1. Introduction
The coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has posed unprecedented challenges to global public health and socio-economic systems [
1]. Since its emergence in late 2019, millions have been infected worldwide, with significant morbidity and mortality [
2]. As of 2022, COVID-19 has resulted in the death of millions globally, causing immense strain on healthcare systems and profoundly affecting the lives of those who survived [
3].
While many who contract COVID-19 experience a full recovery, a significant portion have reported persistent symptoms long after their initial diagnosis [
4]. Termed as “Post-COVID Syndrome” or “Long COVID”, this phenomenon encompasses a myriad of symptoms, including fatigue, joint pain, cognitive disturbances, and respiratory complications, among others [
5]. Nevertheless, some symptoms are associated directly with long-COVID, while others accompany it. The exact physiological mechanism behind long-COVID syndrome remains an area of active research, but its implications for the quality of life of those affected are evident [
6].
Recent studies estimate that a substantial proportion of COVID-19 survivors, ranging from 10% to 30%, may experience symptoms of long-COVID syndrome [
7,
8]. The persistence and unpredictability of these symptoms have led to mounting concerns about long-term health impacts, healthcare needs, and the subsequent socio-economic ramifications. This has ignited global interest in understanding the spectrum of post-acute sequelae of SARS-CoV-2 infection and identifying nterventions to mitigate these lasting effects [
9,
10].
The rollout of COVID-19 vaccinations has been a beacon of hope, significantly reducing infection rates, hospitalizations, and deaths in many parts of the world, with a worldwide campaign initiated at the end of 2020, during the first year of the pandemic, giving credits to the mRNA technology [
11,
12,
13]. While vaccines are predominantly used for preventing acute COVID-19, there is growing evidence indicating that vaccination may also play a role in reducing the incidence of long-COVID symptoms in vaccinated individuals. However, the complete relationship between vaccination status and the incidence and severity of long-COVID is yet to be thoroughly understood [
14,
15]. Nevertheless, long-COVID is still a disputed topic, and despite the volume of research surrounding COVID-19, there remains a limited understanding of the interplay between quality of life, coping strategies, and the psychological impacts, specifically depression, in individuals diagnosed with long-COVID syndrome. Gaining insights into these areas is essential to devising holistic care strategies for affected individuals.
Therefore, the present study aims to undertake a longitudinal assessment of quality of life, coping strategies, anxiety, and depression in COVID-19 patients, drawing comparisons between those with and without long-COVID syndrome. Our hypotheses posit that individuals with long-COVID syndrome will report diminished quality of life, different coping mechanisms, and higher rates of anxiety and depression compared to their counterparts without the syndrome. Through this research, we aspire to illuminate the psychosocial dimensions of long-COVID and contribute to the collective understanding of its long-term implications.
2. Materials and Methods
2.1. Research Design and Ethical Considerations
The study employed a longitudinal research design to explore the quality of life, coping strategies, anxiety and depression among COVID-19 patients from the onset of their diagnosis and subsequently over a defined period. This approach was taken to understand the trajectory of these parameters, especially in the context of long-COVID syndrome. Patients were recruited after admission to the Victor Babes Hospital for Infectious Diseases and Pulmonology in Timisoara, Romania, affiliated with the Victor Babes University of Medicine and Pharmacy from Timisoara. Adhering to the strictest ethical standards, the research was approved by the Local Commission of Ethics for Scientific Research, which is in alignment with the EU GCP Directives 2005/28/EC, ICH guidelines, and the principles specified in the Declaration of Helsinki. Before patient inclusion, a signed informed consent was obtained from all patients willing to participate in the study after carefully explaining the study methods and objectives.
