
Partial Decellularization for Segmental Tracheal Scaffold Tissue Engineering: A Preliminary Study in Rabbits



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
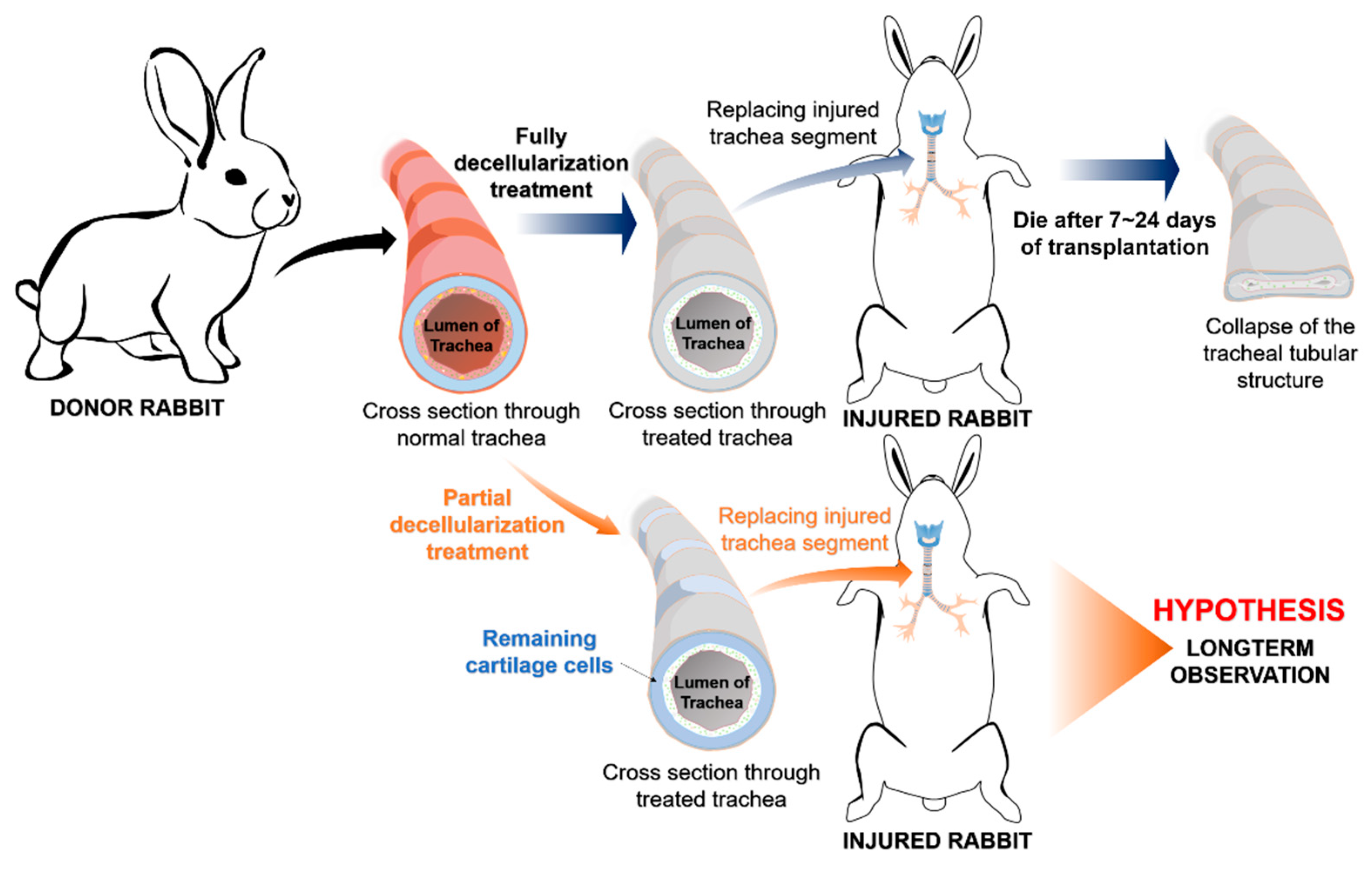
2.1. Animals and Study Design
2.2. Manufacturing the Trachea Scaffold
2.2.1. Partial Decellularization of the Rabbit Trachea
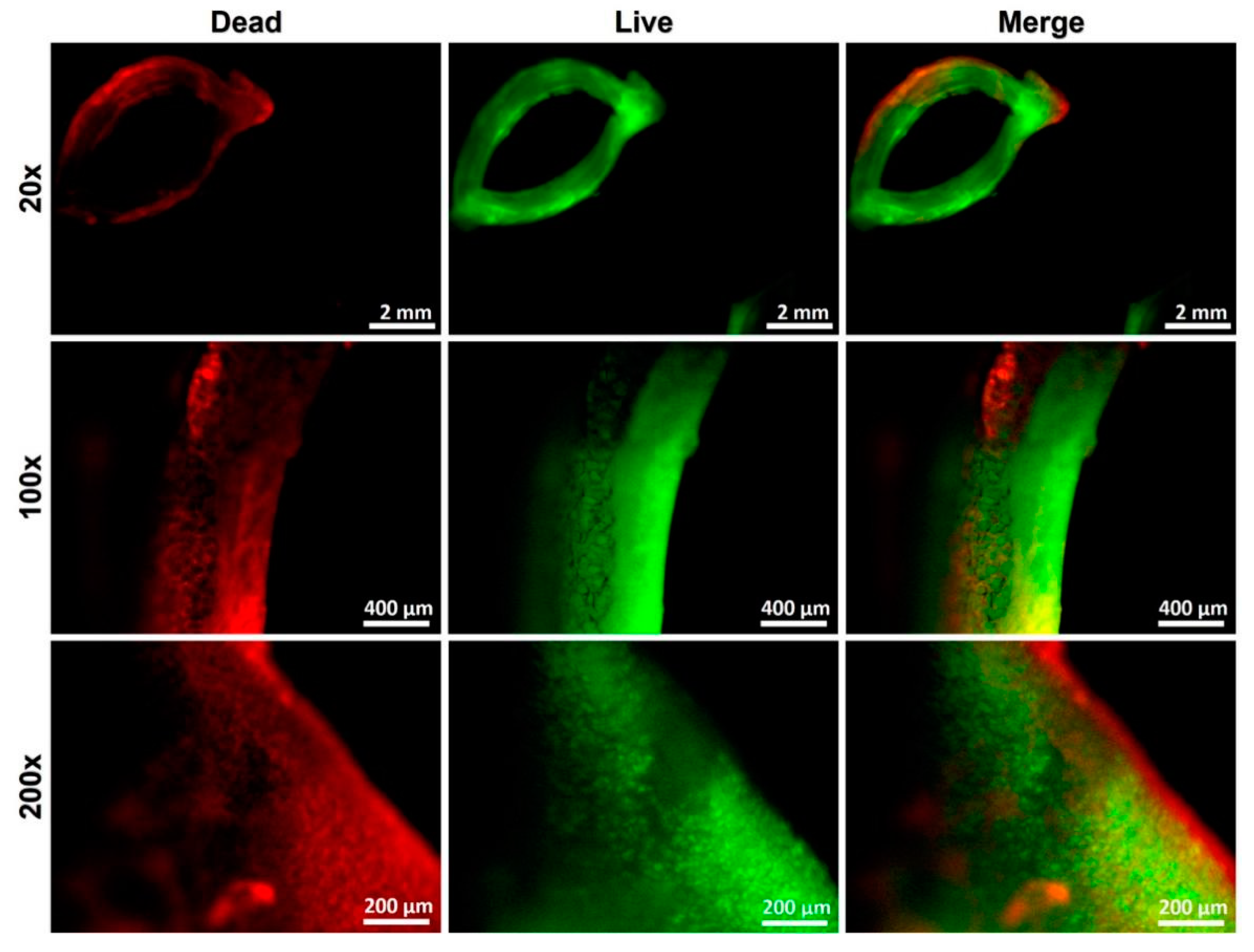
2.2.2. Decellularized Scaffold Evaluation—Vital Staining Test
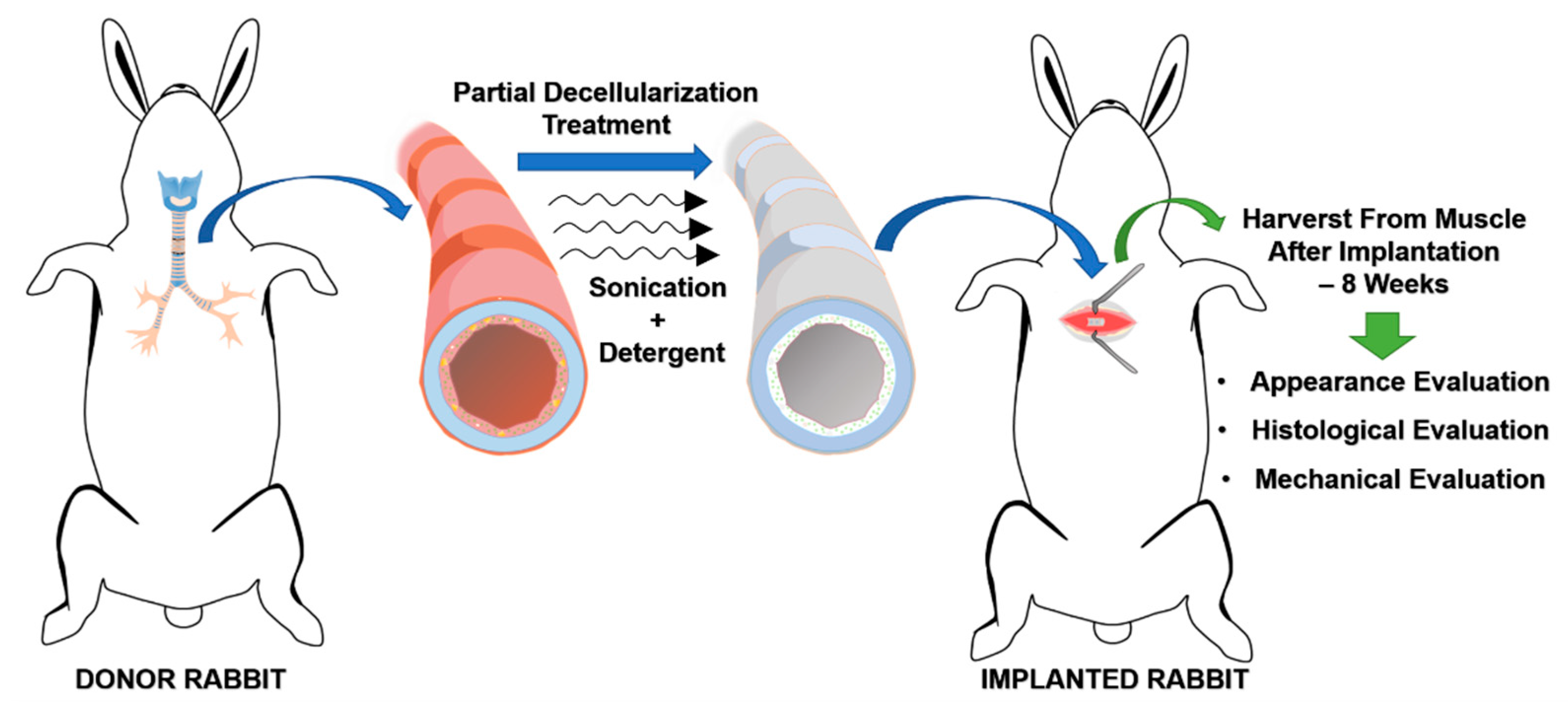
2.3. Heterotopic Implantation of the Decellularized Graft
2.3.1. Surgical Procedure
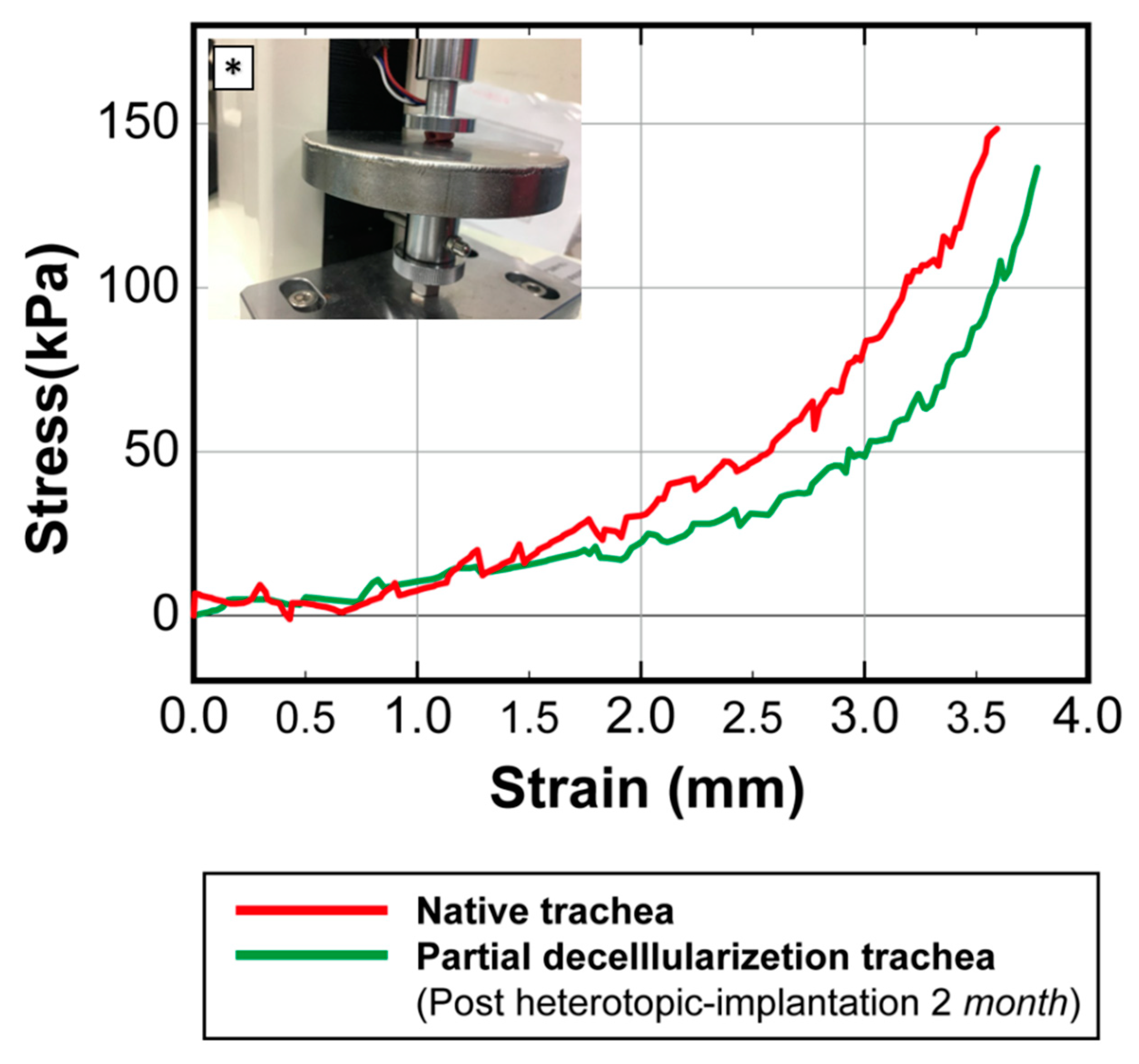
2.3.2. Histological Evaluations and Mechanical Testing for Heterotopic Transplants
2.4. Allograft Orthotopic Transplantation
2.4.1. Surgical Procedure
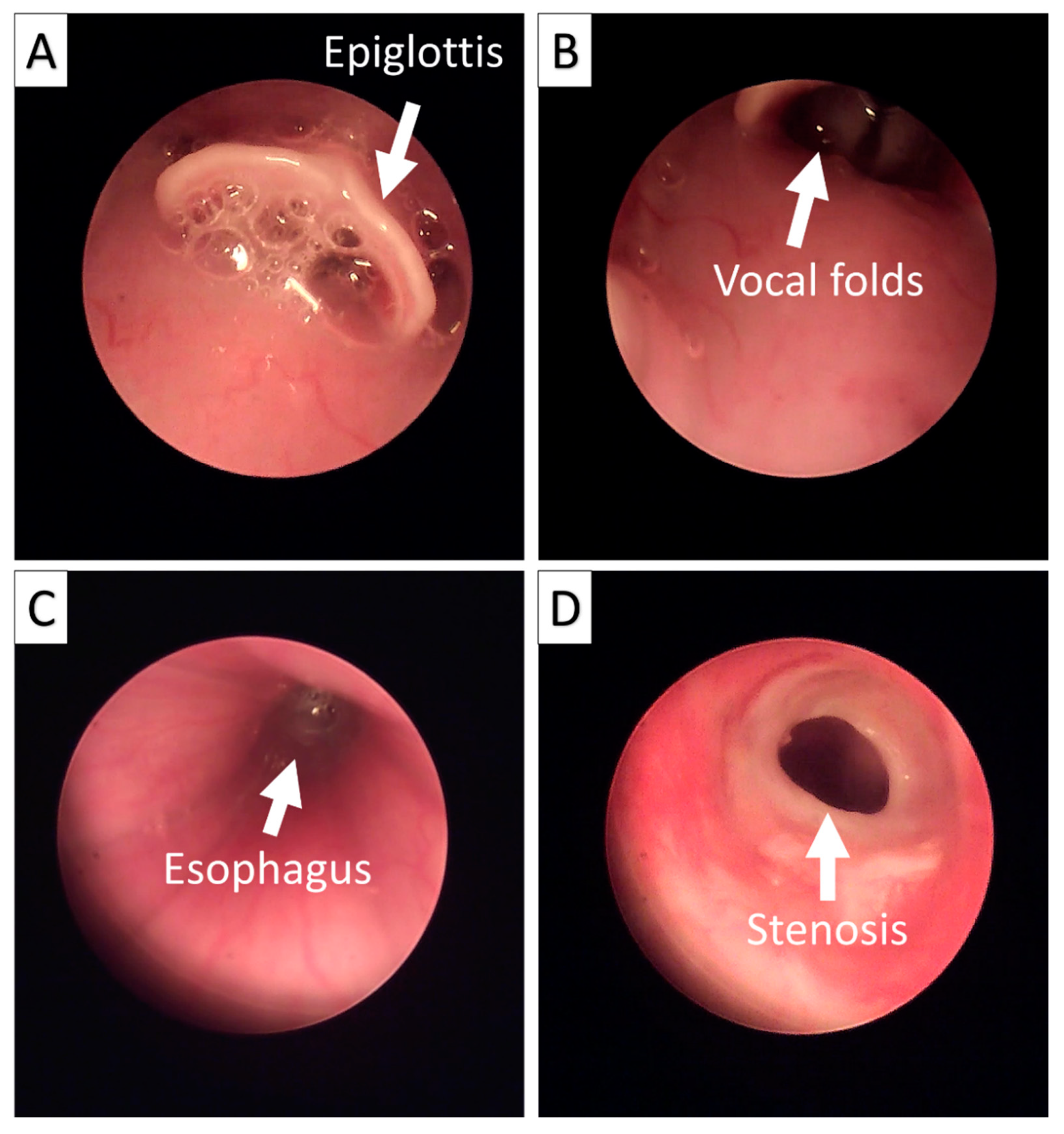
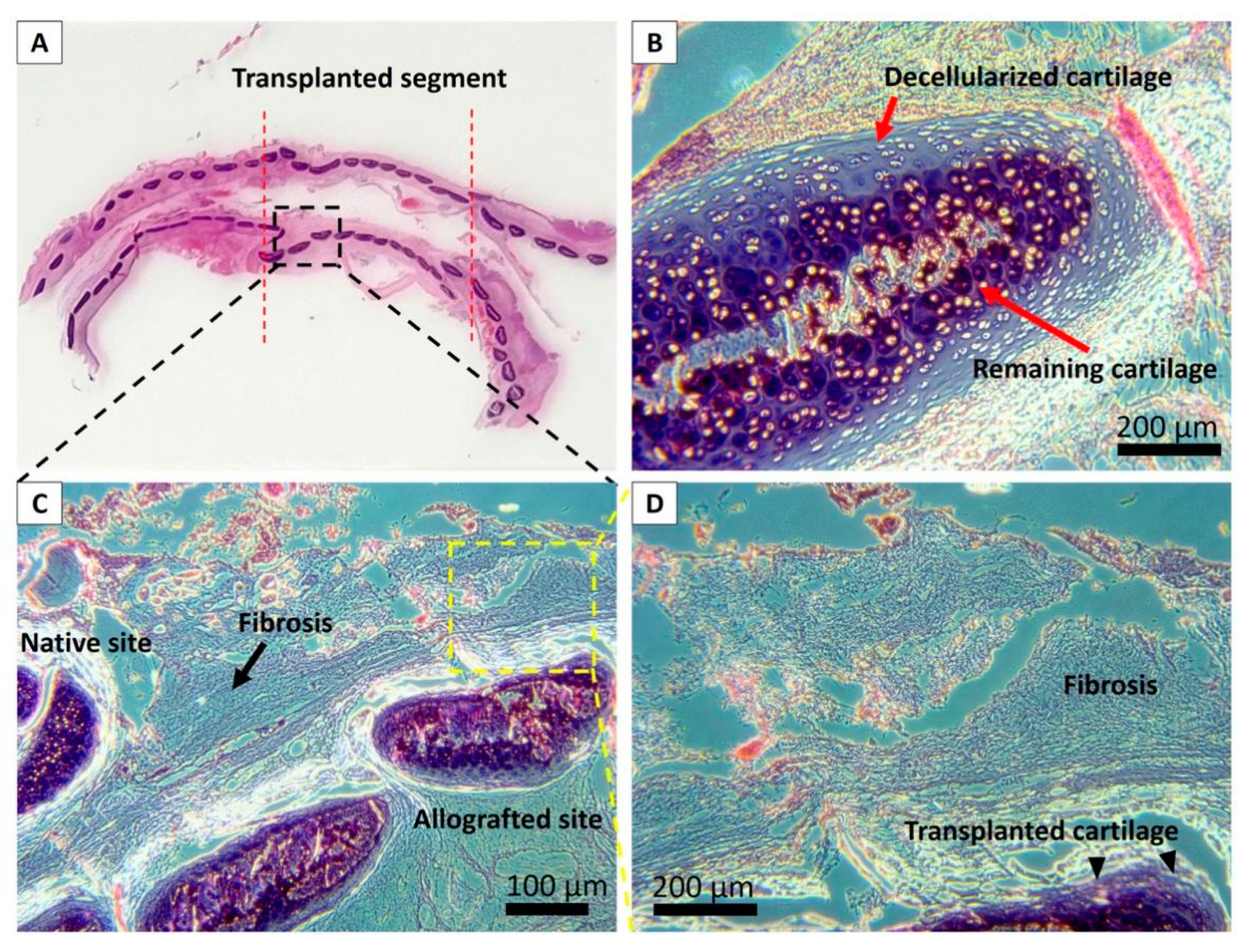
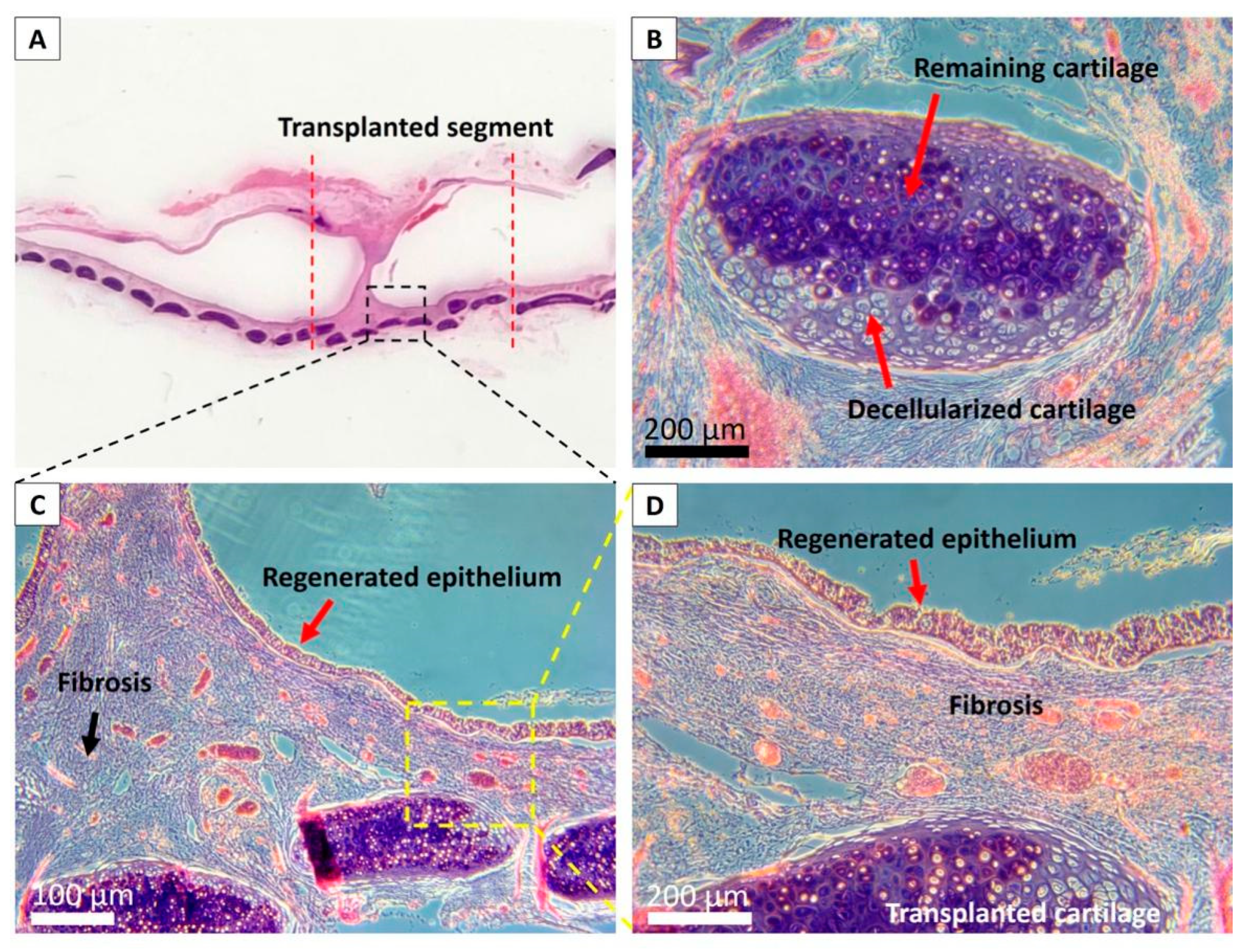
2.4.2. Endoscopic and Histological Analyses after Allograft Transplantation
3. Results
3.1. Partially Decellularized Trachea Scaffold Manufacturing and Evaluation
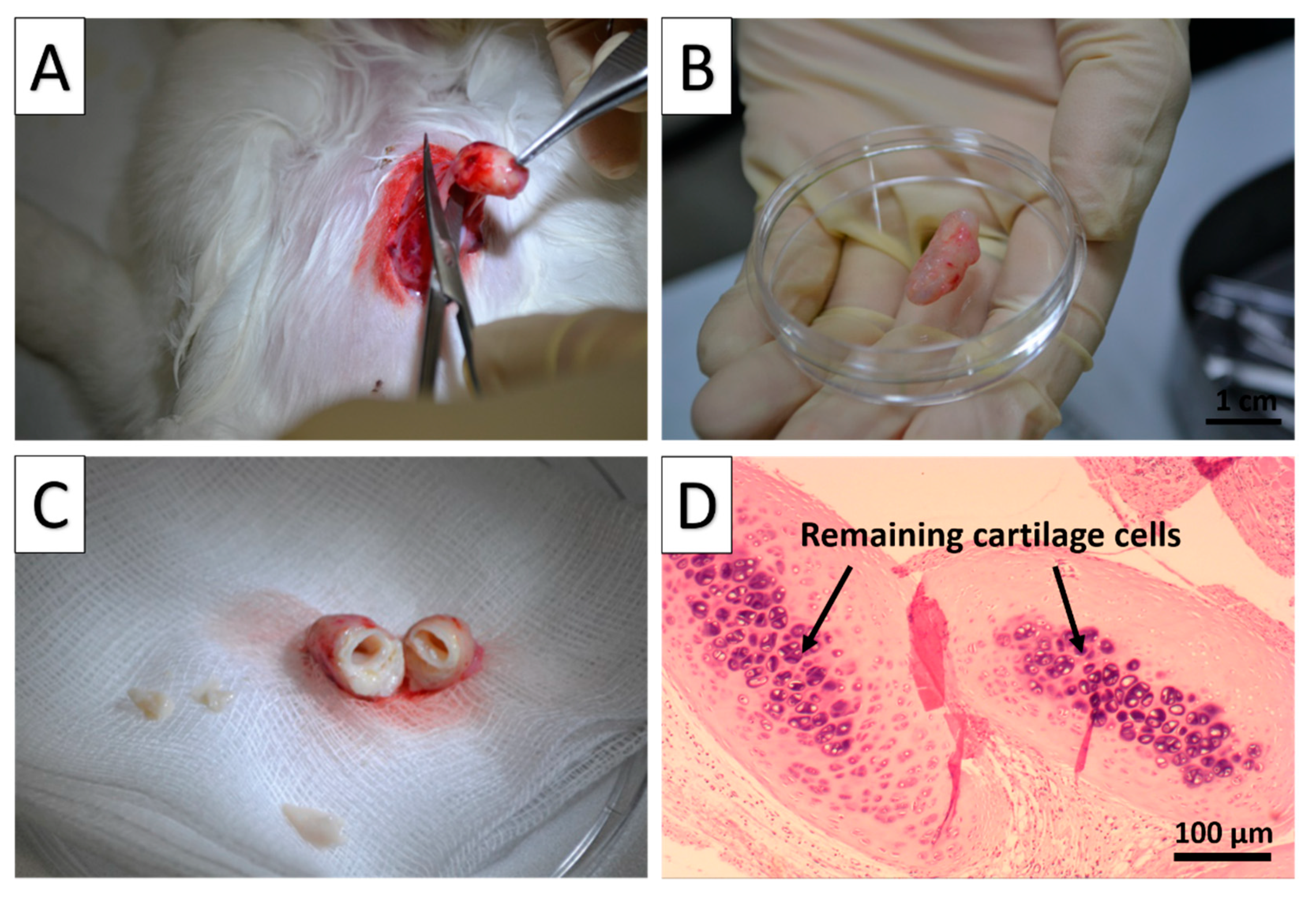
3.2. Heterotopic Implantation Test of the Allograft
3.3. Transplantation of the Partially Decellularized Trachea Segment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Ecker, R.R.; Libertini, R.V.; Rea, W.J.; Sugg, W.L.; Webb, W.R. Injuries of the Trachea and Bronchi. Ann. Thorac. Surg. 1971, 11, 289–298. [Google Scholar] [CrossRef]
