
Elevated Levels of Renalase, the β-NAD(P)H Isomerase, Can Be Used as Risk Factors of Major Adverse Cardiovascular Events and All-Cause Death in Patients with Chronic Kidney Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Material
2.3. Methods
2.4. Statistical Analysis
3. Results
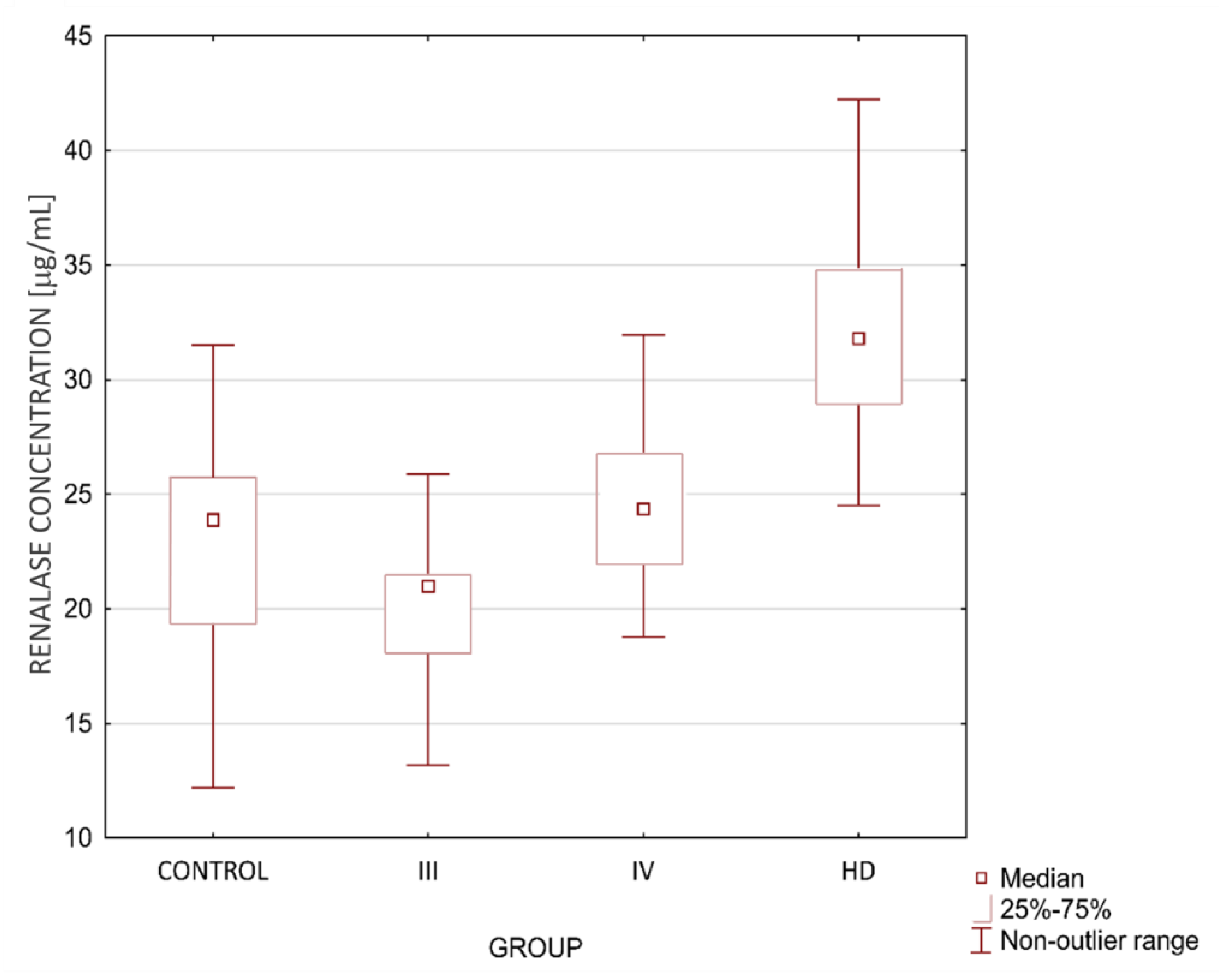
3.1. Data Obtained during Recruitment
3.2. Follow-Up Data
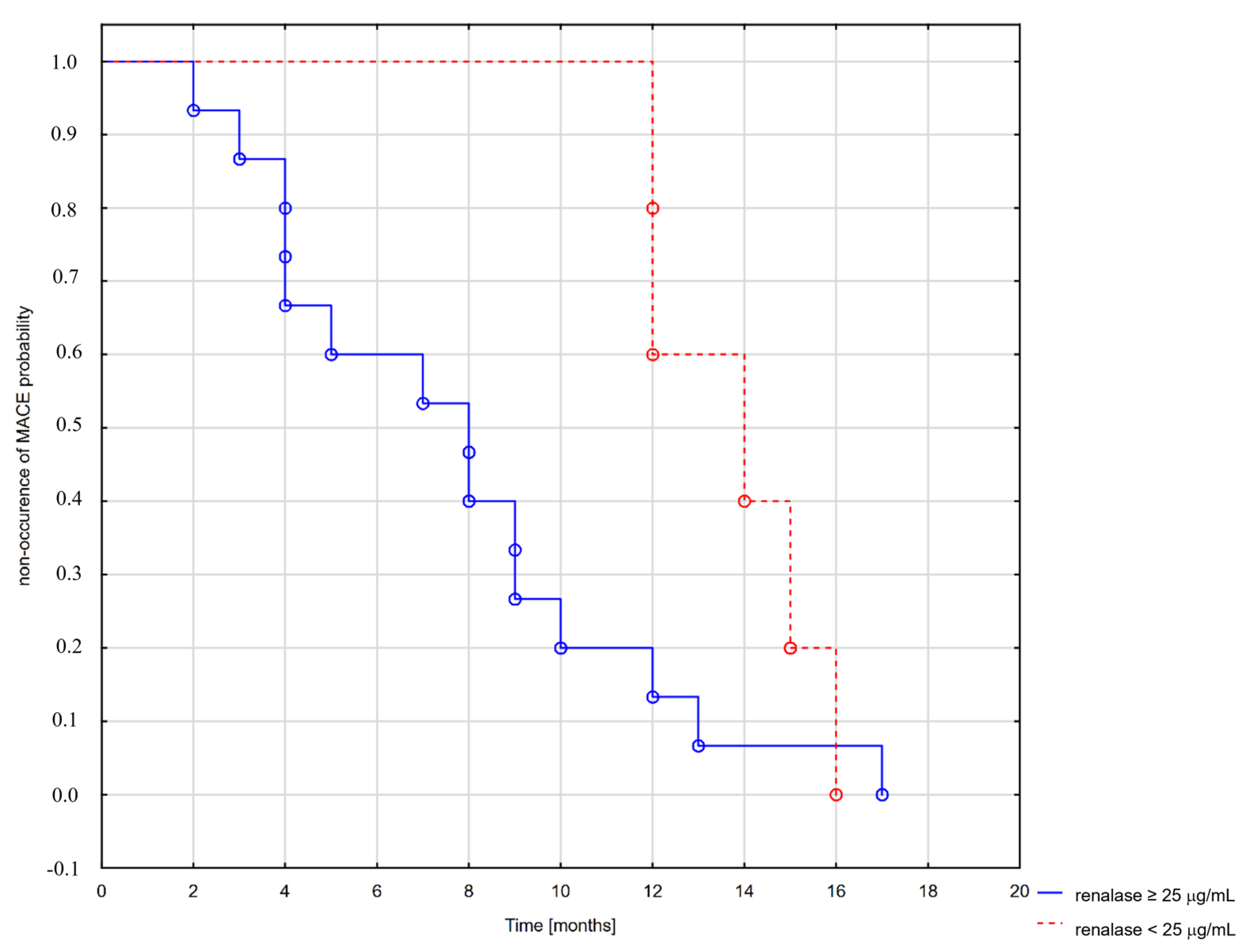
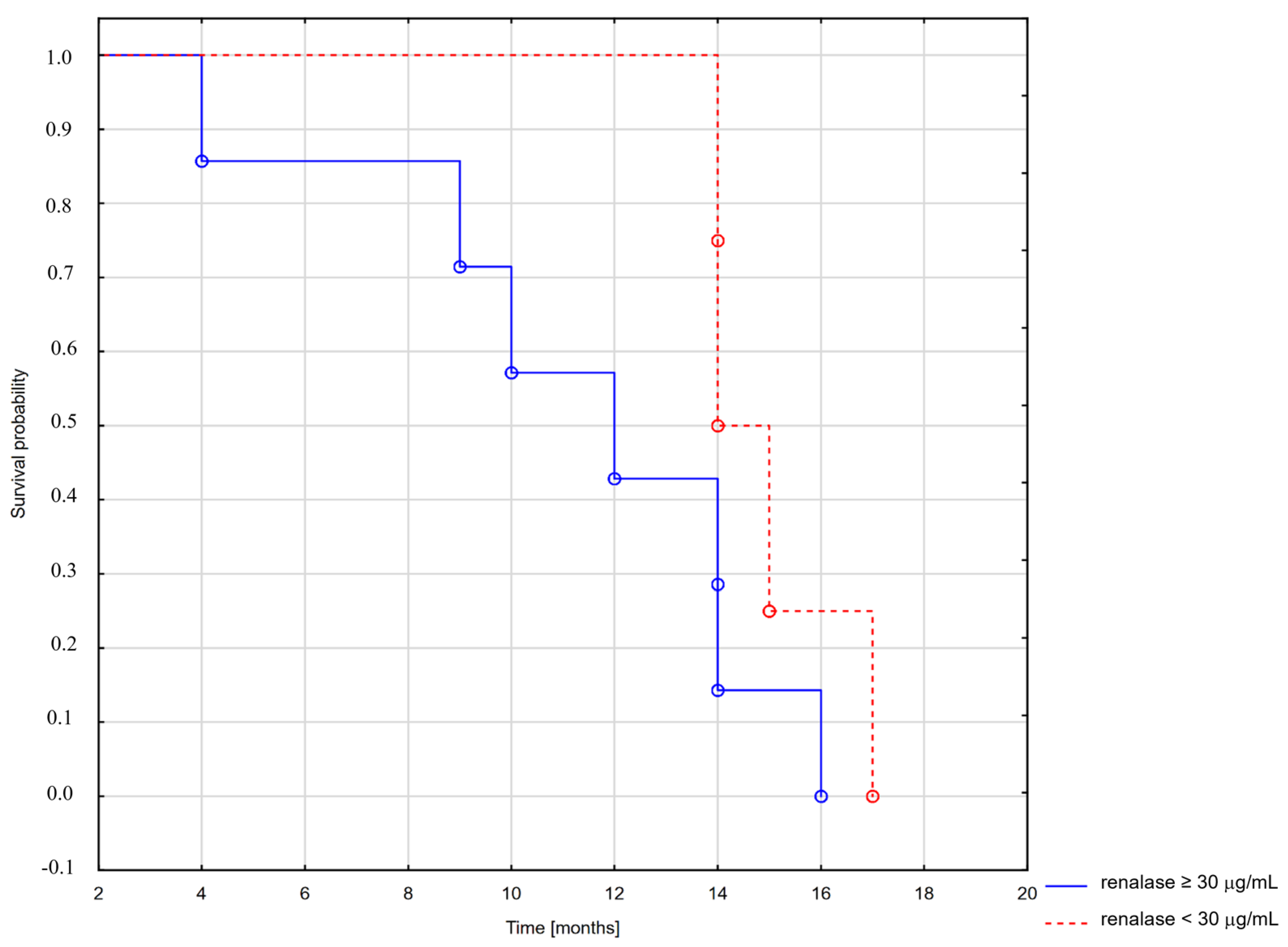
3.3. Analysis of Survival and MACE Occurrence
4. Discussion
5. Conclusions
- Elevated renalase levels (>25 µL/mL) are a risk factor of MACE in patients with chronic kidney disease, but its long-term utility needs further research.