2.2. Inclusion Criteria and Definitions
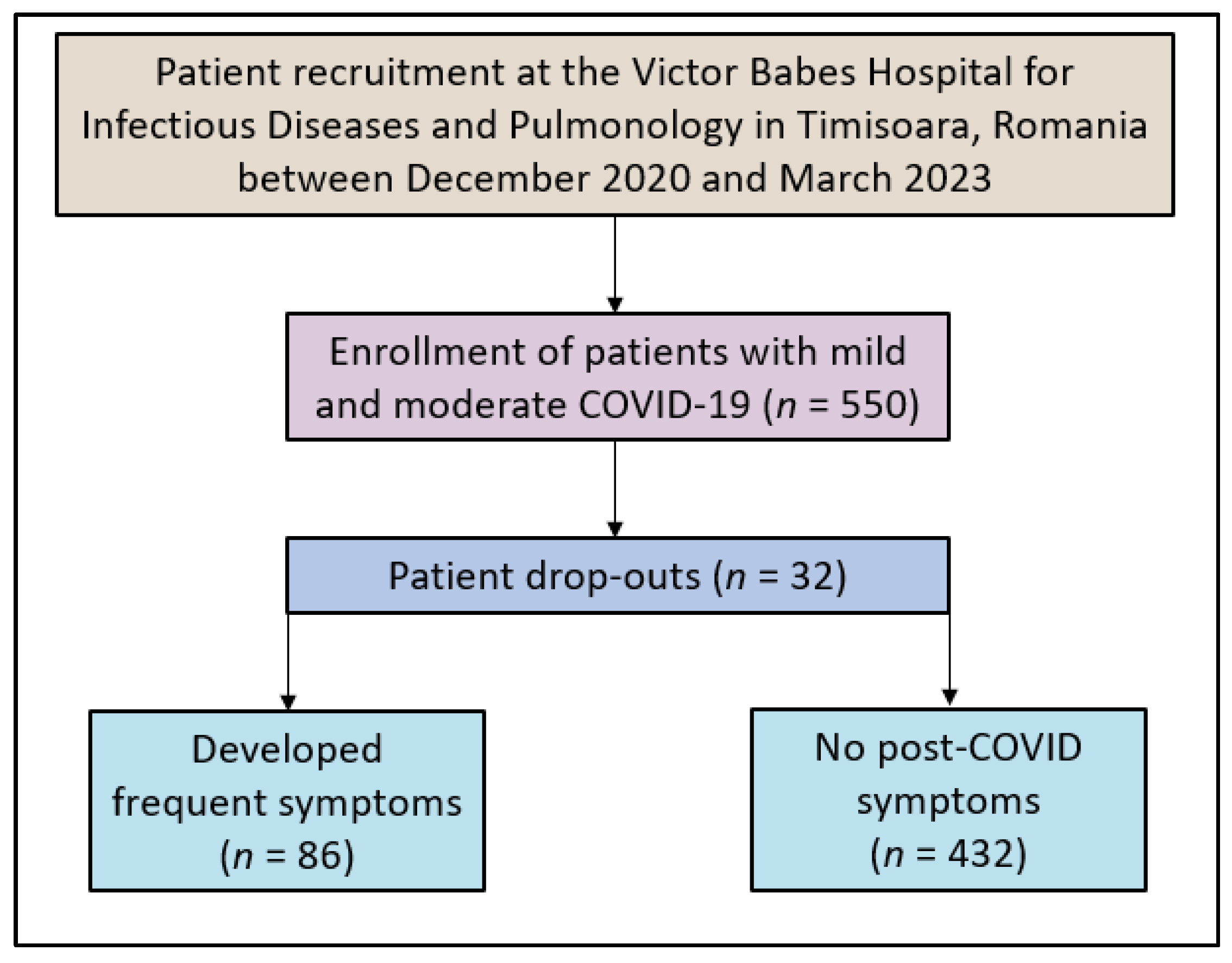
In our study, we employed a methodical and continuous selection process to recruit patients, focusing on those willing to participate, according to the study flowchart presented in
Figure 1. The participant selection began by collaborating with treating physicians to identify potential candidates diagnosed with mild to moderate COVID-19. Eligible patients were adults aged 18 and above who were admitted to hospitals for their condition, ensuring the exclusion of severe cases and thereby eliminating potential confounding factors. For each month of the study, a specific number of patients were targeted to ensure a substantial sample size for the entire research duration. The exclusion criteria included patients who did not consent to participate in the study, those with a history of pre-existing chronic respiratory or psychiatric conditions, and those with incomplete questionnaire responses. Only patients after mild or moderate COVID-19 were considered for study inclusion to avoid confounding effects of severe COVID-19. The decision to assign patients to the two groups was binary: the development of frequent symptoms or disease resolution without symptoms at 6 months.
