
Atrial Natriuretic Peptides, Right Atrial Infarction and Prognosis of Patients with Myocardial Infarction—A Single-Center Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. NT-proANP Assay
2.4. Statistical Analysis
3. Results
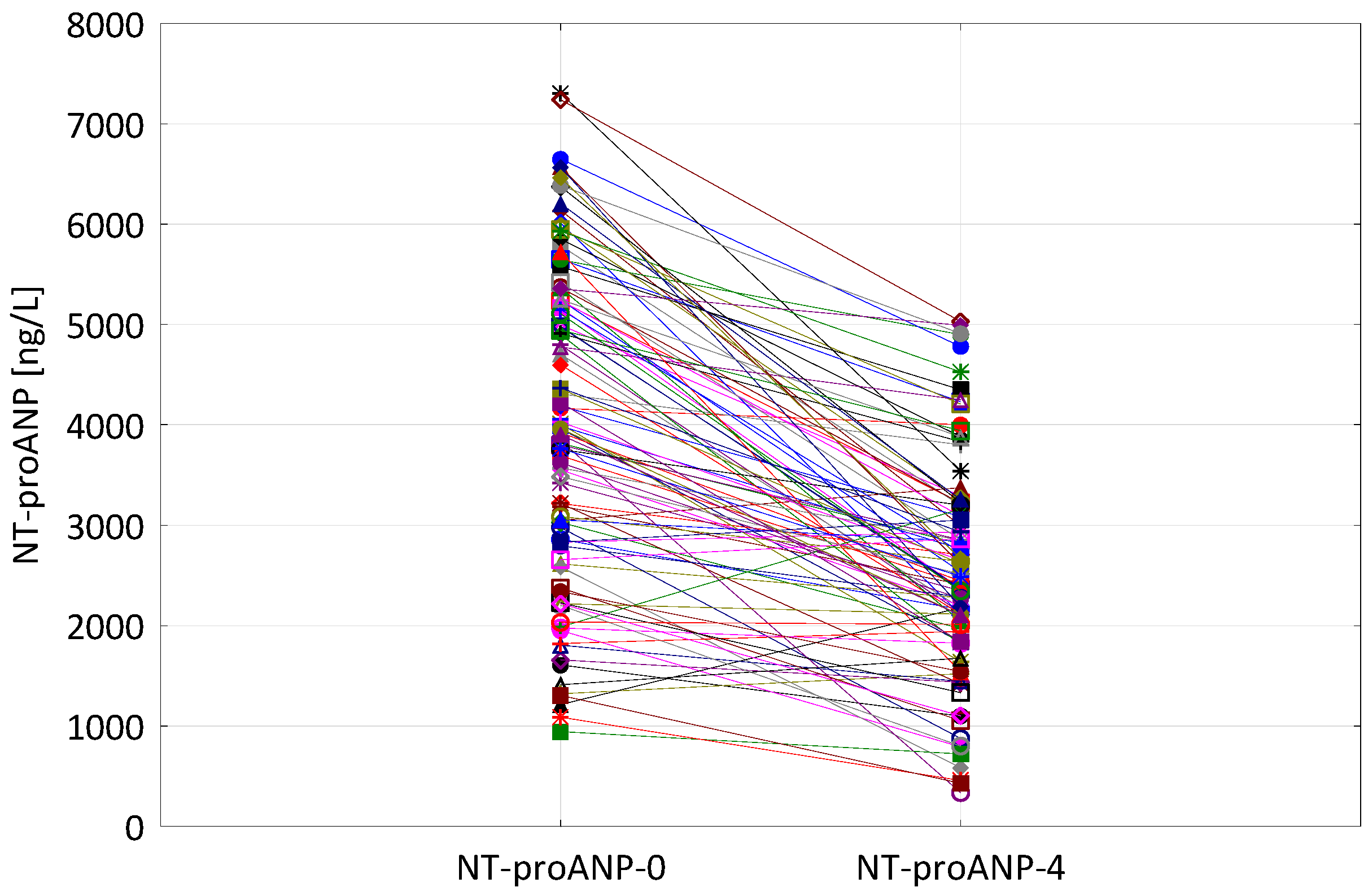
3.1. NT-proANP Levels—Relation to Clinical Data
3.2. Right Atrial Infarction–Relation to Clinical Data
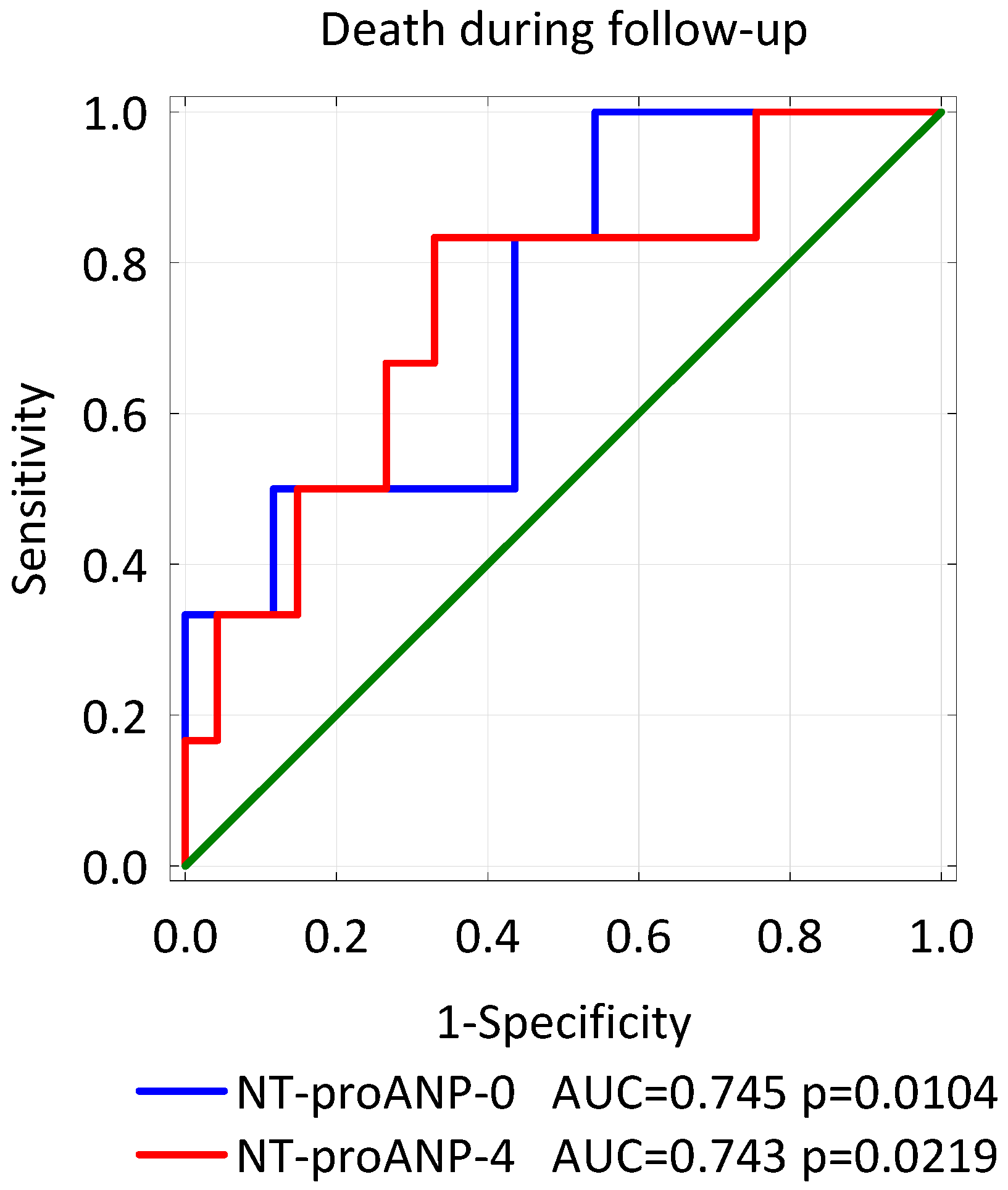
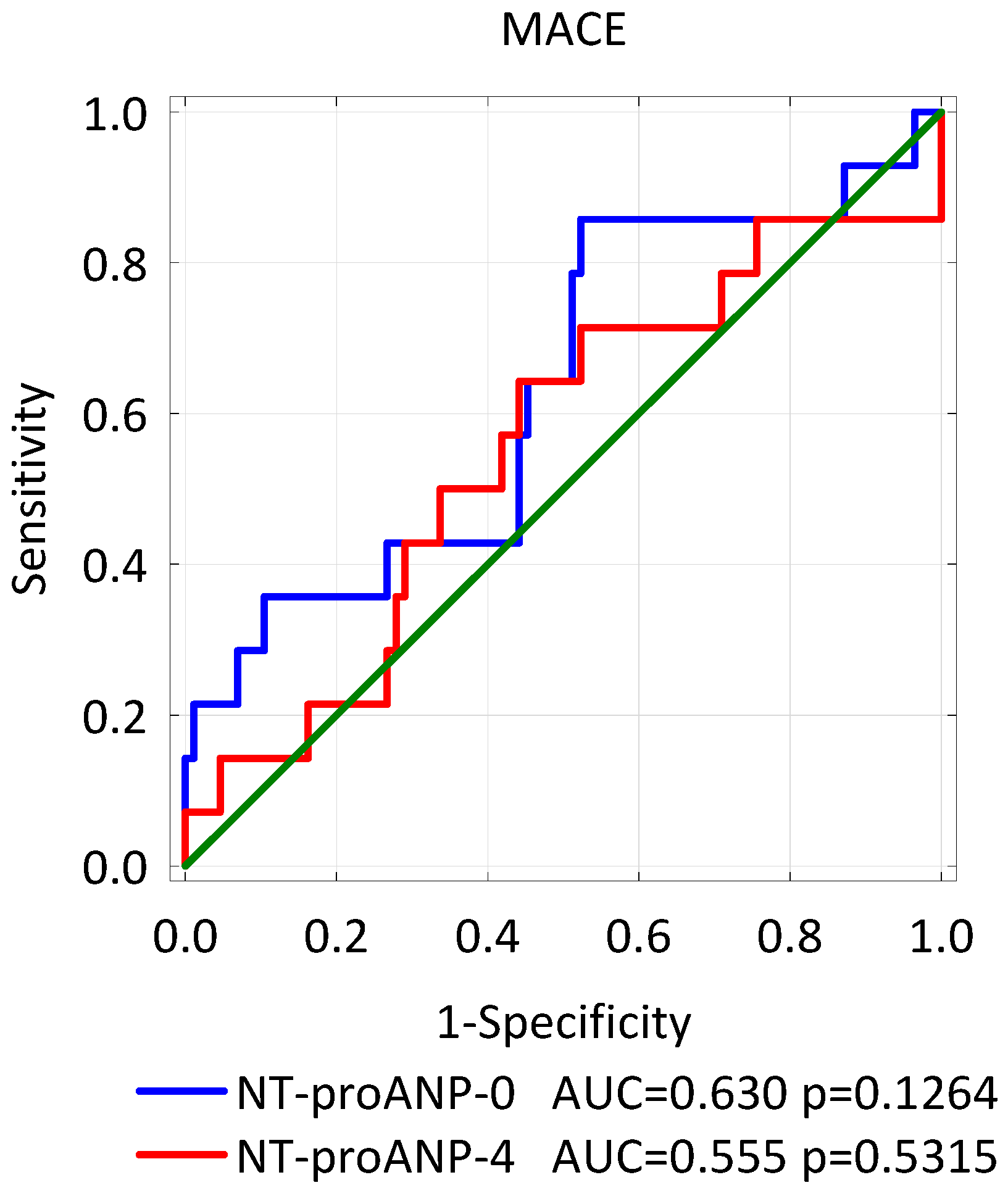
3.3. NT-proANP Levels, Right Atrium Infarction—Prognostic Implications
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Potter, L.R.; Yoder, A.R.; Flora, D.R.; Antos, L.K.; Dickey, D.M. Natriuretic Peptides: Their Structures, Receptors, Physiologic Functions and Therapeutic Applications. Handb. Exp. Pharmacol. 2009, 191, 341–366. [Google Scholar] [CrossRef] [Green Version]
- Saito, Y. Roles of Atrial Natriuretic Peptide and Its Therapeutic Use. J. Cardiol. 2010, 56, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakao, K.; Sugawara, A.; Morii, N.; Sakamoto, M.; Yamada, T.; Itoh, H.; Shiono, S.; Saito, Y.; Nishimura, K.; Ban, T. The Pharmacokinetics of Alpha-Human Atrial Natriuretic Polypeptide in Healthy Subjects. Eur. J. Clin. Pharmacol. 1986, 31, 101–103. [Google Scholar] [CrossRef] [PubMed]
- Yandle, T.G.; Richards, A.M.; Nicholls, M.G.; Cuneo, R.; Espiner, E.A.; Livesey, J.H. Metabolic Clearance Rate and Plasma Half Life of Alpha-Human Atrial Natriuretic Peptide in Man. Life Sci. 1986, 38, 1827–1833. [Google Scholar] [CrossRef]