- High renalase levels (>30 µg/mL) can be a risk factor of death among CKD patients.
- In HD patients, all deaths were observed among patients with a renalase serum concentration greater than 30 μg/mL. Further research could show a possible “threshold” level, prompting an evaluation of patients to either intensify treatment or start discussing palliative measures.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Uhlén, M.; Fagerberg, L.; Hallström, B.M. Tissue Expression of RNLS—Summary—The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000184719-RNLS/tissue (accessed on 29 November 2020).
- Wiśniewska, M.; Serwin, N.; Dziedziejko, V.; Marchelek-Myśliwiec, M.; Dołęgowska, B.; Domański, L.; Ciechanowski, K.; Safranow, K.; Pawlik, A. Chronic Kidney Disease Is Associated with Increased Levels of Renalase in Serum and Decreased in Erythrocytes. Pol. Arch. Intern. Med. 2019, 129, 790–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Inker, L.A.; Coresh, J. GFR Estimation: From Physiology to Public Health. Am. J. Kidney Dis. 2014, 63, 820–834. [Google Scholar] [CrossRef] [Green Version]
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 49–73. [Google Scholar] [CrossRef] [Green Version]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Kalinowska, A.; Kowalczyk, M.; Pruszko, C.; Dostęp, P.T. Do Świadczeń Nefrologicznych w Polsce. Raport 2019. Available online: http://www.korektorzdrowia.pl/wp-content/uploads/raport_dostep_do_swiadczen_nefrologicznych.pdf (accessed on 24 July 2021).
