
Lipid Profile, Eating Habit, and Physical Activity in Children with Down Syndrome: A Prospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DS | Down Syndrome |
| KIDMED | Mediterranean Diet Quality Index in children and adolescents |
| Godin | Godin–Shepard Leisure-Time Physical Activity Questionnaire |
| BMI | Body Mass Index |
| LDL-c | Low-density lipoprotein cholesterol |
| HDL-c | High-density lipoprotein cholesterol |
| TGC | Triglycerides |
| TC | Total cholesterol |
| SD | Standard deviation |
References
- Asim, A.; Kumar, A.; Muthuswamy, S.; Jain, S.; Agarwal, S. Down syndrome: An insight of the disease. J. Biomed. Sci. 2015, 22, 41. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, S.E.; Skotko, B.G.; Rafii, M.S.; Strydom, A.; Pape, S.E.; Bianchi, D.W.; Sherman, S.L.; Reeves, R.H. Down syndrome. Nat. Rev. Dis. Primers 2020, 6, 9. [Google Scholar] [CrossRef]
- de Graaf, G.; Buckley, F.; Skotko, B.G. Estimation of the number of people with Down syndrome in Europe. Eur. J. Hum. Genet. 2021, 29, 402–410. [Google Scholar] [CrossRef]
- Lott, I.T.; Head, E. Dementia in Down syndrome: Unique insights for Alzheimer disease research. Nat. Rev. Neurol. 2019, 15, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Bertapelli, F.; Pitetti, K.; Agiovlasitis, S.; Guerra-Junior, G. Overweight and obesity in children and adolescents with Down syndrome—Prevalence, determinants, consequences, and interventions: A literature review. Res. Dev. Disabil. 2016, 57, 181–192. [Google Scholar] [CrossRef] [PubMed]
- van Gameren-Oosterom, H.B.; van Dommelen, P.; Schönbeck, Y.; Oudesluys-Murphy, A.M.; van Wouwe, J.P.; Buitendijk, S.E. Prevalence of overweight in Dutch children with Down syndrome. Pediatrics. 2012, 130, e1520–e1526. [Google Scholar] [CrossRef] [PubMed]
- Polfuss, M.; Sawin, J.K.; Papanek, P.E.; Bandini, L.; Forseth, B.; Moosreiner, A.; Zvara, K.; Schoeller, D.A. Total energy expenditure and body composition of children with developmental disabilities. Disabil. Health J. 2018, 11, 442–446. [Google Scholar] [CrossRef]
