
The Role of Androgens and Androgen Receptor in Human Bladder Cancer


 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
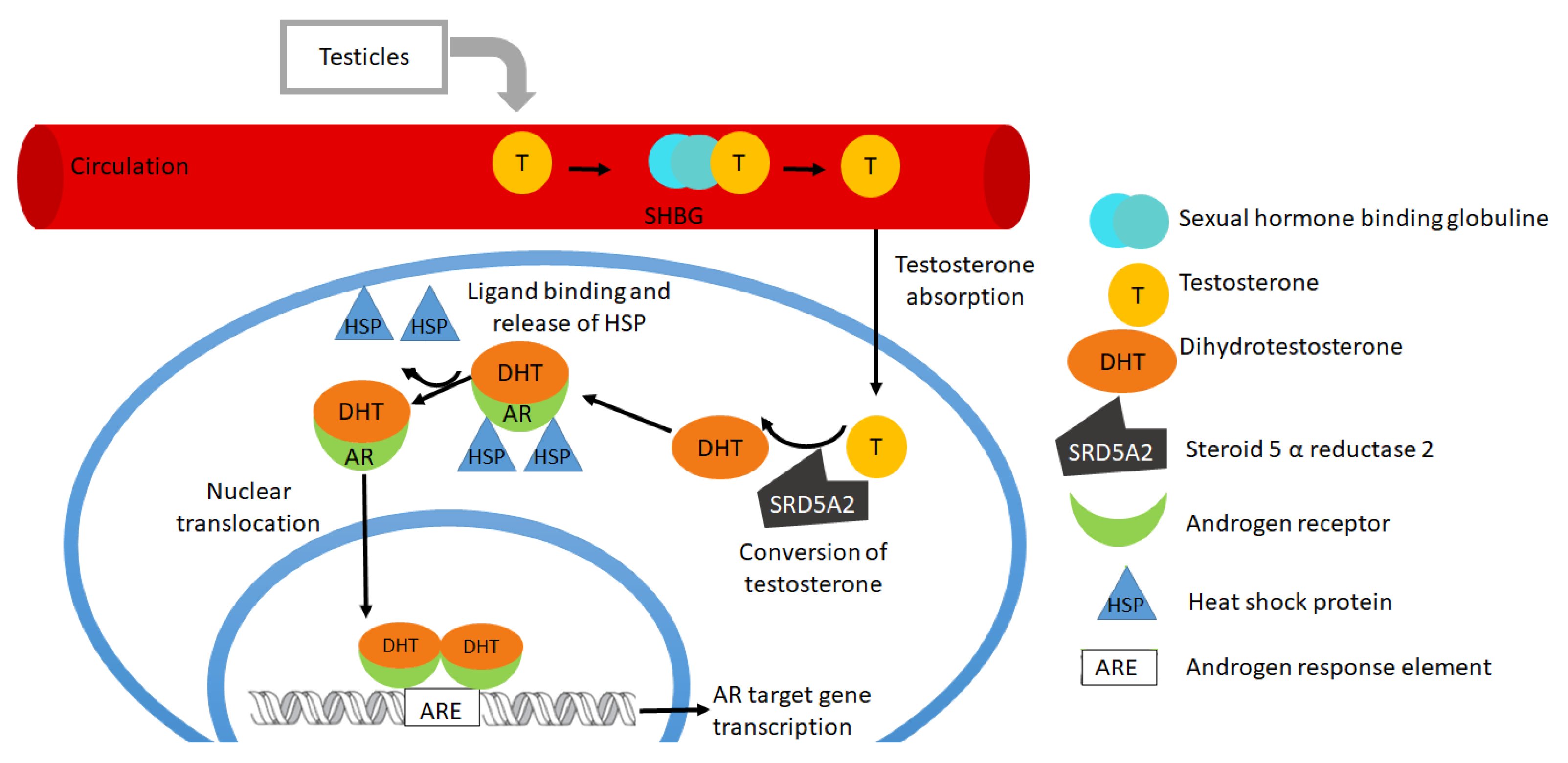
2. Structure of Androgens and Androgen Receptors
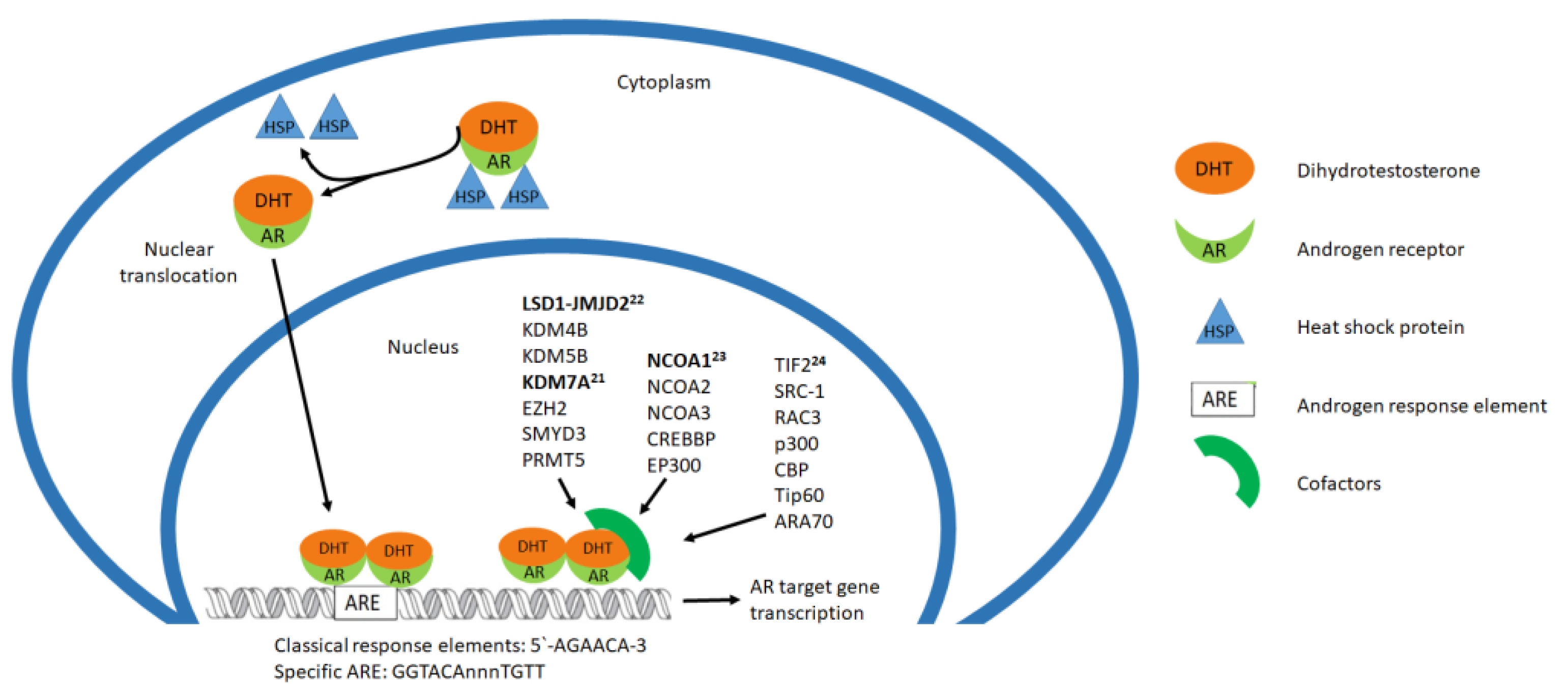
3. Activation of Androgen Receptor and Cofactors
4. Physiological Role of Androgen Receptors
5. Classification of Bladder Cancer and Its Risk Factors
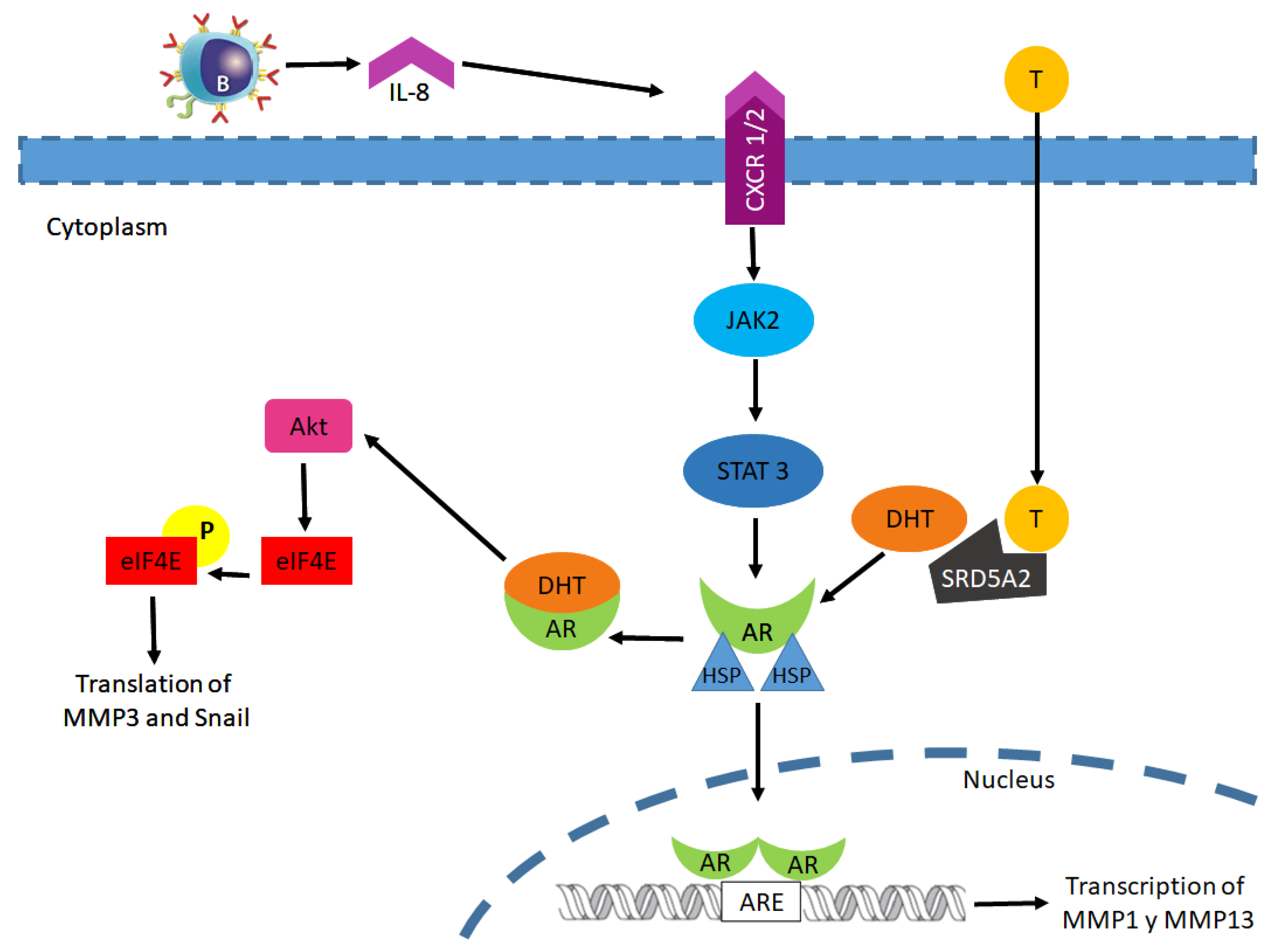
6. AR Signaling in Bladder Cancer Carcinogenesis: Initiation and Promotion
7. AR Signaling and Bladder Cancer Progression
8. Bladder Cancer Therapies
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lenis, A.T.; Lec, P.M.; Chamie, K. Mshs Bladder Cancer. JAMA 2020, 324, 1980–1991. [Google Scholar] [CrossRef]
- American Cancer Society. Available online: https://www.cancer.org/content/dam/CRC/PDF/Public/8557.00.pdf (accessed on 11 January 2021).
