
A Standardised Approach to the Biomechanical Evaluation of Tracheal Grafts

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Animal Research
2.2. Tracheal Specimens
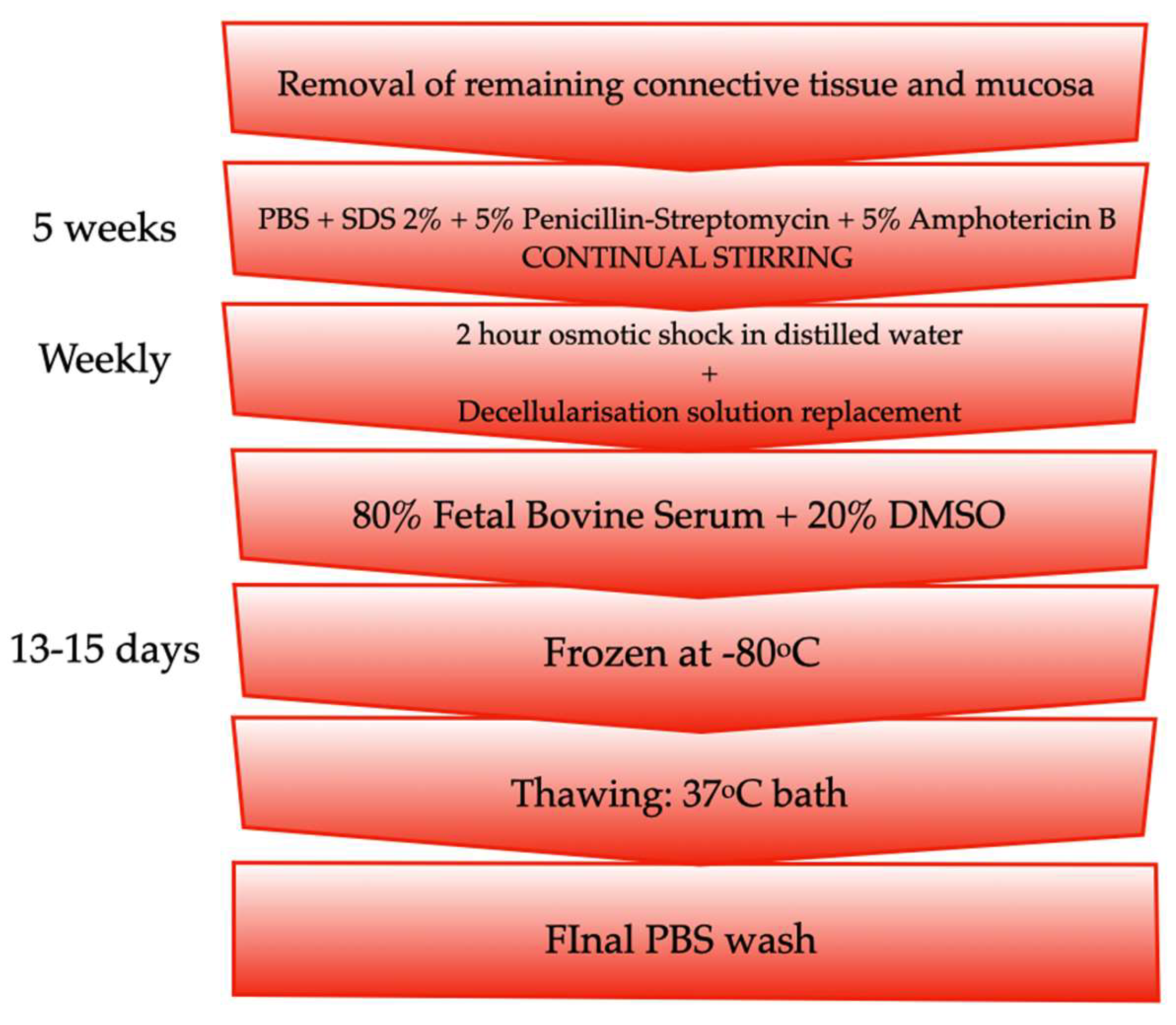
2.3. Tracheal Decellularisation
2.4. Biomechanical Study
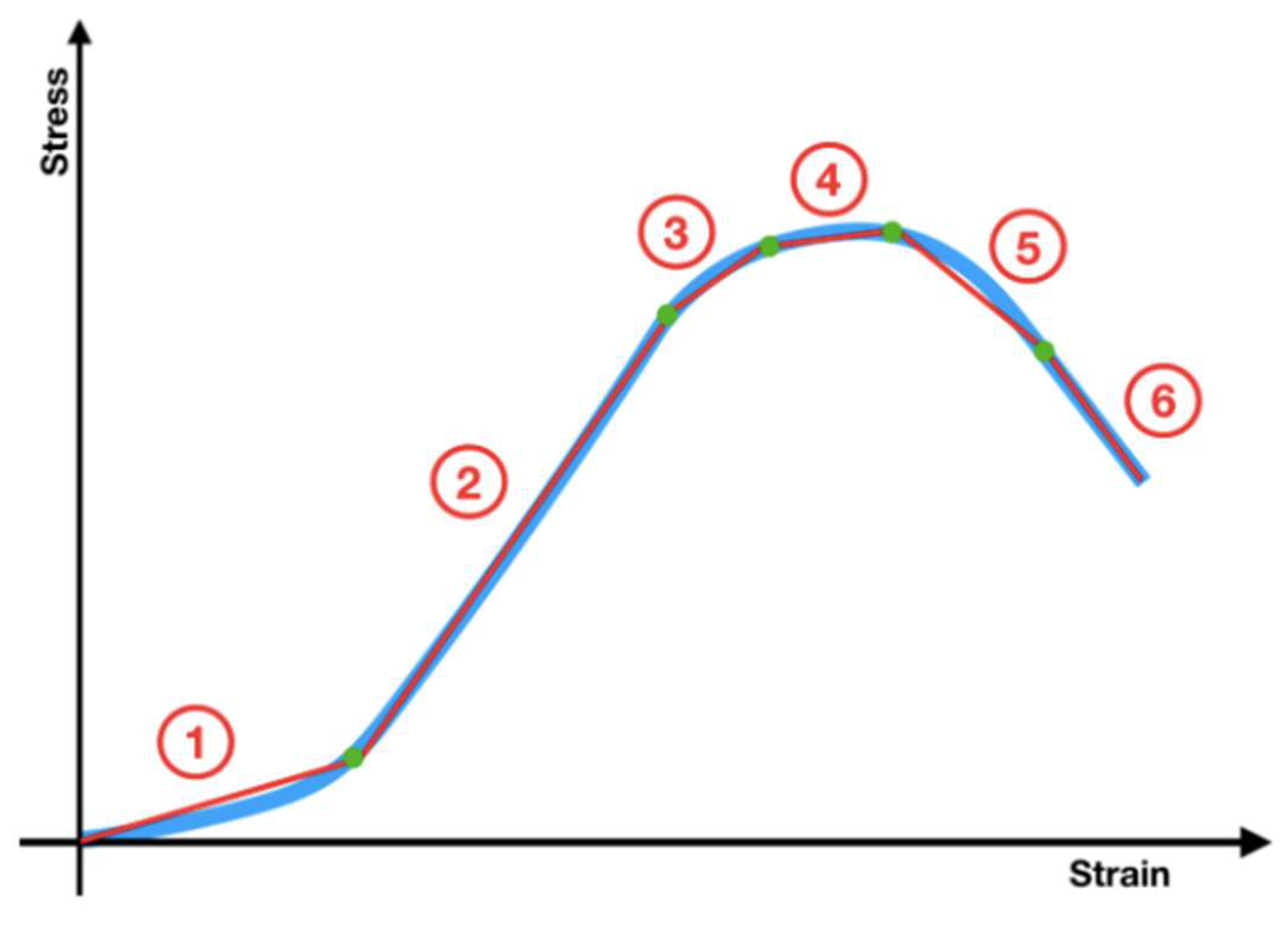
2.4.1. Tensile Tests
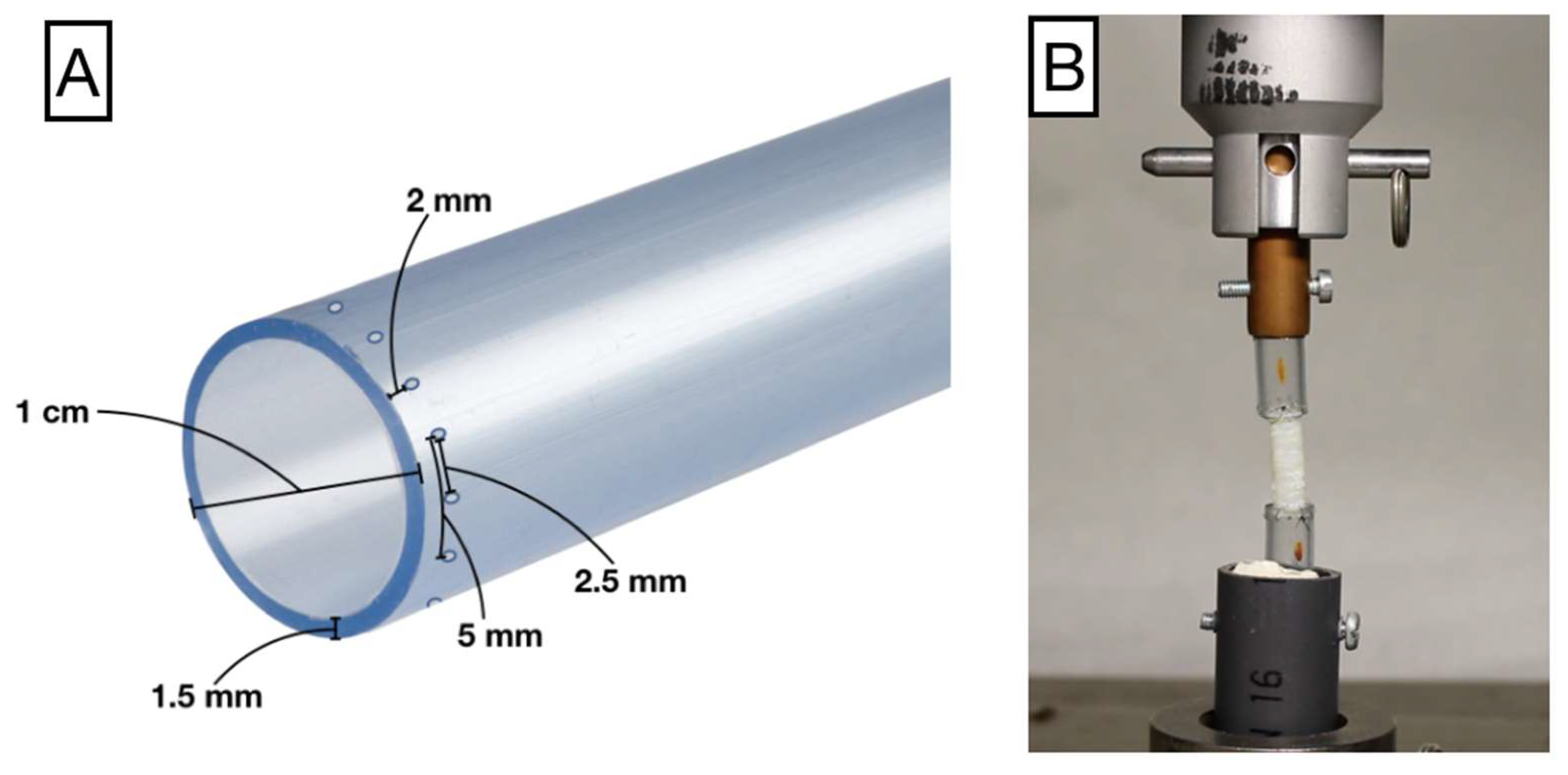
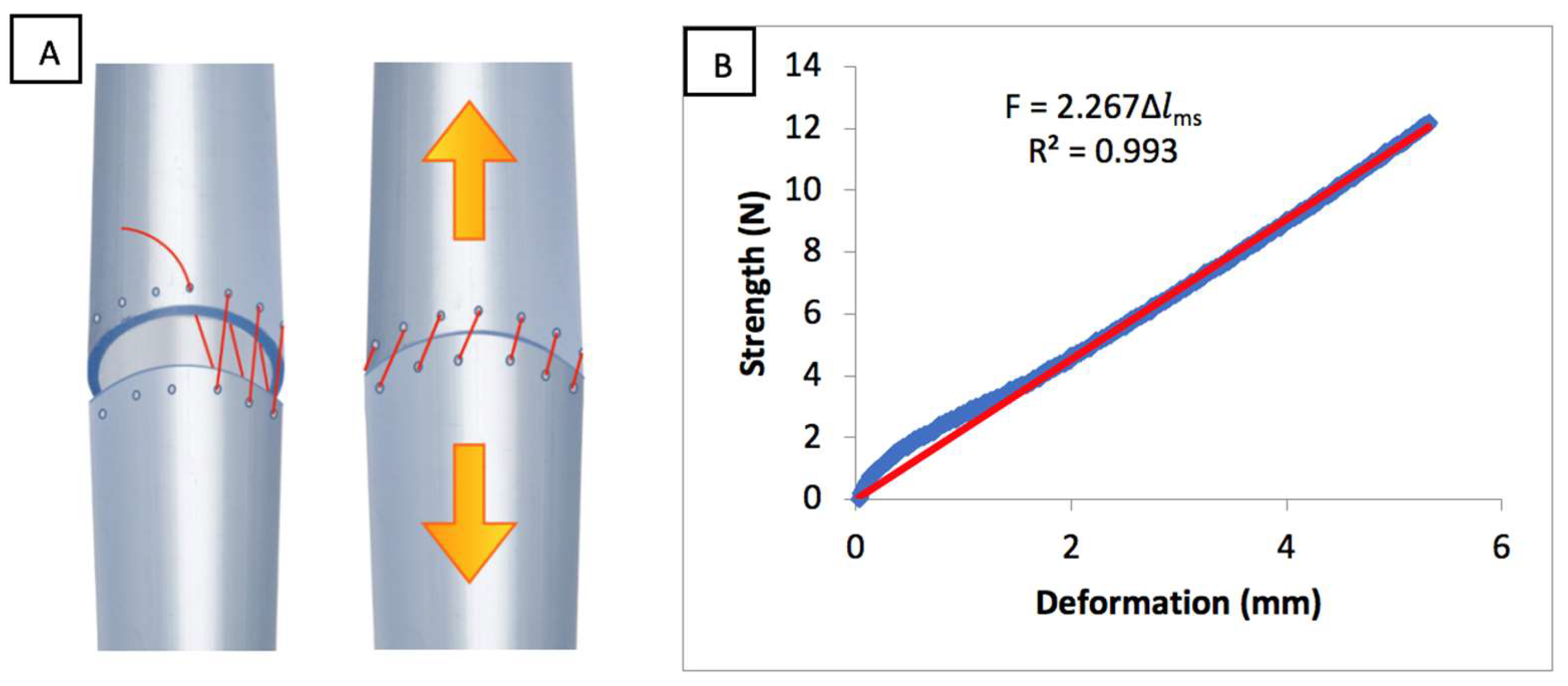
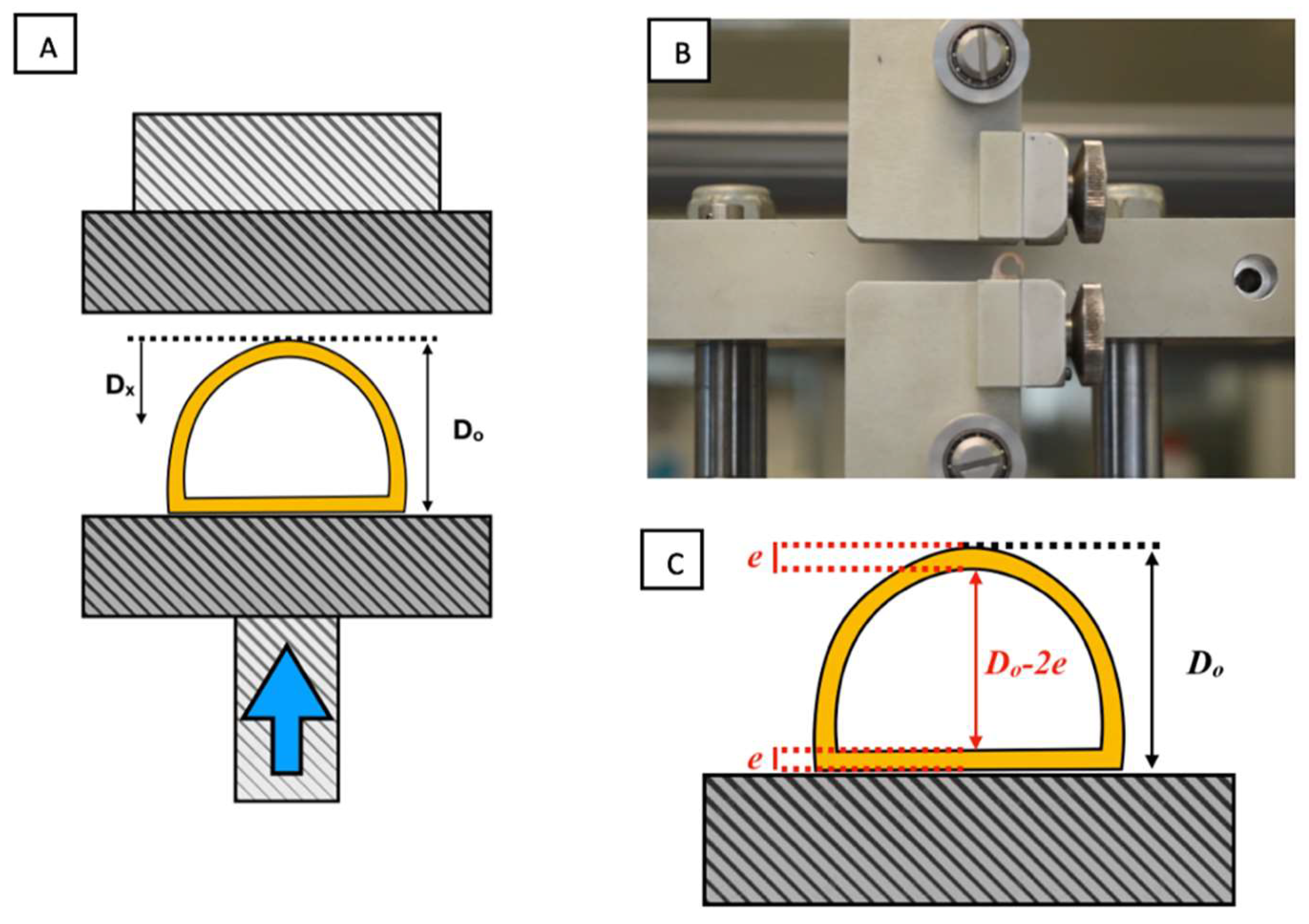
2.4.2. Radial Compression Test
2.5. Statistical Analysis
3. Results
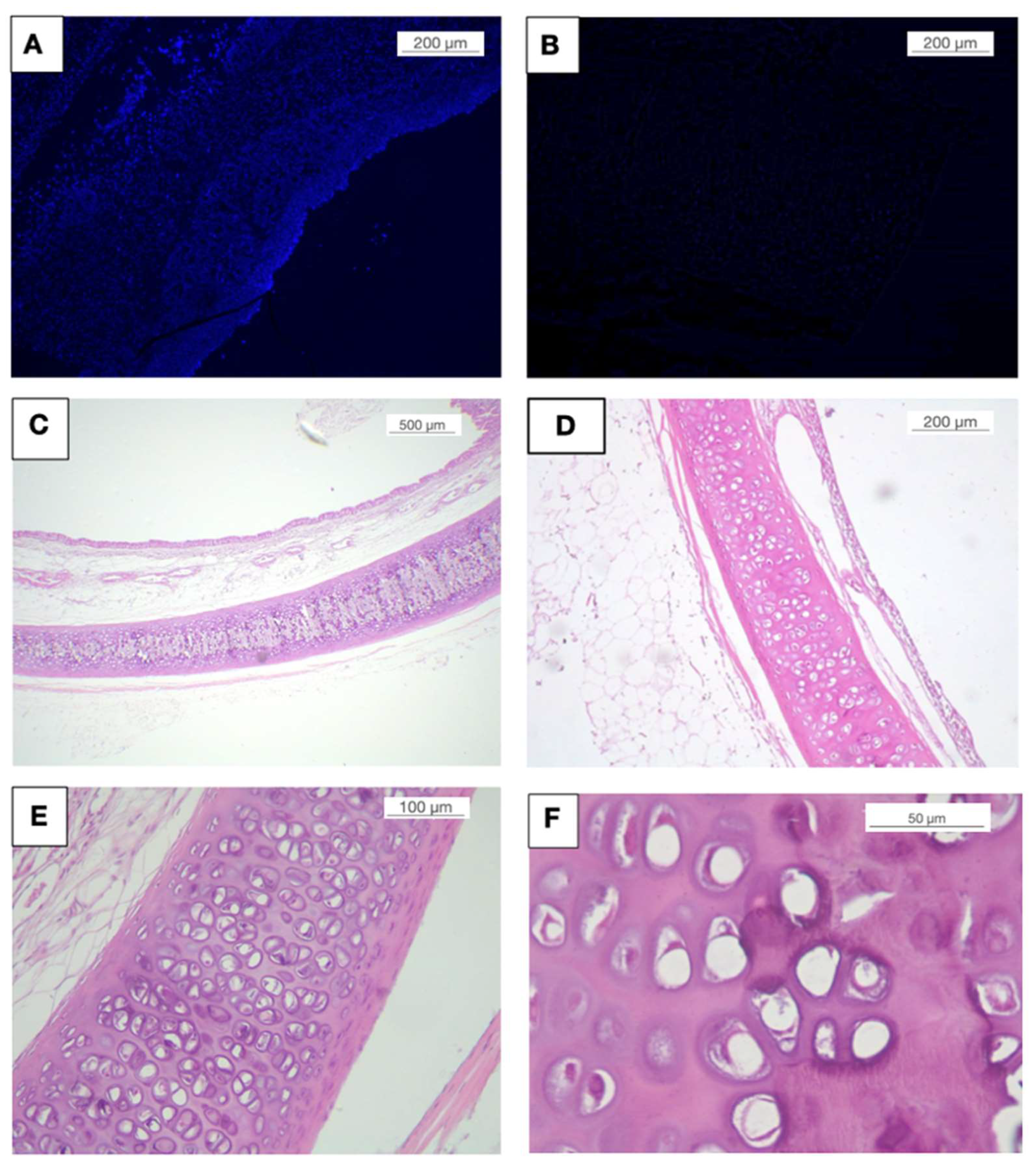
3.1. Decellularisation
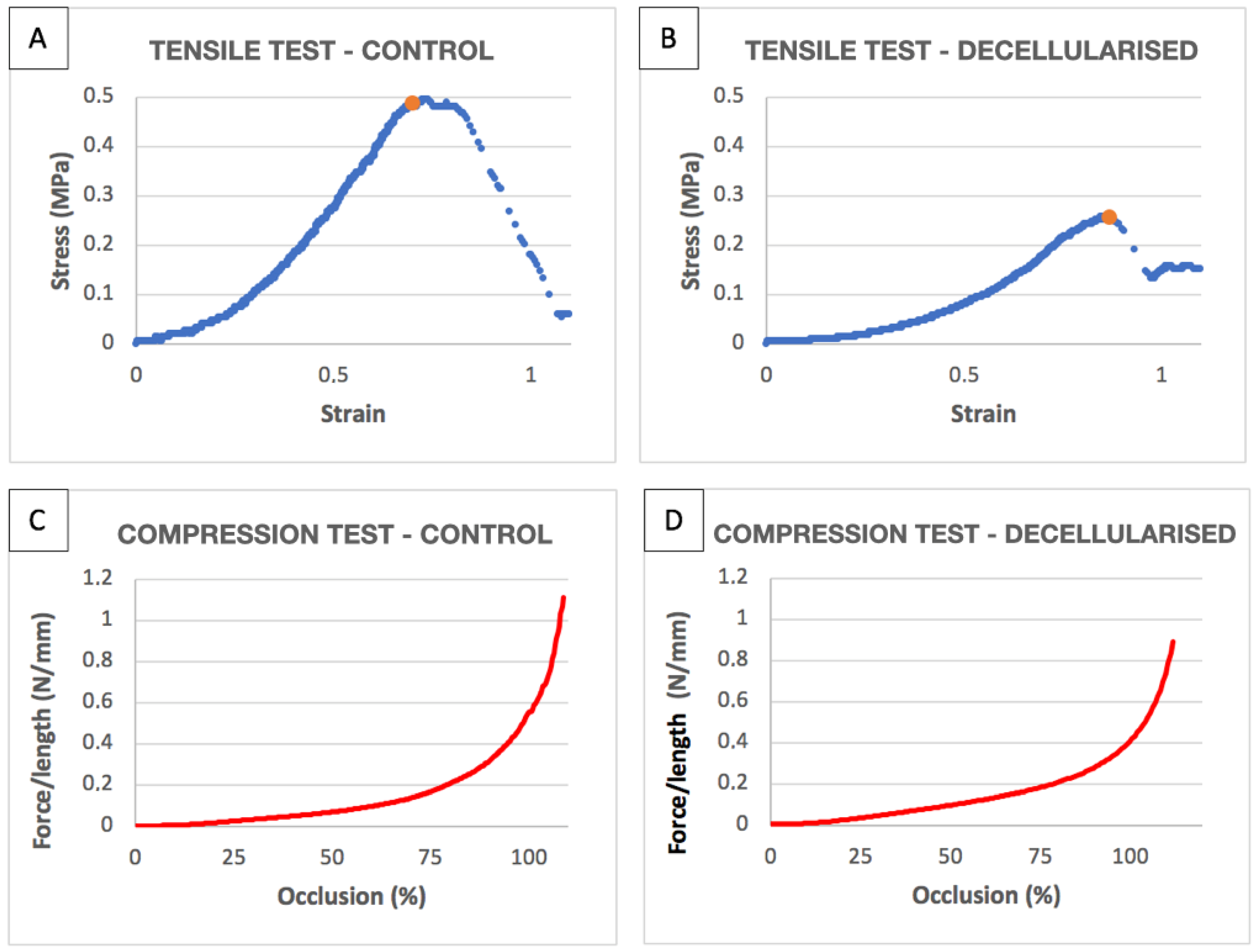
3.2. Tensile Tests
3.3. Compression Tests
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| R2 | |||||
|---|---|---|---|---|---|
| Control 1 | 0.40420303 | 0.90215056 | 0.12909439 | 0.953563904 | 0.99875489 |
| Control 2 | 0.54856126 | 0.81976858 | 0.15110825 | 1.368955241 | 0.99938136 |
| Control 3 | 0.38803491 | 0.93763317 | 0.12716517 | 0.83060708 | 0.99864644 |
| Control 4 | 0.63815134 | 1.01073746 | 0.30837771 | 1.16485761 | 0.99327878 |
| Control 5 | 0.48841058 | 0.69674901 | 0.15157978 | 1.08214574 | 0.99917287 |
| Decellularised 1 | 0.23126649 | 0.8447467 | 0.08295248 | 0.450701404 | 0.997401629 |
| Decellularised 2 | 0.07906587 | 0.60231885 | 0.02377653 | 0.194237888 | 0.995152737 |
| Decellularised 3 | 0.25704701 | 0.86614847 | 0.08670318 | 0.560490726 | 0.99803033 |
