, 14–18. [Google Scholar]
- Dos Santos Lde, F.; Carvalho Ade, A.; Leao, J.C.; Cruz Perez, D.E.; Castro, J.F. Effect of low-level laser therapy in the treatment of burning mouth syndrome: A case series. Photomed. Laser Surg. 2011, 29, 793–796. [Google Scholar] [CrossRef]
- Yang, H.W.; Huang, Y.F. Treatment of burning mouth syndrome with a low-level energy diode laser. Photomed. Laser Surg. 2011, 29, 123–125. [Google Scholar] [CrossRef]
- Valenzuela, S.; Pons-Fuster, A.; Lopez-Jornet, P. Effect of a 2% topical chamomile application for treating burning mouth syndrome: A controlled clinical trial. J. Oral Pathol. Med. 2016, 45, 528–533. [Google Scholar] [CrossRef]
- Saraceno, R.; Lorè, B.; Pavlidis, A.; Karaiskou, M.; Arcuri, C.; Chimenti, S.; Magnato, R. Cyclosporine: A novel therapeutic approach for Burning Mouth Syndrome. G. Ital. Dermatol. Venereol. 2016, 151, 480–484. [Google Scholar] [PubMed]
- Hartmann, A.; Seeberger, R.; Bittner, M.; Rolke, R.; Welte-Jzyk, C.; Daublander, M. Profiling intraoral neuropathic disturbances following lingual nerve injury and in burning mouth syndrome. BMC. Oral Health 2017, 17, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, Z.; Egbuniwe, O.; Renton, T. The Detection of Small-Fiber Neuropathies in Burning Mouth Syndrome and Iatrogenic Lingual Nerve Injuries: Use of Quantitative Sensory Testing. J. Oral Facial Pain Headache 2016, 30, 87–98. [Google Scholar] [CrossRef]
- Honda, M.; Iida, T.; Kamiyama, H.; Masuda, M.; Kawara, M.; Svensson, P.; Komiyama, O. Mechanical sensitivity and psychological factors in patients with burning mouth syndrome. Clin. Oral Investig. 2019, 23, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Forssell, H.; Jääskeläinen, S.; Tenovuo, O.; Hinkka, S. Sensory dysfunction in burning mouth syndrome. Pain 2002, 99, 41–47. [Google Scholar] [CrossRef]
- Kolkka, M.; Forssell, H.; Virtanen, A.; Puhakka, A.; Pesonen, U.; Jaaskelainen, S.K. Neurophysiology and genetics of burning mouth syndrome. Eur. J. Pain 2019, 23, 1153–1161. [Google Scholar] [CrossRef]
- Mo, X.; Zhang, J.; Fan, Y.; Svensson, P.; Wang, K. Thermal and mechanical quantitative sensory testing in Chinese patients with burning mouth syndrome--a probable neuropathic pain condition? J. Headache Pain 2015, 16, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Noma, N.; Sekine, N.; Takanezawa, D.; Hirota, C.; Eliav, E.; Imamura, Y. Association of somatosensory dysfunction with symptom duration in burning mouth syndrome. Clin. Oral Investig. 2019, 23, 3471–3477. [Google Scholar] [CrossRef]
- Yang, G.; Su, S.; Jie, H.; Baad-Hansen, L.; Wang, K.; Yan, S.; Liu, H.; Xie, Q.F.; Svensson, P. Somatosensory Profiling of Patients with Burning Mouth Syndrome and Correlations with Psychologic Factors. J. Oral Facial Pain Headache 2019, 33, 278–286. [Google Scholar] [CrossRef]
- Moura, B.S.; Ferreira, N.D.R.; DosSantos, M.F.; Janini, M.E.R. Changes in the vibration sensitivity and pressure pain thresholds in patients with burning mouth syndrome. PLoS ONE 2018, 13, e0197834. [Google Scholar] [CrossRef]
- Kaplan, I.; Levin, T.; Papoiu, A.D.; Patel, N.; Patel, T.; Calderon, S.; Littner, M.; McGlone, F.; Yosipovitch, G. Thermal sensory and pain thresholds in the tongue and chin change with age, but are not altered in burning mouth syndrome. Skin Res. Technol. 2011, 17, 196–200. [Google Scholar] [CrossRef]