- Wang, C.-S.; Li, C.-C.; Juan, Y.-S.; Wu, W.-J.; Lee, H.-Y. 5α-reductase inhibitors impact prognosis of urothelial carcinoma. BMC Cancer 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Hu, H.; Zhou, H.; Xu, D. A review of the effects and molecular mechanisms of dimethylcurcumin (ASC-J9) on androgen receptor-related diseases. Chem. Biol. Drug Des. 2021, 97, 821–835. [Google Scholar] [CrossRef]
- Wang, D.; Li, M.; Li, J.; Wan, X.; Huang, Y.; Wang, C.; Zhang, P.; Xu, Y.; Kong, Z.; Lu, Y.; et al. Comprehensive Characterization of Androgen-Responsive lncRNAs Mediated Regulatory Network in Hormone-Related Cancers. Dis. Markers 2020, 2020, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Chen, J.; Miyamoto, H. Androgen Receptor Signaling in Bladder Cancer. Cancers 2017, 9, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brzozowska, M.; Lewiński, A. Changes of androgens levels in menopausal women. Menopausal Rev. 2020, 19, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Estébanez-Perpiñá, E.; Bevan, C.; McEwan, I. Eighty Years of Targeting Androgen Receptor Activity in Prostate Cancer: The Fight Goes on. Cancers 2021, 13, 509. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-M.; Guan, Z.-X.; Wang, F.; Zhang, D.; Ding, H. Application of Machine Learning Methods in Predicting Nuclear Receptors and their Families. Med. Chem. 2020, 16, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.P.H.; A Cidlowski, J.; Kelly, E.; Mathie, A.; A Peters, J.; Veale, E.L.; Armstrong, J.F.; Faccenda, E.; Harding, S.D.; Pawson, A.J.; et al. THE CONCISE GUIDE TO PHARMACOLOGY 2019/20: Nuclear hormone receptors. Br. J. Pharmacol. 2019, 176, S229–S246. [Google Scholar] [CrossRef] [Green Version]
- Narayanan, R.; Coss, C.C.; Dalton, J.T. Development of selective androgen receptor modulators (SARMs). Mol. Cell. Endocrinol. 2018, 465, 134–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter, B.A.; Ortiz, M.A.; Bratslavsky, G.; Kotula, L. Structure and Function of the Nuclear Receptor Superfamily and Current Targeted Therapies of Prostate Cancer. Cancers 2019, 11, 1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishigami-Yuasa, M.; Kagechika, H. Chemical Screening of Nuclear Receptor Modulators. Int. J. Mol. Sci. 2020, 21, 5512. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, A.; Gupta, S. Androgen receptor in bladder cancer: A promising therapeutic target. Asian J. Urol. 2020, 7, 284–290. [Google Scholar] [CrossRef]
- Aurilio, G.; Cimadamore, A.; Mazzucchelli, R.; Lopez-Beltran, A.; Verri, E.; Scarpelli, M.; Massari, F.; Cheng, L.; Santoni, M.; Montironi, R. Androgen Receptor Signaling Pathway in Prostate Cancer: From Genetics to Clinical Applications. Cells 2020, 9, 2653. [Google Scholar] [CrossRef]
- Messner, E.A.; Steele, T.M.; Tsamouri, M.M.; Hejazi, N.; Gao, A.C.; Mudryj, M.; Ghosh, P.M. The Androgen Receptor in Prostate Cancer: Effect of Structure, Ligands and Spliced Variants on Therapy. Biomedicines 2020, 8, 422. [Google Scholar] [CrossRef]
- Wen, S.; Niu, Y.; Huang, H. Posttranslational regulation of androgen dependent and independent androgen receptor activities in prostate cancer. Asian J. Urol. 2020, 7, 203–218. [Google Scholar] [CrossRef]
- Eftekharzadeh, B.; Banduseela, V.C.; Chiesa, G.; Martínez-Cristóbal, P.; Rauch, J.N.; Nath, S.R.; Schwarz, D.M.C.; Shao, H.; Marin-Argany, M.; Di Sanza, C.; et al. Hsp70 and Hsp40 inhibit an inter-domain interaction necessary for transcriptional activity in the androgen receptor. Nat. Commun. 2019, 10, 1–14. [Google Scholar] [CrossRef]
- Senapati, D.; Kumari, S.; Heemers, H.V. Androgen receptor co-regulation in prostate cancer. Asian J. Urol. 2020, 7, 219–232. [Google Scholar] [CrossRef]
- Liu, S.; Kumari, S.; Hu, Q.; Senapati, D.; Venkadakrishnan, V.B.; Wang, D.; DePriest, A.D.; E Schlanger, S.; Ben-Salem, S.; Valenzuela, M.M.; et al. A comprehensive analysis of coregulator recruitment, androgen receptor function and gene expression in prostate cancer. eLife 2017, 6, e28482. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-H.; Kim, B.-C.; Jeong, S.-H.; Jeong, C.W.; Ku, J.H.; Kim, H.H.; Kwak, C. Histone Demethylase KDM7A Regulates Androgen Receptor Activity, and Its Chemical Inhibitor TC-E 5002 Overcomes Cisplatin-Resistance in Bladder Cancer Cells. Int. J. Mol. Sci. 2020, 21, 5658. [Google Scholar] [CrossRef]
- Kauffman, E.C.; Robinson, B.D.; Downes, M.J.; Powell, L.G.; Lee, M.M.; Scherr, D.S.; Gudas, L.J.; Mongan, N.P. Role of androgen receptor and associated lysine-demethylase coregulators, LSD1 and JMJD2A, in localized and advanced human bladder cancer. Mol. Carcinog. 2011, 50, 931–944. [Google Scholar] [CrossRef] [Green Version]
- A Boorjian, S.; Heemers, H.V.; Frank, I.; A Farmer, S.; Schmidt, L.J.; Sebo, T.J.; Tindall, D.J. Expression and significance of androgen receptor coactivators in urothelial carcinoma of the bladder. Endocrine-Related Cancer 2009, 16, 123–137. [Google Scholar] [CrossRef] [Green Version]
