
Biological Rhythm and Chronotype: New Perspectives in Health

 , ,
, ,  ,
,  , and
, and {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Study Records (Selection and Data Collection Process)
3. Results
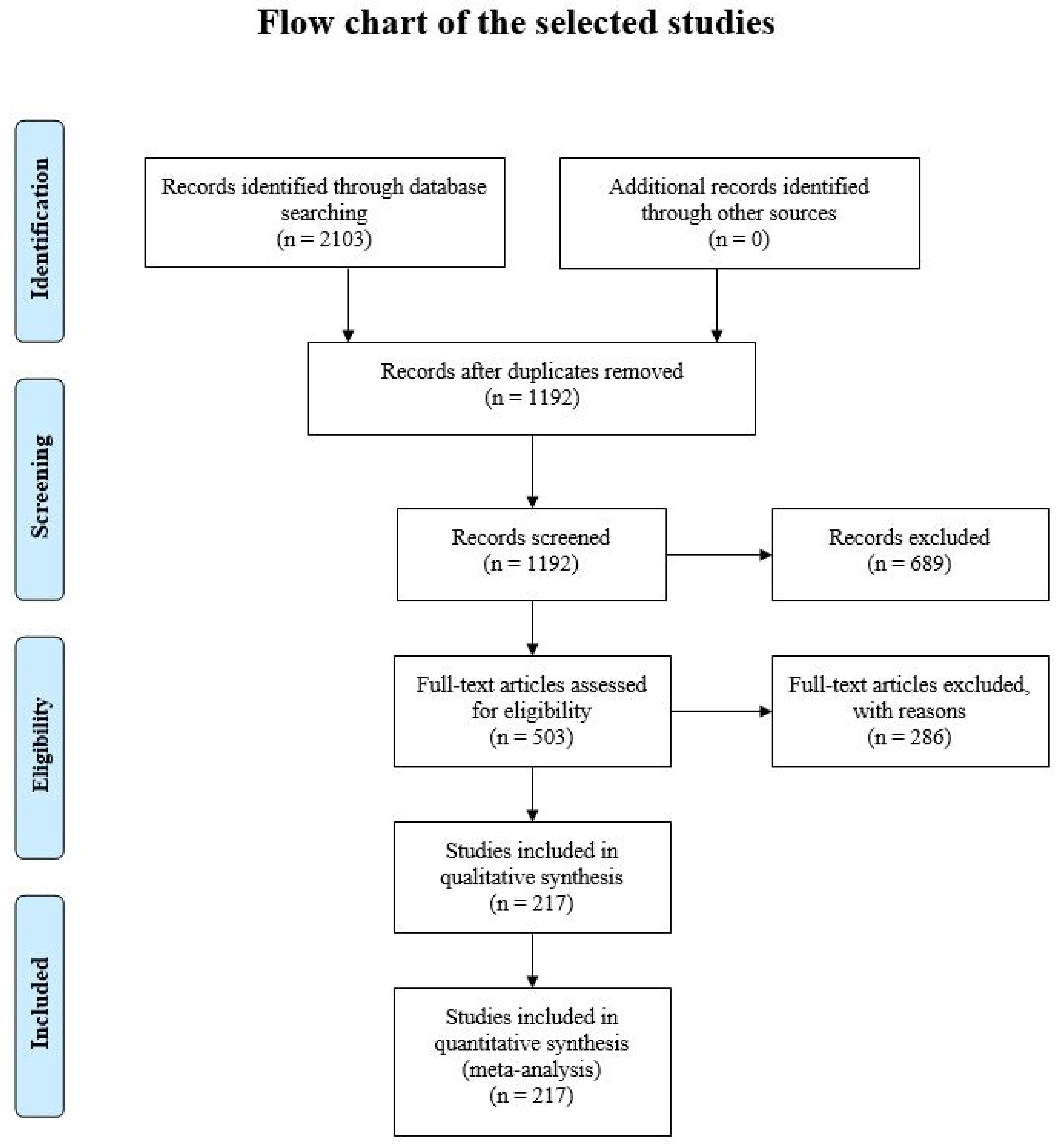
3.1. Study Selection
3.2. Circadian Rhythm and Sleep–Wake Alterations
3.2.1. Circadian Rhythm Assessment
3.2.2. Circadian Rhythm and Sleep–Wake Alterations in Aging
3.2.3. Circadian Rhythm and Sleep–Wake Alterations in Cancer
3.2.4. Circadian Rhythm and Sleep–Wake Alterations in Neurodegenerative Disease
3.2.5. Circadian Rhythm and Sleep–Wake Alterations in Cardiovascular Disease
3.2.6. Circadian Rhythm and Sleep–Wake Alterations in Eating and Metabolic Disorders
3.3. Chronotype, Sleep and Social Jet Lag Aspects
3.3.1. Chronotype Assessment
3.3.2. Chronotype: Influences of Gender and Age
3.3.3. Chronotype and Sleep
3.3.4. Chronotype and Social Jet Lag
3.3.5. Relationship between Chronotype and Melatonin
3.3.6. Chronotype and Chemotherapy Effects
4. Discussion and Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between Clocks: Daily Temporal Patterns of Human Chronotypes. J. Biol. Rhythms 2003, 18, 80–90. [Google Scholar] [CrossRef] [Green Version]
- Bonaconsa, M.; Malpeli, G.; Montaruli, A.; Carandente, F.; Grassi-Zucconi, G.; Bentivoglio, M. Differential Modulation of Clock Gene Expression in the Suprachiasmatic Nucleus, Liver and Heart of Aged Mice. Exp. Gerontol. 2014, 55, 70–79. [Google Scholar] [CrossRef]
- Hastings, M.H.; Reddy, A.B.; Maywood, E.S. A Clockwork Web: Circadian Timing in Brain and Periphery, in Health and Disease. Nat. Rev. Neurosci. 2003, 4, 649–661. [Google Scholar] [CrossRef]
- Nováková, M.; Sládek, M.; Sumová, A. Human Chronotype Is Determined in Bodily Cells Under Real-Life Conditions. Chronobiol. Int. 2013, 30, 607–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roveda, E.; Montaruli, A.; Galasso, L.; Pesenti, C.; Bruno, E.; Pasanisi, P.; Cortellini, M.; Rampichini, S.; Erzegovesi, S.; Caumo, A.; et al. Rest–activity Circadian Rhythm and Sleep Quality in Patients with Binge Eating Disorder. Chronobiol. Int. 2018, 35, 198–207. [Google Scholar] [CrossRef]
- Roveda, E.; Bruno, E.; Galasso, L.; Mulè, A.; Castelli, L.; Villarini, A.; Caumo, A.; Esposito, F.; Montaruli, A.; Pasanisi, P. Rest–activity Circadian Rhythm in Breast Cancer Survivors at 5 Years after the Primary Diagnosis. Chronobiol. Int. 2019, 36, 1156–1165. [Google Scholar] [CrossRef]
- Galasso, L.; Montaruli, A.; Mulè, A.; Castelli, L.; Bruno, E.; Caumo, A.; Esposito, F.; Roveda, E. The Multidisciplinary Therapy in Binge Eating Disorder Is Able to Influence the Interdaily Stability and Sleep Quality? Chronobiol. Int. 2019, 36, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Tevy, M.F.; Giebultowicz, J.; Pincus, Z.; Mazzoccoli, G.; Vinciguerra, M. Aging Signaling Pathways and Circadian Clock-Dependent Metabolic Derangements. Trends Endocrinol. Metab. 2013, 24, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Mormont, M.-C.; Waterhouse, J. Contribution of the Rest–Activity Circadian Rhythm to Quality of Life in Cancer Patients. Chronobiol. Int. 2002, 19, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Tranah, G.J.; Blackwell, T.; Stone, K.L.; Ancoli-Israel, S.; Paudel, M.L.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Hillier, T.A.; Cummings, S.R.; et al. Circadian Activity Rhythms and Risk of Incident Dementia and Mild Cognitive Impairment in Older Women. Ann. Neurol. 2011, 70, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Tranah, G.J.; Blackwell, T.; Ancoli-Israel, S.; Paudel, M.L.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Hillier, T.A.; Cummings, S.R.; Stone, K.L.; et al. Circadian Activity Rhythms and Mortality: The Study of Osteoporotic Fractures. J. Am. Geriatr. Soc. 2010, 58, 282–291. [Google Scholar] [CrossRef]
- Paudel, M.L.; Taylor, B.C.; Ancoli-Israel, S.; Blackwell, T.; Stone, K.L.; Tranah, G.; Redline, S.; Cummings, S.R.; Ensrud, K.E. Osteoporotic Fractures in Men (MrOS) Study. Rest/Activity Rhythms and Mortality in Older Man: MROS Sleep Study. Chronobiol. Int. 2010, 27, 363–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zerón-Rugerio, M.F.; Díez-Noguera, A.; Izquierdo-Pulido, M.; Cambras, T. Higher Eating Frequency Is Associated with Lower Adiposity and Robust Circadian Rhythms: A Cross-Sectional Study. Am. J. Clin. Nutr. 2021, 113, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Sack, R.L.; Auckley, D.; Auger, R.R.; Carskadon, M.A.; Wright, K.P.; Vitiello, M.V.; Zhdanova, I.V.. Circadian Rhythm Sleep Disorders: Part I, Basic Principles, Shift Work and Jet Lag Disorders. Sleep 2007, 30, 1460–1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sack, R.L.; Auckley, D.; Auger, R.R.; Carskadon, M.A.; Wright, K.P.; Vitiello, M.V.; Zhdanova, I.V.; American Academy of Sleep Medicine. Circadian Rhythm Sleep Disorders: Part II, Advanced Sleep Phase Disorder, Delayed Sleep Phase Disorder, Free-Running Disorder, and Irregular Sleep–wake Rhythm. An American Academy of Sleep Medicine Review. Sleep 2007, 30, 1484–1501. [Google Scholar] [CrossRef] [Green Version]
- Adan, A.; Archer, S.N.; Hidalgo, M.P.; Di Milia, L.; Natale, V.; Randler, C. Circadian Typology: A Comprehensive Review. Chronobiol. Int. 2012, 29, 1153–1175. [Google Scholar] [CrossRef] [Green Version]
- Montaruli, A.; Galasso, L.; Caumo, A.; Cè, E.; Pesenti, C.; Roveda, E.; Esposito, F. The Circadian Typology: The Role of Physical Activity and Melatonin. Sport Sci. Health 2017, 13, 469–476. [Google Scholar] [CrossRef]
- Mongrain, V.; Lavoie, S.; Selmaoui, B.; Paquet, J.; Dumont, M. Phase Relationships between Sleep–wake Cycle and Underlying Circadian Rhythms in Morningness–Eveningness. J. Biol. Rhythms 2004, 19, 248–257. [Google Scholar] [CrossRef]
- Taillard, J.; Philip, P.; Chastang, J.-F.; Bioulac, B. Validation of Horne and Ostberg Morningness–Eveningness Questionnaire in a Middle-Aged Population of French Workers. J. Biol. Rhythms 2004, 19, 76–86. [Google Scholar] [CrossRef]
- Zajenkowski, M.; Jankowski, K.S.; Stolarski, M. Why Do Evening People Consider Themselves More Intelligent than Morning Individuals? The Role of Big Five, Narcissism, and Objective Cognitive Ability. Chronobiol. Int. 2019, 36, 1741–1751. [Google Scholar] [CrossRef]