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Fox, C.S.; Matsushita, K.; Woodward, M.; Bilo, H.J.G.; Chalmers, J.; Lambers Heerspink, H.J.; Lee, B.J.; Perkins, R.M.; Rossing, P.; Sairenchi, T.; et al. Associations of Kidney Disease Measures with Mortality and End-Stage Renal Disease in Individuals with and without Diabetes: A Meta-Analysis. Lancet 2012, 380, 1662–1673. [Google Scholar] [CrossRef] [Green Version]
- Mahmoodi, B.K.; Matsushita, K.; Woodward, M.; Blankestijn, P.J.; Cirillo, M.; Ohkubo, T.; Rossing, P.; Sarnak, M.J.; Stengel, B.; Yamagishi, K.; et al. Associations of Kidney Disease Measures with Mortality and End-Stage Renal Disease in Individuals with and without Hypertension: A Meta-Analysis. Lancet 2012, 380, 1649–1661. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, K.; Coresh, J.; Sang, Y.; Chalmers, J.; Fox, C.; Guallar, E.; Jafar, T.; Jassal, S.K.; Landman, G.W.D.; Muntner, P.; et al. Estimated Glomerular Filtration Rate and Albuminuria for Prediction of Cardiovascular Outcomes: A Collaborative Meta-Analysis of Individual Participant Data. Lancet Diabetes Endocrinol. 2015, 3, 514–525. [Google Scholar] [CrossRef] [Green Version]
- Van Der Velde, M.; Matsushita, K.; Coresh, J.; Astor, B.C.; Woodward, M.; Levey, A.; De Jong, P.; Gansevoort, R.T.; El-Nahas, M.; Eckardt, K.U.; et al. Lower Estimated Glomerular Filtration Rate and Higher Albuminuria Are Associated with All-Cause and Cardiovascular Mortality. A Collaborative Meta-Analysis of High-Risk Population Cohorts. Kidney Int. 2011, 79, 1341–1352. [Google Scholar] [CrossRef] [Green Version]
- Carney, E.F. The Impact of Chronic Kidney. Nat. Rev. Nephrol. 2020, 16, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarnak, M.J.; Amann, K.; Bangalore, S.; Cavalcante, J.L.; Charytan, D.M.; Craig, J.C.; Gill, J.S.; Hlatky, M.A.; Jardine, A.G.; Landmesser, U.; et al. Chronic Kidney Disease and Coronary Artery Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1823–1838. [Google Scholar] [CrossRef]
- Shah, N.S.; Molsberry, R.; Rana, J.S.; Sidney, S.; Capewell, S.; O’Flaherty, M.; Carnethon, M.; Lloyd-Jones, D.M.; Khan, S.S. Heterogeneous Trends in Burden of Heart Disease Mortality by Subtypes in the United States, 1999-2018: Observational Analysis of Vital Statistics. BMJ-BRIT Med. J. 2020, 370. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.E.; Tighiouart, H.; Elsayed, E.F.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. The Framingham Predictive Instrument in Chronic Kidney Disease. J. Am. Coll. Cardiol. 2007, 50, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Crowley, S.; Desir, G.V.; Xu, J.; Li, G.; Wang, P.; Velazquez, H.; Yao, X.; Li, Y. Renalase Is a Novel, Soluble Monoamine Oxidase That Regulates Cardiac Function and Blood Pressure Find the Latest Version: Renalase Is a Novel, Soluble Monoamine Oxidase That Regulates Cardiac Function and Blood Pressure. J. Clin. Investig. 2005, 115, 1275–1280. [Google Scholar] [CrossRef] [Green Version]
- Pandini, V.; Ciriello, F.; Tedeschi, G.; Rossoni, G.; Zanetti, G.; Aliverti, A. Synthesis of Human Renalase1 in Escherichia Coli and Its Purification as a FAD-Containing Holoprotein. Protein Expr. Purif. 2010, 72, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Eikelis, N.; Hennebry, S.C.; Lambert, G.W.; Schlaich, M.P. Does Renalase Degrade Catecholamines ? Kidney Int. 2011, 79, 1380. [Google Scholar] [CrossRef] [Green Version]