- Momota, Y.; Takano, H.; Kani, K.; Matsumoto, F.; Motegi, K.; Aota, K.; Yamamura, Y.; Omori, M.; Tomioka, S.; Azuma, M. Frequency analysis of heart rate variability: A useful assessment tool of linearly polarized near-infrared irradiation to stellate ganglion area for burning mouth syndrome. Pain Med. 2013, 14, 351–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koszewicz, M.; Mendak, M.; Konopka, T.; Koziorowska-Gawron, E.; Budrewicz, S. The characteristics of autonomic nervous system disorders in burning mouth syndrome and Parkinson disease. J. Orofac. Pain 2012, 26, 315–320. [Google Scholar] [PubMed]
- Gremeau-Richard, C.; Dubray, C.; Aublet-Cuvelier, B.; Ughetto, S.; Woda, A. Effect of lingual nerve block on burning mouth syndrome (stomatodynia): A randomized crossover trial. Pain 2010, 149, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Braud, A.; Descroix, V.; Ungeheuer, M.N.; Rougeot, C.; Boucher, Y. Taste function assessed by electrogustometry in burning mouth syndrome: A case-control study. Oral Dis. 2017, 23, 395–402. [Google Scholar] [CrossRef]
- Bonenfant, D.; Rompre, P.H.; Rei, N.; Jodoin, N.; Soland, V.L.; Rey, V.; Brefel-Courbon, C.; Ory-Magne, F.; Rascol, O.; Blanchet, P.J. Characterization of Burning Mouth Syndrome in Patients with Parkinson’s Disease. J. Oral Facial Pain Headache 2016, 30, 318–322. [Google Scholar] [CrossRef] [Green Version]
- De Siqueira, S.R.; Teixeira, M.J.; de Siqueira, J.T. Somatosensory investigation of patients with orofacial pain compared with controls. J. Neuropsychiatry Clin. Neurosci. 2014, 26, 376–381. [Google Scholar] [CrossRef]
- Svensson, P.; Bjerring, P.; Arendt-Nielsen, L.; Kaaber, S. Sensory and pain thresholds to orofacial argon laser stimulation in patients with chronic burning mouth syndrome. Clin. J. Pain 1993, 9, 207–215. [Google Scholar] [CrossRef]
- Ito, M.; Kurita, K.; Ito, T.; Arao, M. Pain threshold and pain recovery after experimental stimulation in patients with burning mouth syndrome. Psychiatry Clin. Neurosci. 2002, 56, 161–168. [Google Scholar] [CrossRef]
- Siviero, M.; Teixeira, M.J.; Siqueira, J.T.; Siqueira, S.R. Central mechanisms in burning mouth syndrome involving the olfactory nerve: A preliminary study. Clinics 2011, 66, 509–512. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Wang, Y.; Wang, Z. Assessment of trigeminal somatosensory evoked potentials in burning mouth syndrome. Chin. J. Dent. Res. 2000, 3, 40–46. [Google Scholar] [PubMed]
- Honda, M.; Baad-Hansen, L.; Iida, T.; Dagsdottir, L.K.; Komiyama, O.; Kawara, M.; Svensson, P. Perceptual distortion of the tongue by lingual nerve block and topical application of capsaicin in healthy women. Clin. Oral Investig. 2017, 21, 2045–2052. [Google Scholar] [CrossRef]
- Tan, Y.; Wu, X.; Chen, J.; Kong, L.; Qian, Z. Structural and Functional Connectivity Between the Amygdala and Orbital Frontal Cortex in Burning Mouth Syndrome: An fMRI Study. Front. Psychol. 2019, 10, 1700. [Google Scholar] [CrossRef]