| Decellularised 4 | 0.45882506 | 0.58685413 | 0.12242781 | 1.54950156 | 0.998076727 |
Appendix B
| R2 | |||||
|---|---|---|---|---|---|
| Control 1 | 25% | 0.025101336 | 0.1638327 | 0.997012177 | 0.11763228 |
| 50% | 0.068802392 | 0.222956354 | 0.998417427 | ||
| 75% | 0.16695744 | 0.719024065 | 0.998370916 | ||
| 100% | 0.55047896 | 2.884581423 | 0.986746954 | ||
| Control 2 | 25% | 0.01263868 | 0.07017383 | 0.91366111 | 0.06175561 |
| 50% | 0.03600847 | 0.11793468 | 0.98844924 | ||
| 75% | 0.08392836 | 0.36330023 | 0.99356025 | ||
| 100% | 0.29732534 | 2.4991525 | 0.99724707 | ||
| Control 3 | 25% | 0.02655163 | 0.12965658 | 0.97408101 | 0.09201494 |
| 50% | 0.05756974 | 0.15144803 | 0.98578378 | ||
| 75% | 0.1216738 | 0.47044318 | 0.99818636 | ||
| 100% | 0.4415049 | 3.42037414 | 0.99662314 | ||
| Control 4 | 25% | 0.02830126 | 0.11819036 | 0.98279867 | 0.0896916 |
| 50% | 0.05960658 | 0.14729238 | 0.98500466 | ||
| 75% | 0.12236075 | 0.40243118 | 0.99626884 | ||
| 100% | 0.4391475 | 4.46150808 | 0.99538744 | ||
| Control 5 | 25% | 0.01756126 | 0.05047939 | 0.99219239 | 0.04554423 |
| 50% | 0.03210593 | 0.06333302 | 0.99822932 | ||
| 75% | 0.06119527 | 0.18608305 | 0.99595152 | ||
| 100% | 0.16047853 | 0.98869009 | 0.98834538 | ||
| Decellularised 1 | 25% | 0.00918811 | 0.01024683 | 0.90599479 | 0.01422099 |
| 50% | 0.01152998 | 0.01038917 | 0.96669188 | ||
| 75% | 0.01660403 | 0.04111375 | 0.98696429 | ||