- Mohamed, B.A.; Alhamdan, A.A.; Samarkandy, M.M. Dietary Practice and Physical Activity in Children with Down Syndrome and Their Siblings in Saudi Arabia. Can. J. Clin. Nutr. 2013, 1, 35–46. [Google Scholar] [CrossRef]
- Holmes, G. Gastrointestinal disorders in Down syndrome. Gastroenterol. Hepatol. Bed Bench. 2014, 7, 6–8. [Google Scholar] [PubMed]
- Abdallah, A.M.; Raffa, S.; Alaidaroos, T.; Obaid, R.; Abuznada, J. Nutritional Status of some Children and Adolescents with Down syndrome in Jeddah. Life Sci. J. 2013, 10, 1310–1318. [Google Scholar]
- Grammatikopoulou, M.G.; Manai, A.; Tsigga, M.; Tsiligiroglou-Fachantidou, A.; Galli-Tsinopoulou, A.; Zakas, A. Nutrient intake and anthropometry in children and adolescents with Down syndrome-a preliminary study. Dev. Neurorehabil. 2008, 11, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Białek-Dratwa, A.; Żur, S.; Wilemska-Kucharzewska, K.; Szczepańska, E.; Kowalski, O. Nutrition as Prevention of Diet-Related Diseases-A Cross-Sectional Study among Children and Young Adults with Down Syndrome. Children 2022, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Morris, L.; Bhatnagar, D. The Mediterranean diet. Curr. Opin. Lipidol. 2016, 27, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, V.; Germani, A.; Capuzzo, E.D.; Donini, L.M.; del Balzo, V. The new modern mediterranean diet italian pyramid. Ann. Ig. 2016, 28, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Velázquez-López, L.; Santiago-Díaz, G.; Nava-Hernández, J.; Muñoz-Torres, A.V.; Medina-Bravo, P.; Torres-Tamayo, M. Mediterranean-style diet reduces metabolic syndrome components in obese children and adolescents with obesity. BMC Pediatr. 2014, 14, 175. [Google Scholar] [CrossRef] [PubMed]
- Archero, F.; Ricotti, R.; Solito, A.; Carrera, D.; Civello, F.; Di Bella, R.; Bellone, S.; Prodam, F. Adherence to the Mediterranean Diet among School Children and Adolescents Living in Northern Italy and Unhealthy Food Behaviors Associated to Overweight. Nutrients 2018, 10, 1322. [Google Scholar] [CrossRef] [PubMed]
- Močnik, M.; Marčun Varda, N. Lipid Biomarkers and Atherosclerosis—Old and New in Cardiovascular Risk in Childhood. Int. J. Mol. Sci. 2023, 24, 2237. [Google Scholar] [CrossRef]