- Zavoreo, I.; Vucicevic Boras, V.; Zadravec, D.; Basic Kes, V.; Ciliga, D.; Gabric, D. The Significance of Brain Transcranial Sonography in Burning Mouth Syndrome: A Pilot Study. Acta Stomatol. Croat. 2017, 51, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.L.; Yao, H.; Zheng, X.J.; Du, G.H.; Shen, X.M.; Zhou, Y.M.; Tang, G.Y. Low regional cerebral blood flow in burning mouth syndrome patients with depression. Oral Dis. 2015, 21, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Keaser, M.L.; Meiller, T.F.; Seminowicz, D.A. Altered structure and function in the hippocampus and medial prefrontal cortex in patients with burning mouth syndrome. Pain 2014, 155, 1472–1480. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, A.; Okamoto, Y.; Doi, M.; Okada, G.; Takamura, M.; Ichikawa, N.; Yamawaki, S. Functional Alterations of Postcentral Gyrus Modulated by Angry Facial Expressions during Intraoral Tactile Stimuli in Patients with Burning Mouth Syndrome: A Functional Magnetic Resonance Imaging Study. Front. Psychiatry 2017, 8, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinding, C.; Gransjoen, A.M.; Schlumberger, G.; Grushka, M.; Frasnelli, J.; Singh, P.B. Grey matter changes of the pain matrix in patients with burning mouth syndrome. Eur. J. Neurosci. 2016, 43, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.C.; Jahng, G.H.; Ryu, C.W.; Byun, J.Y. Change in gray matter volume and cerebral blood flow in patients with burning mouth syndrome. J. Oral Pathol. Med. 2019, 48, 335–342. [Google Scholar] [CrossRef]
- Wada, A.; Shizukuishi, T.; Kikuta, J.; Yamada, H.; Watanabe, Y.; Imamura, Y.; Shinozaki, T.; Dezawa, K.; Haradome, H.; Abe, O. Altered structural connectivity of pain-related brain network in burning mouth syndrome-investigation by graph analysis of probabilistic tractography. Neuroradiology 2017, 59, 525–532. [Google Scholar] [CrossRef]
- Hagelberg, N.; Forssell, H.; Rinne, J.O.; Scheinin, H.; Taiminen, T.; Aalto, S.; Luutonen, S.; Någren, K.; Jääskeläinen, S. Striatal dopamine D1 and D2 receptors in burning mouth syndrome. Pain 2003, 101, 149–154. [Google Scholar] [CrossRef]
- Shinozaki, T.; Imamura, Y.; Kohashi, R.; Dezawa, K.; Nakaya, Y.; Sato, Y.; Watanabe, K.; Morimoto, Y.; Shizukuishi, T.; Abe, O.; et al. Spatial and Temporal Brain Responses to Noxious Heat Thermal Stimuli in Burning Mouth Syndrome. J. Dent. Res. 2016, 95, 1138–1146. [Google Scholar] [CrossRef]
- Barry, A.; O’Halloran, K.D.; McKenna, J.P.; McCreary, C.; Downer, E.J. Plasma IL-8 signature correlates with pain and depressive symptomatology in patients with burning mouth syndrome: Results from a pilot study. J. Oral Pathol. Med. 2018, 47, 158–165. [Google Scholar] [CrossRef]
- Ji, E.H.; Diep, C.; Liu, T.; Li, H.; Merrill, R.; Messadi, D.; Hu, S. Potential protein biomarkers for burning mouth syndrome discovered by quantitative proteomics. Mol. Pain 2017, 13, 1744806916686796. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Xia, J.; Lin, M.; Zhou, H.; Li, B. Serum interleukin-6 in patients with burning mouth syndrome and relationship with depression and perceived pain. Mediat. Inflamm. 2007, 2007, 45327. [Google Scholar] [CrossRef]