- Svanegaard, J.; Johansen, J.B.; Klitgaard, N.A.; Thayssen, P.; Haghfelt, T. Correlation Between Serial Changes in Left-Sided Heart Chambers and Atrial Natriuretic Peptide and N-Terminal Pro Atrial Natriuretic Peptide after a First Myocardial Infarction: An Echocardiographic Study. Scand. Cardiovasc. J. 1999, 33, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.L.R.; Venecia, T.D.; Patnaik, S.; Figueredo, V.M. Atrial Myocardial Infarction: A Tale of the Forgotten Chamber. Int. J. Cardiol. 2016, 202, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Gardin, J.M.; Singer, D.H. Atrial Infarction: Importance, Diagnosis, and Localization. Arch. Intern. Med. 1981, 141, 1345–1348. [Google Scholar] [CrossRef] [PubMed]
- Cushing, E.H.; Feil, H.S.; Stanton, E.J.; Wartman, W.B. Infarction of the Cardiac Auricles (Atria): Clinical, Pathological, and Experimental Studies. Heart 1942, 4, 17–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duque-González, L.; Orrego-Garay, M.J.; Lopera-Mejía, L.; Duque-Ramírez, M. Atrial Infarction: A Literature Review. Cardiovasc. Metab. Sci. 2020, 31, 17–24. [Google Scholar] [CrossRef]
- Liu, C.K.; Greenspan, G.; Piccirillo, R.T. Atrial Infarction of the Heart. Circulation 1961, 23, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, J.C.; Kao, P.C.; Hu, D.C.; Heser, D.W.; Heublein, D.; Granger, J.P.; Opgenorth, T.J.; Reeder, G.S. Atrial Natriuretic Peptide Elevation in Congestive Heart Failure in the Human. Science 1986, 231, 1145–1147. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, S.; Nonogi, H.; Miyazaki, S.; Goto, Y.; Haze, K. Hyposecretion of Trial Natriuretic Peptide Due to Associated Right Atrial Infarction in a Patient with Acute Right Ventricular Infarction? Eur. Heart J. 1994, 15, 718–719. [Google Scholar] [CrossRef] [PubMed]