- Makarem, N.; Paul, J.; Giardina, E.-G.V.; Liao, M.; Aggarwal, B. Evening Chronotype Is Associated with Poor Cardiovascular Health and Adverse Health Behaviors in a Diverse Population of Women. Chronobiol. Int. 2020, 37, 673–685. [Google Scholar] [CrossRef]
- Lim, S.-T.; Kim, D.-Y.; Kwon, H.-T.; Lee, E. Sleep Quality and Athletic Performance According to Chronotype. BMC Sports Sci. Med. Rehabil. 2021, 13, 2. [Google Scholar] [CrossRef]
- Hill, D.W.; Chtourou, H. The Effect of Time of Day and Chronotype on the Relationships between Mood State and Performance in a Wingate Test. Chronobiol. Int. 2020, 37, 1599–1610. [Google Scholar] [CrossRef]
- Mulè, A.; Galasso, L.; Castelli, L.; Condemi, V.; Bisconti, A.V.A.V.; Esposito, F.; Roveda, E.; Montaruli, A. Effect of Chronotype on Rating of Perceived Exertion in Active Young People. Sport Sci. Health 2020, 16, 331–336. [Google Scholar] [CrossRef]
- Roveda, E.; Mulè, A.; Galasso, L.; Castelli, L.; Scurati, R.; Michielon, G.; Esposito, F.; Caumo, A.; Montaruli, A. Effect of Chronotype on Motor Skills Specific to Soccer in Adolescent Players. Chronobiol. Int. 2020, 37, 552–563. [Google Scholar] [CrossRef]
- Montaruli, A.; Castelli, L.; Galasso, L.; Mulè, A.; Bruno, E.; Esposito, F.; Caumo, A.; Roveda, E. Effect of Chronotype on Academic Achievement in a Sample of Italian University Students. Chronobiol. Int. 2019, 36, 1482–1495. [Google Scholar] [CrossRef]
- Li, T.; Xie, Y.; Tao, S.; Yang, Y.; Xu, H.; Zou, L.; Tao, F.; Wu, X. Chronotype, Sleep, and Depressive Symptoms Among Chinese College Students: A Cross-Sectional Study. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef]
- Belfry, K.D.; Deibel, S.H.; Kolla, N.J. Time of Day Matters: An Exploratory Assessment of Chronotype in a Forensic Psychiatric Hospital. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Hashemipour, S.; Yazdi, Z.; Mahabad, N. Association of Evening Chronotype with Poor Control of Type 2 Diabetes: Roles of Sleep Duration and Insomnia Level. Int. J. Endocrinol. Metab. 2020, 18. [Google Scholar] [CrossRef] [PubMed]
- Schulte, P.F.J.; Riemersma-van der Lek, R.F. Evening Chronotype, Disordered Eating Behavior, Bipolar Disorder, and Light Therapy. Acta Psychiatr. Scand. 2021, 143, 181–182. [Google Scholar] [CrossRef]
- Bauducco, S.; Richardson, C.; Gradisar, M. Chronotype, Circadian Rhythms and Mood. Curr. Opin. Psychol. 2019, 34, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.J.; Hasler, B.P. Chronotype and Mental Health: Recent Advances. Curr. Psychiatry Rep. 2018, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Kivelä, L.; Papadopoulos, M.R.; Antypa, N. Chronotype and Psychiatric Disorders. Curr. Sleep Med. Reports 2018, 4, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Halberg, F.; Johnson, E.; Nelson, W.; Runge, W.; Sothern, R. Autorhythmometry-Procedures for Physiologic Self-Measurement and Their Analysis. Physiol. Teach. 1972, 1, 1–11. [Google Scholar]
- Halberg, F.; Reinberg, A. Circadian Rhythm and Low Frequency Rhythms in Human Physiology. J. Physiol. 1967, 59 (Suppl. 1), 117–200. [Google Scholar]
- De Prins, J.; Cornelissen, G.; Halberg, F. Harmonic Interpolation on Equispaced Series Covering Integral Period of Anticipated Circadian Rhythm in Adriamycin Tolerance. Chronobiologia 1977, 4, 173. [Google Scholar]
- Koukkari, W.L.; Halberg, F.; Gordon, S.A. Quantifying Rhythmic Movements of Albizzia Julibrissin Pinnules. Plant Physiol. 1973, 51, 1084–1088. [Google Scholar] [CrossRef] [Green Version]
- Koukkari, W.L.; Duke, S.H.; Halberg, F.; Lee, J.K. Circadian Rhythmic Leaflet Movements: Student Exercise in Chronobiology. Chronobiologia 1974, 1, 281–302. [Google Scholar]
- Bartter, F.C.; Delea, C.S.; Baker, W.; Halberg, F.; Lee, J.K. Chronobiology in the Diagnosis and Treatment of Mesor Hypertension. Chronobiologia 1976, 3, 199–213. [Google Scholar]
- Ancoli-Israel, S.; Cole, R.; Alessi, C.; Chambers, M.; Moorcroft, W.; Pollak, C.P. The Role of Actigraphy in the Study of Sleep and Circadian Rhythms. Sleep 2003, 26, 342–392. [Google Scholar] [CrossRef] [Green Version]
- Calogiuri, G.; Beldo, S.; Roveda, E.; Montaruli, A.; Carandente, F.; Weydahl, A. Training Time and Adaptation to Lack of Daylight: A Case Report. Sport Sci. Health 2009, 5, 37–41. [Google Scholar] [CrossRef]
- Calogiuri, G.; Weydahl, A.; Roveda, E. Effects of Sleep Loss and Strenuous Physical Activity on the Rest–Activity Circadian Rhythm. Biol. Res. Nurs. 2011, 13, 409–418. [Google Scholar] [CrossRef]
- Roveda, E.; Sciolla, C.; Montaruli, A.; Calogiuri, G.; Angeli, A.; Carandente, F. Effects of Endurance and Strength Acute Exercise on Night Sleep Quality. Int. Sport. J. 2011, 12, 113–124. [Google Scholar]
- Montaruli, A.; Patrini, P.; Roveda, E.; Carandente, F. Physical Activity and Breast Cancer. Sport Sci. Health 2012, 8, 1–13. [Google Scholar] [CrossRef]
- Halberg, F.; Carandente, F.; Cornelissen, G.; Katinas, G.S. Glossary of Chronobiology (Author’s Transl). Chronobiologia 1977, 4 (Suppl. 1), 1–189. [Google Scholar]
- Nelson, W.; Tong, Y.L.; Lee, J.K.; Halberg, F. Methods for Cosinor-Rhythmometry. Chronobiologia 1979, 6, 305–323. [Google Scholar]
- Huang, Q.; Cohen, D.; Komarzynski, S.; Li, X.-M.; Innominato, P.; Lévi, F.; Finkenstädt, B. Hidden Markov Models for Monitoring Circadian Rhythmicity in Telemetric Activity Data. J. R. Soc. Interface 2018, 15, 20170885. [Google Scholar] [CrossRef]
- Minors, D.; Akerstedt, T.; Atkinson, G.; Dahlitz, M.; Folkard, S.; Levi, F.; Mormont, C.; Parkes, D.; Waterhouse, J. The Difference between Activity When in Bed and out of Bed. I. Healthy Subjects and Selected Patients. Chronobiol. Int. 1996, 13, 27–34. [Google Scholar] [CrossRef]
- Marler, M.R.; Gehrman, P.; Martin, J.L.; Ancoli-Israel, S. The Sigmoidally Transformed Cosine Curve: A Mathematical Model for Circadian Rhythms with Symmetric Non-Sinusoidal Shapes. Stat. Med. 2006, 25, 3893–3904. [Google Scholar] [CrossRef]
- Huang, Y.-L.; Liu, R.-Y.; Wang, Q.-S.; Van Someren, E.J.W.; Xu, H.; Zhou, J.-N. Age-Associated Difference in Circadian Sleep–Wake and Rest–Activity Rhythms. Physiol. Behav. 2002, 76, 597–603. [Google Scholar] [CrossRef]
- Cornelissen, G.; Otsuka, K. Chronobiology of Aging: A Mini-Review. Gerontology 2017, 63, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Halberg, F.; Lubanovic, W.A.; Sothern, R.B.; Brockway, B.; Powell, E.W.; Pasley, J.N.; Scheving, L.E. Nomifensine Chronopharmacology, Schedule-Shifts and Circadian Temperature Rhythms in Di-Suprachiasmatically Lesioned Rats--Modeling Emotional Chronopathology and Chronotherapy. Chronobiologia 1979, 6, 405–424. [Google Scholar] [PubMed]
