
Sexual Functioning and Impact on Quality of Life in Patients with Early-Onset Colorectal Cancer: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria and Definitions
2.3. Definitions
2.4. Data Collection Process
2.5. Risk of Bias and Quality Assessment
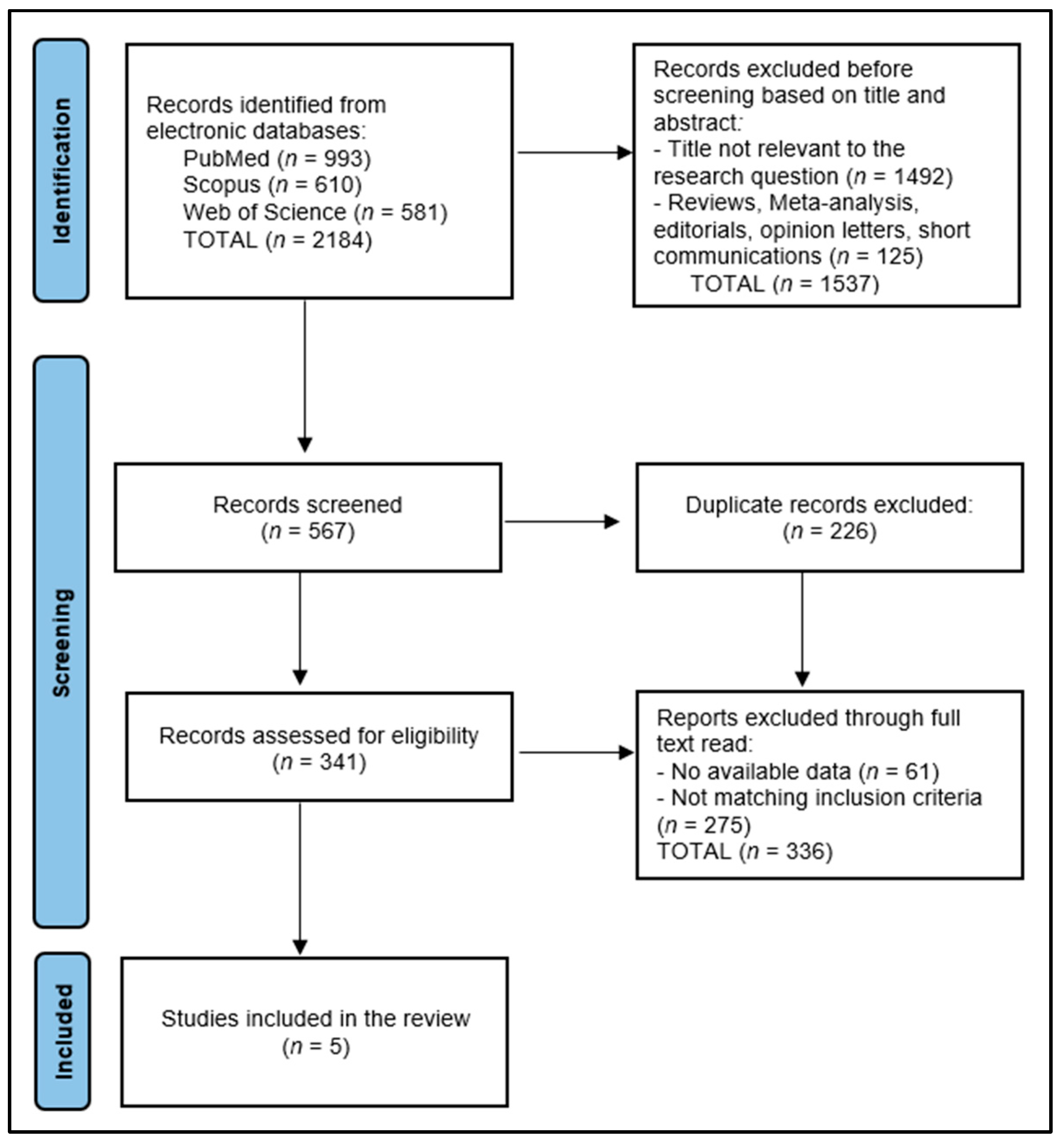
3. Results
3.1. Study Characteristics
3.2. Patients’ Characteristics
3.3. Disease Characteristics
3.4. Sexual Function and Quality of Life
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Constantinou, V.; Constantinou, C. Focusing on colorectal cancer in young adults (Review). Mol. Clin. Oncol. 2023, 20, 1–10. [Google Scholar] [CrossRef]
- Sifaki-Pistolla, D.; Poimenaki, V.; Fotopoulou, I.; Saloustros, E.; Mavroudis, D.; Vamvakas, L.; Lionis, C. Significant Rise of Colorectal Cancer Incidence in Younger Adults and Strong Determinants: 30 Years Longitudinal Differences between under and over 50s. Cancers 2022, 14, 4799. [Google Scholar] [CrossRef]
- Adigun, A.O.; Adebile, T.M.; Okoye, C.; Ogundipe, T.I.; Ajekigbe, O.R.; Mbaezue, R.N.; Okobi, O.E. Causes and Prevention of Early-Onset Colorectal Cancer. Cureus 2023, 15, e45095. [Google Scholar] [CrossRef] [PubMed]
- Ullah, F.; Pillai, A.B.; Omar, N.; Dima, D.; Harichand, S. Early-Onset Colorectal Cancer: Current Insights. Cancers 2023, 15, 3202. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.W.-K.; Lui, R.N. Early-onset colorectal cancer: Current insights and future directions. World J. Gastrointest. Oncol. 2022, 14, 230–241. [Google Scholar] [CrossRef]
- Danpanichkul, P.; Ongsupankul, S.; Moolkaew, P.; Yamsiri, R.; Panpradist, N. Increased Incidence of Early-Onset Colorectal Cancer in Low Sociodemographic Index Countries: Higher Rising Burden in Young Females. Cureus 2023, 15, e38998. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, V.; Laan, E.T.M.; Oudsten, B.L.D. Sexual health-related care needs among young adult cancer patients and survivors: A systematic literature review. J. Cancer Surviv. 2022, 16, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Heyne, S.; Taubenheim, S.; Dietz, A.; Lordick, F.; Götze, H.; Mehnert-Theuerkauf, A. Physical and psychosocial factors associated with sexual satisfaction in long-term cancer survivors 5 and 10 years after diagnosis. Sci. Rep. 2023, 13, 2011. [Google Scholar] [CrossRef] [PubMed]
- AlZaabi, A.; AlHarrasi, A.; AlMusalami, A.; AlMahyijari, N.; Al Hinai, K.; Aladawi, H.; Al-Shamsi, H.O. Early onset colorectal cancer: Challenges across the cancer care continuum. Ann. Med. Surg. 2022, 82, 104453. [Google Scholar] [CrossRef]
- Khoo, A.M.; Lau, J.; Loh, X.; Ng, C.W.; Griva, K.; Tan, K. Understanding the psychosocial impact of colorectal cancer on young-onset patients: A scoping review. Cancer Med. 2022, 11, 1688–1700. [Google Scholar] [CrossRef]