- Grillo, H.C. Tracheal replacement: A critical review. Ann. Thorac. Surg. 2002, 73, 1995–2004. [Google Scholar] [CrossRef]
- Etienne, H.; Fabre, D.; Caro, A.G.; Kolb, F.; Mussot, S.; Mercier, O.; Mitilian, D.; Stephan, F.; Fadel, E.; Dartevelle, P. Tracheal replacement. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef] [PubMed]
- Udelsman, B.; Mathisen, D.J.; Ott, H.C. A reassessment of tracheal substitutes—A systematic review. Ann. Cardiothorac. Surg. 2018, 7, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Law, J.X.; Liau, L.L.; Aminuddin, B.S.; Ruszymah, B.H.I. Tissue-Engineered trachea: A review. Int. J. Pediatr. Otorhinolaryngol. 2016, 91, 55–63. [Google Scholar] [CrossRef]
- Park, J.H.; Yoon, J.K.; Lee, J.B.; Shin, Y.M.; Lee, K.W.; Bae, S.W.; Lee, J.H.; Yu, J.J.; Jung, C.R.; Youn, Y.N.; et al. Experimental Tracheal Replacement Using 3-dimensional Bioprinted Artificial Trachea with Autologous Epithelial Cells and Chondrocytes. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Gao, B.; Jing, H.; Gao, M.; Wang, S.; Fu, W.; Zhang, X.; He, X.; Zheng, J. Long-Segmental tracheal reconstruction in rabbits with pedicled Tissue-Engineered trachea based on a 3D-printed scaffold. Acta Biomater. 2019, 97, 177–186. [Google Scholar] [CrossRef]