- Carskadon, M.A.; Dement, W.C. Sleep Loss in Elderly Volunteers. Sleep 1985, 8, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Monk, T.H.; Reynolds, C.F.; Buysse, D.J.; Hoch, C.C.; Jarrett, D.B.; Jennings, J.R.; Kupfer, D.J. Circadian Characteristics of Healthy 80-Year-Olds and Their Relationship to Objectively Recorded Sleep. J. Gerontol. 1991, 46, M171–M175. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.J.; Kerkhof, G.A.; Hofman, W.F. Age Differences in Sleep–Wake Behavior under Natural Conditions. Pers. Individ. Dif. 1999, 27, 853–860. [Google Scholar] [CrossRef]
- Renfrew, J.W.; Pettigrew, K.D.; Rapoport, S.I. Motor Activity and Sleep Duration as a Function of Age in Healthy Men. Physiol. Behav. 1987, 41, 627–634. [Google Scholar] [CrossRef]
- Dallosso, H.M.; Morgan, K.; Bassey, E.J.; Ebrahim, S.B.J.; Fentem, P.H.; Arie, T.H. Levels of Customary Physical Activity among the Old and the Very Old Living at Home. J. Epidemiol. Community Health 1988, 42, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Elia, M.; Ritz, P.; Stubbs, R. Total Energy Expenditure in the Elderly. Eur. J. Clin. Nutr. 2000, 54, S92–S103. [Google Scholar] [CrossRef]
- Padmashree, R.; Mishal, I.S.; Ritu, A. Time Will Tell: Circadian Clock Dysregulation in Triple Negative Breast Cancer. Front. Biosci. 2019, 11, 178–192. [Google Scholar] [CrossRef]
- Galasso, L.; Montaruli, A.; Mulè, A.; Castelli, L.; Bruno, E.; Pasanisi, P.; Caumo, A.; Esposito, F.; Roveda, E. Rest–activity Rhythm in Breast Cancer Survivors: An Update Based on Non-Parametric Indices. Chronobiol. Int. 2020, 1–6. [Google Scholar] [CrossRef]
- Sephton, S.E. Diurnal Cortisol Rhythm as a Predictor of Breast Cancer Survival. J. Natl. Cancer Inst. 2000, 92, 994–1000. [Google Scholar] [CrossRef]
- Lévi, F.; Dugué, P.-A.; Innominato, P.; Karaboué, A.; Dispersyn, G.; Parganiha, A.; Giacchetti, S.; Moreau, T.; Focan, C.; Waterhouse, J.; et al. Wrist Actimetry Circadian Rhythm as a Robust Predictor of Colorectal Cancer Patients Survival. Chronobiol. Int. 2014, 31, 891–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sephton, S.E.; Lush, E.; Dedert, E.A.; Floyd, A.R.; Rebholz, W.N.; Dhabhar, F.S.; Spiegel, D.; Salmon, P. Diurnal Cortisol Rhythm as a Predictor of Lung Cancer Survival. Brain. Behav. Immun. 2013, 30, S163–S170. [Google Scholar] [CrossRef]
- Cohen, L.; Cole, S.W.; Sood, A.K.; Prinsloo, S.; Kirschbaum, C.; Arevalo, J.M.G.; Jennings, N.B.; Scott, S.; Vence, L.; Wei, Q.; et al. Depressive Symptoms and Cortisol Rhythmicity Predict Survival in Patients with Renal Cell Carcinoma: Role of Inflammatory Signaling. PLoS ONE 2012, 7, e42324. [Google Scholar] [CrossRef]
- Mormont, M.C.; Lévi, F. Circadian-System Alterations during Cancer Processes: A Review. Int. J. Cancer 1997, 70, 241–247. [Google Scholar] [CrossRef]
- Antoni, M.H.; Lutgendorf, S.K.; Cole, S.W.; Dhabhar, F.S.; Sephton, S.E.; McDonald, P.G.; Stefanek, M.; Sood, A.K. The Influence of Bio-Behavioural Factors on Tumour Biology: Pathways and Mechanisms. Nat. Rev. Cancer 2006, 6, 240–248. [Google Scholar] [CrossRef]
- Sephton, S.; Spiegel, D. Circadian Disruption in Cancer: A Neuroendocrine-Immune Pathway from Stress to Disease? Brain. Behav. Immun. 2003, 17, 321–328. [Google Scholar] [CrossRef]
- Eismann, E.A.; Lush, E.; Sephton, S.E. Circadian Effects in Cancer-Relevant Psychoneuroendocrine and Immune Pathways. Psychoneuroendocrinology 2010, 35, 963–976. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Liu, L.; Marler, M.R.; Parker, B.A.; Jones, V.; Sadler, G.R.; Dimsdale, J.; Cohen-Zion, M.; Fiorentino, L. Fatigue, Sleep, and Circadian Rhythms Prior to Chemotherapy for Breast Cancer. Support. Care Cancer 2006, 14, 201–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roscoe, J.A.; Morrow, G.R.; Hickok, J.T.; Bushunow, P.; Matteson, S.; Rakita, D.; Andrews, P.L.R. Temporal Interrelationships among Fatigue, Circadian Rhythm and Depression in Breast Cancer Patients Undergoing Chemotherapy Treatment. Support. Care Cancer 2002, 10, 329–336. [Google Scholar] [CrossRef]
- Savard, J.; Laroche, L.; Simard, S.; Ivers, H.; Morin, C.M. Chronic Insomnia and Immune Functioning. Psychosom. Med. 2003, 65, 211–221. [Google Scholar] [CrossRef]
- Fu, L.; Lee, C.C. The Circadian Clock: Pacemaker and Tumour Suppressor. Nat. Rev. Cancer 2003, 3, 350–361. [Google Scholar] [CrossRef]
- Tamakoshi, A.; Ohno, Y. Self-Reported Sleep Duration as a Predictor of All-Cause Mortality: Results from the JACC Study, Japan. Sleep 2004, 27, 51–54. [Google Scholar] [CrossRef] [Green Version]
- Hublin, C.; Partinen, M.; Koskenvuo, M.; Kaprio, J. Sleep and Mortality: A Population-Based 22-Year Follow-up Study. Sleep 2007, 30, 1245–1253. [Google Scholar] [CrossRef] [Green Version]
- Vijayalaxmi; Thomas, C.R.; Reiter, R.J.; Herman, T.S. Melatonin: From Basic Research to Cancer Treatment Clinics. J. Clin. Oncol. 2002, 20, 2575–2601. [Google Scholar] [CrossRef]
- Meier-Ewert, H.K.; Ridker, P.M.; Rifai, N.; Regan, M.M.; Price, N.J.; Dinges, D.F.; Mullington, J.M. Effect of Sleep Loss on C-Reactive Protein, an Inflammatory Marker of Cardiovascular Risk. J. Am. Coll. Cardiol. 2004, 43, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Vgontzas, A.N.; Zoumakis, E.; Bixler, E.O.; Lin, H.M.; Follett, H.; Kales, A.; Chrousos, G.P. Adverse Effects of Modest Sleep Restriction on Sleepiness, Performance, and Inflammatory Cytokines. J. Clin. Endocrinol. Metab. 2004, 89, 2119–2126. [Google Scholar] [CrossRef] [Green Version]
- Megdal, S.P.; Kroenke, C.H.; Laden, F.; Pukkala, E.; Schernhammer, E.S. Night Work and Breast Cancer Risk: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2005, 41, 2023–2032. [Google Scholar] [CrossRef]
- Dimitrov, S.; Lange, T.; Nohroudi, K.; Born, J. Number and Function of Circulating Human Antigen Presenting Cells Regulated by Sleep. Sleep 2007, 30, 401–411. [Google Scholar] [CrossRef] [Green Version]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of Sleep Debt on Metabolic and Endocrine Function. Lancet 1999, 354, 1435–1439. [Google Scholar] [CrossRef]