- Denlinger, C.S.; Barsevick, A.M. The Challenges of Colorectal Cancer Survivorship. J. Natl. Compr. Cancer Netw. 2009, 7, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Prodan-Bărbulescu, C.; Watz, C.-G.; Moacă, E.-A.; Faur, A.-C.; Dehelean, C.-A.; Faur, F.I.; Grigoriţă, L.O.; Maghiari, A.L.; Tuţac, P.; Duţă, C.; et al. A Preliminary Report Regarding the Morphological Changes of Nano-Enabled Pharmaceutical Formulation on Human Lung Carcinoma Monolayer and 3D Bronchial Microtissue. Medicina 2024, 60, 208. [Google Scholar] [CrossRef]
- Faur, I.F.; Dobrescu, A.; Clim, A.I.; Pasca, P.; Prodan-Barbulescu, C.; Gherle, B.D.; Tarta, C.; Isaic, A.; Brebu, D.; Duta, C.; et al. The Value of Tumor Infiltrating Lymphocytes (TIL) for Predicting the Response to Neoadjuvant Chemotherapy (NAC) in Breast Cancer according to the Molecular Subtypes. Biomedicines 2023, 11, 3037. [Google Scholar] [CrossRef]
- Virzob, C.R.B.; Poenaru, M.; Morar, R.; Horhat, I.D.; Balica, N.C.; Prathipati, R.; Moleriu, R.D.; Toma, A.-O.; Juganaru, I.; Bloanca, V.; et al. Efficacy of Bilateral Cochlear Implantation in Pediatric and Adult Patients with Profound Sensorineural Hearing Loss: A Retrospective Analysis in a Developing European Country. J. Clin. Med. 2023, 12, 2948. [Google Scholar] [CrossRef]
- Roussin, M.; Lowe, J.; Hamilton, A.; Martin, L. Sexual quality of life in young gynaecological cancer survivors: A qualitative study. Qual. Life Res. 2023, 32, 2107–2115. [Google Scholar] [CrossRef]
- Faur, I.F.; Clim, A.; Dobrescu, A.; Prodan, C.; Hajjar, R.; Pasca, P.; Capitanio, M.; Tarta, C.; Isaic, A.; Noditi, G.; et al. VRAM Flap for Pelvic Floor Reconstruction after Pelvic Exenteration and Abdominoperineal Excision. J. Pers. Med. 2023, 13, 1711. [Google Scholar] [CrossRef]
- Hansen, S.B.; Oggesen, B.T.; Fonnes, S.; Rosenberg, J. Erectile Dysfunction Is Common after Rectal Cancer Surgery: A Cohort Study. Curr. Oncol. 2023, 30, 9317–9326. [Google Scholar] [CrossRef]
- Schover, L.R.; van der Kaaij, M.; van Dorst, E.; Creutzberg, C.; Huyghe, E.; Kiserud, C.E. Sexual dysfunction and infertility as late effects of cancer treatment. Eur. J. Cancer Suppl. 2014, 12, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 372. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Bailey, C.E.; Cao, H.S.T.; Hu, C.-Y.; Chang, G.J.; Feig, B.W.; Rodriguez-Bigas, M.A.; Nguyen, S.T.; Skibber, J.M.; You, Y.N. Functional Deficits and Symptoms of Long-Term Survivors of Colorectal Cancer Treated by Multimodality Therapy Differ by Age at Diagnosis. J. Gastrointest. Surg. 2015, 19, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Sanford, S.D.; Zhao, F.; Salsman, J.M.; Chang, V.T.; Wagner, L.I.; Fisch, M.J. Symptom burden among young adults with breast or colorectal cancer. Cancer 2014, 120, 2255–2263. [Google Scholar] [CrossRef]
- Perl, G.; Nordheimer, S.; Lando, S.; Benedict, C.; Brenner, B.; Perry, S.; Shmoisman, G.; Purim, O.; Amit, L.; Stemmer, S.M.; et al. Young patients and gastrointestinal (GI) tract malignancies—Are we addressing the unmet needs? BMC Cancer 2016, 16, 630. [Google Scholar] [CrossRef]
- REACCT Collaborative. Post-Operative Functional Outcomes in Early Age Onset Rectal Cancer. Front. Oncol. 2022, 12, 868359. [Google Scholar] [CrossRef]