- Miyauchi, T.; Tokura, T.; Kimura, H.; Ito, M.; Umemura, E.; Sato Boku, A.; Nagashima, W.; Tonoike, T.; Yamamoto, Y.; Saito, K.; et al. Effect of antidepressant treatment on plasma levels of neuroinflammation-associated molecules in patients with somatic symptom disorder with predominant pain around the orofacial region. Hum. Psychopharmacol. 2019, 34, e2698. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, A.L.; de Sa, A.R.; Victoria, J.M.; de Fatima Correia-Silva, J.; Gomez, M.V.; Gomez, R.S. Interleukin-1beta and serotonin transporter gene polymorphisms in burning mouth syndrome patients. J. Pain 2006, 7, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Treldal, C.; Petersen, J.; Mogensen, S.; Therkildsen, C.; Jacobsen, J.; Andersen, O.; Pedersen, A.M.L. Characterization of burning mouth syndrome profiles based on response to a local anaesthetic lozenge. Oral Dis. 2020, 26, 656–669. [Google Scholar] [CrossRef]
- Penza, P.; Majorana, A.; Lombardi, R.; Camozzi, F.; Bonadeo, S.; Sapelli, P.; Lauria, G. “Burning tongue” and “burning tip”: The diagnostic challenge of the burning mouth syndrome. Clin. J. Pain 2010, 26, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Puhakka, A.; Forssell, H.; Soinila, S.; Virtanen, A.; Roytta, M.; Laine, M.; Tenovuo, O.; Teerijoki-Oksa, T.; Jaaskelainen, S.K. Peripheral nervous system involvement in primary burning mouth syndrome--results of a pilot study. Oral Dis. 2016, 22, 338–344. [Google Scholar] [CrossRef]
- Beneng, K.; Renton, T.; Yilmaz, Z.; Yiangou, Y.; Anand, P. Sodium channel Na v 1.7 immunoreactivity in painful human dental pulp and burning mouth syndrome. BMC Neurosci. 2010, 11, 71. [Google Scholar] [CrossRef] [Green Version]
- Beneng, K.; Yilmaz, Z.; Yiangou, Y.; McParland, H.; Anand, P.; Renton, T. Sensory purinergic receptor P2 × 3 is elevated in burning mouth syndrome. Int. J. Oral Maxillofac. Surg. 2010, 39, 815–819. [Google Scholar] [CrossRef]
- Wandeur, T.; de Moura, S.A.; de Medeiros, A.M.; Machado, M.A.; Alanis, L.R.; Gregio, A.M.; Trevilatto, P.C.; de Lima, A.A. Exfoliative cytology of the oral mucosa in burning mouth syndrome: A cytomorphological and cytomorphometric analysis. Gerodontology 2011, 28, 44–48. [Google Scholar] [CrossRef]
- O’Neill, F.; Marshall, A.; Ferdousi, M.; Malik, R.A. Corneal Confocal Microscopy Detects Small-Fiber Neuropathy in Burning Mouth Syndrome: A Cross-Sectional Study. J. Oral Facial Pain Headache 2019, 33, 337–341. [Google Scholar] [CrossRef]
- Morr Verenzuela, C.S.; Davis, M.D.P.; Bruce, A.J.; Torgerson, R.R. Burning mouth syndrome: Results of screening tests for vitamin and mineral deficiencies, thyroid hormone, and glucose levels-experience at Mayo Clinic over a decade. Int. J. Dermatol. 2017, 56, 952–956. [Google Scholar] [CrossRef]
- Lopez-Jornet, P.; Juan, H.; Alvaro, P.F. Mineral and trace element analysis of saliva from patients with BMS: A cross-sectional prospective controlled clinical study. J. Oral Pathol. Med. 2014, 43, 111–116. [Google Scholar] [CrossRef]
- Boucher, Y.; Braud, A.; Dufour, E.; Agbo-Godeau, S.; Baaroun, V.; Descroix, V.; Guinnepain, M.T.; Ungeheuer, M.N.; Ottone, C.; Rougeot, C. Opiorphin levels in fluids of burning mouth syndrome patients: A case-control study. Clin. Oral Investig. 2017, 21, 2157–2164. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.; O’Halloran, K.D.; McKenna, J.P.; McCreary, C.; Harhen, B.; Kerr, D.M.; Finn, D.P.; Downer, E.J. Plasma N-acylethanolamine and endocannabinoid levels in burning mouth syndrome: Potential role in disease pathogenesis. J. Oral Pathol. Med. 2018, 47, 440–442. [Google Scholar] [CrossRef]