- Bae, S.W.; Lee, K.W.; Park, J.H.; Lee, J.H.; Jung, C.R.; Yu, J.J.; Kim, H.Y.; Kim, D.H. 3D bioprinted artificial trachea with epithelial cells and chondrogenic-differentiated bone marrow-derived mesenchymal stem cells. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef] [Green Version]
- Lu, T.; Huang, Y.; Qiao, Y.; Zhang, Y.; Liu, Y. Evaluation of changes in cartilage viability in detergent-treated tracheal grafts for immunosuppressant-free allotransplantation in dogs. Eur. J. Cardio Thorac. Surg. 2018, 53, 672–679. [Google Scholar] [CrossRef]
- Maughan, E.F.; Butler, C.R.; Crowley, C.; Teoh, G.Z.; Hondt, M.D.; Hamilton, N.J.; Hynds, R.E.; Lange, P.; Ansari, T.; Urbani, L.; et al. A comparison of tracheal scaffold strategies for pediatric transplantation in a rabbit model. Laryngoscope 2017, 127, E449–E457. [Google Scholar] [CrossRef] [Green Version]
- Jungebluth, P.; Go, T.; Asnaghi, A.; Bellini, S.; Martorell, J.; Calore, C.; Urbani, L.; Ostertag, H.; Mantero, S.; Conconi, M.T.; et al. Structural and morphologic evaluation of a novel detergent-enzymatic tissue-engineered tracheal tubular matrix. J. Thorac. Cardiovasc. Surg. 2009, 138, 586–593. [Google Scholar] [CrossRef]
- Ohno, M.; Fuchimoto, Y.; Higuchi, M.; Yamaoka, T.; Komura, M.; Umezawa, A.; Hsu, H.C.; Enosawa, S.; Kuroda, T. Long-Term observation of airway reconstruction using decellularized tracheal allografts in micro-miniature pigs at growing stage. Regen. Ther. 2020, 15, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Ohno, M.; Fuchimoto, Y.; Hsu, H.C.; Higuchi, M.; Komura, M.; Yamaoka, T.; Umezawa, A.; Enosawa, S.; Kuroda, T. Airway reconstruction using decellularized tracheal allografts in a porcine model. Pediatr. Surg. Int. 2017, 33, 1065–1071. [Google Scholar] [CrossRef]
- Hung, S.H.; Su, C.H.; Lin, S.E.; Tseng, H. Preliminary experiences in trachea scaffold tissue engineering with segmental organ decellularization. Laryngoscope 2016, 126, 2520–2527. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.R.; Hynds, R.E.; Crowley, C.; Gowers, K.H.C.; Partington, L.; Hamilton, N.J.; Carvalho, C.; Platé, M.; Samuel, E.R.; Burns, A.J.; et al. Vacuum-Assisted decellularization: An accelerated protocol to generate tissue-engineered human tracheal scaffolds. Biomaterials 2017, 124, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Remlinger, N.T.; Czajka, C.A.; Juhas, M.E.; Vorp, D.A.; Stolz, D.B.; Badylak, S.F.; Gilbert, S.; Gilbert, T.W. Hydrated xenogeneic decellularized tracheal matrix as a scaffold for tracheal reconstruction. Biomaterials 2010, 31, 3520–3526. [Google Scholar] [CrossRef]
- Maughan, E.F.; Hynds, R.E.; Proctor, T.J.; Janes, S.M.; Elliott, M.; Birchall, M.A.; Lowdell, M.W.; de Coppi, P. Autologous Cell Seeding in Tracheal Tissue Engineering. Curr. Stem Cell Rep. 2017, 3, 279–289. [Google Scholar] [CrossRef] [Green Version]