| 100% | 0.04080339 | 0.2084726 | 0.98459284 | ||
| Decellularised 2 | 25% | 0.00520851 | 0.01083867 | 0.95625405 | 0.00895111 |
| 50% | 0.0082675 | 0.01479881 | 0.97195543 | ||
| 75% | 0.01204025 | 0.01638842 | 0.98380543 | ||
| 100% | 0.01815821 | 0.04074716 | 0.98841792 | ||
| Decellularised 3 | 25% | 0.00699906 | 0.01305482 | 0.9419434 | 0.01376554 |
| 50% | 0.01157826 | 0.01950127 | 0.97465106 | ||
| 75% | 0.01832657 | 0.03969066 | 0.99386615 | ||
| 100% | 0.0390535 | 0.24461473 | 0.97000712 | ||
| Decellularised 4 | 25% | 0.03447359 | 0.23078059 | 0.99953159 | 0.12094272 |
| 50% | 0.09601747 | 0.27874796 | 0.99952229 | ||
| 75% | 0.18117175 | 0.45357536 | 0.99904677 | ||
| 100% | 0.40507942 | 1.9143551 | 0.99285479 | ||
References
- Grillo, H.C. Development of tracheal surgery: A historical review. Part 2: Treatment of Tracheal Diseases. Ann. Thorac. Surg. 2003, 75, 1039–1047. [Google Scholar] [CrossRef]
- Yamamoto, K.; Kojima, F.; Tomiyama, K.; Nakamura, T.; Hayashino, Y. Meta-analysis of therapeutic procedures for acquired subglottic stenosis in Adults. Ann. Thorac. Surg. 2011, 91, 1747–1753. [Google Scholar] [CrossRef]
- Furlow, P.W.; Mathisen, D.J. Surgical anatomy of the trachea. Ann. Cardiothorac. Surg. 2018, 7, 255–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grillo, H.C. Anatomy of the trachea. In Surgery of the Trachea and Bronchi; DB Decker Inc.: London, UK, 2004; pp. 39–59. [Google Scholar]