- Anania, C.; Perla, F.M.; Olivero, F.; Pacifico, L.; Chiesa, C. Mediterranean diet and nonalcoholic fatty liver disease. World J. Gastroenterol. 2018, 24, 2083–2094. [Google Scholar] [CrossRef]
- Misciagna, G.; Del Pilar Díaz, M.; Caramia, D.V.; Bonfiglio, C.; Franco, I.; Noviello, M.R.; Chiloiro, M.; Abbrescia, D.I.; Mirizzi, A.; Tanzi, M.; et al. Effect of a Low Glycemic Index Mediterranean Diet on Non-Alcoholic Fatty Liver Disease. A Randomized Controlled Clinici Trial. J. Nutr. Health Aging. 2017, 21, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Soliman, G.A. Dietary Fiber, Atherosclerosis, and Cardiovascular Disease. Nutrients 2019, 11, 1155. [Google Scholar] [CrossRef] [PubMed]
- Hernáez, Á.; Castañer, O.; Goday, A.; Ros, E.; Pintó, X.; Estruch, R.; Salas-Salvadó, J.; Corella, D.; Arós, F.; Serra-Majem, L.; et al. The Mediterranean Diet decreases LDL atherogenicity in high cardiovascular risk individuals: A randomized controlled trial. Mol. Nutr. Food Res. 2017, 61, 1601015. [Google Scholar] [CrossRef] [PubMed]
- Fox, B.; Moffett, G.E.; Kinnison, C.; Brooks, G.; Case, L.E. Physical Activity Levels of Children with Down Syndrome. Pediatr. Phys. Ther. 2019, 31, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Baynard, T.; Pitetti, K.H.; Guerra, M.; Unnithan, V.B.; Fernhall, B. Age-related changes in aerobic capacity in individuals with mental retardation: A 20-yr review. Med. Sci. Sports Exerc. 2008, 40, 1984–1989. [Google Scholar] [CrossRef] [PubMed]
- Mercer, V.S.; Lewis, C.L. Hip Abductor and Knee Extensor Muscle Strength of Children with and without Down Syndrome. Pediatr. Phys. Ther. 2001, 13, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Pitetti, K.; Baynard, T.; Agiovlasitis, S. Children and adolescents with Down syndrome, physical fitness and physical activity. J. Sport. Health Sci. 2013, 2, 47–57. [Google Scholar] [CrossRef]
- Roizen, N.J.; Patterson, D. Down’s syndrome. Lancet 2003, 361, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular disease risk in healthy children and its association with body mass index: Systematic review and meta-analysis. BMJ 2012, 345, e4759. [Google Scholar] [CrossRef] [PubMed]