- Wencker, M.; Lechleitner, P.; Dienstl, F.; Hauptlorenz, S.; Puschendorf, B. Early Decrease in Atrial Natriuretic Peptide in Acute Myocardial Infarction. Lancet 1987, 329, 1369. [Google Scholar] [CrossRef]
- Maeda, K.; Tsutamoto, T.; Wada, A.; Mabuchi, N.; Hayashi, M.; Hisanaga, T.; Kamijo, T.; Kinoshita, M. Insufficient Secretion of Atrial Natriuretic Peptide at Acute Phase of Myocardial Infarction. J. Appl. Physiol. 2000, 89, 458–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, M.L.R.; Nwakile, C.; Bhalla, V.; De Venecia, T.; Shah, M.; Figueredo, V.M. Prognostic Significance of Abnormal P Wave Morphology and PR-Segment Displacement after ST-Elevation Myocardial Infarction. Int. J. Cardiol. 2015, 197, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Yıldız, S.S.; Keskin, K.; Avsar, M.; Cetinkal, G.; Sigirci, S.; Aksan, G.; Cetin, S.; Okuyan, E.; Kilickesmez, K.O. Electrocardiographic Diagnosis of Atrial Infarction in Patients with Acute Inferior ST-segment Elevation Myocardial Infarction. Clin. Cardiol. 2018, 41, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Kurl, S.; Ala-Kopsala, M.; Vuolteenaho, O.; Ruskoaho, H.; Nyyssönen, K.; Salonen, J.T. Plasma N-Terminal Fragments of Natriuretic Propeptides Predict the Risk of Cardiovascular Events and Mortality in Middle-Aged Men. Eur. Heart J. 2006, 27, 1230–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omland, T.; Bonarjee, V.V.; Nilsen, D.W.; Sundsfjord, J.A.; Lie, R.T.; Thibault, G.; Dickstein, K. Prognostic