Long COVID-19 syndrome refers to a collection of symptoms that persist beyond four weeks from the onset of the initial acute symptoms of the SARS-CoV-2 virus. Despite biochemical evidence that viral replication ceases about four weeks after initial infection, some individuals continue to experience lingering symptoms. The Center for Disease Control (CDC) has formulated the term “post-COVID syndrome” to encompass long-COVID symptoms and persistent post-COVID syndrome (PPCS), multiorgan effects of COVID-19, and the impacts of COVID-19 treatment or hospitalization [
16]. Common manifestations of this syndrome include fatigue, brain fog, dyspnea, autonomic dysfunction, and various symptoms related to cardiovascular, pulmonary, renal, neuropsychiatric, endocrine, and hematologic systems. The duration, severity, and specific manifestations can vary widely among patients.
COVID-19 severity was classified according to the World Health Organization (WHO) guidelines [
17]. Mild COVID-19 cases are characterized by symptoms such as fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, and loss of taste and smell without evidence of viral pneumonia or hypoxia. Moderate cases involve clinical signs of pneumonia (fever, cough, dyspnea, tachypnea) but no signs of severe pneumonia, including SpO2 ≥ 90% on room air. All cases were confirmed through the use of a RT-PCR test.
2.3. Variables
The longitudinal assessment spanned over a 6 months period post-admission, observing the potential emergence and persistence of long-COVID syndrome. Variables assessed included the patient’s age, gender, socio-economic background, medical history, and COVID-19 severity. A paramount focus was placed on their quality of life, coping strategies, and mental health status. Through these methods, the study aimed to discern patterns and correlations that might offer insights into the evolution of long-COVID syndrome over time. All data collected were anonymized in accordance with the EU GDPR requirements.
2.4. Surveys Employed
In the study, a thorough approach was taken to understand the experiences of the participants, employing various validated instruments. The WHOQOL-BREF [
18], consisting of 26 questions, was used to assess the overall quality of life. Additionally, to evaluate the coping strategies of patients during and post their COVID-19 illness, the COPE-60 [
19] tool was introduced. The study also incorporated the Hospital Anxiety and Depression Scale (HADS) [
20], which includes 14 items, to determine the levels of anxiety and depression among the participants. Furthermore, a set of specific questions was designed to gather detailed information about the patients’ experiences with COVID-19, including symptoms, hospitalization, and health status after recovery.
The COPE-60 tool is divided into various subscales, each representing different coping methods. The disengagement subscale measures avoidance coping, where individuals distance themselves from stressors or related emotions; higher scores suggest a tendency to avoid confronting stressors. The Engagement subscale evaluates an approach coping strategy, indicating how individuals actively deal with stressors; a higher score here implies a proactive approach to stress. The emotion-focused subscale focuses on managing emotional distress rather than the actual problem, with higher scores indicating a preference for strategies like seeking emotional support or expressing feelings. Lastly, the problem-focused subscale assesses direct problem-solving strategies, where higher scores mean a preference for directly addressing and resolving stressors.
2.5. Data Collection and Quality Control
Participants were given the aforementioned surveys upon their admission (baseline) and at a predefined interval of 6 months post their discharge. This structured approach ensured consistent tracking and assessment. Data were collated and analyzed using SPSS v.26 (SPSS Inc., Chicago, IL, USA) statistical software. Descriptive statistics were first employed to understand the demographic distribution, followed by inferential statistics to decipher potential correlations and patterns. Ensuring data integrity and consistency, double data entry methods were employed. Regular audits of the data collection process were scheduled to confirm adherence to the study protocol. Any inconsistencies or discrepancies identified during these audits were addressed promptly to maintain the quality of the study findings.