- Adelekan, T.; Magge, S.; Shults, J.; Stallings, V.; Stettler, N. Lipid profiles of children with Down syndrome compared with their siblings. Pediatrics 2012, 129, e1382–e1387. [Google Scholar] [CrossRef]
- Garcia-de la Puente, S.; Flores-Arizmendi, K.A.; Delgado-Montemayor, M.J.; Vargas-Robledo, T.T. Lipid profile of Mexican children with Down syndrome. BMC Pediatr. 2021, 21, 77. [Google Scholar] [CrossRef]
- de la Piedra, M.J.; Alberti, G.; Cerda, J.; Cárdenas, A.; Paul, M.A.; Lizama, M. Alta frecuencia de dislipidemias en niños y adolescentes con Síndrome de Down [High frequency of dyslipidemia in children and adolescents with Down Syndrome]. Rev. Chil. Pediatr. 2017, 88, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M.; et al. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Eloranta, A.M.; Sallinen, T.; Viitasalo, A.; Lintu, N.; Väistö, J.; Jalkanen, H.; Tompuri, T.T.; Soininen, S.; Haapala, E.A.; Kiiskinen, S.; et al. The effects of a 2-year physical activity and dietary intervention on plasma lipid concentrations in children: The PANIC Study. Eur. J. Nutr. 2021, 60, 425–434. [Google Scholar] [CrossRef] [PubMed]
- van den Driessen Mareeuw, F.A.; Coppus, A.M.W.; Delnoij, D.M.J.; de Vries, E. Quality of health care according to people with Down syndrome, their parents and support staff-A qualitative exploration. J. Appl. Res. Intellect. Disabil. 2020, 33, 496–514. [Google Scholar] [CrossRef] [PubMed]
- Wexler, I.D.; Abu-Libdeh, A.; Kastiel, Y.; Nimrodi, A.; Kerem, E.; Tenenbaum, A. Optimizing health care for individuals with Down syndrome in Israel. Isr. Med. Assoc. J. 2009, 11, 655–659. [Google Scholar] [PubMed]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public. Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire. Health Fit. J. Can. 2011, 4, 18–22. [Google Scholar] [CrossRef]
- R Core Team R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 10 November 2023).