- Weir, M.R.; Eikelis, N.; Hennebry, S.C.; Lambert, G.W.; Schlaich, M.P. Does Renalase Degrade Catecholamines ? The Author Replies. Kidney Int. 2011, 79, 1380–1381. [Google Scholar] [CrossRef] [Green Version]
- Desir, G. Novel Insights into the Physiology of Renalase and Its Role in Hypertension and Heart Disease. Pediatr. Nephrol. 2012, 27, 719–725. [Google Scholar] [CrossRef]
- Medvedev, A.E.; Veselovsky, A.V.; Fedchenko, V.I. Renalase, a New Secretory Enzyme Responsible for Selective Degradation of Catecholamines: Achievements and Unsolved Problems. Biochemistry 2010, 75, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Beaupre, B.A.; Hoag, M.R.; Moran, G.R. Renalase Does Not Catalyze the Oxidation of Catecholamines. Arch. Biochem. Biophys. 2015, 579, 62–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaupre, B.A.; Carmichael, B.R.; Hoag, M.R.; Shah, D.D.; Moran, G.R. Renalase Is an α-NAD(P)H Oxidase/Anomerase. J. Am. Chem. Soc. 2013, 135, 13980–13987. [Google Scholar] [CrossRef]
- Moran, G.R. The Catalytic Function of Renalase: A Decade of Phantoms. Biochim. Biophys. Acta Proteins Proteom. 2016, 1864, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Milani, M.; Ciriello, F.; Baroni, S.; Pandini, V.; Canevari, G.; Bolognesi, M.; Aliverti, A. FAD-Binding Site and NADP Reactivity in Human Renalase: A New Enzyme Involved in Blood Pressure Regulation. J. Mol. Biol. 2011, 411, 463–473. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Velazquez, H.; Moeckel, G.; Chang, J.; Ham, A.; Lee, H.T.; Safirstein, R.; Desir, G.V. Renalase Prevents AKI Independent of Amine Oxidase Activity. J. Am. Soc. Nephrol. 2014, 25, 1226–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Velazquez, H.; Chang, J.; Safirstein, R.; Desir, G.V. Identification of a Receptor for Extracellular Renalase. PLoS ONE 2015, 10, e0122932. [Google Scholar] [CrossRef]
- Mohamed, T.M.A.; Abou-Leisa, R.; Stafford, N.; Maqsood, A.; Zi, M.; Prehar, S.; Baudoin-Stanley, F.; Wang, X.; Neyses, L.; Cartwright, E.J.; et al. The Plasma Membrane Calcium ATPase 4 Signalling in Cardiac Fibroblasts Mediates Cardiomyocyte Hypertrophy. Nat. Commun. 2016, 7, 11074. [Google Scholar] [CrossRef] [PubMed]
- Little, R.; Cartwright, E.J.; Neyses, L.; Austin, C. Plasma Membrane Calcium ATPases (PMCAs) as Potential Targets for the Treatment of Essential Hypertension. Pharmacol. Ther. 2016, 159, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Gu, J.; Guo, J.; Chen, K.; Li, H.; Wang, J. Renalase Attenuates Mouse Fatty Liver Ischemia/Reperfusion Injury through Mitigating Oxidative Stress and Mitochondrial Damage via Activating SIRT1. Oxid. Med. Cell. Longev. 2019, 2019, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, B.; Zhao, Q.; Li, J.; Xing, T.; Wang, F.; Wang, N. Renalase Protects against Contrast-Induced Nephropathy in Sprague-Dawley Rats. PLoS ONE 2015, 10, e0116583. [Google Scholar] [CrossRef]
- Daiber, A.; Hahad, O.; Andreadou, I.; Steven, S.; Daub, S.; Münzel, T. Redox-Related Biomarkers in Human Cardiovascular Disease—Classical Footprints and Beyond. Redox Biol. 2021, 42, 101875. [Google Scholar] [CrossRef]