2.6. Statistical Analysis
The study’s data management and analysis procedures were carried out using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA). The participant selection was based on a convenience sampling method, aiming for at least 180 respondents. This sample size was determined to ensure a 95% confidence level with a margin of error of 10%. In terms of data representation, continuous variables were shown as mean ± standard deviation (SD). On the other hand, categorical variables were presented through their frequencies and percentages. For the purpose of comparing two means of continuous variables, Student’s t-test was employed. Additionally, the Chi-square test was used for analyzing categorical variables. The study established a p-value of less than 0.05 as the criterion for considering results to be statistically significant (95% statistical acceptance level). All results were double-checked to ensure accuracy and reliability.
3. Results
In the current study, we observed a total of 86 patients presenting frequent post-acute COVID-19 symptoms and compared them to 432 individuals who reported no symptoms at 6 months after hospital discharge. Both groups were similar in age, with means of 55.2 ± 8.6 years for those with symptoms and 54.8 ± 8.9 years for the asymptomatic group (
p = 0.786). BMI values were also comparable, averaging 24.5 ± 4.2 and 24.8 ± 4.0, respectively (
p = 0.656). The proportion of individuals who smoked was virtually identical in both groups at around 21%. Alcohol use was reported by 51 (58.1%) of symptomatic individuals and 214 (49.5%) of those without symptoms, but this difference was not statistically significant (
p = 0.302). Similarly, substance use and urban origins showed no significant variations between the cohorts. When considering education levels, distributions across high school, college, and university degrees were evenly matched between groups (
p = 0.730). The percentage of individuals vaccinated against COVID-19 was slightly lower among symptomatic patients at 18 (20.9%) compared to 122 (28.2%) in the asymptomatic group, though this difference was not quite significant (
p = 0.072). The Charlson Comorbidity Index (CCI) and initial COVID-19 severity similarly revealed no significant disparities between the two groups, as described in
Table 1.
In the unstandardized survey presented in
Table 2, it was observed that lingering fatigue or tiredness after COVID-19 was considerably more pronounced in the frequent symptoms group, with a mean score of 8.2, as opposed to 5.1 in the asymptomatic group (
p < 0.001). Similarly, cognitive difficulties like brain fog or memory issues were notably higher among the symptomatic patients, scoring an average of 7.5 in sharp contrast to 5.4 in their counterparts (
p < 0.001). Respiratory challenges after recovery also showed a significant disparity: those with frequent symptoms rated it at 6.8, while those without symptoms reported a milder impact with a score of 4.8 (
p < 0.001). The toll on the overall quality of life post-illness was palpable among those with symptoms, scoring 7.0 compared to 3.2 in the asymptomatic group (
p < 0.001).
Sadness, hopelessness, or depressive feelings were more predominant among the symptomatic individuals, with an average of 7.3 out of a maximum of 10, while the no-symptoms group averaged 5.9 (p < 0.001). Likewise, reliance on coping strategies post-recovery was higher among the symptomatic group, with a score of 6.7 against 5.0 for the other group (p < 0.001). Evaluations of current mental well-being in comparison to the pre-COVID period were lower among those with symptoms, scoring 4.8, as opposed to 6.5 in the no-symptoms cohort (p < 0.001). Patients with frequent symptoms also reported persistent symptoms related to organs post-recovery (p < 0.001). Interestingly, when questioned about feeling supported in managing lingering symptoms or challenges post-COVID-19, those with symptoms felt less supported, scoring 5.6, whereas the no-symptoms group felt more supported with a score of 7.5 (p < 0.001). Lastly, the experience of COVID-19 seemed to have a more profound influence on the health and wellness perspective of those with frequent symptoms.