- Costa, A.R.; Fontes, F.; Pereira, S.; Gonçalves, M.; Azevedo, A.; Lunet, N. Impact of Breast Cancer Treatments on Sleep Disturbances—A Systematic Review. Breast 2014, 23, 697–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savard, J.; Davidson, J.R.; Ivers, H.; Quesnel, C.; Rioux, D.; Dupéré, V.; Lasnier, M.; Simard, S.; Morin, C.M. The Association between Nocturnal Hot Flashes and Sleep in Breast Cancer Survivors. J. Pain Symptom Manag. 2004, 27, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Gehrman, P.; Marler, M.; Martin, J.L.; Shochat, T.; Corey-Bloom, J.; Ancoli-Israel, S. The Timing of Activity Rhythms in Patients With Dementia Is Related to Survival. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M1050–M1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satlin, A.; Volicer, L.; Stopa, E.G.; Harper, D. Circadian Locomotor Activity and Core-Body Temperature Rhythms in Alzheimer’s Disease. Neurobiol. Aging 1995, 16, 765–771. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Klauber, M.R.; Jones, D.W.; Kripke, D.F.; Martin, J.; Mason, W.; Pat-Horenczyk, R.; Fell, R. Variations in Circadian Rhythms of Activity, Sleep, and Light Exposure Related to Dementia in Nursing-Home Patients. Sleep 1997, 20, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Gehrman, P.; Marler, M.; Martin, J.L.; Shochat, T.; Corey-Bloom, J.; Ancoli-Israel, S. The Relationship between Dementia Severity and Rest/Activity Circadian Rhythms. Neuropsychiatr. Dis. Treat. 2005, 1, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Someren, E.J.W.; Hagebeuk, E.E.O.; Lijzenga, C.; Scheltens, P.; de Rooij, S.E.J.A.; Jonker, C.; Pot, A.-M.; Mirmiran, M.; Swaab, D.F. Circadian Rest—Activity Rhythm Disturbances in Alzheimer’s Disease. Biol. Psychiatry 1996, 40, 259–270. [Google Scholar] [CrossRef] [Green Version]
- Benca, R.; Duncan, M.J.; Frank, E.; McClung, C.; Nelson, R.J.; Vicentic, A. Biological Rhythms, Higher Brain Function, and Behavior: Gaps, Opportunities, and Challenges. Brain Res. Rev. 2009, 62, 57–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harmar, A.J.; Marston, H.M.; Shen, S.; Spratt, C.; West, K.M.; Sheward, W.J.; Morrison, C.F.; Dorin, J.R.; Piggins, H.D.; Reubi, J.-C.; et al. The VPAC2 Receptor Is Essential for Circadian Function in the Mouse Suprachiasmatic Nuclei. Cell 2002, 109, 497–508. [Google Scholar] [CrossRef]
- Hastings, M.H.; Maywood, E.S.; Reddy, A.B. Two Decades of Circadian Time. J. Neuroendocrinol. 2008, 20, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Kyriacou, C.P.; Hastings, M.H. Circadian Clocks: Genes, Sleep, and Cognition. Trends Cogn. Sci. 2010, 14, 259–267. [Google Scholar] [CrossRef]
- Foley, D.J.; Monjan, A.A.; Brown, S.L.; Simonsick, E.M.; Wallace, R.B.; Blazer, D.G. Sleep Complaints Among Elderly Persons: An Epidemiologic Study of Three Communities. Sleep 1995, 18, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Espiritu, J.R.D. Aging-Related Sleep Changes. Clin. Geriatr. Med. 2008, 24, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chokroverty, S. Sleep Disorders Medicine, 3rd ed.; Chokroverty, S., Ed.; Springer New York: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Vitiello, M.V.; Prinz, P.N. Alzheimer’s Disease: Sleep and Sleep/Wake Patterns. Clin. Geriatr. Med. 1989, 5, 289–299. [Google Scholar] [CrossRef]
- Beaulieu-Bonneau, S.; Hudon, C. Sleep Disturbances in Older Adults with Mild Cognitive Impairment. Int. Psychogeriatr. 2009, 21, 654–666. [Google Scholar] [CrossRef] [PubMed]
- Moe, K.E.; Vitiello, M.V.; Larsen, L.H.; Prinz, P.N. Symposium: Cognitive Processes and Sleep Disturbances: Sleep/Wake Patterns in Alzheimer’s Disease: Relationships with Cognition and Function. J. Sleep Res. 1995, 4, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.S.P.; Yu, L.; Kowgier, M.; Schneider, J.A.; Buchman, A.S.; Bennett, D.A. Modification of the Relationship of the Apolipoprotein E Ε4 Allele to the Risk of Alzheimer Disease and Neurofibrillary Tangle Density by Sleep. JAMA Neurol. 2013, 70, 1544–1551. [Google Scholar] [CrossRef] [Green Version]
- Landry, G.J.; Liu-Ambrose, T. Buying Time: A Rationale for Examining the Use of Circadian Rhythm and Sleep Interventions to Delay Progression of Mild Cognitive Impairment to Alzheimer’s Disease. Front. Aging Neurosci. 2014, 6, 1–21. [Google Scholar] [CrossRef]
- Paudel, M.L.; Taylor, B.C.; Ancoli-Israel, S.; Stone, K.L.; Tranah, G.; Redline, S.; Barrett-Connor, E.; Stefanick, M.L.; Ensrud, K.E. Rest/Activity Rhythms and Cardiovascular Disease in Older Men. Chronobiol. Int. 2011, 28, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Muller, J.E.; Tofler, G.H.; Stone, P.H. Circadian Variation and Triggers of Onset of Acute Cardiovascular Disease. Circulation 1989, 79, 733–743. [Google Scholar] [CrossRef] [Green Version]
- King, C.R.; Knutson, K.L.; Rathouz, P.J.; Sidney, S.; Liu, K.; Lauderdale, D.S. Short Sleep Duration and Incident Coronary Artery Calcification. JAMA 2008, 300, 2859–2866. [Google Scholar] [CrossRef] [Green Version]
- Chandola, T.; Ferrie, J.E.; Perski, A.; Akbaraly, T.; Marmot, M.G. The Effect of Short Sleep Duration on Coronary Heart Disease Risk Is Greatest Among Those with Sleep Disturbance: A Prospective Study from the Whitehall II Cohort. Sleep 2010, 33, 739–744. [Google Scholar] [CrossRef] [Green Version]
- Cappuccio, F.P.; Cooper, D.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep Duration Predicts Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Studies. Eur. Heart J. 2011, 32, 1484–1492. [Google Scholar] [CrossRef] [Green Version]
- Yaggi, H.K.; Araujo, A.B.; McKinlay, J.B. Sleep Duration as a Risk Factor for the Development of Type 2 Diabetes. Diabetes Care 2006, 29, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep Duration and All-Cause Mortality: A Systematic Review and Meta-Analysis of Prospective Studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef]
- Holliday, E.G.; Magee, C.A.; Kritharides, L.; Banks, E.; Attia, J. Short Sleep Duration Is Associated with Risk of Future Diabetes but Not Cardiovascular Disease: A Prospective Study and Meta-Analysis. PLoS ONE 2013, 8, e82305. [Google Scholar] [CrossRef]
- Jackson, C.L.; Redline, S.; Kawachi, I.; Hu, F.B. Association between Sleep Duration and Diabetes in Black and White Adults. Diabetes Care 2013, 36, 3557–3565. [Google Scholar] [CrossRef] [Green Version]