- Jungebluth, P.; Haag, J.C.; Sjöqvist, S.; Gustafsson, Y.; Rodríguez, A.B.; Del Gaudio, C.; Bianco, A.; Dehnisch, I.; Uhlén, P.; Baiguera, S.; et al. Tracheal tissue engineering in rats. Nat. Protoc. 2014, 9, 2164–2179. [Google Scholar] [CrossRef]
- Ma, R.; Li, M.; Luo, J.; Yu, H.; Sun, Y.; Cheng, S.; Cui, P. Structural integrity, ECM components and immunogenicity of decellularized laryngeal scaffold with preserved cartilage. Biomaterials 2013, 34, 1790–1798. [Google Scholar] [CrossRef]
- Cui, P.; Liu, P.; Li, S.; Ma, R. De-Epithelialized Heterotopic Tracheal Allografts without Immunosuppressants in Dogs: Long-Term Results for Cartilage Viability and Structural Integrity. Ann. Otol. Rhinol. Laryngol. 2021, 130, 441–449. [Google Scholar] [CrossRef]
- Aoki, F.G.; Varma, R.; Marin-Araujo, A.E.; Lee, H.; Soleas, J.P.; Li, A.H.; Soon, K.; Romero, D.; Moriya, H.T.; Haykal, S.; et al. De-Epithelialization of porcine tracheal allografts as an approach for tracheal tissue engineering. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Nakamura, T.; Sekine, T.; Matsumoto, K.; Ueda, H.; Yoshitani, M.; Toba, T.; Shimizu, Y. New type of tracheal bioartificial organ treated with detergent: Maintaining cartilage viability is necessary for successful immunosuppressant free allotransplantation. ASAIO J. 2002, 48, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, Y.; Liu, Y.; Dan, L.; Yin, Z.; Huo, Y.; Jiang, G.; Yang, Y.; Wang, Z.; Li, Y.; et al. Porous decellularized trachea scaffold prepared by a laser micropore technique. J. Mech. Behav. Biomed. Mater. 