- Fancher, A.T.; Hua, Y.; Strock, C.J.; Johnston, P.A. Assays to Interrogate the Ability of Compounds to Inhibit the AF-2 or AF-1 Transactivation Domains of the Androgen Receptor. ASSAY Drug Dev. Technol. 2019, 17, 364–386. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Yi, P.; Hamilton, R.A.; Shen, H.; Chen, M.; Foulds, C.E.; Mancini, M.A.; Ludtke, S.J.; Wang, Z.; O’Malley, B.W. Structural Insights of Transcriptionally Active, Full-Length Androgen Receptor Coactivator Complexes. Mol. Cell 2020, 79, 812–823.e4. [Google Scholar] [CrossRef] [PubMed]
- Stallcup, M.R.; Poulard, C. Gene-Specific Actions of Transcriptional Coregulators Facilitate Physiological Plasticity: Evidence for a Physiological Coregulator Code. Trends Biochem. Sci. 2020, 45, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Venkadakrishnan, V.B.; Ben-Salem, S.; Heemers, H.V. AR-dependent phosphorylation and phospho-proteome targets in prostate cancer. Endocrine-Related Cancer 2020, 27, R193–R210. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Chen, Q.; Liu, Y.; Wen, X. Baicalein suppresses the androgen receptor (AR)-mediated prostate cancer progression via inhibiting the AR N-C dimerization and AR-coactivators interaction. Oncotarget 2017, 8, 105561–105573. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.; Kesten, N.; Font-Tello, A.; Chang, M.E.K.; Vadhi, R.; Lim, K.; Flory, M.R.; Cejas, P.; Mohammed, H.; Long, H.W.; et al. ERG-Mediated Coregulator Complex Formation Maintains Androgen Receptor Signaling in Prostate Cancer. Cancer Res. 2020, 80, 4612–4619. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Shi, X.; Li, Y.; Xiao, Y.; Butler, W.; Huang, Y.; Du, L.; Wu, T.; Bian, X.; Shi, G.; et al. LINC00675 activates androgen receptor axis signaling pathway to promote castration-resistant prostate cancer progression. Cell Death Dis. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Fan, H.; Hou, J.; Liu, S.; Xiao, Z.; Cui, J. Long Non-Coding RNA DARS-AS1 Contributes to Prostate Cancer Progression Through Regulating the MicroRNA-628-5p/MTDH Axis. Cancer Manag. Res. 2020, ume 12, 8363–8377. [Google Scholar] [CrossRef]
- Eringyte, I.; Losada, J.N.Z.; Powell, S.M.; Bevan, C.L.; Fletcher, C.E. Coordinated AR and microRNA regulation in prostate cancer. Asian J. Urol. 2020, 7, 233–250. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-W.; Wen, S.; Chen, L.; Wei, Y.; Niu, Y.; Zhao, Y. Functional roles of antisense enhancer RNA for promoting prostate cancer progression. Theranostics 2021, 11, 1780–1794. [Google Scholar] [CrossRef]
- Gibson, D.A.; Saunders, P.T.; McEwan, I.J. Androgens and androgen receptor: Above and beyond. Mol. Cell. Endocrinol. 2018, 465, 1–3. [Google Scholar] [CrossRef]
- Rey, R.A.; Grinspon, R.P. Androgen Treatment in Adolescent Males with Hypogonadism. Am. J. Men’s Health 2020, 14, 1557988320922443. [Google Scholar] [CrossRef] [PubMed]
- Bienenfeld, A.; Azarchi, S.; Sicco, K.L.; Marchbein, S.; Shapiro, J.; Nagler, A.R. Androgens in women. J. Am. Acad. Dermatol. 2019, 80, 1497–1506. [Google Scholar] [CrossRef]
- A Skiba, M.; Bell, R.J.; Islam, R.M.; Handelsman, D.J.; Desai, R.; Davis, S.R. Androgens During the Reproductive Years: What Is Normal for Women? J. Clin. Endocrinol. Metab. 2019, 104, 5382–5392. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.M.; McPhaul, M.J. A and B forms of the androgen receptor are expressed in a variety of human tissues. Mol. Cell. Endocrinol. 1996, 120, 51–57. [Google Scholar] [CrossRef]
- Zhang, X.P.; Zhang, W.Y.; Huo, F.; Hu, H.; Wang, Q.; Xu, K.X. Outcome of surgical management and pathogenesis of female primary bladder neck obstruction. Beijing Da Xue Xue Bao Yi Xue Ban 2019, 51, 1052–1055. [Google Scholar] [CrossRef] [PubMed]
- Chavalmane, A.K.; Comeglio, P.; Morelli, A.; Filippi, S.; Fibbi, B.; Vignozzi, L.; Sarchielli, E.; Marchetta, M.; Failli, P.; Sandner, P.; et al. Sex Steroid Receptors in Male Human Bladder: Expression and Biological Function. J. Sex. Med. 2010, 7, 2698–2713. [Google Scholar] [CrossRef] [PubMed]
- Lombard, A.P.; Mudryj, M. The emerging role of the androgen receptor in bladder cancer. Endocrine-Related Cancer 2015, 22, R265–R277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magari, T.; Shibata, Y.; Arai, S.; Kashiwagi, B.; Suzuki, K.; Suzuki, K. Time-dependent effects of castration on the bladder function and histological changes in the bladder and blood vessels. Asian J. Androl. 2014, 16, 457–460. [Google Scholar] [CrossRef]
- Tuygun, C.; Kankaya, D.; Imamoglu, A.; Sertçelik, A.; Zengin, K.; Oktay, M.; Sertcelik, N. Sex-specific hormone receptors in urothelial carcinomas of the human urinary bladder: A comparative analysis of clinicopathological features and survival outcomes according to receptor expression. Urol. Oncol. Semin. Orig. Investig. 2011, 29, 43–51. [Google Scholar] [CrossRef]
- Mashhadi, R.; Pourmand, G.; Kosari, F.; Mehrsai, A.; Salem, S.; Pourmand, M.R.; Alatab, S.; Khonsari, M.; Heydari, F.; Beladi, L.; et al. Role of steroid hormone receptors in formation and progression of bladder carcinoma: A case-control study. Urol. J. 2014, 11, 1968–1976. [Google Scholar] [PubMed]
- Farling, K.B. Bladder cancer. Nurse Pr. 2017, 42, 26–33. [Google Scholar] [CrossRef] [PubMed]