- Wolff, B.; Völzke, H.; Schwahn, C.; Robinson, D.; Kessler, C.; John, U. Relation of Self-Reported Sleep Duration with Carotid Intima-Media Thickness in a General Population Sample. Atherosclerosis 2008, 196, 727–732. [Google Scholar] [CrossRef]
- Grandner, M.A.; Hale, L.; Moore, M.; Patel, N.P. Mortality Associated with Short Sleep Duration: The Evidence, the Possible Mechanisms, and the Future. Sleep Med. Rev. 2010, 14, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Cesari, F.; Casini, A.; Macchi, C.; Abbate, R.; Gensini, G.F. Insomnia and Risk of Cardiovascular Disease: A Meta-Analysis. Eur. J. Prev. Cardiol. 2014, 21, 57–64. [Google Scholar] [CrossRef]
- Spiegel, K.; Tasali, E.; Penev, P.; van Cauter, E. Brief Communication: Sleep Curtailment in Healthy Young Men Is Associated with Decreased Leptin Levels, Elevated Ghrelin Levels, and Increased Hunger and Appetite. Ann. Intern. Med. 2004, 141, 846. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Heymsfield, S.B.; Boden-Albala, B.; Buijs, R.M.; Kreier, F.; Opler, M.G.; Pickering, T.G.; Rundle, A.G.; Zammit, G.K.; Malaspina, D. Sleep Duration Associated with Mortality in Elderly, but Not Middle-Aged, Adults in a Large US Sample. Sleep 2008, 31, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of Poor and Short Sleep on Glucose Metabolism and Obesity Risk. Nat. Rev. Endocrinol. 2009, 5, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, K.; Knutson, K.; Leproult, R.; Tasali, E.; van Cauter, E. Sleep Loss: A Novel Risk Factor for Insulin Resistance and Type 2 Diabetes. J. Appl. Physiol. 2005, 99, 2008–2019. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.A.; Cappuccio, F.P. Inflammation, Sleep, Obesity and Cardiovascular Disease. Curr. Vasc. Pharmacol. 2007, 5, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Taggart, F.M.; Kandala, N.-B.; Currie, A.; Peile, E.; Stranges, S.; Miller, M.A. Meta-Analysis of Short Sleep Duration and Obesity in Children and Adults. Sleep 2008, 31, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.R.; Blackwell, T.; Redline, S.; Ancoli-Israel, S.; Cauley, J.A.; Hillier, T.A.; Lewis, C.E.; Orwoll, E.S.; Stefanick, M.L.; Taylor, B.C.; et al. The Association between Sleep Duration and Obesity in Older Adults. Int. J. Obes. 2008, 32, 1825–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.R.; Hayes, A.L.; Blackwell, T.; Evans, D.S.; Ancoli-Israel, S.; Wing, Y.K.; Stone, K.L.; Osteoporotic Fractures in Men (MrOS); Study of Osteoporotic Fractures (SOF) Research Groups. The Association between Sleep Patterns and Obesity in Older Adults. Int. J. Obes. 2014, 38, 1159–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, K.G.; Reid, K.J.; Kern, A.S.; Zee, P.C. Role of Sleep Timing in Caloric Intake and BMI. Obesity 2011, 19, 1374–1381. [Google Scholar] [CrossRef]
- Coakley, E.; Rimm, E.; Colditz, G.; Kawachi, I.; Willett, W. Predictors of Weight Change in Men: Results from The Health Professionals Follow-Up Study. Int. J. Obes. 1998, 22, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Van Der Heijden, A.A.W.A.; Hu, F.B.; Rimm, E.B.; van Dam, R.M. A Prospective Study of Breakfast Consumption and Weight Gain among U.S. Men. Obesity 2007, 15, 2463–2469. [Google Scholar] [CrossRef] [PubMed]
- Timlin, M.T.; Pereira, M.A.; Story, M.; Neumark-Sztainer, D. Breakfast Eating and Eeight Change in a 5-Year Prospective Analysis of Adolescents: Project EAT (Eating among Teens). Pediatrics 2008, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, J.; Cheung, B.; Ho, S.; Sham, A.; Lam, T.H. Influence of Dietary Pattern on the Development of Overweight in a Chinese Population. Eur. J. Clin. Nutr. 2008, 62, 480–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra-Johnson, J.; Undén, A.L.; Linestrand, M.; Rosell, M.; Sjogren, P.; Kolak, M.; De Faire, U.; Fisher, R.M.; Hellénius, M.L. Eating Meals Irregularly: A Novel Environmental Risk Factor for the Metabolic Syndrome. Obesity 2008, 16, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Vardar, E.; Caliyurt, O.; Arikan, E.; Tuglu, C. Sleep Quality and Psychopathological Features in Obese Binge Eaters. Stress Heal. 2004, 20, 35–41. [Google Scholar] [CrossRef]
- Tzischinsky, O.; Latzer, Y.; Epstein, R.; Tov, N. Sleep–wake Cycles in Women with Binge Eating Disorder. Int. J. Eat. Disord. 2000, 27, 43–48. [Google Scholar] [CrossRef]
- Trace, S.E.; Thornton, L.M.; Runfola, C.D.; Lichtenstein, P.; Pedersen, N.L.; Bulik, C.M. Sleep Problems Are Associated with Binge Eating in Women. Int. J. Eat. Disord. 2012, 45, 695–703. [Google Scholar] [CrossRef] [Green Version]
- Yeh, S.S.S.; Brown, R.F. Disordered Eating Partly Mediates the Relationship between Poor Sleep Quality and High Body Mass Index. Eat. Behav. 2014, 15, 291–297. [Google Scholar] [CrossRef]
- Aspen, V.; Weisman, H.; Vannucci, A.; Nafiz, N.; Gredysa, D.; Kass, A.E.; Trockel, M.; Jacobi, C.; Wilfley, D.E.; Taylor, C.B. Psychiatric Co-Morbidity in Women Presenting across the Continuum of Disordered Eating. Eat. Behav. 2014, 15, 686–693. [Google Scholar] [CrossRef] [Green Version]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short Sleep Duration Is Associated with Reduced Leptin, Elevated Ghrelin, and Increased Body Mass Index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Chaput, J.P.; Després, J.P.; Bouchard, C.; Tremblay, A. Short Sleep Duration Is Associated with Reduced Leptin Levels and Increased Adiposity: Results from the Québec Family Study. Obesity 2007, 15, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Schmid, S.M.; Hallschmid, M.; Jauch-Chara, K.; Born, J.; Schultes, B. A Single Night of Sleep Deprivation Increases Ghrelin Levels and Feelings of Hunger in Normal-Weight Healthy Men. J. Sleep Res. 2008, 17, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Ahima, R.S.; Saper, C.B.; Flier, J.S.; Elmquist, J.K. Leptin Regulation of Neuroendocrine Systems. Front. Neuroendocrinol. 2000, 21, 263–307. [Google Scholar] [CrossRef] [PubMed]
- Chin-Chance, C.; Polonsky, K.S.; Schoeller, D.A. Twenty-Four-Hour Leptin Levels Respond to Cumulative Short-Term Energy Imbalance and Predict Subsequent Intake. J. Clin. Endocrinol. Metab. 2000, 85, 2685–2691. [Google Scholar] [CrossRef] [PubMed]
- Wren, A.M.; Seal, L.J.; Cohen, M.A.; Brynes, A.E.; Frost, G.S.; Murphy, K.G.; Dhillo, W.S.; Ghatei, M.A.; Bloom, S.R. Ghrelin Enhances Appetite and Increases Food Intake in Humans. J. Clin. Endocrinol. Metab. 2001, 86, 5992. [Google Scholar] [CrossRef]