Significance of N-Terminal pro-Atrial Natriuretic Factor (1–98) in Acute Myocardial Infarction: Comparison with Atrial Natriuretic Factor (99–126) and Clinical Evaluation. Heart 1993, 70, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.; Cannon, C.P.; Forman, S.; Braunwald, E. Prognostic Value of N-Terminal Proatrial Natriuretic Factor Plasma Levels Measured within the First 12 Hours after Myocardial Infarction. J. Am. Coll. Cardiol. 1995, 26, 1452–1456. [Google Scholar] [CrossRef] [Green Version]
- Otterstad, J.E.; St. John Sutton, M.G.; Froeland, G.S.; Holme, I.; Skjærpe, T.; Hall, C. Prognostic Value of Two-Dimensional Echocardiography and N-Terminal Proatrial Natriuretic Peptide Following an Acute Myocardial Infarction. Assessment of Baseline Values (2–7 Days) and Changes at 3 Months in Patients with a Preserved Systolic Function. Eur. Heart J. 2002, 23, 1011–1020. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major | 1. P-Ta-segment elevation > 0.5 mm in leads V5–V6 and reciprocal depression of P-Ta segment in V1 and V2 leads |
| 2. P-Ta-segment elevation > 0.5 mm in lead I and reciprocal depression of P-Ta segment in II and III leads | |
| 3. P-Ta-segment depression > 1.5 mm in precordial leads and >1.2 mm in leads I, II, III associated with any kind of atrial arrhythmia | |
| Minor | Abnormal P-waves, flattering of P-wave in M-shape or W-shape, irregular or notched P-wave |
| Patient Characteristic | N = 100 | Right Atrial Infarction (N = 36) | No Right Atrial Infarction (N = 64) | p |