- Izquierdo-Gomez, R.; Martinez-Gómez, D.; Esteban-Cornejo, I.; Hallal, P.C.; García-Cervantes, L.; Villagra, A.; Veiga, O.L.; UP&DOWN study group. Changes in objectively measured physical activity in adolescents with Down syndrome: The UP&DOWN longitudinal study. J. Intellect. Disabil. Res. 2017, 61, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, L.; Flores-Barrantes, P.; Moreno, L.A.; Manios, Y.; Gonzalez-Gil, E.M. The Influence of Parental Dietary Behaviors and Practices on Children’s Eating Habits. Nutrients 2021, 13, 1138. [Google Scholar] [CrossRef]
- Gupta, R.S.; Shuman, S.; Taveras, E.M.; Kulldorff, M.; Finkelstein, J.A. Opportunities for health promotion education in childcare. Pediatrics 2005, 116, e499–e505. [Google Scholar] [CrossRef]
- Scaglioni, S.; Arrizza, C.; Vecchi, F.; Tedeschi, S. Determinants of children’s eating behavior. Am. J. Clin. Nutr. 2011, 94, 2006S–2011S. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Raaijmakers, L.G.; Gerards, S.M.; Kremers, S.P. Dietary Intake by Dutch 1- to 3-Year-Old Children at Childcare and at Home. Nutrients 2014, 6, 304–318. [Google Scholar] [CrossRef] [PubMed]
- McGrath, W. Ambivalent partners: Power, trust, and partnership in relationships between mothers and teachers in a full-time child-care center. Teach. Coll. Rec. 2007, 109, 1401–1422. [Google Scholar] [CrossRef]
- Dev, D.A.; Byrd-Williams, C.; Ramsay, S.; McBride, B.; Srivastava, D.; Murriel, A.; Arcan, C.; Adachi-Mejia, A.M. Engaging parents to promote children’s nutrition and health: Providers’ barriers and strategies in head start and child care centers. Am. J. Health Promot. 2017, 31, 153–162. [Google Scholar] [CrossRef]
- Pecoraro, L.; Solfa, M.; Ferron, E.; Mirandola, M.; Lauriola, S.; Piacentini, G.; Pietrobelli, A. Mediterranean diet and physical activity in Down syndrome pediatric subjects: The DONUT STUDY. Int. J. Food Sci. Nutr. 2022, 73, 973–980. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Baseline (n = 44) | 2-Year Follow-Up (n = 44) | p-Value |
|---|---|---|---|
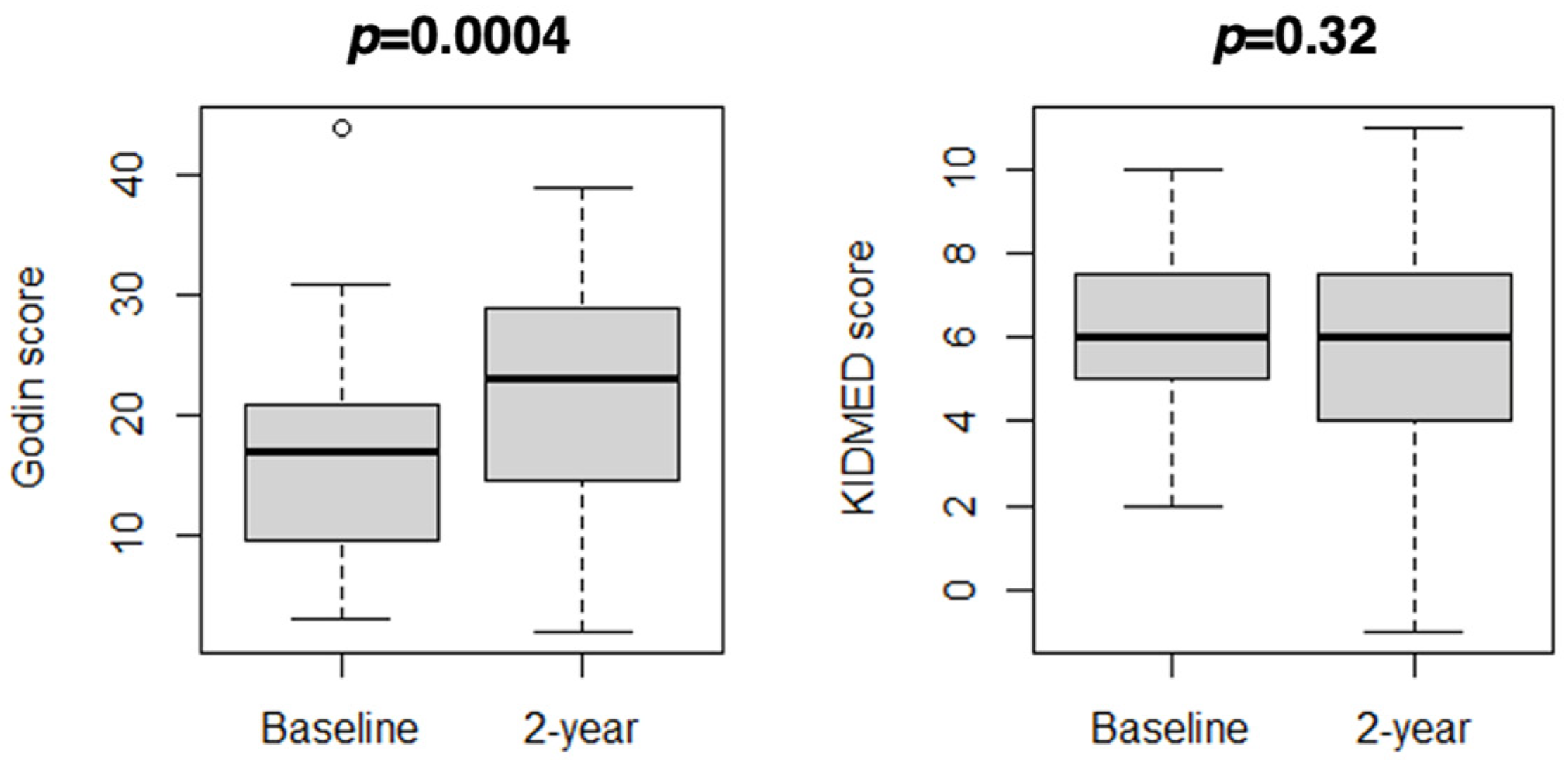
| Godin score: | 0.0004 | ||
| Mean (SD) | 17 (8) | 22 (10) | |
| Median (IQR) | 17 (10–21) | 23 (15–29) | |
| Min; max | 3; 44 | 2; 39 | |
| Physical activity, n (%): | 0.002 | ||
| Active | 6 (14%) | 22 (50%) | |