- Mulliken, J.B.; Grillo, H.C. The limits of tracheal resection with primary anastomosis: Further anatomical studies in man. J. Thorac. Cardiovasc. Surg. 1968, 55, 418–421. [Google Scholar] [CrossRef]
- Brand-Saberi, B.E.M.; Schäfer, T. Trachea: Anatomy and Physiology. Thorac. Surg. Clin. 2014, 24, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Delaere, P.; Lerut, T.; Van Raemdonck, D. Tracheal transplantation: State of the art and key role of blood supply in its success. Thorac. Surg. Clin. 2018, 28, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Wurtz, A.; Hysi, I.; Kipnis, E.; Zawadzki, C.; Hubert, T.; Jashari, R.; Copin, M.C.; Jude, B. Tracheal reconstruction with a composite graft: Fascial flap-wrapped allogenic aorta with external cartilage-ring support. Interact. Cardiovasc. Thorac. Surg. 2013, 16, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Boiselle, P.M. Imaging of the large airways. Clin. Chest Med. 2008, 29, 181–193. [Google Scholar] [CrossRef]
- Batioglu-Karaaltin, A.; Karaaltin, M.V.; Ovali, E.; Yigit, O.; Kongur, M.; Inan, O.; Bozkurt, E.; Cansiz, H. In vivo tissue-engineered allogenic trachea transplantation in rabbits: A preliminary report. Stem Cell Rev. Rep. 2015, 11, 347–356. [Google Scholar] [CrossRef]