- Tatullo, M.; Marrelli, M.; Scacco, S.; Lorusso, M.; Doria, S.; Sabatini, R.; Auteri, P.; Cagiano, R.; Inchingolo, F. Relationship between oxidative stress and “burning mouth syndrome” in female patients: A scientific hypothesis. Eur. Rev. Med. Pharmacol. Sci 2012, 16, 1218–1221. [Google Scholar] [PubMed]
- Kang, J.H.; Kim, Y.Y.; Chang, J.Y.; Kho, H.S. Relationships between oral MUC1 expression and salivary hormones in burning mouth syndrome. Arch. Oral Biol. 2017, 78, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Loeb, L.M.; Naffah-Mazzacoratti, M.G.; Porcionatto, M.A.; Martins, J.R.; Kouyoumdjian, M.; Weckx, L.M.; Nader, H.B. Chondroitin sulfate and kallikrein in saliva: Markers for glossodynia. Int. Immunopharmacol. 2008, 8, 1056–1058. [Google Scholar] [CrossRef] [PubMed]
- Koike, K.; Shinozaki, T.; Hara, K.; Noma, N.; Okada-Ogawa, A.; Asano, M.; Shinoda, M.; Eliav, E.; Gracely, R.H.; Iwata, K.; et al. Immune and endocrine function in patients with burning mouth syndrome. Clin. J. Pain 2014, 30, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Heckmann, S.M.; Heckmann, J.G.; HiIz, M.J.; Popp, M.; Marthol, H.; Neundörfer, B.; Hummel, T. Oral mucosal blood flow in patients with burning mouth syndrome. Pain 2001, 90, 281–286. [Google Scholar] [CrossRef]
- Zidverc-Trajkovic, J.; Stanimirovic, D.; Obrenovic, R.; Tajti, J.; Vecsei, L.; Gardi, J.; Nemeth, J.; Mijajlovic, M.; Sternic, N.; Jankovic, L. Calcitonin gene-related peptide levels in saliva of patients with burning mouth syndrome. J. Oral Pathol. Med. 2009, 38, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Shinoda, M.; Takeda, M.; Honda, K.; Maruno, M.; Katagiri, A.; Satoh-Kuriwada, S.; Shoji, N.; Tsuchiya, M.; Iwata, K. Involvement of peripheral artemin signaling in tongue pain: Possible mechanism in burning mouth syndrome. Pain 2015, 156, 2528–2537. [Google Scholar] [CrossRef]
- Lopez-Jornet, P.; Lucero-Berdugo, M.; Castillo-Felipe, C.; Zamora Lavella, C.; Ferrandez-Pujante, A.; Pons-Fuster, A. Assessment of self-reported sleep disturbance and psychological status in patients with burning mouth syndrome. J. Eur. Acad. Derm. Venereol. 2015, 29, 1285–1290. [Google Scholar] [CrossRef]
- Malik, R.; Goel, S.; Misra, D.; Panjwani, S.; Misra, A. Assessment of anxiety and depression in patients with burning mouth syndrome: A clinical trial. J. Midlife Health 2012, 3, 36–39. [Google Scholar] [CrossRef]
- Sevrain, M.; Brenaut, E.; Le Toux, G.; Misery, L. Primary Burning Mouth Syndrome: A Questionnaire Study of Neuropathic and Psychological Components. Am. J. Clin. Dermatol. 2016, 17, 171–178. [Google Scholar] [CrossRef]
- Lopez-Jornet, P.; Molino-Pagan, D.; Parra-Perez, P.; Valenzuela, S. Neuropathic Pain in Patients with Burning Mouth Syndrome Evaluated Using painDETECT. Pain Med. 2017, 18, 1528–1533. [Google Scholar] [CrossRef]
- Kim, M.J.; Kim, J.; Kho, H.S. Comparison between burning mouth syndrome patients with and without psychological problems. Int. J. Oral Maxillofac. Surg. 2018, 47, 879–887. [Google Scholar] [CrossRef]
- Schiavone, V.; Adamo, D.; Ventrella, G.; Morlino, M.; De Notaris, E.B.; Ravel, M.G.; Kusmann, F.; Piantadosi, M.; Pollio, A.; Fortuna, G.; et al. Anxiety, depression, and pain in burning mouth syndrome: First chicken or egg? Headache 2012, 52, 1019–1025. [Google Scholar] [CrossRef]
- Carlson, C.R.; Miller, C.S.; Reid, K.I. Psychosocial profiles of patients with burning mouth syndrome. J. Orofac. Pain 2000, 14, 59–64. [Google Scholar]