- Izadpanah, P.; Asadian, F.; Jangjou, A. Association of Serum Renalase Levels and Renalase Rs10887800 Polymorphism with Unstable Angina Pectoris Patients Having Metabolic Syndrome. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 3249–3259. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, D.; Mitic, V.; Stojanovic, M.; Petrovic, D.; Ignjatovic, A.; Stefanovic, N.; Cvetkovic, T.; Kocic, G.; Bojanic, V.; Deljanin Ilic, M. The Partnership between Renalase and Ejection Fraction as a Risk Factor for Increased Cardiac Remodeling Biomarkers in Chronic Heart Failure Patients. Curr. Med. Res. Opin. 2020, 36, 909–919. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, D.; Mitic, V.; Petrovic, D.; Stojanovic, M.; Ignjatovic, A.; Stefanovic, N.; Cvetkovic, T.; Bojanic, V.; Kocic, G.; Ilic, M.D. Association of Plasma Renalase and Left Ventricle Mass Index in Heart Failure Patients Stratified to the Category of the Ejection Fraction: A Pilot Study. Dis. Markers 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safdar, B.; Guo, X.; Johnson, C.; D’Onofrio, G.; Dziura, J.; Sinusas, A.J.; Testani, J.; Rao, V.; Desir, G. Elevated Renalase Levels in Patients with Acute Coronary Microvascular Dysfunction—A Possible Biomarker for Ischemia. Int. J. Cardiol. 2019, 279, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-T.; Sheu, W. Serum Renalase Levels Are Predicted by Brain-Derived Neurotrophic Factor and Associated with Cardiovascular Events and Mortality after Percutaneous Coronary Intervention. J. Clin. Med. 2018, 7, 437. [Google Scholar] [CrossRef] [Green Version]
- Czubilińska-Łada, J.; Gliwińska, A.; Badeński, A.; Szczepańska, M. Associations between Renalase Concentration and the Occurrence of Selected Diseases. Endokrynol. Pol. 2020, 71, 334–342. [Google Scholar] [CrossRef]
- Li, Y.; Wu, W.; Liu, W.; Zhou, M. Roles and Mechanisms of Renalase in Cardiovascular Disease: A Promising Therapeutic Target. Biomed. Pharmacother. 2020, 131, 110712. [Google Scholar] [CrossRef] [PubMed]
- Wiśniewska, M.; Serwin, N.M.; Gomółka, A.; Knop, W.; Heryć, R.; Cecerska-Heryć, E.; Skwirczyńska, E.; Dołęgowska, B. Renalaza—Działanie, Aspekty Kliniczne i Potencjał Terapeutyczny. Forum Nefrol. 2020, 13, 59–68. [Google Scholar]
- Gluba-Brzózka, A.; Michalska-Kasiczak, M.; Franczyk-Skóra, B.; Nocuń, M.; Banach, M.; Rysz, J. Markers of Increased Cardiovascular Risk in Patients with Chronic Kidney Disease. Lipids Health Dis. 2014, 13, 135. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.; Guo, X.; Rao, V.; Gromisch, E.S.; Chung, S.; Kluger, H.M.; Cha, C.; Gorelick, F.; Testani, J.; Safirstein, R.; et al. Identification of Two Forms of Human Plasma Renalase, and Their Association with All-Cause Mortality. Kidney Int. Rep. 2020, 5, 362–368. [Google Scholar] [CrossRef] [Green Version]
- Na, K.Y.; Baek, S.H.; Cha, R.-H.; Kang, S.W.; Park, C.W.; Cha, D.R.; Kim, S.G.; Yoon, S.A.; Kim, S.; Han, S.-Y.; et al. Circulating Renalase Predicts All-Cause Mortality and Renal Outcomes in Patients with Advanced Chronic Kidney Disease. Korean J. Intern. Med. 2019, 34, 858–866. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, A.; Quelhas-Santos, J.; Ferreira, I.; Sampaio, S.; Relvas, M.; Marques, N.; Dias, C.C.; Pestana, M. Circulating Renalase as Predictor of Renal and Cardiovascular Outcomes in Pre-Dialysis CKD Patients: A 5-Year Prospective Cohort Study. Life 2021, 11, 210. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control n = 30 | CKD III n = 30 | CKD IV n = 30 | HD n = 30 | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (LQ-UQ) | Mean ± SD | Median (LQ-UQ) | Mean ± SD | Median (LQ-UQ) | Mean ± SD | Median (LQ-UQ) | ||