- Stal, J.; Yi, S.Y.; Cohen-Cutler, S.; Gallagher, P.; Barzi, A.; Freyer, D.R.; Kaslander, J.N.; Anto-Ocrah, M.; Lenz, H.-J.; Miller, K.A. Sexual dysfunction among early-onset colorectal cancer survivors: Sex-specific correlates of sexual health discussions between patients and providers. Cancer Causes Control. 2024, 35, 111–120. [Google Scholar] [CrossRef]
- Heyne, S.; Esser, P.; Geue, K.; Friedrich, M.; Mehnert-Theuerkauf, A. Frequency of Sexual Problems and Related Psychosocial Characteristics in Cancer Patients—Findings From an Epidemiological Multicenter Study in Germany. Front. Psychol. 2021, 12, 679870. [Google Scholar] [CrossRef] [PubMed]
- Scrobotă, I.; Alb, C.; Calniceanu, H. Assessment of Serum Lipid Peroxidation and Redox Thiol System Status in Different Stages of Oral Careinogenesis. Rev Chim-Buchar. 2015, 66, 1467–1470. [Google Scholar]
- Ramlachan, P.; Tammary, E.; Joachim, O.; Edward, I.M.; Magueye, S. Management of Psychosocial and Sexual Complains Among Cancer Patients in the African Context: A scoping review. Sex. Med. 2022, 10, 100494. [Google Scholar] [CrossRef]
- Dolghi, A.; Buzatu, R.; Dobrescu, A.; Olaru, F.; Popescu, G.A.; Marcovici, I.; Pinzaru, I.; Navolan, D.; Cretu, O.M.; Popescu, I.; et al. Phytochemical Analysis and In Vitro Cytotoxic Activity against Colorectal Adenocarcinoma Cells of Hippophae rhamnodies L., Cymbopogon citratus (D.C.) Stapf, and Ocimum basilicum L. Essential Oils. Plants 2021, 10, 2752. [Google Scholar] [CrossRef]
- Jacobsen, R.L.; Macpherson, C.F.; Pflugeisen, B.M.; Johnson, R.H. Care experience, by site of care, for adolescents and young adults with cancer. JCO Oncol. Pract. 2021, 17, e817–e826. [Google Scholar] [CrossRef]
- McKay, G.E.; Zakas, A.L.; Osman, F.; Lee-Miller, C.; Pophali, P.; Parkes, A. Disparities between provider assessment and documentation of care needs in the care of adolescent and young adult patients with sarcoma. JCO Oncol. Pract. 2021, 17, e891–e900. [Google Scholar] [CrossRef] [PubMed]
- Holowatyj, A.N.; Eng, C.; Lewis, M.A. Incorporating Reproductive Health in the Clinical Management of Early-Onset Colorectal Cancer. JCO Oncol. Pract 2021, 18, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Averyt, J.C.; Nishimoto, P.W. Addressing sexual dysfunction in colorectal cancer survivorship care. J. Gastrointest. Oncol. 2014, 5, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Blum-Barnett, E.; Ma, S.M.; Burnett-Hartman, A.; Mueller, S.R.; McMullen, C.K.; Dwyer, A.; Feigelson, H.S. Financial burden and quality of life among early-onset colorectal cancer survivors: A qualitative analysis. Health Expect. 2019, 22, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Traa, M.J.; De Vries, J.; Roukema, J.A.; Oudsten, B.L.D. Sexual (dys)function and the quality of sexual life in patients with colorectal cancer: A systematic review. Ann. Oncol. 2011, 23, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Liot, E.; Christou, N.; de Sousa, S.; Klein, J.; Pouya, I.; Guedj, D.; Buchs, N.C.; Ris, F. Patients’ related sexual outcomes in colorectal surgery. Front. Oncol. 2022, 12, 968978. [Google Scholar] [CrossRef] [PubMed]