- Maughan, E.F.; Butler, C.R.; Crowley, C.; Teoh, G.Z.; Hondt, M.D.; Hamilton, N.J.; Hynds, R.E.; Lange, P.; Ansari, T.; Urbani, L.; et al. A comparison of tracheal scaffold strategies for pediatric transplantation in a rabbit model. Laryngoscope 2017, 127, E449–E457. [Google Scholar] [CrossRef] [Green Version]
- Sun, F.; Jiang, Y.; Xu, Y.; Shi, H.; Zhang, S.; Liu, X.; Pan, S.; Ye, G.; Zhang, W.; Zhang, F.; et al. Genipin cross-linked decellularized tracheal tubular matrix for tracheal tissue engineering applications. Sci. Rep. 2016, 6, 24429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, C.; Sheshadri, P.; Ketchum, J.M.; Narayanan, L.K.; Weinberger, P.M.; Shirwaiker, R.A. In vitro characterization of design and compressive properties of 3D-biofabricated/decellularized hybrid grafts for tracheal tissue engineering. J. Mech. Behav. Biomed. Mater. 2016, 59, 572–585. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Hong, J.M.; Ju, Y.M.; Jung, J.W.; Kang, H.W.; Lee, S.J.; Yoo, J.J.; Kim, S.W.; Kim, S.H.; Cho, D.W. A novel tissue-engineered trachea with a mechanical behavior similar to native trachea. Biomaterials 2015, 62, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.C.; Rueggeberg, F.A.; Faircloth, H.A.; Cunningham, A.J.; Bush, C.M.; Prosser, J.D.; Waller, J.L.; Postma, G.N.; Weinberger, P.M. Defining the biomechanical properties of the rabbit trachea. Laryngoscope 2014, 124, 2352–2358. [Google Scholar] [CrossRef]