- McBeth, L.; Grabnar, M.; Selman, S.; Hinds, T.D. Involvement of the Androgen and Glucocorticoid Receptors in Bladder Cancer. Int. J. Endocrinol. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Hata, S.; Ise, K.; Azmahani, A.; Konosu-Fukaya, S.; McNamara, K.M.; Fujishima, F.; Shimada, K.; Mitsuzuka, K.; Arai, Y.; Sasano, H.; et al. Expression of AR, 5αR1 and 5αR2 in bladder urothelial carcinoma and relationship to clinicopathological factors. Life Sci. 2017, 190, 15–20. [Google Scholar] [CrossRef]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Mo, Q.; Shen, H.; Wang, S.; Liu, B. Reproductive and hormonal factors and bladder cancer risk: A prospective study and meta-analysis. Aging 2020, 12, 14691–14698. [Google Scholar] [CrossRef]
- Chen, J.; Cui, Y.; Li, P.; Liu, L.; Li, C.; Zu, X. Expression and clinical significance of androgen receptor in bladder cancer: A meta-analysis. Mol. Clin. Oncol. 2017, 7, 919–927. [Google Scholar] [CrossRef] [Green Version]
- Dobruch, J.; Daneshmand, S.; Fisch, M.; Lotan, Y.; Noon, A.P.; Resnick, M.J.; Shariat, S.F.; Zlotta, A.R.; Boorjian, S.A. Gender and Bladder Cancer: A Collaborative Review of Etiology, Biology, and Outcomes. Eur. Urol. 2016, 69, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Jalloh, M.; Cassell, A.; Diallo, T.; Gaye, O.; Ndoye, M.; Mbodji, M.M.; Mahamat, M.A.; Diallo, A.; Dial, C.; Labou, I.; et al. Is Schistosomiasis a Risk Factor for Bladder Cancer? Evidence-Based Facts. J. Trop. Med. 2020, 2020, 1–6. [Google Scholar] [CrossRef]
- Fouad, Y.A.; Aanei, C. Revisiting the hallmarks of cancer. Am. J. Cancer Res. 2017, 7, 1016–1036. [Google Scholar]
- Izumi, K.; Zheng, Y.; Hsu, J.-W.; Chang, C.; Miyamoto, H. Androgen receptor signals regulate UDP-glucuronosyltransferases in the urinary bladder: A potential mechanism of androgen-induced bladder carcinogenesis. Mol. Carcinog. 2011, 52, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Dehm, S.; Tindall, D.J. Prostate Cancer: Cellular and Genetic Mechanisms of Disease Development and Progression; Springe Nature Publisher: ChamCity, Switzerland, 2019; Volume 14, pp. 319–332. [Google Scholar]
- Ide, H.; Mizushima, T.; Jiang, G.; Goto, T.; Nagata, Y.; Teramoto, Y.; Inoue, S.; Li, Y.; Kashiwagi, E.; Baras, A.S.; et al. FOXO1 as a tumor suppressor inactivated via AR/ERβ signals in urothelial cells. Endocrine-Related Cancer 2020, 27, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Quan, Z.; Zhong, B.; Zhang, M.; Zhou, B.; Wang, S.; Luo, X.; Tang, C. lncRNA XIST promotes glioma proliferation and metastasis through miR-133a/SOX4. Exp. Ther. Med. 2020, 19, 1641–1648. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Cao, M.; Zhang, J.; Li, X.; Sun, Q. LncRNA XIST modulates HIF-1A/AXL signaling pathway by inhibiting miR-93-5p in colorectal cancer. Mol. Genet. Genom. Med. 2020, 8, e1112. [Google Scholar] [CrossRef] [Green Version]
- Hai, B.; Pan, X.; Du, C.; Mao, T.; Jia, F.; Liu, Y.; Ma, Y.; Liu, X.; Zhu, B. LncRNA XIST Promotes Growth of Human Chordoma Cells by Regulating miR-124-3p/iASPP Pathway. OncoTargets Ther. 2020, ume 13, 4755–4765. [Google Scholar] [CrossRef]
- Zachari, M.; Longo, M.; Ganley, I.G. Aberrant autophagosome formation occurs upon small molecule inhibition of ULK1 kinase activity. Life Sci. Alliance 2020, 3, e202000815. [Google Scholar] [CrossRef] [PubMed]
- Gerada, C.; Ryan, K.M. Autophagy, the innate immune response and cancer. Mol. Oncol. 2020, 14, 1913–1929. [Google Scholar] [CrossRef]
- Demeter, A.; Romero-Mulero, M.C.; Csabai, L.; Ölbei, M.; Sudhakar, P.; Haerty, W.; Korcsmáros, T. ULK1 and ULK2 are less redundant than previously thought: Computational analysis uncovers distinct regulation and functions of these autophagy induction proteins. Sci. Rep. 2020, 10, 10940. [Google Scholar] [CrossRef]
- Hao, K.; Zhao, S.; Cui, D.; Zhang, Y.; Jiang, C.; Jing, Y.; Xia, S.; Han, B. Androgen receptor antagonist bicalutamide induces autophagy and apoptosis via ULK2 upregulation in human bladder cancer cells. Int. J. Clin. Exp. Pathol. 2017, 10, 7603–7615. [Google Scholar]
- Inoue, S.; Mizushima, T.; Ide, H.; Jiang, G.; Goto, T.; Nagata, Y.; Netto, G.J.; Miyamoto, H. ATF2 promotes urothelial cancer outgrowth via cooperation with androgen receptor signaling. Endocr. Connect. 2018, 7, 1397–1408. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Wang, L.; Li, Y.; Chen, M.; He, W.; Qi, L. The Long Non-Coding RNA XIST Interacted with MiR-124 to Modulate Bladder Cancer Growth, Invasion and Migration by Targeting Androgen Receptor (AR). Cell. Physiol. Biochem. 2017, 43, 405–418. [Google Scholar] [CrossRef] [Green Version]
- Xie, X.-Q.; Wang, M.-J.; Li, Y.; Lei, L.-P.; Wang, N.; Lv, Z.-Y.; Chen, K.-L.; Zhou, B.; Ping, J.; Zhou, Z.-G.; et al. miR-124 Intensified Oxaliplatin-Based Chemotherapy by Targeting CAPN2 in Colorectal Cancer. Mol. Ther. Oncolytics 2020, 17, 320–331. [Google Scholar] [CrossRef] [PubMed]