- Mudaranthakam, D.P.; Hughes, D.; Johnson, P.; Mason, T.; Nollen, N.; Wick, J.; Welch, D.R.; Calhoun, E. Career disruption and limitation of financial earnings due to cancer. JNCI Cancer Spectr. 2023, 7, pkad044. [Google Scholar] [CrossRef] [PubMed]
- de Boer, A.G.; de Wind, A.; Coenen, P.; van Ommen, F.A.; Greidanus, M.; Zegers, A.D.A.; Duijts, S.F.; Tamminga, S.J. Cancer survivors and adverse work outcomes: Associated factors and supportive interventions. Br. Med. Bull. 2023, 145, 60–71. [Google Scholar] [CrossRef]
- Acquati, C.; Wittmann, D.; Roth, M.; Rosen, A.; Carr, L.C.; Gresham, Z.; Ionescu, E. Sexual Health Outcomes of Adolescent and Young Adult Colorectal Cancer Survivors and Their Partners: Protocol of a Dyadic Mixed Methods Study. JMIR Res. Protoc. 2023, 12, e41831. [Google Scholar] [CrossRef]
- Velegraki, J.M.; Bacopoulou, F.; Chrousos, G.P.; Panagiotou, M.; Gerakini, O.; Charalampopoulou, M.; Vlachakis, D.; Darviri, C. Reliability and validity of the Dyadic Coping Inventory for Financial Stress in Greek couples. EMBnet J. 2023, 28, e1018. [Google Scholar] [CrossRef]
- Patel, A.; Nair, B.V.S.; Das, S.K.; Kumar, P.; Sharma, P.S.V.N. Re-examining psychometric properties of fertility problem inventory: A clinic-based study from India. J. Hum. Reprod. Sci. 2022, 15, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Yang, C.-Y.; Zhou, M.; Bai, J.; Inder, K.; Chan, S.W.-C. Validity and reliability of an Emotional Thermometer tool: An exploratory cross-sectional study. Contemp. Nurse 2023, 59, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.; Clavijo, R.I. Management of male sexual dysfunction after cancer treatment. Urol. Oncol. Semin. Orig. Investig. 2020, 40, 389–394. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study and Author | Country | Study Year | Study Design | Study Quality |
|---|---|---|---|---|
| 1 [21] Bailey et al. | United States | 2014 | Cross-sectional | Low |
| 2 [22] Sanford et al. | United States | 2014 | Prospective cohort | Medium |
| 3 [23] Perl et al. | Israel | 2016 | Cross-sectional | Medium |
| 4 [24] REACCT | Ireland | 2022 | Prospective cohort | Medium |
| 5 [25] Stal et al. | United States | 2023 | Cross-sectional | Medium |
| Study Number | Sample Size | Age (Years) | Gender Distribution | Comparison Group | Race/Ethnicity |
|---|---|---|---|---|---|
| 1 [21] Bailey et al. | 282 | 43.4 | 143 (50.7%) men 139 (49.3%) women | Late-onset CRC | White: 226 (80.1%) Hispanic: 31 (1.0%) Black: 17 (6.0%) |
| 2 [22] Sanford et al. | 37 | 34.3 | 19 (51.3%) men 18 (48.6%) women | ≥40 years old CRC | White: 31 (83.7%) Black: 6 (16.3%) |
| 3 [23] Perl et al. | 50 | 35.5 | 24 (45%) men 26 (55%) women | Male vs. female with CRC | Jewish: 22 (64%) Arab: 2 (4%) |
| 4 [24] REACCT | 1428 | 42 | 816 (57%) men 612 (43%) women | NR | NR |
| 5 [25] Stal et al. | 234 | 34.6 | 145 (61.9%) men 87 (38.1%) women | Male vs. female with CRC | White: 180 (77.9%) Black: 23 (10.0%) Hispanic: 22 (9.5%) |