- Adamo, D.; Pecoraro, G.; Fortuna, G.; Amato, M.; Marenzi, G.; Aria, M.; Mignogna, M.D. Assessment of oral health-related quality of life, measured by OHIP-14 and GOHAI, and psychological profiling in burning mouth syndrome: A case-control clinical study. J. Oral Rehabil. 2020, 47, 42–52. [Google Scholar] [CrossRef]
- Marino, R.; Picci, R.L.; Ferro, G.; Carezana, C.; Gandolfo, S.; Pentenero, M. Peculiar alexithymic traits in burning mouth syndrome: Case-control study. Clin. Oral Investig. 2015, 19, 1799–1805. [Google Scholar] [CrossRef]
- Das Neves de Araujo Lima, E.; Barbosa, N.G.; Dos Santos, A.C.; AraujoMouraLemos, T.M.; de Souza, C.M.; Trevilatto, P.C.; da Silveira, E.J.; de Medeiros, A.M. Comparative Analysis of Psychological, Hormonal, and Genetic Factors between Burning Mouth Syndrome and Secondary Oral Burning. Pain Med. 2016, 17, 1602–1611. [Google Scholar] [CrossRef]
- Jerlang, B.B. Burning mouth syndrome (BMS) and the concept of alexithymia—A preliminary study. J. Oral Pathol. Med. 1997, 26, 249–253. [Google Scholar] [CrossRef]
- Tokura, T.; Kimura, H.; Ito, M.; Nagashima, W.; Sato, N.; Kimura, Y.; Arao, M.; Aleksic, B.; Yoshida, K.; Kurita, K.; et al. Temperament and character profiles of patients with burning mouth syndrome. J. Psychosom. Res. 2015, 78, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Takenoshita, M.; Sato, T.; Kato, Y.; Katagiri, A.; Yoshikawa, T.; Sato, Y.; Matsushima, E.; Sasaki, Y.; Toyofuku, A. Psychiatric diagnoses in patients with burning mouth syndrome and atypical odontalgia referred from psychiatric to dental facilities. Neuropsychiatr. Dis. Treat. 2010, 6, 699–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tu, T.T.H.; Miura, A.; Shinohara, Y.; Mikuzuki, L.; Kawasaki, K.; Sugawara, S.; Suga, T.; Watanabe, T.; Watanabe, M.; Umezaki, Y.; et al. Evaluating Burning Mouth Syndrome as a Comorbidity of Atypical Odontalgia: The Impact on Pain Experiences. Pain Pract. 2018, 18, 580–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ott, G.; Ott, C. Glossodynia—Psychodynamic basis and results of psychopathometric investigations. J. Psychosom. Res. 1992, 36, 677–686. [Google Scholar] [CrossRef]
- Bogetto, F.; Maina, G.; Ferro, G.; Carbone, M.; Gandolfo, S. Psychiatric comorbidity in patients with burning mouth syndrome. Psychosom. Med. 1998, 60, 378–385. [Google Scholar] [CrossRef]
- Forssell, H.; Teerijoki-Oksa, T.; Puukka, P.; Estlander, A.M. Symptom severity in burning mouth syndrome associates with psychological factors. J. Oral Rehabil. 2020, 47, 713–719. [Google Scholar] [CrossRef] [Green Version]
- Miyaoka, H.; Kamijima, K.; Katayama, Y.; Ebihara, T.; Nagai, T. A Psychiatric Appraisal of “Glossodynia”. Psychosomatics 1996, 37, 346–348. [Google Scholar] [CrossRef]
- Acharya, S.; Carlen, A.; Wenneberg, B.; Jontell, M.; Hagglin, C. Clinical characterization of women with burning mouth syndrome in a case-control study. Acta Odontol. Scand. 2018, 76, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Taiminen, T.; Kuusalo, L.; Lehtinen, L.; Forssell, H.; Hagelberg, N.; Tenovuo, O.; Luutonen, S.; Pertovaara, A.; Jaaskelainen, S. Psychiatric (axis I) and personality (axis II) disorders in patients with burning mouth syndrome or atypical facial pain. Scand. J. Pain 2011, 2, 155–160. [Google Scholar] [CrossRef]