- Rains, J.K.; Bert, J.L.; Roberts, C.R.; Paré, P.D. Mechanical properties of human tracheal cartilage. J. Appl. Physiol. 1992, 72, 219–225. [Google Scholar] [CrossRef]
- Belsey, R. Resection and reconstruction of the intrathoracic trachea. Br. J. Surg. 1950, 38, 200–205. [Google Scholar] [CrossRef]
- Martínez-Hernández, N.J.; Díaz-Cuevas, A.; Milián-Medina, L.; Sancho-Tello, M.; Roselló-Ferrando, J.; Morcillo-Aixelá, A.; Campo-Cañaveral, J.L.; Roig-Bataller, A.; Mata-Roig, M. Decellularized tracheal prelamination implant: A proposed bilateral double organ technique. Artif. Organs 2021. [Google Scholar] [CrossRef]
- Hysi, I.; Wurtz, A.; Zawadzki, C.; Kipnis, E.; Jashari, R.; Hubert, T.; Ung, A.; Copin, M.C.; Jude, B. Immune tolerance of epithelium-denuded-cryopreserved tracheal allograft. Eur. J. Cardiothorac. Surg. 2014, 45, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Özkaya, N.; Nordin, M.; Goldsheyder, D.; Leger, D. Mechanical properties of biological tissues. In Fundamentals of Biomechanics; Springer: Berlin, Germany, 1999; pp. 195–218. [Google Scholar]
- Safshekan, F.; Tafazzoli-Shadpour, M.; Abdouss, M.; Shadmehr, M.B. Mechanical characterization and constitutive modeling of human trachea: Age and gender dependency. Materials 2016, 9, 456. [Google Scholar] [CrossRef] [Green Version]
- AENOR. Biological Evaluation of Medical Devices—Part 6: Tests for Local Effects after Implantation; UNE-EN ISO 10993-6:2007; AENOR: Madrid, Spain, 2009. [Google Scholar]