|---|---|---|---|---|
| Age [years] | 65 ± 10 | 64 ± 11 | 66 ± 10 | 0.277 |
| Women | 39 (39%) | 10 (28%) | 29 (45%) | 0.084 |
| Heart rate [beats/min] | 70 (62; 80) | 70 (64; 80) | 70 (59; 80) | 0.437 |
| Systolic blood pressure [mmHg] | 140 ± 24 | 140 ± 29 | 141 ± 22 | 0.849 |
| Killip class II–IV | 21 (21%) | 4 (11%) | 17 (27%) | 0.069 |
| Hypertension | 64 (64%) | 20 (56%) | 44 (69%) | 0.187 |
| Diabetes | 28 (28%) | 10 (28%) | 18 (28%) | 0.970 |
| Hyperlipidemia | 22 (22%) | 5 (14%) | 17 (27%) | 0.142 |
| Family history of CAD | 21 (21%) | 8 (22%) | 13 (20%) | 0.822 |
| Current or former smoker | 61 (61%) | 24 (67%) | 37 (58%) | 0.384 |
| Troponin T max [ng/L] | 1990 (738; 4198) | 2054 (622; 3813) | 1968 (770; 4436) | 0.906 |
| Serum creatinine [μmol/L] | 87 (70; 107) | 92 (79; 107) | 85 (69; 104) | 0.239 |
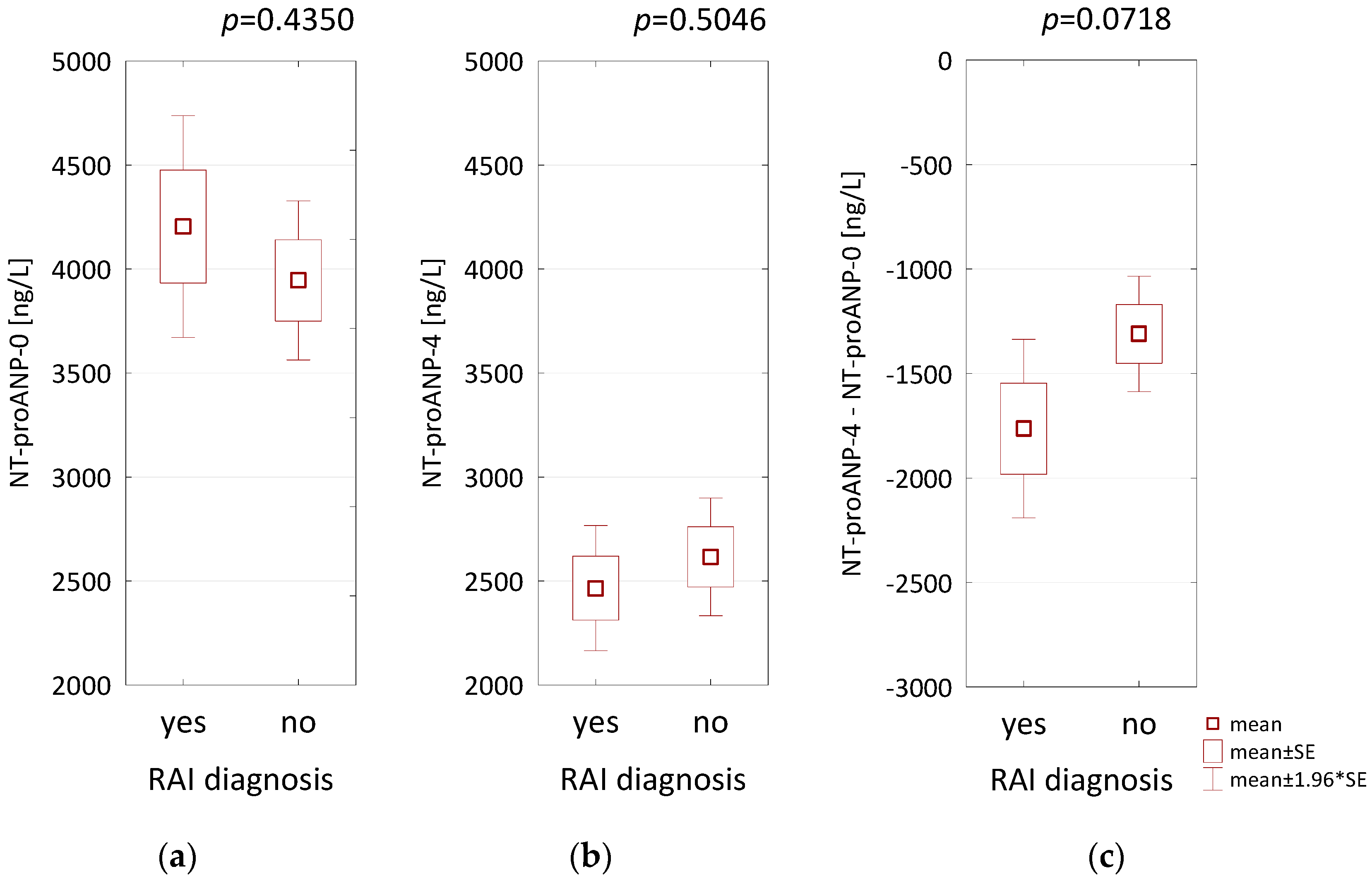
| NT-proANP-0 [ng/L] | 4038 ± 1582 | 4204 ± 1630 | 3945 ± 1559 | 0.435 |
| NT-proANP-4 [ng/L] | 2561 ± 1074 | 2466 ± 920 | 2616 ± 1156 | 0.505 |
| NT-proBNP [ng/L] | 924 (422; 1782) | 985 (260; 1816) | 923 (467; 1705) | 0.511 |
| Atrial fibrillation during hospitalization | 16 (16%) | 4 (11%) | 12 (19%) | 0.317 |
| Multi-vessel disease | 67 (67%) | 30 (83%) | 37 (58%) | 0.009 |
| EF [%] | 51 (47; 56) | 50 (47; 55) | 53 (46; 57) | 0.469 |
| LAVi [mL/m2] | 37 (31; 44) | 38 (31; 44) | 37 (30; 44) | 0.968 |
| RAVi [mL/m2] | 25 (19; 31) | 27 (20; 31) | 23 (19; 30) | 0.436 |
| Concomitant therapy: | ||||
| Aspirin | 99 (99%) | 36 (100%) | 63 (98%) | 0.769 |