- Katleba, K.; Lombard, A.P.; Tsamouri, M.-M.; Baek, H.B.; Nishida, K.S.; Libertini, S.J.; Platero, A.J.; Ma, A.-H.; Pan, C.-X.; Ghosh, P.M.; et al. Depletion of androgen receptor low molecular weight isoform reduces bladder tumor cell viability and induces apoptosis. Cancer Lett. 2021, 504, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Gil, D.; Zarzycka, M.; Dulińska-Litewka, J.; Ciołczyk-Wierzbicka, D.; Lekka, M.; Laidler, P. Dihydrotestosterone increases the risk of bladder cancer in men. Hum. Cell 2019, 32, 379–389. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.K.; Sadar, M.D. Non-Genomic Actions of the Androgen Receptor in Prostate Cancer. Front. Endocrinol. 2017, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robichaud, N.; Del Rincon, S.V.; Huor, B.; Alain, T.; A Petruccelli, L.; Hearnden, J.; Goncalves, C.; Grotegut, S.; Spruck, C.H.; Furic, L.; et al. Phosphorylation of eIF4E promotes EMT and metastasis via translational control of SNAIL and MMP-3. Oncogene 2015, 34, 2032–2042. [Google Scholar] [CrossRef] [Green Version]
- Dai, S.; Wei, S.; Zhang, C.; Li, X.; Liu, Y.; Ma, M.; Lv, H.; Zhang, Z.; Zhao, L.; Shan, B. MTA2 promotes the metastasis of esophageal squamous cell carcinoma via EIF4E-Twist feedback loop. Cancer Sci. 2021, 112, 1060–1074. [Google Scholar] [CrossRef]
- Cao, Y.; Tian, T.; Li, W.; Xu, H.; Zhan, C.; Wu, X.; Wang, C.; Wu, X.; Wu, W.; Zheng, S.; et al. Long non-coding RNA in bladder cancer. Clin. Chim. Acta 2020, 503, 113–121. [Google Scholar] [CrossRef]
- Goossens, S.; Vandamme, N.; Van Vlierberghe, P.; Berx, G. EMT transcription factors in cancer development re-evaluated: Beyond EMT and MET. Biochim. Biophys. Acta BBA Bioenerg. 2017, 1868, 584–591. [Google Scholar] [CrossRef]
- Scheau, C.; Badarau, I.A.; Costache, R.; Caruntu, C.; Mihai, G.L.; Didilescu, A.C.; Constantin, C.; Neagu, M. The Role of Matrix Metalloproteinases in the Epithelial-Mesenchymal Transition of Hepatocellular Carcinoma. Anal. Cell. Pathol. 2019, 2019, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Ou, D.-H.; Zhuang, D.-W.; Zheng, Z.-F.; Lin, M.-E. In silico analysis of the immune microenvironment in bladder cancer. BMC Cancer 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ou, Z.; Wang, Y.; Liu, L.; Li, L.; Yeh, S.; Qi, L.; Chang, C. Tumor microenvironment B cells increase bladder cancer metastasisviamodulation of the IL-8/androgen receptor (AR)/MMPs signals. Oncotarget 2015, 6, 26065–26078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Sun, Y.; Ou, Z.; Yeh, S.; Huang, C.; You, B.; Tsai, Y.; Sheu, T.; Zu, X.; Chang, C. Androgen receptor-regulated circ FNTA activates KRAS signaling to promote bladder cancer invasion. EMBO Rep. 2020, 21, e48467. [Google Scholar] [CrossRef] [PubMed]
- Barbon, A.; Magri, C. RNA Editing and Modifications in Mood Disorders. Genes 2020, 11, 872. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Koh, M.; Moon, A. Farnesyl transferase inhibitor FTI-277 inhibits breast cell invasion and migration by blocking H-Ras activation. Oncol. Lett. 2016, 12, 2222–2226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ide, H.; Inoue, S.; Miyamoto, H. Histopathological and prognostic significance of the expression of sex hormone receptors in bladder cancer: A meta-analysis of immunohistochemical studies. PLoS ONE 2017, 12, e0174746. [Google Scholar] [CrossRef]
- DeGeorge, K.C.; Holt, H.R.; & Hodges, S.C. Bladder Cancer: Diagnosis and Treatment. Am. Fam. Physician 2017, 96, 507–514. [Google Scholar]
- Matulewicz, R.S.; Steinberg, G.D. Non-muscle-invasive Bladder Cancer: Overview and Contemporary Treatment Land-scape of Neoadjuvant Chemoablative Therapies. Rev. Urol. 2020, 22, 43–51. [Google Scholar]
- Cho, E.; Bang, C.K.; Kim, H.; Lee, H.K. An ensemble approach of urine sediment image analysis and NMP22 test for detection of bladder cancer cells. J. Clin. Lab. Anal. 2020, 34, e23345. [Google Scholar] [CrossRef]
- Ikeda, A.; Kojima, T.; Kawai, K.; Hinotsu, S.; Keino, N.; Shiga, K.; Miyake, H.; Miyata, Y.; Enomoto, Y.; Shimizu, F.; et al. Risk for intravesical recurrence of bladder cancer stratified by the results on two consecutive UroVysion fluorescence in situ hybridization tests: A prospective follow-up study in Japan. Int. J. Clin. Oncol. 2020, 25, 1163–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zang, Y.; Li, X.; Cheng, Y.; Qi, F.; Yang, N. An overview of patients with urothelial bladder cancer over the past two decades: A Surveillance, Epidemiology, and End Results (SEER) study. Ann. Transl. Med. 2020, 8, 1587. [Google Scholar] [CrossRef]
- Satyal, U.; Sikder, R.K.; McConkey, D.; Plimack, E.R.; Abbosh, P.H. Clinical implications of molecular subtyping in bladder cancer. Curr. Opin. Urol. 2019, 29, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, J.; Lamy, P.; Nordentoft, I.; Algaba, F.; Høyer, S.; Ulhøi, B.P.; Vang, S.; Reinert, T.; Hermann, G.G.; Mogensen, K.; et al. Comprehensive Transcriptional Analysis of Early-Stage Urothelial Carcinoma. Cancer Cell 2016, 30, 27–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurst, C.D.; Alder, O.; Platt, F.M.; Droop, A.; Stead, L.F.; Burns, J.E.; Burghel, G.J.; Jain, S.; Klimczak, L.J.; Lindsay, H.; et al. Genomic Subtypes of Non-invasive Bladder Cancer with Distinct Metabolic Profile and Female Gender Bias in KDM6A Mutation Frequency. Cancer Cell 2017, 32, 701–715.e7. [Google Scholar] [CrossRef] [PubMed]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; van Rhijn, B.W.; Winters, B.; Douglas, J.; Van Kessel, K.E.; van de Putte, E.E.F.; Sommerlad, M.; Wang, N.Q.; et al. Impact of Molecular Subtypes in Muscle-invasive Bladder Cancer on Predicting Response and Survival after Neoadjuvant Chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Fong, M.H.Y.; Feng, M.; McConkey, D.J.; Choi, W. Update on bladder cancer molecular subtypes. Transl. Androl. Urol. 2020, 9, 2881–2889. [Google Scholar] [CrossRef]