- Hysi, I.; Kipnis, E.; Fayoux, P.; Copin, M.C.; Zawadzki, C.; Jashari, R.; Hubert, T.; Ung, A.; Ramon, P.; Jude, B.; et al. Successful orthotopic transplantation of short tracheal segments without immunosuppressive therapy. Eur. J. Cardiothorac. Surg. 2014, 47, e54–e61. [Google Scholar] [CrossRef] [Green Version]
- Weidenbecher, M.; Tucker, H.M.; Gilpin, D.A.; Dennis, J.E. Tissue-engineered trachea for airway reconstruction. Laryngoscope 2009, 119, 2118–2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, F.G.; Moriya, H.T. Mechanical Evaluation of tracheal grafts on different scales. Artif. Organs 2018, 42, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Trabelsi, O.; del Palomar, A.P.; López-Villalobos, J.L.; Ginel, A.; Doblaré, M. Experimental characterization and constitutive modeling of the mechanical behavior of the human trachea. Med. Eng. Phys. 2010, 32, 76–82. [Google Scholar] [CrossRef]
- ASTM International. Standard Test Method for Tensile Properties of Plastics; ASTM D638-14; ASTM International: West Conshohocken, PA, USA, 2014. [Google Scholar]
- Grillo, H.C. Postintubation stenosis. In Surgery of the Trachea and Bronchi; Grillo, H.C., Ed.; DB Decker Inc.: London, UK, 2004; pp. 301–339. [Google Scholar]
- Morcillo Aixelá, A.; Bolufer Nadal, S.; Wins Birabén, R.; Galáng Gil, G. Aspectos técnicos quirúrgicos. In Documento de Consenso SECT Sobre Cirugía Traqueal y Laringotraqueal; Martínez Hernández, N.J., López Villalobos, J.L., Eds.; Panamericana: Madrid, Spain, 2015; pp. 32–36. ISBN 978-84-9110-159-8. [Google Scholar]