| Moderately active | 22 (50%) | 12 (27%) | |
| Insufficiently active | 16 (36%) | 10 (23%) | |
| KIDMED score: | 0.32 | ||
| Mean (SD) | 6 (2) | 6 (3) | |
| Median (IQR) | 6 (5–7) | 6 (4–7) | |
| Min; max | 2; 10 | 1; 11 | |
| Diet adherence, n (%): | 0.50 | ||
| High | 11 (25%) | 12 (27%) | |
| Moderate | 28 (64%) | 22 (50%) | |
| Low | 5 (11%) | 10 (23%) |
| Variable | Baseline (n = 44) | 2-Year Follow-Up (n = 44) | p-Value |
|---|---|---|---|
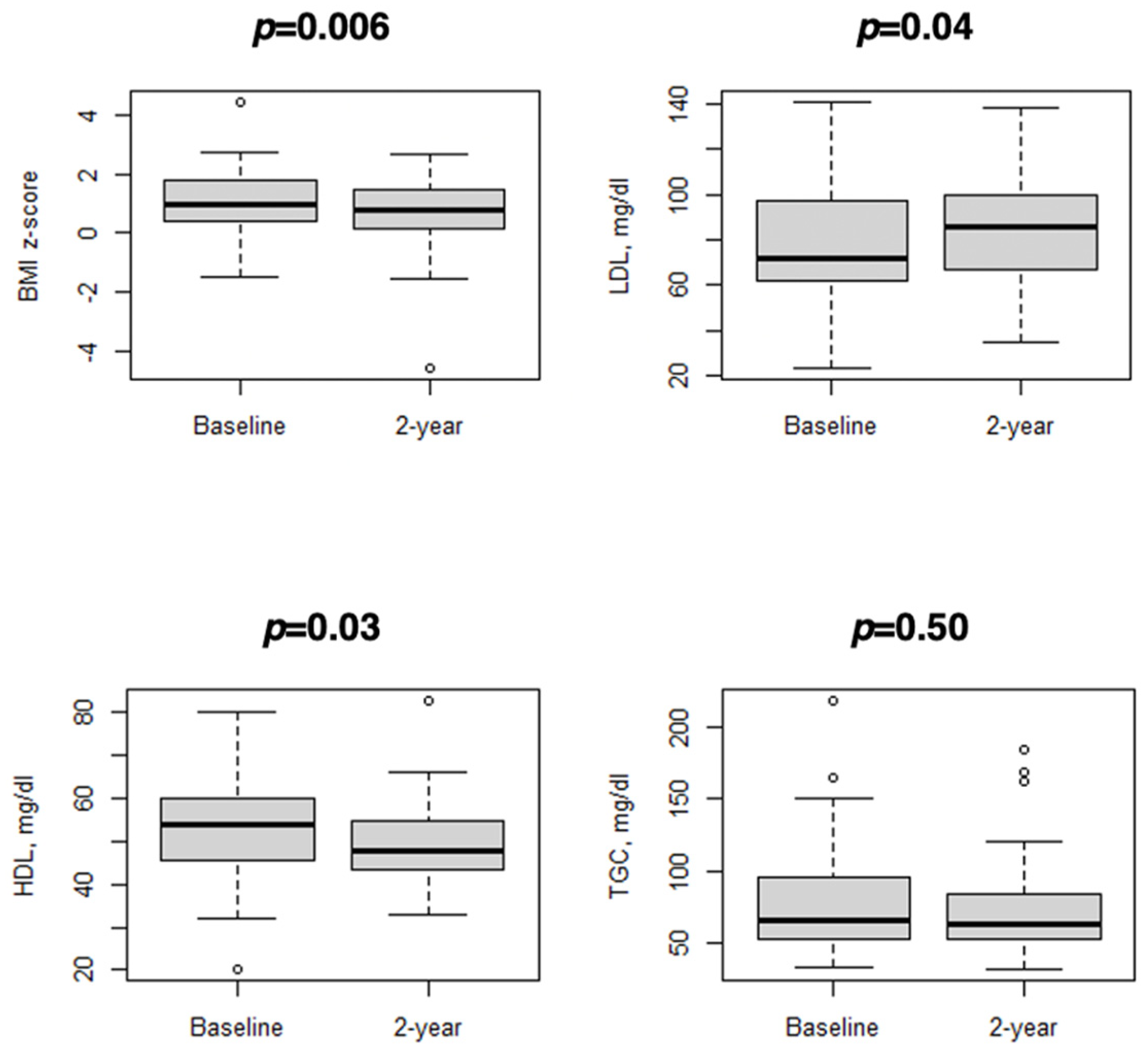
| BMI z-score: | 0.006 | ||
| Mean (SD) | 1.1 (1.2) | 0.7 (1.2) | |
| Median (IQR) | 1.0 (0.4–1.8) | 0.8 (0.1–1.4) | |
| Min; max | −1.5; 4.5 | −4.6; 2.7 | |
| BMI category, n (%): | 0.05 | ||
| Normal weight | 27 (61%) | 29 (66%) | |
| Overweight | 11 (25%) | 13 (30%) | |
| Obese | 6 (14%) | 2 (4%) | |
| LDL, mg/dl: | 0.04 | ||
| Mean (SD) | 78 (27) | 83 (24) | |
| Median (IQR) | 72 (62–97) | 86 (67–100) | |
| Min; max | 23; 141 | 35; 138 | |
| HDL, mg/dl: | 0.03 | ||
| Mean (SD) | 53 (12) | 50 (10) | |
| Median (IQR) | 54 (45–60) | 48 (43–55) | |
| Min; max | 20; 80 | 33; 83 | |
| TGC, mg/dl: | 0.50 | ||
| Mean (SD) | 79 (39) | 73 (33) | |
| Median (IQR) | 66 (53–96) | 63 (52–84) | |
| Min; max | 33; 219 | 31; 184 | |
| Dyslipidemia, n (%): | 13 (30%) | 15 (34%) | 0.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pecoraro, L.; Zadra, M.; Cavallin, F.; Lauriola, S.; Piacentini, G.; Pietrobelli, A. Lipid Profile, Eating Habit, and Physical Activity in Children with Down Syndrome: A Prospective Study. Diseases 2024, 12, 68. https://doi.org/10.3390/diseases12040068
Pecoraro L, Zadra M, Cavallin F, Lauriola S, Piacentini G, Pietrobelli A. Lipid Profile, Eating Habit, and Physical Activity in Children with Down Syndrome: A Prospective Study. Diseases. 2024; 12(4):68. https://doi.org/10.3390/diseases12040068
Chicago/Turabian StylePecoraro, Luca, Melissa Zadra, Francesco Cavallin, Silvana Lauriola, Giorgio Piacentini, and Angelo Pietrobelli. 2024. "Lipid Profile, Eating Habit, and Physical Activity in Children with Down Syndrome: A Prospective Study" Diseases 12, no. 4: 68. https://doi.org/10.3390/diseases12040068