- Merigo, E.; Manfredi, M.; Zanetti, M.R.; Miazza, D.; Pedrazzi, G.; Vescovi, P. Burning mouth syndrome and personality profiles. Minerva. Stomatol. 2007, 56, 159–167. [Google Scholar] [PubMed]
- Jedel, E.; Elfstrom, M.L.; Hagglin, C. Differences in personality, perceived stress and physical activity in women with burning mouth syndrome compared to controls. Scand. J. Pain 2020. [Google Scholar] [CrossRef] [PubMed]
- Komiyama, O.; Obara, R.; Uchida, T.; Nishimura, H.; Iida, T.; Okubo, M.; Shimosaka, M.; Narita, N.; Niwa, H.; Shinoda, M.; et al. Pain intensity and psychosocial characteristics of patients with burning mouth syndrome and trigeminal neuralgia. J. Oral Sci. 2012, 54, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heo, J.Y.; Ok, S.M.; Ahn, Y.W.; Ko, M.Y.; Jeong, S.H. The application of neuropathic pain questionnaires in burning mouth syndrome patients. J. Oral Facial Pain Headache 2015, 29, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Braud, A.; Toure, B.; Agbo-Godeau, S.; Descroix, V.; Boucher, Y. Characteristics of pain assessed with visual analog scale and questionnaire in burning mouth syndrome patients: A pilot study. J. Orofac. Pain 2013, 27, 235–242. [Google Scholar] [CrossRef]
- Zakrzewska, J.M.; Padfield, D.; Ferguson, A. Visual Imagery: A Tool to Explore the Impact of Burning Mouth Syndrome. J. Oral Facial Pain Headache 2019, 33, e8–e14. [Google Scholar] [CrossRef]
- Mignogna, M.D.; Pollio, A.; Fortuna, G.; Leuci, S.; Ruoppo, E.; Adamo, D.; Zarrelli, C. Unexplained somatic comorbidities in patients with burning mouth syndrome: A controlled clinical study. J. Orofac. Pain 2011, 25, 131–140. [Google Scholar]
- Rolke, R.; Baron, R.; Maier, C.A.; Tölle, T.; Treede, R.-D.; Beyer, A.; Binder, A.; Birbaumer, N.; Birklein, F.; Bötefür, I. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): Standardized protocol and reference values. Pain 2006, 123, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.R.; Dziengo, S.; Boers, O.; Goldsmith, C.H.; Graham, N.; Lilge, L.; Burnie, S.; White, R. Low Level Laser Therapy (LLLT) for Neck Pain: A Systematic Review and Meta-Regression. Open Orthop. J. 2013, 7, 396–419. [Google Scholar] [CrossRef] [PubMed]
- Trelles, M.; Mayayo, E.; Miro, L.; Rigau, J.; Baudin, G.; Calderhead, R.G. The action of low reactive level laser therapy (LLLT) on mast cells: A possibte pain relief mechanism examined. Laser Ther. 1989, 1, 27–30. [Google Scholar] [CrossRef] [Green Version]
- Maeda, T. Morphological demonstration of low reactive laser therapeutic pain attenuation effect of the gallium aluminium arsenide diode laser. Laser Ther. 1989, 1, 23–26. [Google Scholar] [CrossRef] [Green Version]
- Chow, R.; Armati, P.; Laakso, E.-L.; Bjordal, J.M.; Baxter, G.D. Inhibitory effects of laser irradiation on peripheral mammalian nerves and relevance to analgesic effects: A systematic review. Photomed. Laser Surg. 2011, 29, 365–381. [Google Scholar] [CrossRef]
- Silvestre, F.J.; Silvestre-Rangil, J.; López-Jornet, P. Burning mouth syndrome: A review and update. Rev. Neurol. 2015, 60, 457–463. [Google Scholar]
- Lamey, P.J. Burning mouth syndrome. Dermatol. Clin. 1996, 14, 339–354. [Google Scholar] [CrossRef]