- Morita, K.; Yokoi, A.; Fukuzawa, H.; Hisamatsu, C.; Endo, K.; Okata, Y.; Tamaki, A.; Mishima, Y.; Oshima, Y.; Maeda, K. Surgical intervention strategies for congenital tracheal stenosis associated with a tracheal bronchus based on the location of stenosis. Pediatr. Surg. Int. 2016, 32, 915–919. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Hernández, N.J.; Mas-Estellés, J.; Milián-Medina, L.; Martínez-Ramos, C.; Cerón-Navarro, J.; Galbis-Caravajal, J.; Roig-Bataller, A.; Mata-Roig, M. A Standardised Approach to the Biomechanical Evaluation of Tracheal Grafts. Biomolecules 2021, 11, 1461. https://doi.org/10.3390/biom11101461
Martínez-Hernández NJ, Mas-Estellés J, Milián-Medina L, Martínez-Ramos C, Cerón-Navarro J, Galbis-Caravajal J, Roig-Bataller A, Mata-Roig M. A Standardised Approach to the Biomechanical Evaluation of Tracheal Grafts. Biomolecules. 2021; 11(10):1461. https://doi.org/10.3390/biom11101461
Chicago/Turabian StyleMartínez-Hernández, Néstor J., Jorge Mas-Estellés, Lara Milián-Medina, Cristina Martínez-Ramos, José Cerón-Navarro, José Galbis-Caravajal, Amparo Roig-Bataller, and Manuel Mata-Roig. 2021. "A Standardised Approach to the Biomechanical Evaluation of Tracheal Grafts" Biomolecules 11, no. 10: 1461. https://doi.org/10.3390/biom11101461