- Kamoun, A.; de Reyniès, A.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef]
- McConkey, D.J.; Choi, W. Molecular Subtypes of Bladder Cancer. Curr. Oncol. Rep. 2018, 20, 77. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.C.; Bondaruk, J.; Yao, H.; Wang, Z.; Zhang, L.; Lee, S.; Lee, J.-G.; Cogdell, D.; Zhang, M.; Yang, G.; et al. Assessment of Luminal and Basal Phenotypes in Bladder Cancer. Sci. Rep. 2020, 10, 9743. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Beltran, A.; Cimadamore, A.; Blanca, A.; Massari, F.; Vau, N.; Scarpelli, M.; Cheng, L.; Montironi, R. Immune Checkpoint Inhibitors for the Treatment of Bladder Cancer. Cancers 2021, 13, 131. [Google Scholar] [CrossRef] [PubMed]
- International Collaboration of Trialists on behalf of the Medical Research Council Advanced Bladder Cancer Working Party (now the National Cancer Research Institute Bladder Cancer Clinical Studies Group), the European Organisation for Research and Treatme International Phase III Trial Assessing Neoadjuvant Cisplatin, Methotrexate, and Vinblastine Chemotherapy for Muscle-Invasive Bladder Cancer: Long-Term Results of the BA06 30894 Trial. J. Clin. Oncol. 2011, 29, 2171–2177. [CrossRef] [Green Version]
- Jiang, D.M.; Gupta, S.; Kitchlu, A.; Meraz-Munoz, A.; North, S.A.; Alimohamed, N.S.; Blais, N.; Sridhar, S.S. Defining cisplatin eligibility in patients with muscle-invasive bladder cancer. Nat. Rev. Urol. 2021, 18, 104–114. [Google Scholar] [CrossRef]
- Reesink, D.J.; Van De Garde, E.M.W.; Peters, B.J.M.; Van Der Nat, P.B.; Los, M.; Horenblas, S.; Van Melick, H.H.E. Treatment patterns and clinical outcomes of chemotherapy treatment in patients with muscle-invasive or metastatic bladder cancer in the Netherlands. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Jiang, D.M.; Chung, P.; Kulkarni, G.S.; Sridhar, S.S. Trimodality Therapy for Muscle-Invasive Bladder Cancer: Recent Advances and Unanswered Questions. Curr. Oncol. Rep. 2020, 22, 14. [Google Scholar] [CrossRef]
- Lim, C.J.; Nguyen, P.H.D.; Wasser, M.; Kumar, P.; Lee, Y.H.; Nasir, N.J.M.; Chua, C.; Lai, L.; Hazirah, S.N.; Loh, J.J.H.; et al. Immunological Hallmarks for Clinical Response to BCG in Bladder Cancer. Front. Immunol. 2021, 11, 615091. [Google Scholar] [CrossRef]
- Srivastava, A.; Rathore, S.; Munshi, A.; Ramesh, R. Extracellular Vesicles in Oncology: From Immune Suppression to Immunotherapy. AAPS J. 2021, 23, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Knox, M.C.; Ni, J.; Bece, A.; Bucci, J.; Chin, Y.; Graham, P.H.; Li, Y. A Clinician’s Guide to Cancer-Derived Exosomes: Immune Interactions and Therapeutic Implications. Front. Immunol. 2020, 11, 1612. [Google Scholar] [CrossRef] [PubMed]
- Lodewijk, I.; Dueñas, M.; Rubio, C.; Munera-Maravilla, E.; Segovia, C.; Bernardini, A.; Teijeira, A.; Paramio, J.M.; Suárez-Cabrera, C. Liquid Biopsy Biomarkers in Bladder Cancer: A Current Need for Patient Diagnosis and Monitoring. Int. J. Mol. Sci. 2018, 19, 2514. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.K.; Liao, J.; Li, M.S.; Khoo, B.L. Urine biopsy technologies: Cancer and beyond. Theranostics 2020, 10, 7872–7888. [Google Scholar] [CrossRef]
- Piao, X.-M.; Cha, E.-J.; Yun, S.J.; Kim, W.-J. Role of Exosomal miRNA in Bladder Cancer: A Promising Liquid Biopsy Biomarker. Int. J. Mol. Sci. 2021, 22, 1713. [Google Scholar] [CrossRef]
- Cavallari, I.; Grassi, A.; Del Bianco, P.; Aceti, A.; Zaborra, C.; Sharova, E.; Bertazzolo, I.; D’Agostino, D.M.; Iafrate, M.; Ciminale, V. Prognostic Stratification of Bladder Cancer Patients with a MicroRNA-based Approach. Cancers 2020, 12, 3133. [Google Scholar] [CrossRef]
- Liu, Y.-L.; Wang, X.-L.; Yang, X.-H.; Wu, X.-H.; He, G.-X.; Xie, L.-M.; Cao, X.-J.; Guo, X.-G. Pooled analysis of Xpert Bladder Cancer based on the 5 mRNAs for rapid diagnosis of bladder carcinoma. World J. Surg. Oncol. 2021, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.; Hutchinson, L.; Tomaszewicz, K.; Caporelli, M.; Meng, X.; McCauley, K.; Fischer, A.H.; Cosar, E.F.; Cornejo, K.M. Diagnostic value of a comprehensive, urothelial carcinoma–specific next-generation sequencing panel in urine cytology and bladder tumor specimens. Cancer Cytopathol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhou, L.; Liu, L.; Hou, Y.; Xiong, M.; Yang, Y.; Hu, J.; Chen, K. Single-cell RNA sequencing highlights the role of inflammatory cancer-associated fibroblasts in bladder urothelial carcinoma. Nat. Commun. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Kang, H.W.; Kim, W.-J.; Choi, W.; Yun, S.J. Tumor heterogeneity in muscle-invasive bladder cancer. Transl. Androl. Urol. 2020, 9, 2866–2880. [Google Scholar] [CrossRef]