- Horne, J.A.; Ostberg, O. A Self-Assessment Questionnaire to Determine Morningness–Eveningness in Human Circadian Rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Torsvall, L.; Åkerstedt, T. A Diurnal Type Scale. Construction, Consistency and Validation in Shift Work. Scand. J. Work. Environ. Health 1980, 6, 283–290. [Google Scholar] [CrossRef]
- Folkard, S.; Monk, T.H.; Lobuan, M.C. Towards a Predictive Test of Adjustment to Shift Work. Ergonomics 1979, 22, 79–91. [Google Scholar] [CrossRef]
- Randler, C.; Díaz-Morales, J.F.; Rahafar, A.; Vollmer, C. Morningness–Eveningness and Amplitude—Development and Validation of an Improved Composite Scale to Measure Circadian Preference and Stability (MESSi). Chronobiol. Int. 2016, 33, 832–848. [Google Scholar] [CrossRef] [PubMed]
- Roveda, E.; Vitale, J.A.; Bruno, E.; Montaruli, A.; Pasanisi, P.; Villarini, A.; Gargano, G.; Galasso, L.; Berrino, F.; Caumo, A.; et al. Protective Effect of Aerobic Physical Activity on Sleep Behavior in Breast Cancer Survivors. Integr. Cancer Ther. 2017, 16, 21–31. [Google Scholar] [CrossRef]
- Vitale, J.A.; Roveda, E.; Montaruli, A.; Galasso, L.; Weydahl, A.; Caumo, A.; Carandente, F. Chronotype Influences Activity Circadian Rhythm and Sleep: Differences in Sleep Quality between Weekdays and Weekend. Chronobiol. Int. 2015, 32, 405–415. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.J.; Lee, S.Y.; Jang, K.H.; Kim, I.S.; Duffy, J.F. Reliability and Validity of the Korean Version of Morningness–Eveningness Questionnaire in Adults Aged 20–39 Years. Chronobiol. Int. 2014, 31, 479–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, S.L.; Heitkemper, M.M. Circadian Rhythmicity of Cortisol and Body Temperature: Morningness–Eveningness Effects. Chronobiol. Int. 2001, 18, 249–261. [Google Scholar] [CrossRef] [PubMed]
- Baehr, E.K.; Revelle, W.; Eastman, C.I. Individual Differences in the Phase and Amplitude of the Human Circadian Temperature Rhythm: With an Emphasis on Morningness–Eveningness. J. Sleep Res. 2000, 9, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Roveda, E.; Vitale, J.A.; Montaruli, A.; Galasso, L.; Carandente, F.; Caumo, A. Predicting the Actigraphy-Based Acrophase Using the Morningness–Eveningness Questionnaire (MEQ) in College Students of North Italy. Chronobiol. Int. 2017, 34, 551–562. [Google Scholar] [CrossRef] [PubMed]
- Montaruli, A.; Galasso, L.; Carandente, F.; Vitale, J.A.; Roveda, E.; Caumo, A. If the Morning-Evening Questionnaire (MEQ) Is Able to Predict the Actigraphy-Based Acrophase, How Does Its Reduced, Five-Item Version (RMEQ) Perform? Chronobiol. Int. 2017, 34, 443–444. [Google Scholar] [CrossRef] [PubMed]
- Adan, A.; Natale, V. Gender Differences in Morningness–Eveningness Preference. Chronobiol. Int. 2002, 19, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Castelli, L.; Galasso, L.; Mulè, A.; Bruno, E.; Shokohyar, S.; Esposito, F.; Montaruli, A.; Roveda, E. Physical Activity, Chronotype and Sleep in a Sample of Italian Elderly Population. Sport Sci. Health 2020, 16, 55–64. [Google Scholar] [CrossRef]
- Kim, K.M.; Han, S.M.; Heo, K.; Kim, W.-J.; Chu, M.K. Sex Differences in the Association between Chronotype and Risk of Depression. Sci. Rep. 2020, 10, 18512. [Google Scholar] [CrossRef] [PubMed]
- Didikoglu, A.; Maharani, A.; Payton, A.; Pendleton, N.; Canal, M.M. Longitudinal Change of Sleep Timing: Association between Chronotype and Longevity in Older Adults. Chronobiol. Int. 2019, 36, 1285–1300. [Google Scholar] [CrossRef]
- Randler, C.; Engelke, J. Gender Differences in Chronotype Diminish with Age: A Meta-Analysis Based on Morningness/Chronotype Questionnaires. Chronobiol. Int. 2019, 36, 888–905. [Google Scholar] [CrossRef] [PubMed]
- Borisenkov, M.F.; Perminova, E.V.; Kosova, A.L. Chronotype, Sleep Length, and School Achievement of 11- to 23-Year-Old Students in Northern European Russia. Chronobiol. Int. 2010, 27, 1259–1270. [Google Scholar] [CrossRef] [PubMed]
- Borisenkov, M.F.; Kosova, A.L.; Kasyanova, O.N. Impact of Perinatal Photoperiod on the Chronotype of 11- to 18-Year-Olds in Northern European Russia. Chronobiol. Int. 2012, 29, 305–310. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Vieira, C.; Acebo, C. Association between Puberty and Delayed Phase Preference. Sleep 1993, 16, 258–262. [Google Scholar] [CrossRef] [Green Version]
- Roenneberg, T.; Kuehnle, T.; Pramstaller, P.P.; Ricken, J.; Havel, M.; Guth, A.; Merrow, M. A Marker for the End of Adolescence. Curr. Biol. 2004, 14, R1038–R1039. [Google Scholar] [CrossRef] [Green Version]
- Werner, H.; LeBourgeois, M.K.; Geiger, A.; Jenni, O.G. Assessment of Chronotype in Four- to Eleven-Year-Old Children: Reliability and Validity of the Children’s ChronoType Questionnaire (CCTQ). Chronobiol. Int. 2009, 26, 992–1014. [Google Scholar] [CrossRef] [Green Version]
- Giannotti, F.; Cortesi, F.; Sebastiani, T.; Vagoni, C. Sleeping Habits in Italian Children and Adolescents. Sleep Biol. Rhythms 2005, 3, 15–21. [Google Scholar] [CrossRef]
- Vitale, J.A.; Bonato, M.; Galasso, L.; La Torre, A.; Merati, G.; Montaruli, A.; Roveda, E.; Carandente, F. Sleep Quality and High Intensity Interval Training at Two Different Times of Day: A Crossover Study on the Influence of the Chronotype in Male Collegiate Soccer Players. Chronobiol. Int. 2017, 34, 260–268. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barclay, N.L.; Eley, T.C.; Buysse, D.J.; Archer, S.N.; Gregory, A.M. Diurnal Preference and Sleep Quality: Same Genes? A Study of Young Adult Twins. Chronobiol. Int. 2010, 27, 278–296. [Google Scholar] [CrossRef] [Green Version]
- Eid, B.; Bou Saleh, M.; Melki, I.; Torbey, P.-H.; Najem, J.; Saber, M.; El Osta, N.; Rabbaa Khabbaz, L. Evaluation of Chronotype Among Children and Associations With BMI, Sleep, Anxiety, and Depression. Front. Neurol. 2020, 11, 416. [Google Scholar] [CrossRef] [PubMed]
- Li, S.X.; Chan, N.Y.; Man Yu, M.W.; Lam, S.P.; Zhang, J.; Yan Chan, J.W.; Li, A.M.; Wing, Y.K. Eveningness Chronotype, Insomnia Symptoms, and Emotional and Behavioural Problems in Adolescents. Sleep Med. 2018, 47, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Merikanto, I.; Kronholm, E.; Peltonen, M.; Laatikainen, T.; Lahti, T.; Partonen, T. Relation of Chronotype to Sleep Complaints in the General Finnish Population. Chronobiol. Int. 2012, 29, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Lehnkering, H.; Siegmund, R. Influence of Chronotype, Season, and Sex of Subject on Sleep Behavior of Young Adults. Chronobiol. Int. 2007, 24, 875–888. [Google Scholar] [CrossRef]