| Age (Years) | 57 ± 11 1,2 | 56 (45– 67) | 68 ± 8 1 | 69 (62–74) | 66 ± 11 2 | 67 (60–75) | 64 ± 11 | 65 (60–74) | 0.0028 |
| Systolic BP (mmHg) | 131 ± 21 1 | 125 (120–140) | 134 ± 12 | 132 (130–140) | 140 ± 18 1 | 140 (130–160) | 140 ± 21 | 140 (130–150) | 0.0216 |
| Diastolic BP (mmHg) | 80 ± 11 | 80 (70–85) | 79 ± 9 | 80 (75–85) | 80 ± 11 | 80 (75–90) | 77 ± 12 | 80 (7–80) | 0.44 |
| eGFR | 85 ± 13 | 85 (72–91) | 41 ± 8 | 41 (34–48) | 22 ± 5 | 21 (17–26) | 7 ± 3 | 7 (5–9) | <0.001 |
| Body Weight (kg) | 83 ± 20 | 80 (70–94) | 84 ± 15 1 | 84 (75–92) | 82 ± 16 | 80 (71–92) | 72 ± 16 1 | 72 (64–83) | 0.0286 |
| Height (cm) | 171 ± 8 | 170 (164–176) | 169 ± 8 | 169 (160–176) | 167 ± 9 | 167 (160–175) | 168 ± 11 | 165 (158–178) | 0.50 |
| LDL (mg/dL) | 122 ± 35 | 124 (97–148) | 119 ± 47 | 128 (79–156) | 119 ± 52 | 106 (82–151) | 110 ± 46 | 105 (70–136) | 0.55 |
| HDL (mg/dL) | 55 ± 16 | 52 (45–61) | 50 ± 17 | 48 (39–61) | 52 ± 27 | 41 (37–65) | 49 ± 11 | 48 (42–54) | 0.37 |
| TC (mg/dL) | 174 ± 48 | 187 (130–208) | 187 ± 47 | 188 (151–232) | 191 ± 64 | 84 (144–247) | 179 ± 57 | 162 (136–203) | 0.66 |
| TG (mg/dL) | 167 ± 91 | 161 (105–214) | 168 ± 102 | 135 (96–208) | 202 ± 26 | 171 (116–246) | 159 ± 81 | 145 (103–196) | 0.60 |
| Renalase (µg /mL) | 21.8 ± 9.2 1 | 23.9 (19.4–25.9) | 20.2 ± 3.1 2,4 | 21.0 (18–21.5) | 24.9 ± 4.1 3,4 | 24.6 (2.0–26.8) | 35.6 ± 13.5 1,2,3 | 31.79 (28.9–34.9) | p < 0.01 |
| CV Risk Prediction Score (%) | 11.3 ± 12.1 1,2 | 6.1 (1.4–19.8) | 24.0 ± 14.6 1 | 24.0 (11.3–31.5) | 25.0 ± 17.2 2 | 22.7 (9.8–39.9) | 20 ± 17 | 17 (6–31) | 0.0012 |
| Parameter | Control n = 30 | CKD III n = 30 | CKD IV n = 30 | HD n = 30 | p-Value |
|---|---|---|---|---|---|
| Hypertension n = 95 | 12 1,2,3 | 28 1 | 29 2 | 26 3 | <0.05 |
| Diabetes n = 37 | 7 | 10 | 11 | 9 | >0.05 |
| Smoking n = 21 | 7 | 6 | 5 | 3 | >0.05 |
| No Residual Diuresis n = 6 | 0 | 0 | 0 | 6 | <0.05 |
| Parameter | Control | CKD | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (LQ–UQ) | Mean ± SD | Median (LQ-UQ) | ||
| Age (Years) | 57 ± 11 | 56 (45–67) | 66 ± 7 | 67 (60–74) | <0.001 |
| Systolic BP (mmHg) | 131 ± 21 | 125 (120–140) | 135 ± 18 | 132 (120–140) | 0.01 |
| Diastolic BP (mmHg) | 80 ± 11 | 80 (70–85) | 80 ± 10 | 80 (70–90) | 0.94 |
| eGFR | 85 ± 13 | 85 (72–91) | 49 ± 28 | 41 (26–72) | <0.001 |
| Body Weight (kg) | 83 ± 20 | 80 (70–94) | 83 ± 17 | 80 (72–92) | 0.74 |
| Height (cm) | 171 ± 8 | 170 (164–176) | 169 ± 9 | 170 (161–176) | 0.20 |
| LDL (mg/dL) | 122 ± 35 | 124 (97–148) | 120 ± 44 | 123 (84–151) | 0.34 |
| HDL (mg/dL) | 55 ± 16 | 52 (45–61) | 52 ± 20 | 50 (40–63) | 0.07 |
| TC (mg/dL) | 174 ± 48 | 187 (130–208) | 184 ± 53 | 184 (144–217) | 0.63 |
| TG (mg/dL) | 167 ± 91 | 161 (105–214) | 179 ± 107 | 161 106–214) | 0.98 |
| Renalase (µg/mL) | 21.8 ± 9.2 | 23.9 (19.4–25.9) | 22.3 ± 6.3 | 22.5 (19.9–25.1) | 0.07 |
| CV risk (%) | 11.3 ± 12.1 | 6.1 (1.4–19.8) | 22.8 ± 16.3 | 20.8 (9.4–31.5) | <0.001 |