| P2Y12 receptor inhibitors | 100 (100%) | 36 (100%) | 64 (100%) | |
| GP IIb/IIIa blocker | 58 (58%) | 22 (61%) | 36 (56%) | 0.636 |
| Statins | 98 (98%) | 35 (97%) | 63 (98%) | 0.743 |
| Beta-blockers | 91 (91%) | 33 (92%) | 58 (91%) | 0.850 |
| ACE-inhibitors | 94 (94%) | 35 (97%) | 59 (92%) | 0.563 |
| NT-proANP-0 [ng/L] | NT-proANP-4 [ng/L] | ||||
|---|---|---|---|---|---|
| Sex | men | 3816 (2584; 5245) | p = 0.3964 | 2453 ± 1127 | p = 0.2089 |
| women | 4165 (3484; 5249) | 2731 ± 976 | |||
| Nutritional status | normal | 4597 (3571; 5357) | p = 0.0915 | 2641 (2112; 3881) | p = 0.1817 |
| over-weight | 3694 (2202; 4976) | 2413 (1824; 3163) | |||
| obesity | 4492 (2831; 5362) | 2400 (1537; 2996) | |||
| Hypertension | yes | 4000 (2705; 5203) | p = 0.7988 | 2485 ± 1130 | p = 0.3428 |
| no | 3755 (2953; 5308) | 2699 ± 968 | |||
| Diabetes | yes | 3765 ± 1462 | p = 0.2833 | 2416 ± 1039 | p = 0.4010 |
| no | 4145 ± 1623 | 2618 ± 1090 | |||
| Hyperlipidemia | yes | 3467 ± 1580 | p = 0.0546 | 1961 ± 1095 | p = 0.0026 |
| no | 4200 ± 1555 | 2731 ± 1012 | |||
| Family history of CAD | yes | 3871 ± 1542 | p = 0.5875 | 2292 ± 1041 | p = 0.1983 |
| no | 4083 ± 1599 | 2633 ± 1078 | |||
| Current or former smoker | yes | 3793 ± 1565 | p = 0.0515 | 2465 ± 1079 | p = 0.2644 |
| no | 4423 ± 1551 | 2713 ± 1064 | |||
| Killip class | I | 3754 (2375; 5235) | p = 0.0071 | 2389 ± 993 | p = 0.0014 |
| II–IV | 4976 (3989; 5646) | 3214 ± 1143 | |||
| Multi-vessel disease | yes | 4073 ± 1562 | p = 0.7590 | 2629 ± 1050 | p = 0.3781 |
| no | 3969 ± 1644 | 2426 ± 1128 | |||