- De Souza, F.T.A.; Teixeira, A.L.; Amaral, T.M.P.; Santos, T.P.M.D.; Abreu, M.H.N.G.; Silva, T.A.; Kummer, A. Psychiatric disorders in burning mouth syndrome. J. Psychosom. Res. 2012, 72, 142–146. [Google Scholar] [CrossRef]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D. Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- Shibata, M.; Ninomiya, T.; Jensen, M.P.; Anno, K.; Yonemoto, K.; Makino, S.; Iwaki, R.; Yamashiro, K.; Yoshida, T.; Imada, Y. Alexithymia is associated with greater risk of chronic pain and negative affect and with lower life satisfaction in a general population: The Hisayama Study. PLoS ONE 2014, 9, e90984. [Google Scholar] [CrossRef] [Green Version]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.A.; Rice, A.S.C.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef] [PubMed]
- Aydede, M.; Shriver, A. Recently introduced definition of “nociplastic pain” by the International Association for the Study of Pain needs better formulation. Pain 2018, 159, 1176–1177. [Google Scholar] [CrossRef] [PubMed]


| Author/Year | Type of Study | Cytokine(s) Evaluated | Sample Type | Significant Results |
|---|---|---|---|---|
| Barry, 2018 [83] | Case control | IL-8, IL-4, IL-2, IL-12p70, IL-13, IFN-c, IL-6, IL-10, TNF–a, IL-1b | Plasma | IL-8 increased in BMS compared to healthy control IL-4, IL-2, IL-12p70, IL-13, IFN-c, IL-6, IL-10, TNF–a, and IL-1b comparable between the two groups |
| Ji, 2017 [84] | Case control | IL-18 | Saliva | IL-18 increased in BMS compared to healthy control |
| Chen, 2007 [85] | Case control | IL-6 | Blood | IL-6 is lower in BMS compared to healthy control |
| Treldal, 2020 [88] | RCT | IL-6, IL-8, IL-17A, IL-23 TNF-α | Blood Plasma Saliva | IL-6, IL-8, IL-17, IL-23, and TNF-α: higher in the No effect group than the patients in the Effect group, but not statistically significant (p-values: 0.068–0.916). Higher levels of IL-6, IL-8, and IL-23 for the No effect group when compared with the Control group (p-values: 0.096–0.542). Only IL-6 was significantly elevated in stimulated parotid saliva for the No effect group (p = 0.020). The cytokine levels in chewing-stimulated whole saliva did not differ between the patient groups |
| Miyauchi, 2019 [86] | Case control | Neuroinflammation-related molecules Cytokine | Plasma | IL-1β, IL-1 receptor antagonist, IL-6, macrophage inflammatory protein-1β, and platelet-derived growth factor-bb significantly higher in patients than in controls. |
| Guimarães, 2006 [87] | Case control | Genetic polymorphisms of IL-1 beta and 5-HTTLPR | Oral mucosa swabs | No statistical difference in 5-HTTLPR genotypes between the case and control groups (p = 0.60) Significant increase in the IL-1b high production genotype CT in BMS subjects (p = 0.005) = > Association between BMS and IL-1b high producer genotype. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orliaguet, M.; Misery, L. Neuropathic and Psychogenic Components of Burning Mouth Syndrome: A Systematic Review. Biomolecules 2021, 11, 1237. https://doi.org/10.3390/biom11081237
Orliaguet M, Misery L. Neuropathic and Psychogenic Components of Burning Mouth Syndrome: A Systematic Review. Biomolecules. 2021; 11(8):1237. https://doi.org/10.3390/biom11081237
Chicago/Turabian StyleOrliaguet, Marie, and Laurent Misery. 2021. "Neuropathic and Psychogenic Components of Burning Mouth Syndrome: A Systematic Review" Biomolecules 11, no. 8: 1237. https://doi.org/10.3390/biom11081237