2019, 90, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, J.C.; Clark, P.M.; Capaldi, F.M. Effect of Decellularization Protocol on the Mechanical Behavior of Porcine Descending Aorta. Int. J. Biomater. 2010, 2010, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nonaka, P.N.; Campillo, N.; Uriarte, J.J.; Garreta, E.; Melo, E.; de Oliveira, L.V.F.; Navajas, D.; Farré, R. Effects of freezing/thawing on the mechanical properties of decellularized lungs. J. Biomed. Mater. Res. Part A 2014, 102, 413–419. [Google Scholar] [CrossRef]
- Rieder, E.; Kasimir, M.T.; Silberhumer, G.; Seebacher, G.; Wolner, E.; Simon, P.; Weigel, G. Decellularization protocols of porcine heart valves differ importantly in efficiency of cell removal and susceptibility of the matrix to recellularization with human vascular cells. J. Thorac. Cardiovasc. Surg. 2004, 127, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, N.C.; Rieder, F.; Wynn, T.A. Fibrosis: From mechanisms to medicines. Nature 2020, 587, 555–566. [Google Scholar] [CrossRef]
- Zahm, J.M.; Kaplan, H.; Hérard, A.L.; Doriot, F.; Pierrot, D.; Somelette, P.; Puchelle, E. Cell migration and proliferation during the in vitro wound repair of the respiratory epithelium. Cell Motil. Cytoskelet. 1997, 37, 33–43. [Google Scholar] [CrossRef]