| NT-proANP-0 [ng/L] | NT-proANP-4 [ng/L] | |||
|---|---|---|---|---|
| r or R | p | r or R | p | |
| Age | r = 0.3770 | 0.0001 | r = 0.4813 | <0.0001 |
| Heart rate [beats/min] | R = −0.029 | 0.7743 | R = −0.0522 | 0.6060 |
| Systolic blood pressure [mmHg] | r = −0.0696 | 0.4911 | r = −0.1283 | 0.2034 |
| Serum creatinine [μmol/L] | R = 0.279 | 0.0049 | R = 0.2003 | 0.0456 |
| NT-proBNP [ng/L] | R = 0.2136 | 0.0329 | R = 0.5473 | <0.0001 |
| C-reactive protein [mg/L] | R = 0.2331 | 0.0196 | R = 0.2180 | 0.0293 |
| Hemoglobin [g/dL] | R = −0.3337 | 0.0007 | R = −0.3319 | 0.0007 |
| Lymphocyte count [103/µL] | R = −0.2960 | 0.0028 | R = −0.3880 | 0.0001 |
| Troponin T max [ng/L] | R = 0.1346 | 0.1819 | R = 0.2737 | 0.0058 |
| LVEF [%] | R = −0.1003 | 0.3208 | R = −0.2564 | 0.0100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kacprzak, M.; Brzeczek, M.; Zielinska, M. Atrial Natriuretic Peptides, Right Atrial Infarction and Prognosis of Patients with Myocardial Infarction—A Single-Center Study. Biomolecules 2021, 11, 1833. https://doi.org/10.3390/biom11121833
Kacprzak M, Brzeczek M, Zielinska M. Atrial Natriuretic Peptides, Right Atrial Infarction and Prognosis of Patients with Myocardial Infarction—A Single-Center Study. Biomolecules. 2021; 11(12):1833. https://doi.org/10.3390/biom11121833
Chicago/Turabian StyleKacprzak, Michal, Magdalena Brzeczek, and Marzenna Zielinska. 2021. "Atrial Natriuretic Peptides, Right Atrial Infarction and Prognosis of Patients with Myocardial Infarction—A Single-Center Study" Biomolecules 11, no. 12: 1833. https://doi.org/10.3390/biom11121833