| Study Number | Disease Duration | Disease Severity | Surgical History | Treatment | Complications |
|---|---|---|---|---|---|
| 1 [21] Bailey et al. | 10.6 years | Metastasis: 41 (14.5%) | Surgery: 276 (97.9%) Ostomy: 44 (15.6%) | Chemotherapy: 243 (86.2%) Radiation: 147 (52.1%) | Active cancer: 24 (8.5%) |
| 2 [22] Sanford et al. | NR | Metastasis: 13 (35.1%) | NR | Chemotherapy: 18 (48%) Radiation: 6 (16.2%) | Disease progression: 26 (70.2%) |
| 3 [23] Perl et al. | NR | Stage IV: 13 (26.0%) | Surgery: 7 (14%) | Chemotherapy: 3 (6%) Chemoradiotherapy: 40 (80%) | NR |
| 4 [24] REACCT | 42 months | Stage IV: 184 (12.8%) | Surgery: 1395 (97%) R0 resection: 1212 (84%) Ostomy: 621 (43%) | Chemoradiotherapy: 487 (34.1%) Radiation: 12 (0.8%) | Major post-operative complication (Clavien Dindo 3–4) |
| 5 [25] Stal et al. | 32.7 months | Stage IV: 6 (2.6%) | Surgery: 124 (53.0%) Ostomy: 82 (35.7%) | Chemotherapy: 82 (35.0%) Radiation: 133 (56.8%) Immunotherapy: 64 (27.4%) | Relapse: 143 (61.4%) |
| Risk Factors | Sexual Function | Psychometrics | Functional | Survey | Conclusion |
|---|---|---|---|---|---|
| 1 [21] Bailey et al. | Impotence 50% Dyspareunia 33% Dysfunction men 58% Dysfunction women 36% | Anxiety 69.6% Low body image 81.8% | Micturition problems 29% Bowel dysfunction 34% Pain 12% | EORTC | High prevalence of impotence in EOCRC compared to old patients Worse body image compared to old patients |
| 2 [22] Sanford et al. | Severe impact of intimate life 24% | Distress 37.8% Sadness 24.3% Low mood 40.5% | Pain 27% Diarrhea 16% | SOAPP MDASI | Significantly higher impact on intimate life compared to old patients |
| 3 [23] Perl et al. | Dysfunction men 58% Dysfunction women 61% | Sleeping disorder 32% | Pain 31% Diarrhea 37% | SF-12 CARES | Worse functioning in women compared with men |
| 4 [24] REACCT | Dysfunction 4.5% Infertility 1% | NR | Bowel dysfunction 16% Bladder dysfunction 7% | NR | NR |
| 5 [25] Stal et al. | FSFI mean 14.3 IIEF mean 13.6 Erection hard enough for penetration never/almost never 37.9% | Low/very low confidence 33.1% | NR | FSFI-6 IIEF-5 | 8 of 10 females reported FSD, almost all males reported ED |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feier, C.V.I.; Paunescu, I.A.; Faur, A.M.; Cozma, G.V.; Blidari, A.R.; Muntean, C. Sexual Functioning and Impact on Quality of Life in Patients with Early-Onset Colorectal Cancer: A Systematic Review. Diseases 2024, 12, 66. https://doi.org/10.3390/diseases12040066
Feier CVI, Paunescu IA, Faur AM, Cozma GV, Blidari AR, Muntean C. Sexual Functioning and Impact on Quality of Life in Patients with Early-Onset Colorectal Cancer: A Systematic Review. Diseases. 2024; 12(4):66. https://doi.org/10.3390/diseases12040066
Chicago/Turabian StyleFeier, Catalin Vladut Ionut, Ionut Andrei Paunescu, Alaviana Monique Faur, Gabriel Veniamin Cozma, Andiana Roxana Blidari, and Calin Muntean. 2024. "Sexual Functioning and Impact on Quality of Life in Patients with Early-Onset Colorectal Cancer: A Systematic Review" Diseases 12, no. 4: 66. https://doi.org/10.3390/diseases12040066