- Duffy, J.F.; Roepke, S.E. Differential Impact of Chronotype on Weekday and Weekend Sleep Timing and Duration. Nat. Sci. Sleep 2010, 2, 213. [Google Scholar] [CrossRef] [Green Version]
- Kabrita, C.; Hajjar-Muça, T.; Duffy, J.F. Predictors of Poor Sleep Quality among Lebanese University Students: Association between Evening Typology, Lifestyle Behaviors, and Sleep Habits. Nat. Sci. Sleep 2014, 14, 11. [Google Scholar] [CrossRef] [Green Version]
- Silva, V.M.; Magalhaes, J.E.d.M.; Duarte, L.L. Quality of Sleep and Anxiety Are Related to Circadian Preference in University Students. PLoS ONE 2020, 15, e0238514. [Google Scholar] [CrossRef]
- Glavin, E.E.; Ceneus, M.; Chanowitz, M.; Kantilierakis, J.; Mendelow, E.; Mosquera, J.; Spaeth, A.M. Relationships between Sleep, Exercise Timing, and Chronotype in Young Adults. J. Health Psychol. 2020, 135910532092653. [Google Scholar] [CrossRef]
- Sun, J.; Chen, M.; Cai, W.; Wang, Z.; Wu, S.; Sun, X.; Liu, H. Chronotype: Implications for Sleep Quality in Medical Students. Chronobiol. Int. 2019, 36, 1115–1123. [Google Scholar] [CrossRef]
- Sasawaki, Y.; Shiotani, H. The Influence of Chronotype and Working Condition on Sleep Status and Health Related Quality of Life of Daytime Office Workers. Kobe J. Med. Sci. 2019, 64, E189–E196. [Google Scholar]
- Waterhouse, J.; Reilly, T.; Atkinson, G.; Edwards, B. Jet Lag: Trends and Coping Strategies. Lancet 2007, 369, 1117–1129. [Google Scholar] [CrossRef]
- Martínez-Lozano, N.; Barraco, G.M.; Rios, R.; Ruiz, M.J.; Tvarijonaviciute, A.; Fardy, P.; Madrid, J.A.; Garaulet, M. Evening Types Have Social Jet Lag and Metabolic Alterations in School-Age Children. Sci. Rep. 2020, 10, 16747. [Google Scholar] [CrossRef]
- Raman, S.; Coogan, A.N. A Cross-Sectional Study of the Associations between Chronotype, Social Jetlag and Subjective Sleep Quality in Healthy Adults. Clocks Sleep 2019, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social Jetlag: Misalignment of Biological and Social Time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Russo, P.M.; Bruni, O.; Lucidi, F.; Ferri, R.; Violani, C. Sleep Habits and Circadian Preference in Italian Children and Adolescents. J. Sleep Res. 2007, 16, 163–169. [Google Scholar] [CrossRef]
- Gau, S.-F.; Soong, W.-T. The Transition of Sleep–wake Patterns in Early Adolescence. Sleep 2003, 26, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Dueker, G.L.; Hasher, L.; Goldstein, D. Children’s Time of Day Preference: Age, Gender and Ethnic Differences. Pers. Individ. Dif. 2002, 33, 1083–1090. [Google Scholar] [CrossRef]
- Shinkoda, H.; Matsumoto, K.; Park, Y.M.; Nagashima, H. Sleep–Wake Habits of Schoolchildren According to Grade. Psychiatry Clin. Neurosci. 2000, 54, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Haraszti, R.Á.; Ella, K.; Gyöngyösi, N.; Roenneberg, T.; Káldi, K. Social Jetlag Negatively Correlates with Academic Performance in Undergraduates. Chronobiol. Int. 2014, 31, 603–612. [Google Scholar] [CrossRef]
- Randler, C.; Díaz-Morales, J.F. Morningness in German and Spanish Students: A Comparative Study. Eur. J. Pers. 2007, 21, 419–427. [Google Scholar] [CrossRef]
- Randler, C.; Ebenhöh, N.; Fischer, A.; Höchel, S.; Schroff, C.; Stoll, J.C.; Vollmer, C. Chronotype but Not Sleep Length Is Related to Salivary Testosterone in Young Adult Men. Psychoneuroendocrinology 2012, 37, 1740–1744. [Google Scholar] [CrossRef]
- Gradisar, M.; Gardner, G.; Dohnt, H. Recent Worldwide Sleep Patterns and Problems during Adolescence: A Review and Meta-Analysis of Age, Region, and Sleep. Sleep Med. 2011, 12, 110–118. [Google Scholar] [CrossRef]
- Beşoluk, Ş.; Önder, İ.; Deveci, İ. Morningness–Eveningness Preferences and Academic Achievement of University Students. Chronobiol. Int. 2011, 28, 118–125. [Google Scholar] [CrossRef]
- Jankowski, K.S.; Linke, M. Angry Night Birds: Emotionality, Activity and Sociability Temperament in Adolescent Chronotypes. Chronobiol. Int. 2020, 37, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Cespedes Feliciano, E.M.; Rifas-Shiman, S.L.; Quante, M.; Redline, S.; Oken, E.; Taveras, E.M. Chronotype, Social Jet Lag, and Cardiometabolic Risk Factors in Early Adolescence. JAMA Pediatr. 2019, 173, 1049. [Google Scholar] [CrossRef]
- Gariépy, G.; Riehm, K.E.; Whitehead, R.D.; Doré, I.; Elgar, F.J. Teenage Night Owls or Early Birds? Chronotype and the Mental Health of Adolescents. J. Sleep Res. 2019, 28, e12723. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; Hahn, C.S.; Hasher, L.; Wiprzycka, U.J.; Zelazo, P.D. Time of Day, Intellectual Performance, and Behavioral Problems in Morning versus Evening Type Adolescents: Is There a Synchrony Effect? Pers. Individ. Dif. 2007, 42, 431–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelbmann, G.; Kuhn-Natriashvili, S.; Pazhedath, T.J.; Ardeljan, M.; Wöber, C.; Wöber-Bingöl, Ç. Morningness: Protective Factor for Sleep-Related and Emotional Problems in Childhood and Adolescence? Chronobiol. Int. 2012, 29, 898–910. [Google Scholar] [CrossRef]
- Kang, H.; Lee, M.; Jang, S.J. The Impact of Social Jetlag on Sleep Quality among Nurses: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 18, 47. [Google Scholar] [CrossRef]
- McGowan, N.M.; Uzoni, A.; Faltraco, F.; Thome, J.; Coogan, A.N. The Impact of Social Jetlag and Chronotype on Attention, Inhibition and Decision Making in Healthy Adults. J. Sleep Res. 2020, 29, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Cajochen, C.; Khatami, R. Social Jetlag and Chronotypes in the Chinese Population: Analysis of Data Recorded by Wearable Devices. J. Med. Internet Res. 2019, 21, e13482. [Google Scholar] [CrossRef] [PubMed]
- Parsons, M.J.; Moffitt, T.E.; Gregory, A.M.; Goldman-Mellor, S.; Nolan, P.M.; Poulton, R.; Caspi, A. Social Jetlag, Obesity and Metabolic Disorder: Investigation in a Cohort Study. Int. J. Obes. 2015, 39, 842–848. [Google Scholar] [CrossRef] [Green Version]
- Alabdulkarim, A.; Alayed, O.; Aloraini, O.; Almozini, M.; Aldawsari, K.; Bin Khathlan, Y.Z. The Association between Social Jetlag and Glycemic Control in Diabetic Patients at King Saud University Medical City. Cureus 2020, 12, e9215. [Google Scholar] [CrossRef]