- GonfiOtti, A.; Jaus, M.O.; Barale, D.; Baiguera, S.; Comin, C.; Lavorini, F.; Fontana, G.; Sibila, O.; Rombolà, G.; Jungebluth, P.; et al. The first tissue-engineered airway transplantation: 5-year follow-up results. Lancet 2014, 383, 238–244. [Google Scholar] [CrossRef]
- Genden, E.M.; Iskander, A.; Bromberg, J.S.; Mayer, L. The kinetics and pattern of tracheal allograft re-epithelialization. Am. J. Respir. Cell Mol. Biol. 2003, 28, 673–681. [Google Scholar] [CrossRef]
- Balyasin, M.V.; Baranovskii, D.S.; Demchenko, A.G.; Fayzullin, A.L.; Krasilnikova, O.A.; Klabukov, I.D.; Krasheninnikov, M.E.; Lyundup, A.V.; Parshin, V.D. Experimental orthotopic implantation of the tissue-engineered graft of trachea based on devitalized scaffold seeded with mesenchymal and epithelial cells. Vestn. Transpl. Iskusstv. Organov 2019, 21, 96–107. [Google Scholar] [CrossRef]
- Hunt, N.C.; Shelton, R.M.; Grover, L.M. Reversible mitotic and metabolic inhibition following the encapsulation of fibroblasts in alginate hydrogels. Biomaterials 2009, 30, 6435–6443. [Google Scholar] [CrossRef]
- Sueyoshi, S.; Chitose, S.I.; Sato, K.; Fukahori, M.; Kurita, T.; Umeno, H. Stable Tracheal Regeneration Using Organotypically Cultured Tissue Composed of Autologous Chondrocytes and Epithelial Cells in Beagles. Ann. Otol. Rhinol. Laryngol. 2019, 128, 585–594. [Google Scholar] [CrossRef]