- Minkler, S.; Lucien, F.; Kimber, M.; Sahoo, D.; Bourgois-Mochel, A.; Musser, M.; Johannes, C.; Frank, I.; Cheville, J.; Allenspach, K.; et al. Emerging Roles of Urine-Derived Components for the Management of Bladder Cancer: One Man’s Trash Is Another Man’s Treasure. Cancers 2021, 13, 422. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaka, Y.; Uesawa, Y. Molecular Image-Based Prediction Models of Nuclear Receptor Agonists and Antagonists Using the DeepSnap-Deep Learning Approach with the Tox21 10K Library. Molecules 2020, 25, 2764. [Google Scholar] [CrossRef]
- Ide, H.; Miyamoto, H. The Role of Steroid Hormone Receptors in Urothelial Tumorigenesis. Cancers 2020, 12, 2155. [Google Scholar] [CrossRef]
- Miyamoto, H.; Yang, Z.; Chen, Y.-T.; Ishiguro, H.; Uemura, H.; Kubota, Y.; Nagashima, Y.; Chang, Y.-J.; Hu, Y.-C.; Tsai, M.-Y.; et al. Promotion of Bladder Cancer Development and Progression by Androgen Receptor Signals. J. Natl. Cancer Inst. 2007, 99, 558–568. [Google Scholar] [CrossRef] [Green Version]
- Moschini, M.; Zaffuto, E.; Karakiewicz, P.; Mattei, A.; Gandaglia, G.; Fossati, N.; Montorsi, F.; Briganti, A.; Shariat, S.F. The effect of androgen deprivation treatment on subsequent risk of bladder cancer diagnosis in male patients treated for prostate cancer. World J. Urol. 2019, 37, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Shiota, M.; Yokomizo, A.; Takeuchi, A.; Imada, K.; Kiyoshima, K.; Inokuchi, J.; Tatsugami, K.; Ohga, S.; Nakamura, K.; Honda, H.; et al. Secondary bladder cancer after anticancer therapy for prostate cancer: Reduced comorbidity after androgen-deprivation therapy. Oncotarget 2015, 6, 14710–14719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanguedolce, F.; Cormio, L.; Carrieri, G.; Calò, B.; Russo, D.; Menin, A.; Pastore, A.L.; Greco, F.; Bozzini, G.; Galfano, A.; et al. Role of androgen receptor expression in non-muscle-invasive bladder cancer: A systematic review and meta-analysis. Histol. Histopathol. 2019, 35, 423–432. [Google Scholar] [PubMed]
- Yang, Z.; Chen, J.; Xie, H.; Liu, T.; Chen, Y.; Ma, Z.; Pei, X.; Yang, W.; Li, L. Androgen receptor suppresses prostate cancer metastasis but promotes bladder cancer metastasis via differentially altering miRNA525-5p/SLPI-mediated vasculogenic mimicry formation. Cancer Lett. 2020, 473, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Yasui, M.; Kawahara, T.; Izumi, K.; Yao, M.; Ishiguro, Y.; Ishiguro, H.; Uemura, H.; Miyoshi, Y. Androgen receptor mRNA expression is a predictor for recurrence-free survival in non-muscle invasive bladder cancer. BMC Cancer 2019, 19, 331. [Google Scholar] [CrossRef]
- Gupta, S.; Dhillon, J.; Magliocco, A.M.; Puskas, J.; Caceres, G.; Masawi, F.; Doronin, Y.; Zhang, J. Results from a phase I/Ib trial of enzalutamide and gemcitabine and cisplatin in metastatic bladder cancer (mBC). J. Clin. Oncol. 2019, 37, 471. [Google Scholar] [CrossRef]
- Dellis, A.E.; Papatsoris, A.G. Perspectives on the current and emerging chemical androgen receptor antagonists for the treatment of prostate cancer. Expert Opin. Pharmacother. 2019, 20, 163–172. [Google Scholar] [CrossRef]
- De Velasco, M.A.; Kura, Y.; Sakai, K.; Hatanaka, Y.; Davies, B.R.; Campbell, H.; Klein, S.; Kim, Y.; MacLeod, A.R.; Sugimoto, K.; et al. Targeting castration-resistant prostate cancer with androgen receptor antisense oligonucleotide therapy. JCI Insight 2019, 4, 122688. [Google Scholar] [CrossRef]
- Huang, C.-P.; Chen, J.; Chen, C.-C.; Liu, G.; Zhang, Y.; Messing, E.; Yeh, S.; Chang, C. ASC-J9® increases the bladder cancer chemotherapy efficacy via altering the androgen receptor (AR) and NF-κB survival signals. J. Exp. Clin. Cancer Res. 2019, 38, 1–13. [Google Scholar] [CrossRef]
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02144051?term=NCT02144051&draw=2&rank=1. (accessed on 22 February 2021).
- Clinical Trials. Available online: https://clinicaltrials.gov/ct2/show/NCT02788201?term=NCT02788201&draw=2&rank=1 (accessed on 22 February 2021).
- Martínez-Rojo, E.; Cariño-Cortés, R.; Berumen, L.C.; García-Alcocer, G.; Escobar-Cabrera, J. Stevia Eupatoria and Stevia Pilosa Extracts Inhibit the Proliferation and Migration of Prostate Cancer Cells. Medicina 2020, 56, 90. [Google Scholar] [CrossRef] [Green Version]
- Hazafa, A.; Rehman, K.-U.-; Jahan, N.; Jabeen, Z. The Role of Polyphenol (Flavonoids) Compounds in the Treatment of Cancer Cells. Nutr. Cancer 2020, 72, 386–397. [Google Scholar] [CrossRef]
- Andl, T.; Ganapathy, K.; Bossan, A.; Chakrabarti, R. MicroRNAs as Guardians of the Prostate: Those Who Stand before Cancer. What Do We Really Know about the Role of microRNAs in Prostate Biology? Int. J. Mol. Sci. 2020, 21, 4796. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rojo, E.; Berumen, L.C.; García-Alcocer, G.; Escobar-Cabrera, J. The Role of Androgens and Androgen Receptor in Human Bladder Cancer. Biomolecules 2021, 11, 594. https://doi.org/10.3390/biom11040594
Martínez-Rojo E, Berumen LC, García-Alcocer G, Escobar-Cabrera J. The Role of Androgens and Androgen Receptor in Human Bladder Cancer. Biomolecules. 2021; 11(4):594. https://doi.org/10.3390/biom11040594
Chicago/Turabian StyleMartínez-Rojo, Elizabeth, Laura Cristina Berumen, Guadalupe García-Alcocer, and Jesica Escobar-Cabrera. 2021. "The Role of Androgens and Androgen Receptor in Human Bladder Cancer" Biomolecules 11, no. 4: 594. https://doi.org/10.3390/biom11040594