- Islam, Z.; Hu, H.; Akter, S.; Kuwahara, K.; Kochi, T.; Eguchi, M.; Kurotani, K.; Nanri, A.; Kabe, I.; Mizoue, T. Social Jetlag Is Associated with an Increased Likelihood of Having Depressive Symptoms among the Japanese Working Population: The Furukawa Nutrition and Health Study. Sleep 2020, 43, zsz204. [Google Scholar] [CrossRef]
- Atkinson, G.; Drust, B.; Reilly, T.; Waterhouse, J. The Relevance of Melatonin to Sports Medicine and Science; Springer: Cham, Switzerland, 2003; Volume 33, pp. 809–831. [Google Scholar] [CrossRef]
- Alonso-Vale, M.I.C.; Andreotti, S.; Mukai, P.Y.; Borges-Silva, C.D.N.; Peres, S.B.; Cipolla-Neto, J.; Lima, F.B. Melatonin and the Circadian Entrainment of Metabolic and Hormonal Activities in Primary Isolated Adipocytes. J. Pineal Res. 2008, 45, 422–429. [Google Scholar] [CrossRef]
- Astiz, M.; Heyde, I.; Oster, H. Mechanisms of Communication in the Mammalian Circadian Timing System. Int. J. Mol. Sci. 2019, 20, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escames, G.; Ozturk, G.; Baño-Otálora, B.; Pozo, M.J.; Madrid, J.A.; Reiter, R.J.; Serrano, E.; Concepción, M.; Acuña-Castroviejo, D. Exercise and Melatonin in Humans: Reciprocal Benefits. J. Pineal Res. 2012, 52, 1–11. [Google Scholar] [CrossRef]
- Kräuchi, K.; Cajochen, C.; Pache, M.; Flammer, J.; Wirz-Justice, A. Thermoregulatory Effects of Melatonin in Relation to Sleepiness. Chronobiol. Int. 2006, 23, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Brzezinski, A. Melatonin in Humans. N. Engl. J. Med. 1997, 336, 186–195. [Google Scholar] [CrossRef]
- Forbes-Robertson, S.; Dudley, E.; Vadgama, P.; Cook, C.; Drawer, S.; Kilduff, L. Circadian Disruption and Remedial Interventions. Sport. Med. 2012, 42, 185–208. [Google Scholar] [CrossRef]
- Bani Issa, W.; Abdul Rahman, H.; Albluwi, N.; Samsudin, A.B.R.; Abraham, S.; Saqan, R.; Naing, L. Morning and Evening Salivary Melatonin, Sleepiness and Chronotype: A Comparative Study of Nurses on Fixed Day and Rotating Night Shifts. J. Adv. Nurs. 2020, 76, 3372–3384. [Google Scholar] [CrossRef]
- Morera-Fumero, A.L.; Abreu-González, P.; Henry-Benítez, M.; Díaz-Mesa, E.; Yelmo-Cruz, S.; Gracia-Marco, R. Chronotype as Modulator of Morning Serum Melatonin Levels. Actas Esp. Psiquiatr. 2013, 41, 149–153. [Google Scholar]
- Tan, D.; Xu, B.; Zhou, X.; Reiter, R. Pineal Calcification, Melatonin Production, Aging, Associated Health Consequences and Rejuvenation of the Pineal Gland. Molecules 2018, 23, 301. [Google Scholar] [CrossRef] [Green Version]
- Bedrosian, T.A.; Fonken, L.K.; Nelson, R.J. Endocrine Effects of Circadian Disruption. Annu. Rev. Physiol. 2016, 78, 109–131. [Google Scholar] [CrossRef] [Green Version]
- Manni, R.; Cremascoli, R.; Perretti, C.; De Icco, R.; Picascia, M.; Ghezzi, C.; Cerri, S.; Sinforiani, E.; Terzaghi, M. Evening Melatonin Timing Secretion in Real Life Conditions in Patients with Alzheimer Disease of Mild to Moderate Severity. Sleep Med. 2019, 63, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Zaki, N.F.W.; Sabri, Y.M.; Farouk, O.; Abdelfatah, A.; Spence, D.W.; Bahammam, A.S.; Pandi-Perumal, S.R. Depressive Symptoms, Sleep Profiles and Serum Melatonin Levels in a Sample of Breast Cancer Patients. Nat. Sci. Sleep 2020, 12, 135–149. [Google Scholar] [CrossRef] [Green Version]
- Hurley, S.; Goldberg, D.; Von Behren, J.; Clague DeHart, J.; Wang, S.; Reynolds, P. Chronotype and Postmenopausal Breast Cancer Risk among Women in the California Teachers Study. Chronobiol. Int. 2019, 36, 1504–1514. [Google Scholar] [CrossRef] [PubMed]
- Son, K.L.; Jung, D.; Lee, K.M.; Hwang, H.; Lee, J.Y.; Kim, T.Y.; Im, S.A.; Lee, K.H.; Spiegel, D.; Hahm, B.J. Morning Chronotype Is a Protective Factor against Chemotherapy-Induced Hot Flashes in Premenopausal Women with Breast Cancer. Support. Care Cancer 2020, 28, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.M.; Jung, D.Y.; Hwang, H.; Kim, W.H.; Lee, J.Y.; Kim, T.Y.; Im, S.A.; Lee, K.H.; Spiegel, D.; Hahm, B.J. Late Chronotypes Are Associated with Neoadjuvant Chemotherapy-Induced Nausea and Vomiting in Women with Breast Cancer. Chronobiol. Int. 2017, 34, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Hrushesky, W. Circadian Timing of Cancer Chemotherapy. Science 1985, 228, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Lévi, F.; Benavides, M.; Chevelle, C.; Le Saunier, F.; Bailleul, F.; Misset, J.L.; Regensberg, C.; Vannetzel, J.M.; Reinberg, A.; Mathé, G. Chemotherapy of Advanced Ovarian Cancer with 4′-O-Tetrahydropyranyl Doxorubicin and Cisplatin: A Randomized Phase II Trial with an Evaluation of Circadian Timing and Dose-Intensity. J. Clin. Oncol. 1990, 8, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Barrett, R.J.; Blessing, J.A.; Homesley, H.D.; Twiggs, L.; Webster, K.D. Circadian-Timed Combination Doxorubicin-Cisplatin Chemotherapy for Advanced Endometrial Carcinoma: A Phase II Study of the Gynecologic Oncology Group. Am. J. Clin. Oncol. Cancer Clin. Trials 1993, 16, 494–496. [Google Scholar] [CrossRef]
- Kobayashi, M.; To, H.; Tokue, A.; Fujimura, A.; Kobayashi, E. Cisplatin-Induced Vomiting Depends on Circadian Timing. Chronobiol. Int. 2001, 18, 851–863. [Google Scholar] [CrossRef]
- Innominato, P.F.; Giacchetti, S.; Moreau, T.; Bjarnason, G.A.; Smaaland, R.; Focan, C.; Garufi, C.; Iacobelli, S.; Tampellini, M.; Tumolo, S.; et al. Fatigue and Weight Loss Predict Survival on Circadian Chemotherapy for Metastatic Colorectal Cancer. Cancer 2013, 119, 2564–2573. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montaruli, A.; Castelli, L.; Mulè, A.; Scurati, R.; Esposito, F.; Galasso, L.; Roveda, E. Biological Rhythm and Chronotype: New Perspectives in Health. Biomolecules 2021, 11, 487. https://doi.org/10.3390/biom11040487
Montaruli A, Castelli L, Mulè A, Scurati R, Esposito F, Galasso L, Roveda E. Biological Rhythm and Chronotype: New Perspectives in Health. Biomolecules. 2021; 11(4):487. https://doi.org/10.3390/biom11040487
Chicago/Turabian StyleMontaruli, Angela, Lucia Castelli, Antonino Mulè, Raffaele Scurati, Fabio Esposito, Letizia Galasso, and Eliana Roveda. 2021. "Biological Rhythm and Chronotype: New Perspectives in Health" Biomolecules 11, no. 4: 487. https://doi.org/10.3390/biom11040487