Another key focus was to evaluate anxiety and depression levels among individuals who reported frequent post-acute COVID-19 symptoms and compare them with those who did not manifest any symptoms post-infection. The assessment was facilitated using the HADS survey, as presented in
Table 3. Upon examination of the data, patients with frequent symptoms demonstrated notably higher levels of anxiety with an average score of 7.1 ± 2.3, in contrast to those without symptoms, who reported a mean score of 5.5 ± 3.6 (
p < 0.001). The trend was similar in terms of depression levels, where those experiencing frequent symptoms had a mean score of 6.8 ± 1.9, significantly higher than the 5.1 ± 2.4 average of the asymptomatic group (
p < 0.001). When the total scores, indicative of overall mental distress, were considered, there was a clear disparity between the two groups. Those with frequent post-acute symptoms had a mean total score of 13.4 ± 4.7, while the group without symptoms averaged 10.6 ± 4.8 (
p < 0.001).
The WHOQOL-BREF survey was employed to evaluate the quality of life in patients presenting with frequent post-acute COVID-19 symptoms and compare it to those without subsequent symptoms after SARS-CoV-2 infection. The results revealed a significant divergence in the quality of life between the two groups across multiple domains. In the physical domain, patients with frequent post-acute symptoms scored notably lower, with an average of 58.8 ± 15.8, as opposed to those without symptoms, who achieved an average score of 67.5 ± 16.7 (p = 0.002). The difference was also evident in the mental domain, where individuals experiencing frequent symptoms averaged 56.3 ± 16.4, contrasting the 64.0 ± 15.9 average of the group devoid of post-COVID symptoms (p = 0.004).
Further differences between the groups emerged in the social domain, with the frequent symptoms cohort scoring 50.2 ± 17.5, significantly lower than the 59.5 ± 18.0 average of their counterparts (
p = 0.002). However, when assessing the environmental domain, while those with symptoms had a lower score (57.0 ± 14.8) compared to those without symptoms (62.4 ± 17.2), the difference was not statistically significant at the conventional threshold, with a
p-value of 0.056, as seen in
Table 4.
The most pronounced divergence was seen in the disengagement coping strategy. A striking 62 (72.1%) of those with ongoing symptoms scored above the median, a substantial increase compared to the 130 (30.1%) observed in the group without symptoms (p < 0.001). These data strongly suggest that patients grappling with continued health issues tend to retreat from stressors more than those who have fully recovered. Regarding emotion-focused coping, 68 (79.1%) of those with symptoms were above the median, indicating a predominant use of emotional management to cope with stress. This is a significant contrast to the 162 (37.5%) in the asymptomatic group (p < 0.001), underscoring a reliance on emotional coping mechanisms among patients with persistent symptoms.
Conversely, problem-focused coping was less prevalent among those with enduring symptoms, with only 24 (27.9%) scoring above the median, as opposed to 186 (43.1%) of those without symptoms (
p = 0.009). This suggests that patients free from post-acute symptoms are more inclined to confront stressors head-on, seeking to address or mitigate them actively. Engagement coping strategies exhibited no significant difference statistically, with 36 (41.8%) of symptomatic individuals and 198 (45.8%) of those without symptoms scoring above the median (
p = 0.498), as described in
Table 5.
The quality of life domains, particularly the mental and physical domains of the WHOQOL-BREF, exhibit a strong negative association with the HADS total score, with coefficients of −0.296 and −0.247, respectively, both reaching statistical significance (
p < 0.001 and
p = 0.004). This suggests that better-perceived quality of life in these domains is associated with lower levels of anxiety and depression among patients. Additionally, coping strategies present contrasting effects, while disengagement shows a positive association with higher HADS scores (coefficient: 0.298,
p < 0.001), indicating that reliance on disengagement strategies might exacerbate mental health challenges. Engagement strategies show a negative association (coefficient: −0.103,
p = 0.046), implying their potential benefit in mitigating anxiety and depression. Furthermore, the presence of lingering fatigue and cognitive difficulties post-COVID are significantly associated with higher HADS scores (coefficients: 0.405 and 0.348, both
p < 0.001), highlighting the substantial mental health impact of these persistent symptoms, as presented in
Table 6.


 ,
, 



{kind=link}