| Parameter | CONTROL n = 29 | CKD III n = 30 | CKD IV n = 29 | HD n = 30 | p-Value |
|---|---|---|---|---|---|
| MACE n = 22 | 2 | 2 | 5 | 13 | 0.0006 |
| Deaths n = 11 | 0 | 0 | 4 | 7 | 0.0035 |
| Dialysis Initiation n = 5 | 0 | 0 | 5 | N/A | N/A |
| Parameter | CONTROL n = 29 | CKD III n = 30 | CKD IV n = 29 | HD n = 30 | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (LQ-UQ) | Mean ± SD | Median (LQ-UQ) | Mean ± SD | Median (LQ-UQ) | Mean ± SD | Median (LQ-UQ) | ||
| Time to MACE (Months) | 6 ± 5 | 6 (3–10) | 9 ± 3 | 9 (7–12) | 14 ± 2 1 | 14 (13–15) | 7 ± 4 1 | 8 (4–9) | 0.028 |
| Time to Death (Months) | N/A | N/A | N/A | N/A | 15 ± 4.5 | 14.5 (14–16) | 11 ± 4 | 12 (9–14) | >0.05 |
| Time to HD Initiation (Months) | N/A | N/A | N/A | N/A | 10 ± 4.5 | 12 (11–12) | N/A | N/A | N/A |
| Publication | Group | Level | Group | Level |
|---|---|---|---|---|
| Markers of Increased Cardiovascular Risk in Patients with Chronic Kidney Disease [41] | Control Group n = 45 | mean: 251.0 ± 157.0 ng/mL | CKD all stages n = 132 | mean: 316.1 ± 155.3 |
| Identification of Two Forms of Human Plasma Renalase, and Their Association with All-Cause Mortality [42] | Normal renal function n = 10 | mean: 20.39 ± 7.70 µg/mL | All patients n = 267 | mean: 18.8 ± 8.5 µg/mL |
| Circulating renalase predicts all-cause mortality and renal outcomes in patients with advanced chronic kidney disease [43] | Control group n = 16 | mean: 28.2 ± 5.1 µg/mL | CKD patients n = 383 | mean: 75.8 ± 34.8 µg/mL |
| Serum Renalase Levels Are Predicted by Brain-Derived Neurotrophic Factor and Associated with Cardiovascular Events and Mortality after Percutaneous Coronary Intervention [37] | Before percutaneous coronary intervention n = 152 | mean: 47.5 ± 17.3 ng/mL | After percutaneous coronary intervention n = 152 | mean: 35.9 ± 11.3 ng/mL |
| Circulating Renalase as Predictor of Renal and Cardiovascular Outcomes in Pre-Dialysis CKD Patients: A 5-Year Prospective Cohort Study [44] | CKD stages 1 and 2 n = 17 | mean: 42.03 µg/mL | CKD stages 4 and 5 n = 14 | mean: 83.53 µg/mL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knop, W.; Serwin, N.M.; Cecerska-Heryć, E.; Grygorcewicz, B.; Dołęgowska, B.; Gomółka, A.; Wiśniewska, M.; Ciechanowski, K. Elevated Levels of Renalase, the β-NAD(P)H Isomerase, Can Be Used as Risk Factors of Major Adverse Cardiovascular Events and All-Cause Death in Patients with Chronic Kidney Disease. Biomolecules 2021, 11, 1514. https://doi.org/10.3390/biom11101514
Knop W, Serwin NM, Cecerska-Heryć E, Grygorcewicz B, Dołęgowska B, Gomółka A, Wiśniewska M, Ciechanowski K. Elevated Levels of Renalase, the β-NAD(P)H Isomerase, Can Be Used as Risk Factors of Major Adverse Cardiovascular Events and All-Cause Death in Patients with Chronic Kidney Disease. Biomolecules. 2021; 11(10):1514. https://doi.org/10.3390/biom11101514
Chicago/Turabian StyleKnop, Wojciech, Natalia Maria Serwin, Elżbieta Cecerska-Heryć, Bartłomiej Grygorcewicz, Barbara Dołęgowska, Aleksandra Gomółka, Magda Wiśniewska, and Kazimierz Ciechanowski. 2021. "Elevated Levels of Renalase, the β-NAD(P)H Isomerase, Can Be Used as Risk Factors of Major Adverse Cardiovascular Events and All-Cause Death in Patients with Chronic Kidney Disease" Biomolecules 11, no. 10: 1514. https://doi.org/10.3390/biom11101514