- Kanzaki, M.; Onuki, T.; Yamato, M.; Hatakeyama, H.; Kohno, C.; Yang, J.; Umemoto, T.; Kikuchi, A.; Okano, T.; Onuki, T. Tissue engineered epithelial cell sheets for the creation of a bioartificial trachea. Tissue Eng. 2006, 12, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Den Hondt, M.; Vanaudenaerde, B.M.; Delaere, P.; Vranckx, J.J. Twenty years of experience with the rabbit model, a versatile model for tracheal transplantation research. Plast. Aesthetic Res. 2016, 3, 223. [Google Scholar] [CrossRef] [Green Version]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, L.H.; Tseng, Y.; Tseng, H.; Hung, S.-H. Partial Decellularization for Segmental Tracheal Scaffold Tissue Engineering: A Preliminary Study in Rabbits. Biomolecules 2021, 11, 866. https://doi.org/10.3390/biom11060866
Dang LH, Tseng Y, Tseng H, Hung S-H. Partial Decellularization for Segmental Tracheal Scaffold Tissue Engineering: A Preliminary Study in Rabbits. Biomolecules. 2021; 11(6):866. https://doi.org/10.3390/biom11060866
Chicago/Turabian StyleDang, Luong Huu, Yuan Tseng, How Tseng, and Shih-Han Hung. 2021. "Partial Decellularization for Segmental Tracheal Scaffold Tissue Engineering: A Preliminary Study in Rabbits" Biomolecules 11, no. 6: 866. https://doi.org/10.3390/biom11060866